
Comparison of Hospital-Based and Home-Based Obstructive Sleep Apnoea Severity Measurements with a Single-Lead Electrocardiogram Patch

 , , ,
, , ,
Abstract
:1. Introduction
2. Related Research
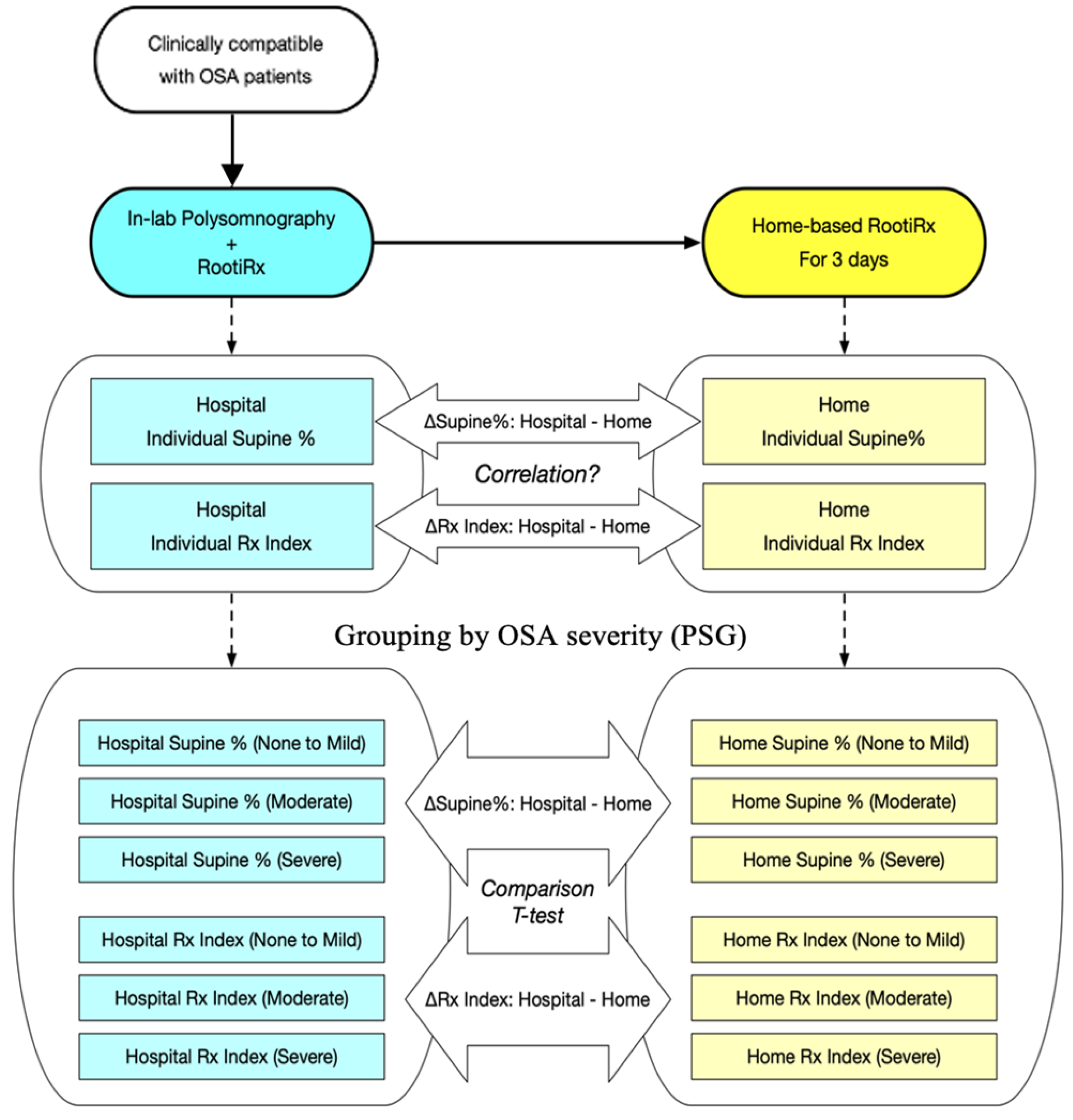
3. Materials and Methods
3.1. Study Population
3.2. PSG Results
3.3. Home Sleep Recording
3.4. Statistical Analysis
4. Results
4.1. Sample Characteristics
4.2. Hospital- and Home-Based Sleep Parameters
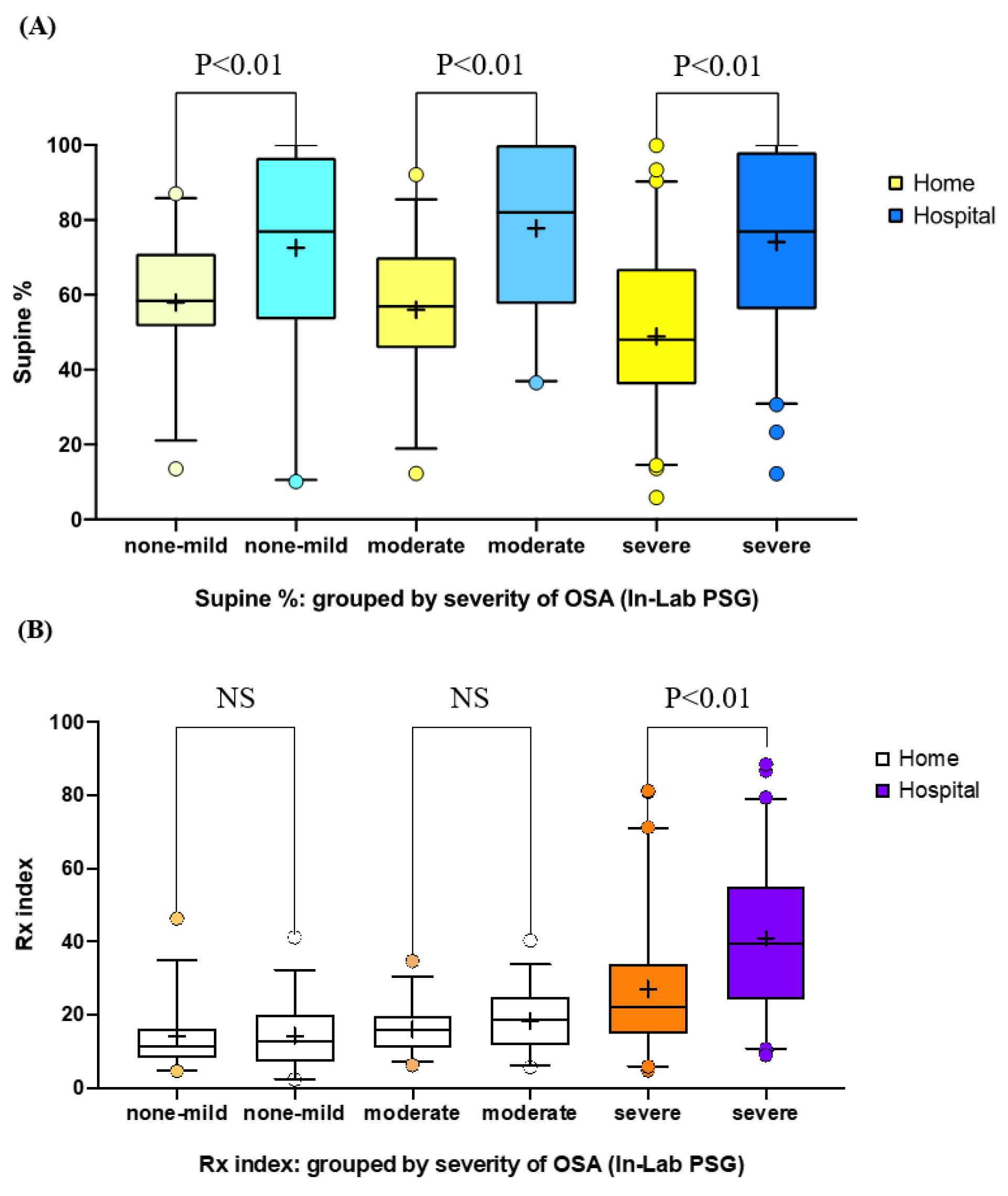
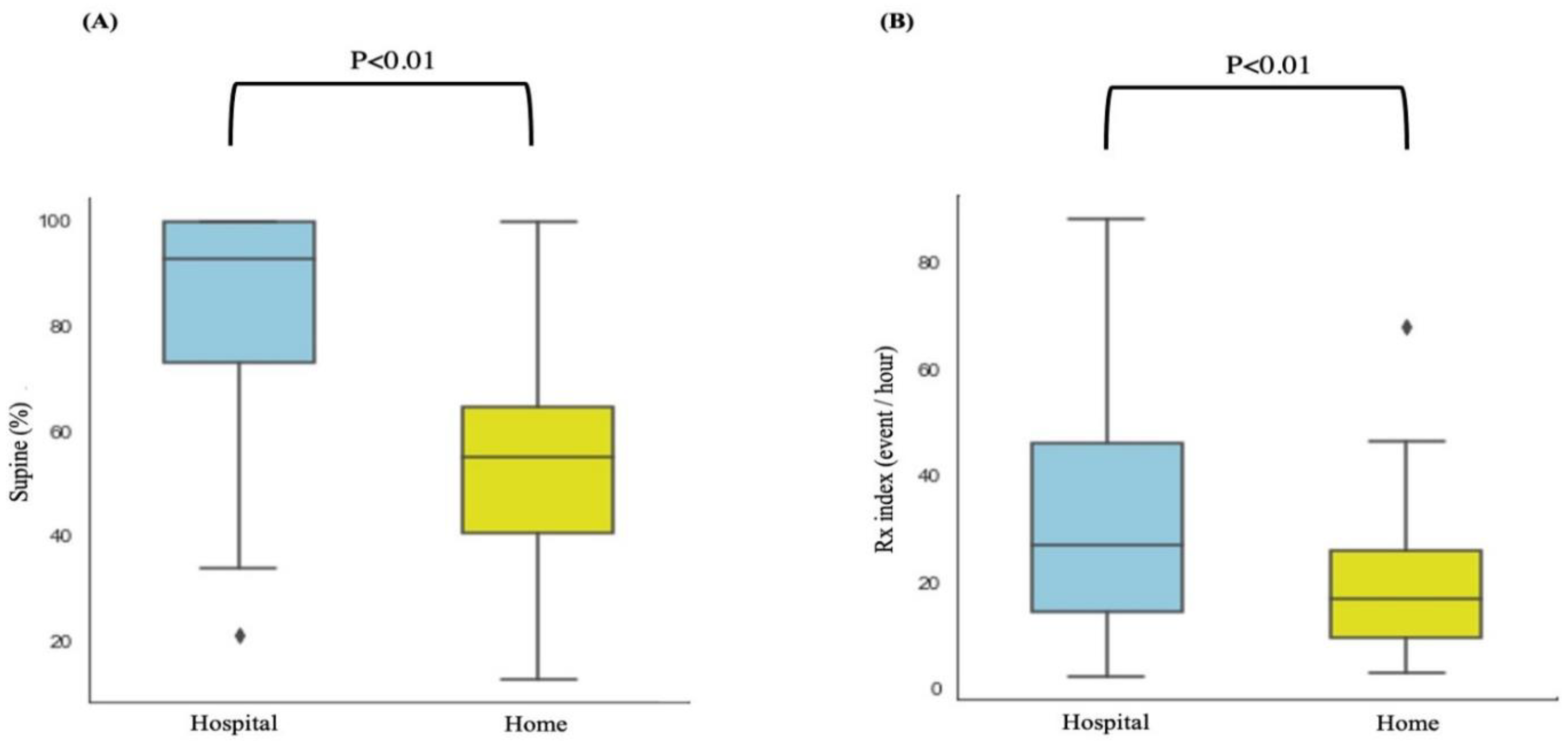
4.3. Sleeping Position and Sleep-Related Indices
4.4. Variations in Sleeping Position and Sleep-Related Indices in Patients with High Sleep Efficiency
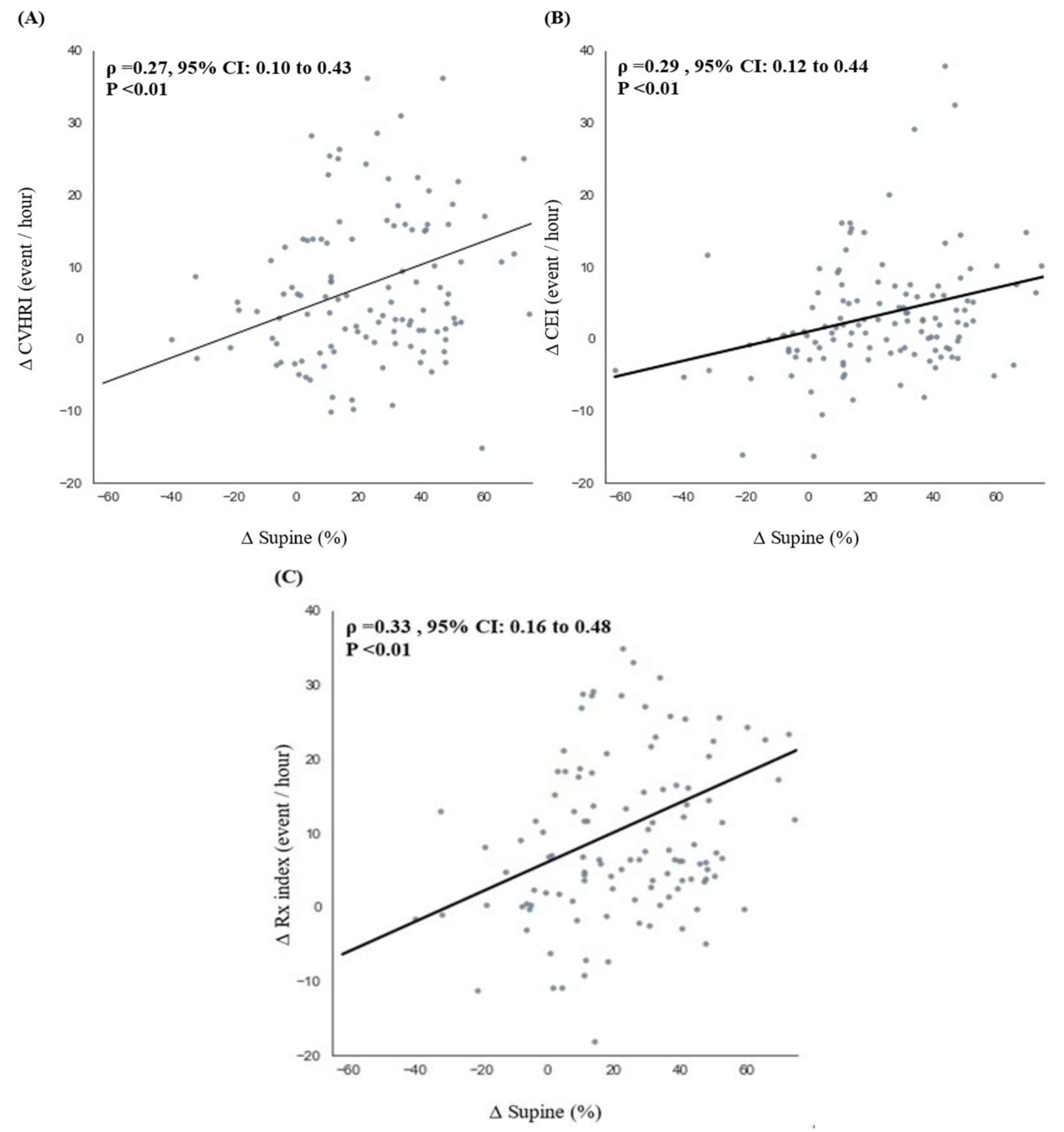
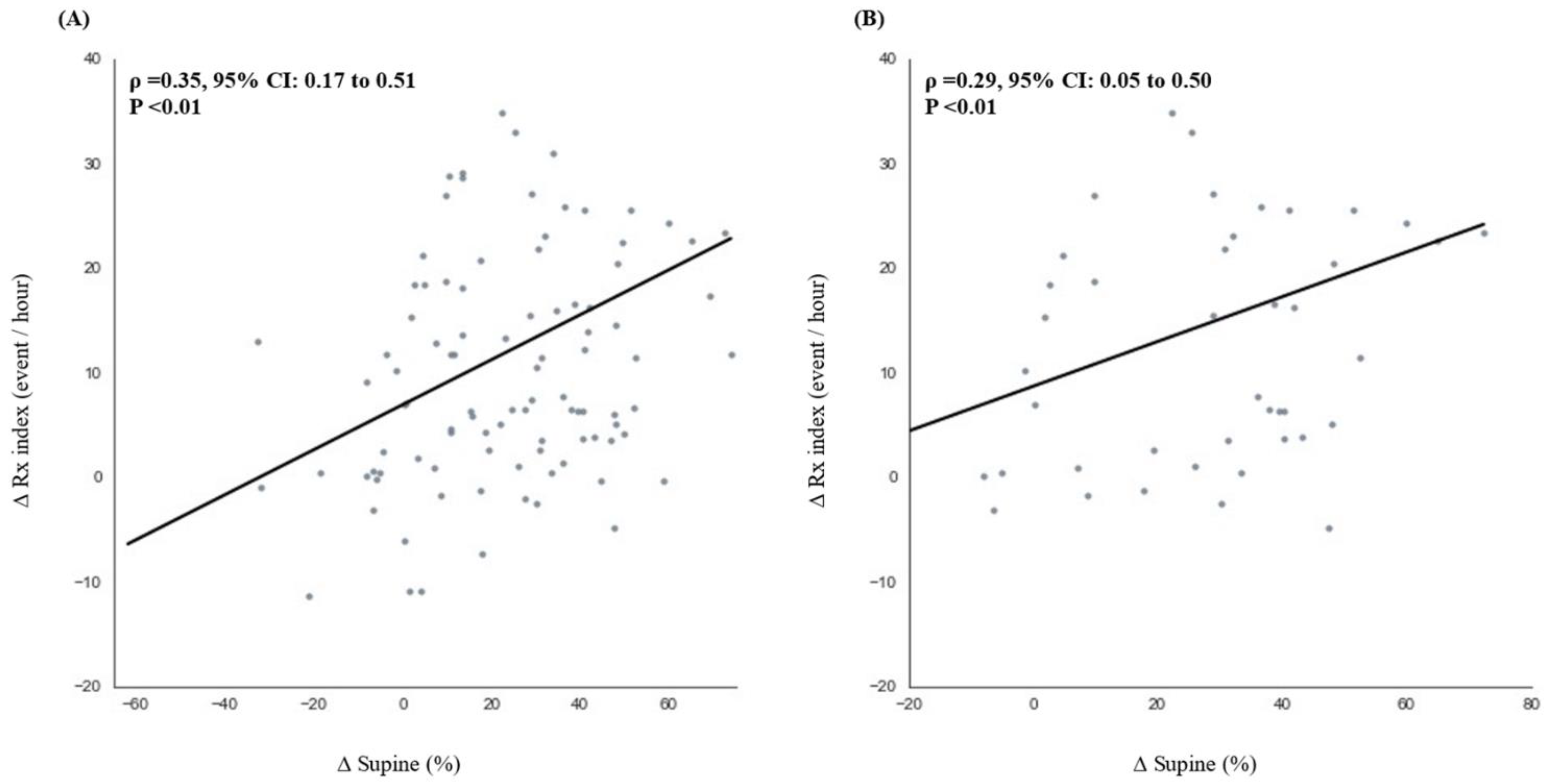
4.5. Correlations between Sleep-Related Indices and Sleeping Position in Patients with High Sleep Efficiency
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Senaratna, C.V.; Perret, J.L.; Lodge, C.J.; Lowe, A.J.; Campbell, B.E.; Matheson, M.C.; Hamilton, G.S.; Dharmage, S.C. Prevalence of obstructive sleep apnea in the general population: A systematic review. Sleep Med. Rev. 2017, 34, 70–81. [Google Scholar] [CrossRef] [PubMed]
- Sweed, R.A.; Hassan, S.; ElWahab, N.H.A.; Aref, S.R.; Mahmoud, M.I. Comorbidities associated with obstructive sleep apnea: A retrospective Egyptian study on 244 patients. Sleep Breath. 2019, 23, 1079–1085. [Google Scholar] [CrossRef] [PubMed]
- Gaig, C.; Iranzo, A. Sleep-Disordered Breathing in Neurodegenerative Diseases. Curr. Neurol. Neurosci. Rep. 2012, 12, 205–217. [Google Scholar] [CrossRef] [PubMed]
- Newell, J.; Mairesse, O.; Verbanck, P.; Neu, D. Is a one-night stay in the lab really enough to conclude? First-night effect and night-to-night variability in polysomnographic recordings among different clinical population samples. Psychiatry Res. 2012, 200, 795–801. [Google Scholar] [CrossRef]
- A Collop, N.; Anderson, W.M.; Boehlecke, B.; Claman, D.; Goldberg, R.; Gottlieb, D.J.; Hudgel, D.; Sateia, M.; Schwab, R. Clinical Guidelines for the Use of Unattended Portable Monitors in the Diagnosis of Obstructive Sleep Apnea in Adult Patients. J. Clin. Sleep Med. 2007, 3, 737–747. [Google Scholar]
- Sadeh, A.; Hauri, P.J.; Kripke, D.F.; Lavie, P. The Role of Actigraphy in the Evaluation of Sleep Disorders. Sleep 1995, 18, 288–302. [Google Scholar] [CrossRef]
- Puri, R.S.; Athanassiadis, A.; Gill, N.; Sathya, S.S.; Rathod, G.; Wahi, A.; Satat, G.; Majmudar, M.; Shah, P. Design and preliminary evaluation of a wearable device for mass-screening of sleep apnea. In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 1870–1873. [Google Scholar] [CrossRef]
- Surrel, G.; Aminifar, A.; Rincon, F.; Murali, S.; Atienza, D. Online Obstructive Sleep Apnea Detection on Medical Wearable Sensors. IEEE Trans. Biomed. Circuits Syst. 2018, 12, 762–773. [Google Scholar] [CrossRef]
- Selvaraj, N.; Narasimhan, R. Automated prediction of the apnea-hypopnea index using a wireless patch sensor. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 26–30 August 2014; pp. 1897–1900. [Google Scholar] [CrossRef]
- Bianchi, M.T.; Goparaju, B. Potential Underestimation of Sleep Apnea Severity by At-Home Kits: Rescoring In-Laboratory Polysomnography Without Sleep Staging. J. Clin. Sleep Med. 2017, 13, 551–555. [Google Scholar] [CrossRef]
- Levendowski, D.J.; Zack, N.; Rao, S.; Wong, K.K.H.; Gendreau, M.; Kranzler, J.; Zavora, T.; Westbrook, P.R. Assessment of the test–retest reliability of laboratory polysomnography. Sleep Breath. 2009, 13, 163–167. [Google Scholar] [CrossRef]
- Sunnergren, O.; Broström, A.; Svanborg, E. Positional sensitivity as a confounder in diagnosis of severity of obstructive sleep apnea. Sleep Breath. 2013, 17, 173–179. [Google Scholar] [CrossRef]
- Guilleminault, C.; Winkle, R.; Connolly, S.; Melvin, K.; Tilkian, A. Cyclical Variation of the Heart Rate in Sleep Apnoea Syndrome: Mechanisms, and Usefulness of 24 h Electrocardiography as a Screening Technique. Lancet 1984, 323, 126–131. [Google Scholar] [CrossRef]
- Hayano, J.; Watanabe, E.; Saito, Y.; Sasaki, F.; Fujimoto, K.; Nomiyama, T.; Kawai, K.; Kodama, I.; Sakakibara, H. Screening for Obstructive Sleep Apnea by Cyclic Variation of Heart Rate. Circ. Arrhythmia Electrophysiol. 2011, 4, 64–72. [Google Scholar] [CrossRef] [Green Version]
- Khandoker, A.H.; Palaniswami, M.; Karmakar, C. Support Vector Machines for Automated Recognition of Obstructive Sleep Apnea Syndrome From ECG Recordings. IEEE Trans. Inf. Technol. Biomed. 2008, 13, 37–48. [Google Scholar] [CrossRef]
- Penzel, T.; McNames, J.; De Chazal, P.; Raymond, B.; Murray, A.; Moody, G. Systematic comparison of different algorithms for apnoea detection based on electrocardiogram recordings. Med. Biol. Eng. Comput. 2002, 40, 402–407. [Google Scholar] [CrossRef]
- A Staats, B.; Bonekat, H.W.; Harris, C.D.; Offord, K.P. Chest wall motion in sleep apnea. Am. Rev. Respir. Dis. 1984, 130, 59–63. [Google Scholar] [CrossRef]
- Wang, F.-T.; Hsu, M.-H.; Fang, S.-C.; Chuang, L.-L.; Chan, H.-L. The Respiratory Fluctuation Index: A global metric of nasal airflow or thoracoabdominal wall movement time series to diagnose obstructive sleep apnea. Biomed. Signal Process. Control 2019, 49, 250–262. [Google Scholar] [CrossRef]
- Richard, W.; Kox, D.; Herder, C.D.; Laman, M.; Van Tinteren, H.; De Vries, N. The role of sleep position in obstructive sleep apnea syndrome. Eur. Arch. Oto-Rhino-Laryngol. 2006, 263, 946–950. [Google Scholar] [CrossRef]
- Oksenberg, A.; Arons, E.; Radwan, H.; Silverberg, D.S. Positional vs nonpositional obstructive sleep apnea patients: Anthropomorphic, nocturnal polysomnographic, and multiple sleep latency test data. Chest 1997, 112, 629–639. [Google Scholar] [CrossRef] [Green Version]
- Zarei, A.; Asl, B.M. Automatic Detection of Obstructive Sleep Apnea Using Wavelet Transform and Entropy-Based Features From Single-Lead ECG Signal. IEEE J. Biomed. Health Inform. 2018, 23, 1011–1021. [Google Scholar] [CrossRef]
- Gutierrez-Tobal, G.C.; Alvarez, D.; Crespo, A.; Del Campo, F.; Hornero, R. Evaluation of Machine-Learning Approaches to Estimate Sleep Apnea Severity From At-Home Oximetry Recordings. IEEE J. Biomed. Health Inform. 2018, 23, 882–892. [Google Scholar] [CrossRef] [Green Version]
- Rundo, J.V.; Downey, R. Polysomnography. Handb. Clin. Neurol. 2019, 160, 381–392. [Google Scholar] [CrossRef] [PubMed]
- Berry, R.B.; Brooks, R.; Gamaldo, C.; Harding, S.M.; Lloyd, R.M.; Quan, S.F.; Troester, M.T.; Vaughn, B.V. AASM Scoring Manual Updates for 2017 (Version 2.4). J. Clin. Sleep Med. 2017, 13, 665–666. [Google Scholar] [CrossRef] [PubMed]
- Berry, R.B.; Budhiraja, R.; Gottlieb, D.J.; Gozal, D.; Iber, C.; Kapur, V.K.; Marcus, C.L.; Mehra, R.; Parthasarathy, S.; Quan, S.F.; et al. Rules for Scoring Respiratory Events in Sleep: Update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. Deliberations of the Sleep Apnea Definitions Task Force of the American Academy of Sleep Medicine. J. Clin. Sleep Med. 2012, 8, 597–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, Y.S.; Chen, T.-Y.; Wu, D.; Lin, C.-M.; Juang, J.-N.; Liu, W.-T. Screening of obstructive sleep apnea in patients who snore using a patch-type device with electrocardiogram and 3-axis accelerometer. J. Clin. Sleep Med. 2020, 16, 1149–1160. [Google Scholar] [CrossRef]
- Kukwa, W.; Migacz, E.; Lis, T.; Ishman, S.L. The effect of in-lab polysomnography and home sleep polygraphy on sleep position. Sleep Breath. 2021, 25, 251–255. [Google Scholar] [CrossRef]
- Bignold, J.J.; Mercer, J.D.; Antic, N.A.; McEvoy, D.; Catcheside, P.G. Accurate Position Monitoring and Improved Supine-Dependent Obstructive Sleep Apnea with a New Position Recording and Supine Avoidance Device. J. Clin. Sleep Med. 2011, 7, 376–383. [Google Scholar] [CrossRef]
- Metersky, M.L.; Castriotta, R.J. The Effect of Polysomnography on Sleep Position: Possible Implications on the Diagnosis of Positional Obstructive Sleep Apnea. Respiration 1996, 63, 283–287. [Google Scholar] [CrossRef]
- Vonk, P.E.; De Vries, N.; Ravesloot, M.J.L. Polysomnography and sleep position, a Heisenberg phenomenon? HNO 2019, 67, 679–684. [Google Scholar] [CrossRef]
- Lombardi, C.; Caravita, S.; Parati, G. Central sleep apnea during continuous positive airway pressure therapy in obstructive sleep apnea patients: From the compliance to adaptation, maladaptation and reflexes. J. Thorac. Dis. 2017, 9, 4152–4156. [Google Scholar] [CrossRef]
- Permut, I.; Diaz-Abad, M.; Chatila, W.; Crocetti, J.; Gaughan, J.P.; D’Alonzo, G.E.; Krachman, S.L. Comparison of posi-tional therapy to CPAP in patients with positional obstructive sleep apnea. J. Clin. Sleep Med. 2010, 6, 238–243. [Google Scholar] [CrossRef] [Green Version]
- Karlen, W.; Floreano, D. Adaptive Sleep–Wake Discrimination for Wearable Devices. IEEE Trans. Biomed. Eng. 2010, 58, 920–926. [Google Scholar] [CrossRef] [Green Version]
- Karlen, W.; Mattiussi, C.; Floreano, D. Adaptive Sleep/Wake Classification Based on Cardiorespiratory Signals for Wearable Devices. In Proceedings of the 2007 IEEE Biomedical Circuits and Systems Conference, Montreal, QC, Canada, 27–30 November 2007; pp. 203–206. [Google Scholar] [CrossRef] [Green Version]
- Karlen, W.; Mattiussi, C.; Floreano, D. Sleep and Wake Classification With ECG and Respiratory Effort Signals. IEEE Trans. Biomed. Circuits Syst. 2009, 3, 71–78. [Google Scholar] [CrossRef] [Green Version]
- Byun, J.-H.; Kim, K.T.; Moon, H.-J.; Motamedi, G.K.; Cho, Y.W. The first night effect during polysomnography, and patients’ estimates of sleep quality. Psychiatry Res. 2019, 274, 27–29. [Google Scholar] [CrossRef]
- Choi, J.H.; Kim, E.J.; Kim, Y.S.; Choi, J.; Kim, T.H.; Kwon, S.Y.; Lee, H.M.; Lee, S.H.; Shin, C.; Lee, S.H. Validation study of portable device for the diagnosis of obstructive sleep apnea according to the new AASM scoring criteria: Watch-PAT 100. Acta Oto-Laryngol. 2010, 130, 838–843. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Categorical Variables | No-to-Mild Group (n = 33) | Moderate Group (n = 31) | Severe Group (n = 61) | p Value |
|---|---|---|---|---|
| Age (year) | 42.0 ± 11.0 | 45.3 ± 12.4 | 45.2 ± 12.8 | 0.44 a |
| Body mass index (kg/m2) | 24.4 ± 2.9 | 25.5 ± 3.7 | 28.7 ± 4.5 | <0.01 b |
| Sex (male/female) | 22/11 | 23/8 | 51/10 | 0.16 c |
| Neck circumference (cm) | 37.0 ± 2.5 | 37.5 ± 3.6 | 39.9 ± 3.4 | <0.01 b |
| Mean SpO2 (%) | 96.6 ± 1.1 | 95.9 ± 1.1 | 91.5 ± 4.4 | <0.01 b |
| Lowest SpO2 (%) | 89.3 ± 5.8 | 84.6 ± 4.5 | 75.3 ± 10.2 | <0.01 b |
| Oxygen desaturation index (≥3%, events/h) | 3.3 ± 3.9 | 8.8 ± 7.9 | 44.8 ± 23.1 | <0.01 b |
| AHI (events/h) | 8.4 ± 3.7 | 21.5 ± 4.5 | 54.0 ± 18.5 | <0.01 b |
| Variables | Group | Hospital | Home | p Value |
|---|---|---|---|---|
| CVHRI (events/h) | No-to-mild, n = 33 | 10.3 ± 8.1 | 9.3 ± 9.9 | 0.50 a |
| Moderate, n = 31 | 11.8 ± 8.5 | 10.1 ± 7.0 | 0.41 b | |
| Severe, n = 61 | 33.8 ± 21.1 | 20.4 ± 18.2 | <0.01 a | |
| CEI (events/h) | No-to-mild, n = 33 | 5.4 ± 4.4 | 5.0 ± 2.7 | 0.78 a |
| Moderate, n = 31 | 9.2 ± 4.4 | 7.6 ± 4.1 | 0.16 a | |
| Severe, n = 61 | 18.2 ± 12.2 | 13.1 ± 9.9 | <0.01 a | |
| Rx index (events/h) | No-to-mild, n = 33 | 14.2 ± 8.6 | 14.0 ± 8.6 | 0.79 a |
| Moderate, n = 31 | 18.4 ± 8.0 | 16.0 ± 6.6 | 0.20 a | |
| Severe, n = 61 | 40.9 ± 21.1 | 27.1 ± 18.4 | <0.01 a | |
| Supine sleep time (%) | No-to-mild, n = 33 | 72.5 ± 27.0 | 58.0 ± 17.9 | <0.01 a |
| Moderate, n = 31 | 77.7 ± 21.4 | 56.0 ± 18.0 | <0.01 a | |
| Severe, n = 61 | 74.1 ± 23.9 | 48.9 ± 21.9 | <0.01 a |
| Variables | Group | Hospital | Home | p Value |
|---|---|---|---|---|
| CVHRI (events/h) | No-to-mild, n = 24 | 10.14 ± 8.66 | 9.36 ± 10.36 | 0.70 a |
| Moderate, n = 24 | 12.15 ± 7.34 | 9.88 ± 6.65 | 0.27 b | |
| Severe, n = 55 | 34.39 ± 21.27 | 20.17 ± 17.89 | < 0.01 a | |
| CEI (events/h) | No-to-mild, n = 24 | 6.02 ± 4.91 | 5.10 ± 2.98 | 0.90 a |
| Moderate, n = 24 | 9.08 ± 4.65 | 7.00 ± 3.12 | 0.17 a | |
| Severe, n = 55 | 18.22 ± 11.44 | 13.58 ± 10.21 | < 0.05 a | |
| Rx index (events/h) | No-to-mild, n = 24 | 14.45 ± 9.28 | 14.06 ± 9.29 | 0.83 a |
| Moderate, n = 24 | 18.55 ± 7.22 | 15.48 ± 6.00 | 0.12 b | |
| Severe, n = 55 | 41.42 ± 21.01 | 27.16 ± 18.41 | < 0.01 a | |
| Supine sleep time (%) | No-to-mild, n = 24 | 69.40 ± 28.43 | 54.93 ± 19.26 | 0.02 a |
| Moderate, n = 24 | 80.51 ± 19.85 | 57.60 ± 17.91 | < 0.01 a | |
| Severe, n = 55 | 75.07 ± 23.81 | 48.97 ± 22.28 | < 0.01 a |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, W.-T.; Lin, S.-Y.; Tsai, C.-Y.; Liu, Y.-S.; Hsu, W.-H.; Majumdar, A.; Lin, C.-M.; Lee, K.-Y.; Wu, D.; Kuan, Y.-C.; et al. Comparison of Hospital-Based and Home-Based Obstructive Sleep Apnoea Severity Measurements with a Single-Lead Electrocardiogram Patch. Sensors 2021, 21, 8097. https://0-doi-org.brum.beds.ac.uk/10.3390/s21238097
Liu W-T, Lin S-Y, Tsai C-Y, Liu Y-S, Hsu W-H, Majumdar A, Lin C-M, Lee K-Y, Wu D, Kuan Y-C, et al. Comparison of Hospital-Based and Home-Based Obstructive Sleep Apnoea Severity Measurements with a Single-Lead Electrocardiogram Patch. Sensors. 2021; 21(23):8097. https://0-doi-org.brum.beds.ac.uk/10.3390/s21238097
Chicago/Turabian StyleLiu, Wen-Te, Shang-Yang Lin, Cheng-Yu Tsai, Yi-Shin Liu, Wen-Hua Hsu, Arnab Majumdar, Chia-Mo Lin, Kang-Yun Lee, Dean Wu, Yi-Chun Kuan, and et al. 2021. "Comparison of Hospital-Based and Home-Based Obstructive Sleep Apnoea Severity Measurements with a Single-Lead Electrocardiogram Patch" Sensors 21, no. 23: 8097. https://0-doi-org.brum.beds.ac.uk/10.3390/s21238097