
Limitations of Muscle Ultrasound Shear Wave Elastography for Clinical Routine—Positioning and Muscle Selection

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
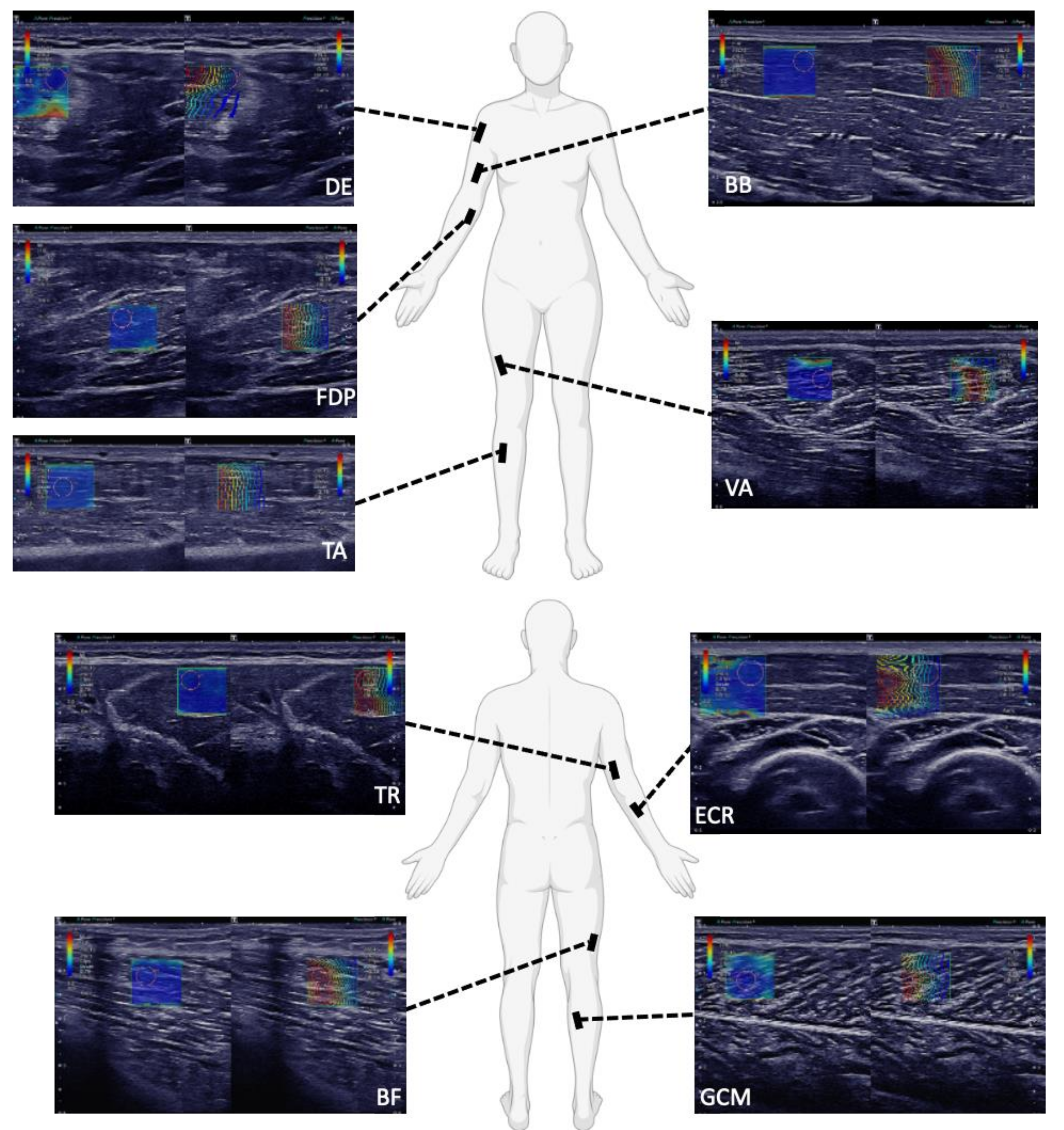
2.2. SWE Measurements and Subject Positioning
2.3. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

References
- Gennisson, J.-L.; Deffieux, T.; Fink, M.; Tanter, M. Ultrasound elastography: Principles and techniques. Diagn. Interv. Imaging 2013, 94, 487–495. [Google Scholar] [CrossRef]
- Bouillard, K.; Nordez, A.; Hug, F. Estimation of Individual Muscle Force Using Elastography. PLoS ONE 2011, 6, e29261. [Google Scholar] [CrossRef]
- Leong, H.-T.; Ng, G.Y.; Leung, V.Y.; Fu, S.N. Quantitative Estimation of Muscle Shear Elastic Modulus of the Upper Trapezius with Supersonic Shear Imaging during Arm Positioning. PLoS ONE 2013, 8, e67199. [Google Scholar] [CrossRef] [Green Version]
- Cosgrove, D.O.; Berg, W.A.; Doré, C.J.; Skyba, D.M.; Henry, J.-P.; Gay, J.; Cohen-Bacrie, C.; The BE1 Study Group. Shear wave elastography for breast masses is highly reproducible. Eur. Radiol. 2012, 22, 1023–1032. [Google Scholar] [CrossRef] [Green Version]
- Barr, R.G.; Nakashima, K.; Amy, D.; Cosgrove, D.; Farrokh, A.; Schafer, F.; Bamber, J.C.; Castera, L.; Choi, B.I.; Chou, Y.-H.; et al. WFUMB guidelines and recommendations for clinical use of ultrasound elastography: Part 2: Breast. Ultrasound Med. Biol. 2015, 41, 1148–1160. [Google Scholar] [CrossRef] [Green Version]
- Ferraioli, G.; Filice, C.; Castera, L.; Choi, B.I.; Sporea, I.; Wilson, S.R.; Cosgrove, D.; Dietrich, C.F.; Amy, D.; Bamber, J.C.; et al. WFUMB guidelines and recommendations for clinical use of ultrasound elastography: Part 3: Liver. Ultrasound Med. Biol. 2015, 41, 1161–1179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lacourpaille, L.; Hug, F.; Guével, A.; Péréon, Y.; Magot, A.; Hogrel, J.-Y.; Nordez, A. Non-invasive assessment of muscle stiffness in patients with duchenne muscular dystrophy: Short Report. Muscle Nerve 2015, 51, 284–286. [Google Scholar] [CrossRef]
- Pichiecchio, A.; Alessandrino, F.; Bortolotto, C.; Cerica, A.; Rosti, C.; Raciti, M.V.; Rossi, M.; Berardinelli, A.; Baranello, G.; Bastianello, S.; et al. Muscle ultrasound elastography and MRI in preschool children with Duchenne muscular dystrophy. Neuromuscul. Disord. 2018, 28, 476–483. [Google Scholar] [CrossRef]
- Alfuraih, A.M.; Tan, A.L.; O’Connor, P.; Emery, P.; Wakefield, R.J. The effect of ageing on shear wave elastography muscle stiffness in adults. Aging Clin. Exp. Res. 2019, 31, 1755–1763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bachasson, D.; Dubois, G.J.R.; Allenbach, Y.; Benveniste, O.; Hogrel, J.-Y. Muscle Shear Wave Elastography in Inclusion Body Myositis: Feasibility, Reliability and Relationships with Muscle Impairments. Ultrasound Med. Biol. 2018, 44, 1423–1432. [Google Scholar] [CrossRef] [PubMed]
- Kronlage, C.; Grimm, A.; Romano, A.; Stahl, J.-H.; Martin, P.; Winter, N.; Marquetand, J. Muscle Ultrasound Shear Wave Elastography as a Non-Invasive Biomarker in Myotonia. Diagnostics 2021, 11, 163. [Google Scholar] [CrossRef] [PubMed]
- Gennisson, J.-L.; Deffieux, T.; Macé, E.; Montaldo, G.; Fink, M.; Tanter, M. Viscoelastic and Anisotropic Mechanical Properties of in vivo Muscle Tissue Assessed by Supersonic Shear Imaging. Ultrasound Med. Biol. 2010, 36, 789–801. [Google Scholar] [CrossRef]
- Alfuraih, A.M.; O’Connor, P.; Tan, A.L.; Hensor, E.; Emery, P.; Wakefield, R.J. An investigation into the variability between different shear wave elastography systems in muscle. Med. Ultrason. 2017, 19, 392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alfuraih, A.M.; O’Connor, P.; Hensor, E.; Tan, A.L.; Emery, P.; Wakefield, R.J. The effect of unit, depth, and probe load on the reliability of muscle shear wave elastography: Variables affecting reliability of SWE. J. Clin. Ultrasound 2018, 46, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Bernabei, M.; Lee, S.S.M.; Perreault, E.J.; Sandercock, T.G. Shear wave velocity is sensitive to changes in muscle stiffness that occur independently from changes in force. J. Appl. Physiol. 2020, 128, 8–16. [Google Scholar] [CrossRef]
- Crutison, J.; Klatt, D.; Sandercock, T.G.; Perreault, E.J.; Royston, T. Muscle elastography: Stress versus stiffness. J. Acoust. Soc. Am. 2021, 150, A287. [Google Scholar] [CrossRef]
- Jenkyn, T.R.; Ehman, R.L.; An, K.-N. Noninvasive muscle tension measurement using the novel technique of magnetic resonance elastography (MRE). J. Biomech. 2003, 36, 1917–1921. [Google Scholar] [CrossRef]
- Zonnino, A.; Smith, D.R.; Delgorio, P.L.; Johnson, C.L.; Sergi, F. MM-MRE: A new technique to quantify individual muscle forces during isometric tasks of the wrist using MR elastography. IEEE Int. Conf. Rehabil. Robot. Proc. 2019, 2019, 270–275. [Google Scholar] [CrossRef]
- Săftoiu, A.; Gilja, O.H.; Sidhu, P.S.; Dietrich, C.F.; Cantisani, V.; Amy, D.; Bachmann-Nielsen, M.; Bob, F.; Bojunga, J.; Brock, M.; et al. The EFSUMB Guidelines and Recommendations for the Clinical Practice of Elastography in Non-Hepatic Applications: Update 2018. Ultraschall Med.-Eur. J. Ultrasound 2019, 40, 425–453. [Google Scholar] [CrossRef] [Green Version]
- Lacourpaille, L.; Hug, F.; Bouillard, K.; Hogrel, J.-Y.; Nordez, A. Supersonic shear imaging provides a reliable measurement of resting muscle shear elastic modulus. Physiol. Meas. 2012, 33, N19–N28. [Google Scholar] [CrossRef]
- Dubois, G.; Kheireddine, W.; Vergari, C.; Bonneau, D.; Thoreux, P.; Rouch, P.; Tanter, M.; Gennisson, J.-L.; Skalli, W. Reliable Protocol for Shear Wave Elastography of Lower Limb Muscles at Rest and During Passive Stretching. Ultrasound Med. Biol. 2015, 41, 2284–2291. [Google Scholar] [CrossRef] [Green Version]
- Sigrist, R.M.S.; Liau, J.; Kaffas, A.E.; Chammas, M.C.; Willmann, J.K. Ultrasound Elastography: Review of Techniques and Clinical Applications. Theranostics 2017, 7, 1303–1329. [Google Scholar] [CrossRef]
- Zaidman, C.M.; van Alfen, N. Ultrasound in the Assessment of Myopathic Disorders. J. Clin. Neurophysiol. 2016, 33, 103–111. [Google Scholar] [CrossRef]
- Alfuraih, A.M.; O’Connor, P.; Tan, A.L.; Hensor, E.M.A.; Ladas, A.; Emery, P.; Wakefield, R.J. Muscle shear wave elastography in idiopathic inflammatory myopathies: A case-control study with MRI correlation. Skeletal Radiol. 2019, 48, 1209–1219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paramalingam, S.; Needham, M.; Raymond, W.; Mastaglia, F.; Lightowler, D.; Morin, N.; Counsel, P.; Keen, H.I. Muscle shear wave elastography, conventional B mode and power doppler ultrasonography in healthy adults and patients with autoimmune inflammatory myopathies: A pilot cross-sectional study. BMC Musculoskelet. Disord. 2021, 22, 537. [Google Scholar] [CrossRef]
- Maïsetti, O.; Hug, F.; Bouillard, K.; Nordez, A. Characterization of passive elastic properties of the human medial gastrocnemius muscle belly using supersonic shear imaging. J. Biomech. 2012, 45, 978–984. [Google Scholar] [CrossRef]
- Koo, T.K.; Guo, J.-Y.; Cohen, J.H.; Parker, K.J. Relationship between shear elastic modulus and passive muscle force: An ex-vivo study. J. Biomech. 2013, 46, 2053–2059. [Google Scholar] [CrossRef] [PubMed]
- Koo, T.K.; Guo, J.-Y.; Cohen, J.H.; Parker, K.J. Quantifying the passive stretching response of human tibialis anterior muscle using shear wave elastography. Clin. Biomech. 2014, 29, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Hug, F.; Tucker, K.; Gennisson, J.-L.; Tanter, M.; Nordez, A. Elastography for Muscle Biomechanics: Toward the Estimation of Individual Muscle Force. Exerc. Sport Sci. Rev. 2015, 43, 125–133. [Google Scholar] [CrossRef]
- Eby, S.F.; Cloud, B.A.; Brandenburg, J.E.; Giambini, H.; Song, P.; Chen, S.; LeBrasseur, N.K.; An, K.-N. Shear wave elastography of passive skeletal muscle stiffness: Influences of sex and age throughout adulthood. Clin. Biomech. 2015, 30, 22–27. [Google Scholar] [CrossRef] [Green Version]
- Šarabon, N.; Kozinc, Ž.; Podrekar, N. Using shear-wave elastography in skeletal muscle: A repeatability and reproducibility study on biceps femoris muscle. PLoS ONE 2019, 14, e0222008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, J.; He, W.; Du, L.-J.; Chen, J.; Park, D.; Wells, M.; Fowlkes, B.; O’Dell, M. Quantitative Ultrasound Imaging to Assess the Biceps Brachii Muscle in Chronic Post-Stroke Spasticity: Preliminary Observation. Ultrasound Med. Biol. 2018, 44, 1931–1940. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ewertsen, C.; Carlsen, J.F.; Christiansen, I.R.; Jensen, J.A.; Nielsen, M.B. Evaluation of healthy muscle tissue by strain and shear wave elastography—Dependency on depth and ROI position in relation to underlying bone. Ultrasonics 2016, 71, 127–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
| Summary of Participants’ Characteristics | |||||
|---|---|---|---|---|---|
| Protocol | Age in Years Mean (SD) | Height in cm Mean (SD) | Weight in kg Mean (SD) | BMI in kg/m2 Mean (SD) | Number of Participants Male, Female |
| Protocol 1 (Clinical Feasibility) | 33.0 (13.3) | 177.0 (8.8) | 72.7 (11.7) | 23.1 (2.5) | 17, 8 |
| Protocol 2 (Optimized, Rigid SWE-Protocol) | 26.5 (3.1) | 176.0 (7.6) | 67.4 (10.1) | 21.7 (2.2) | 15, 12 |
| p | 0.032 * | 0.640 | 0.113 | 0.058 | 0.361 |
| Joint Position | ||||||||
| Muscle | This Study (Protocol 2) | Alfuraih et al. (2018 & 2019) | Ewertsen et al. (2016) | Carpenter et al. (2015) | Akagi et al. (2015) | Cortez et al. (2017) | Lacourpaille et al. (2012) | Dubois et al. (2015) |
|---|---|---|---|---|---|---|---|---|
| DE | Supine, elbow resting on a pillow, arm bent at the elbow 90° | |||||||
| BB | Supine, elbow resting on a pillow, arm bent at the elbow 90° | Supine, elbow resting on a pillow, arm bent at the elbow 90° | Sitting, forearm resting, supinated underarm | Arm bent at the elbow 90° | Prone, 90° bent between legs and thighs | |||
| ECR | Supine, elbow resting on a pillow, arm bent at the elbow 90° | |||||||
| FDP | Supine, arm stretched out | |||||||
| TR | Left lateral recumbent | Arm at full extension | ||||||
| VA | Supine, legs almost completely stretched out with a small pillow under the knees | Supine, knees fully extended and feet slightly everted | Prone, lower extremity fully supported | Knee fully extended | Sitting upright, hip bent at 90° | |||
| BF | Sitting, feet flat on the floor | Prone, bent knees (90°), legs rested against a wall | ||||||
| TA | Sitting, lower leg free hanging | Supine, leg extended and heel on the examination table | Knee fully extended, ankle in neutral position | |||||
| GCM or GCL | Sitting, lower leg free hanging | Prone, feet relaxed, hanging from bed | Prone, lower extremity fully supported | Prone, hip and knee at ~ 0°, ankle at 20° plantar flexion | Supine, knee flexed and hip in external rotation | Knee bent at 90°, ankle in neutral position | Prone, 90° bent between legs and thighs | |
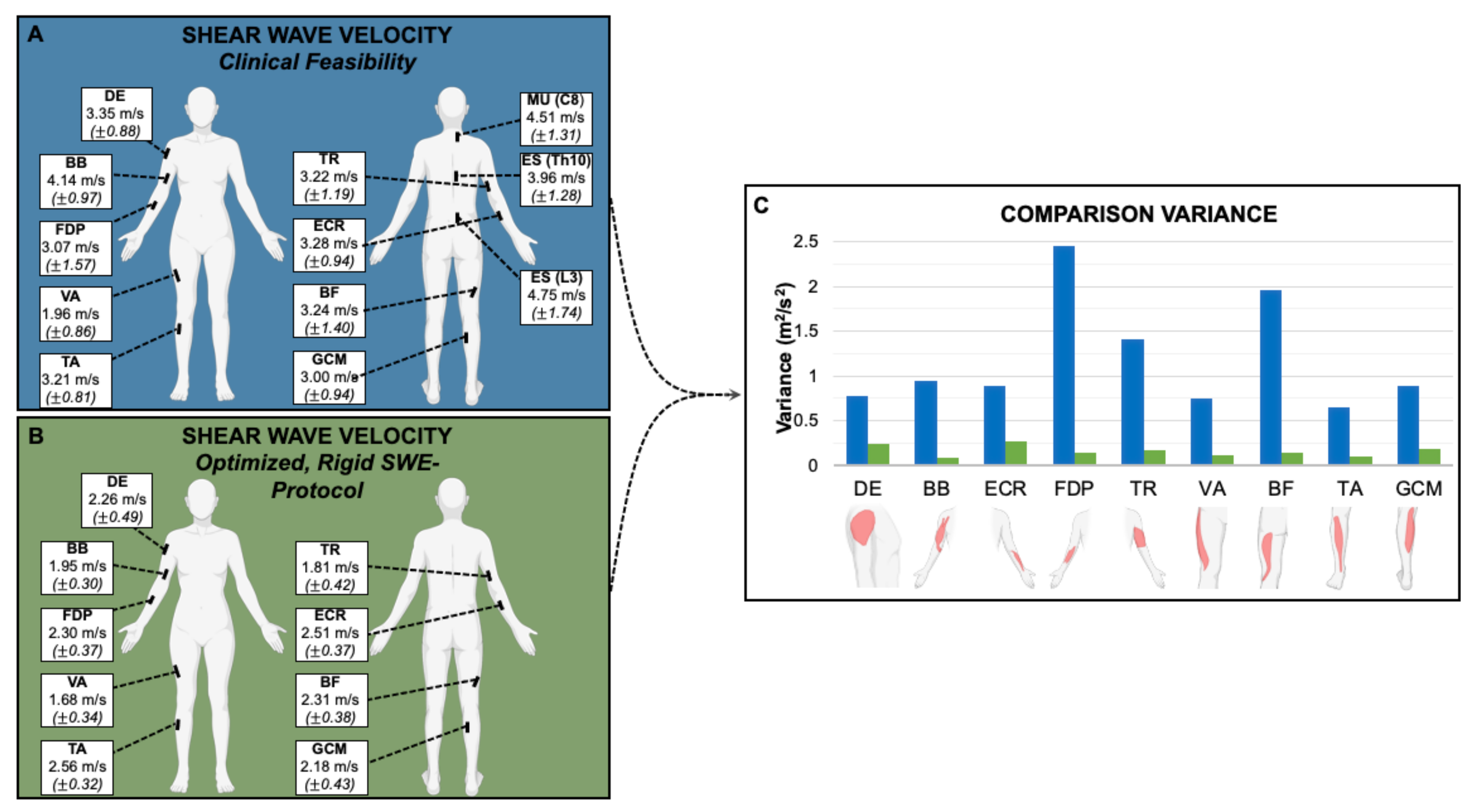
| Muscle | Protocol 1 (Clinical Feasibility) n = 25 | Protocol 2 (Optimized, Rigid SWE-Protocol) n = 27 | p |
|---|---|---|---|
| SWE m/s (SD) | SWE m/s (SD) | ||
| DE | 3.35 (0.88) | 2.26 (0.49) | <0.001 |
| BB | 4.14 (0.97) | 1.95 (0.30) | <0.001 |
| ECR | 3.28 (0.94) | 2.51 (0.37) | <0.001 |
| FDP | 3.07 (1.57) | 2.30 (0.37) | 0.001 |
| TR | 3.22 (1.19) | 1.81 (0.42) | <0.001 |
| MU (C8) | 4.51 (1.31) | ||
| ES (Th10) | 3.96 (1.28) | ||
| ES (L3) | 4.75 (1.74) | ||
| VA | 1.96 (0.86) | 1.68 (0.34) | 0.098 |
| BF | 3.24 (1.40) | 2.31 (0.38) | <0.001 |
| TA | 3.21 (0.81) | 2.56 (0.32) | <0.001 |
| GCM | 3.00 (0.94) | 2.18 (0.43) | <0.001 |
| Average | 3.74 (1.15) | 2.17 (0.38) | 0.001 |
| Author | This Study (Protocol 2) | Alfuraih et al. 2018 | Alfuraih et al. 2019 | Ewertsen et al. 2016 ^ | Carpenter et al. 2015 * | Akagi et al. 2015 # | Cortez et al. 2017 |
|---|---|---|---|---|---|---|---|
| Cohort | n = 27 | n = 20 | n = 26 | n = 10 | n = 5 | n = 31 | n = 16 |
| Age in years mean (SD) | 26.5 (3.1) | 36.7 (11.8) | 28.1 (4.1) | Median: 32.5 | Range: 27–33 | 22 (1) | 25 (12) |
| BMI in kg/m2 mean (SD) | 21.7 (2.2) | 23.0 (3.1) | 24.5 (5.3) | All < 31 | Not given | 21.5 | 23.2 (2.97) |
| Device and Probe | Canon Aplio i800, PLI 1205 BX/i18Lx5 probe | General Electric LOGIQ-E9 System, linear 9- to 5-MHz probe | Two-dimensional Aixplorer, SuperLinearTM SL10-2 MHz probe | Acuson S3000 Helx, linear array probe (9L4) or low frequency, curved array probe (4C1) | Siemens S3000 Unit, 9-MHz linear transducer | Acuson S2000, electronic linear array probe (9L4 Transducer) 4–9 MHz | Supersonic Shear Imaging Module, SL15-4 high frequency linear probe |
| Muscle | SWE m/s (SD) | SWE m/s (SD) | SWE m/s (SD) | SWE m/s (SD) | SWE m/s (SD) | SWE m/s (SD) | SWE m/s (SD) |
| DE | 2.26 (0.49) | ||||||
| BB | 1.95 (0.30) | 1.76 (0.10) | 1.95 (0.22) | 2.22 (0.64) | |||
| ECR | 2.51 (0.37) | ||||||
| FDP | 2.30 (0.37) | ||||||
| TR | 3.22 (1.19) | ||||||
| VA | 1.68 (0.34) | 1.76 (0.10) | 1.77 (0.15) | 4.52 (1.49) | |||
| BF | 2.31 (0.38) | 1.54 (0.12) | 1.73 (0.12) | ||||
| TA | 2.56 (0.32) | 3.49 (0.58) & 3.86 (0.46) | |||||
| GCM | 2.18 (0.43) | 1.77 (0.79) | 1.89 (0.32) & 2.38 (0.58) | ||||
| GCL | 1.77 (0.79) | 4.34 (1.56) | 1.63 (0.99) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romano, A.; Staber, D.; Grimm, A.; Kronlage, C.; Marquetand, J. Limitations of Muscle Ultrasound Shear Wave Elastography for Clinical Routine—Positioning and Muscle Selection. Sensors 2021, 21, 8490. https://0-doi-org.brum.beds.ac.uk/10.3390/s21248490
Romano A, Staber D, Grimm A, Kronlage C, Marquetand J. Limitations of Muscle Ultrasound Shear Wave Elastography for Clinical Routine—Positioning and Muscle Selection. Sensors. 2021; 21(24):8490. https://0-doi-org.brum.beds.ac.uk/10.3390/s21248490
Chicago/Turabian StyleRomano, Alyssa, Deborah Staber, Alexander Grimm, Cornelius Kronlage, and Justus Marquetand. 2021. "Limitations of Muscle Ultrasound Shear Wave Elastography for Clinical Routine—Positioning and Muscle Selection" Sensors 21, no. 24: 8490. https://0-doi-org.brum.beds.ac.uk/10.3390/s21248490