Non-Contact Measurements of Electrocardiogram and Cough-Associated Electromyogram from the Neck Using In-Pillow Common Cloth Electrodes: A Proof-of-Concept Study


Abstract
:1. Introduction
2. Materials and Methods
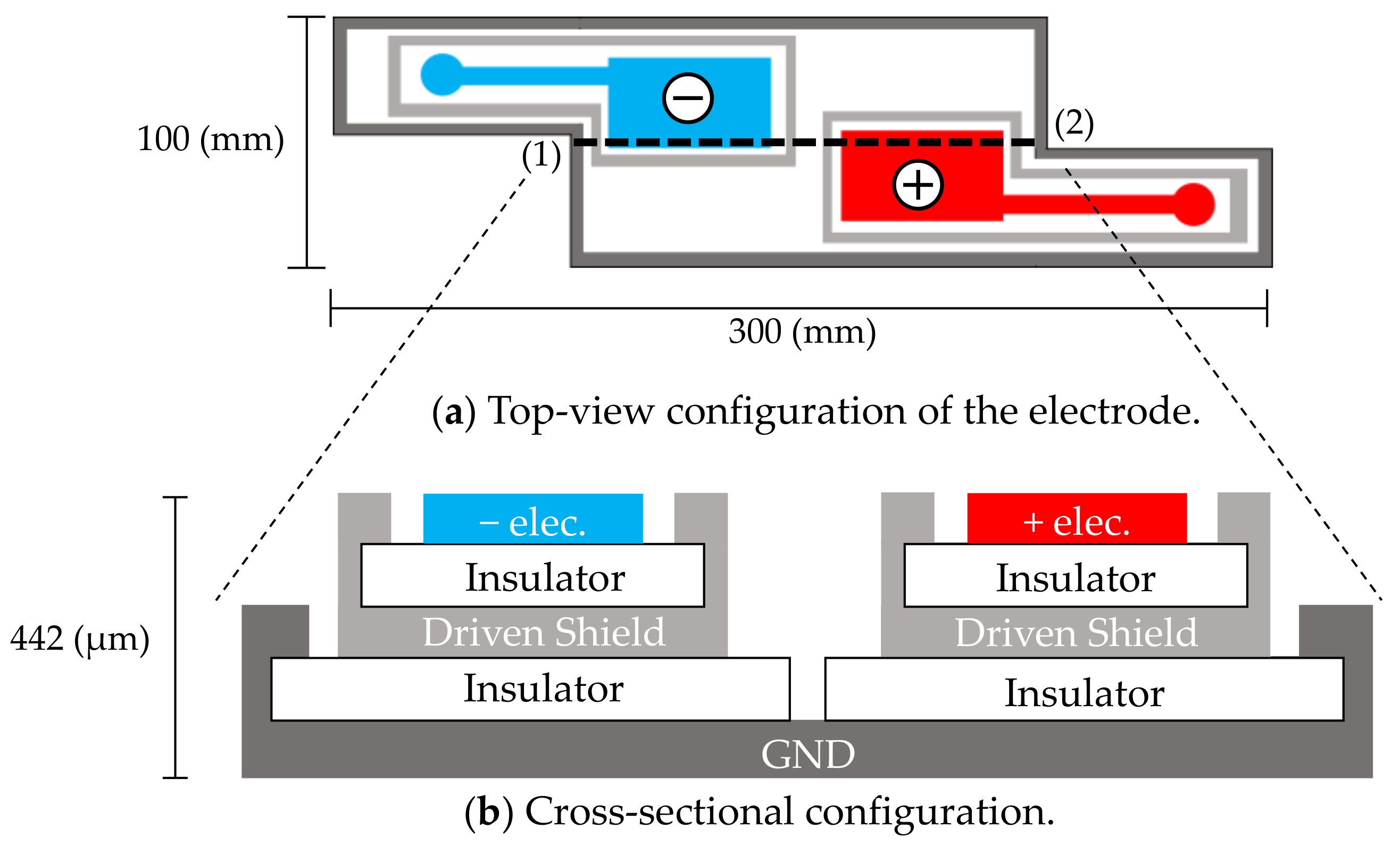
2.1. In-Pillow Cloth Electrodes
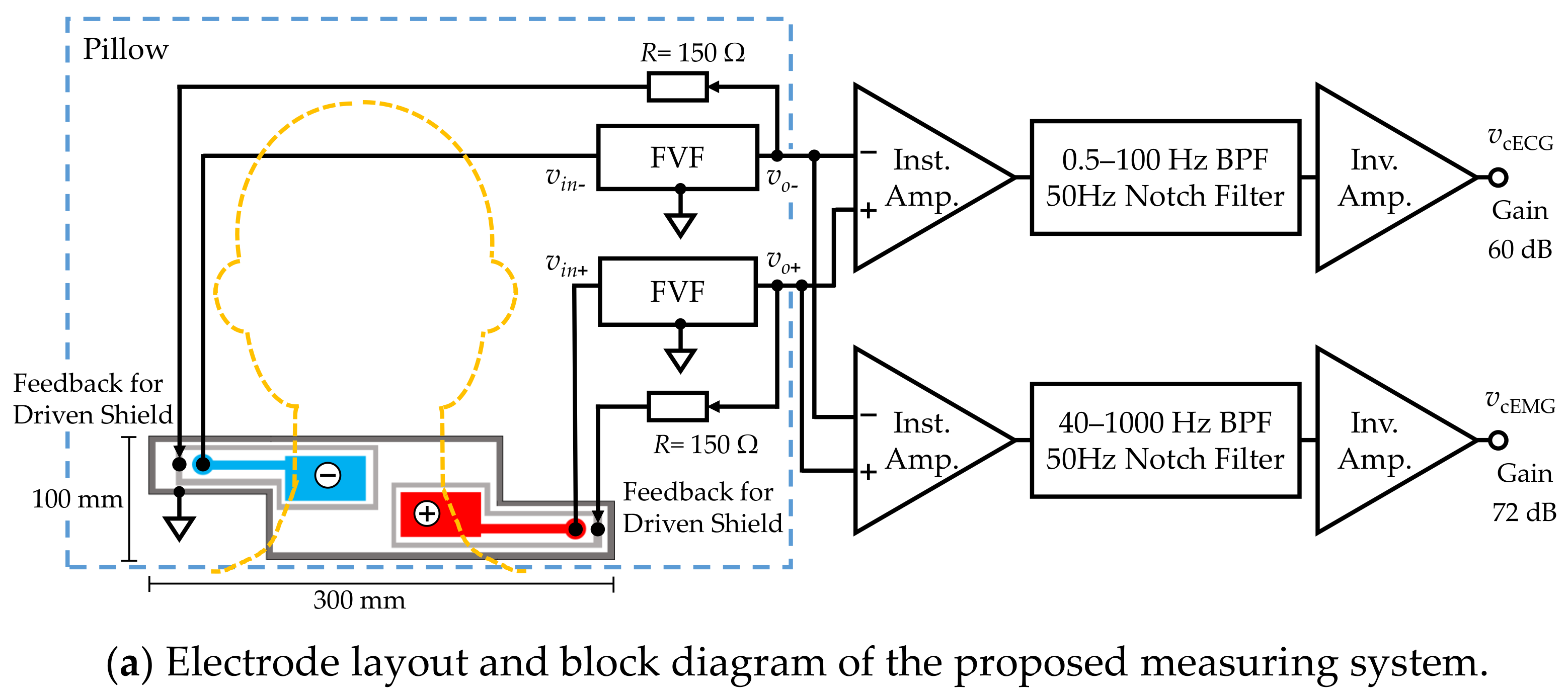
2.2. Measurement System
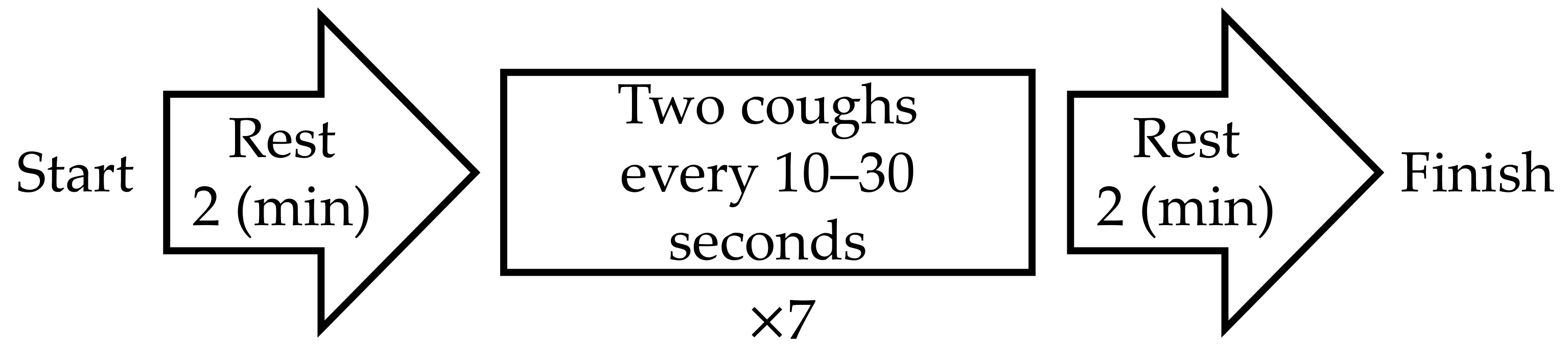
2.3. Experimental Methods
2.4. Analytical Metheds
2.4.1. Analysis of ECG Signals
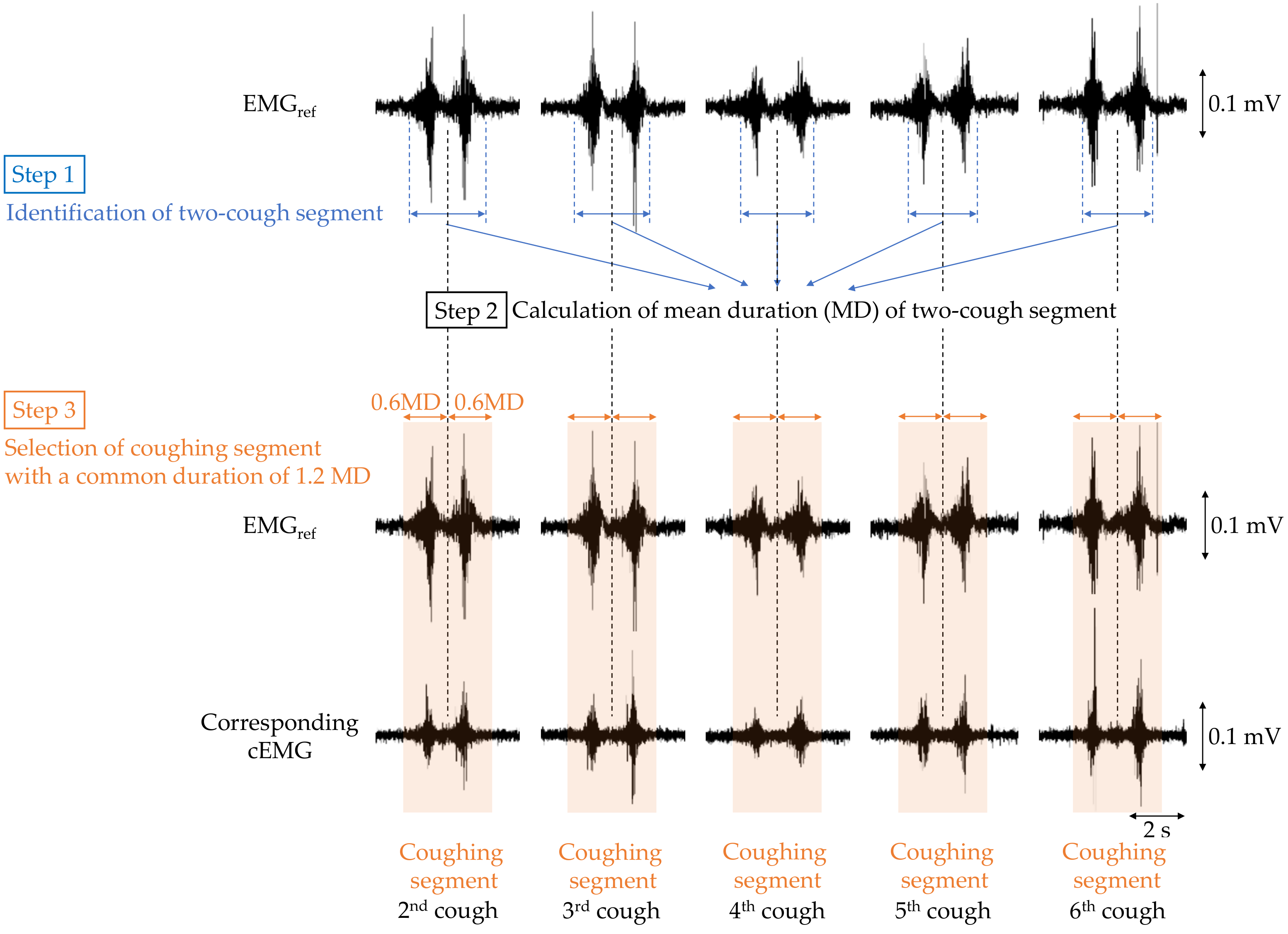
2.4.2. Analysis of EMG Signals
3. Results
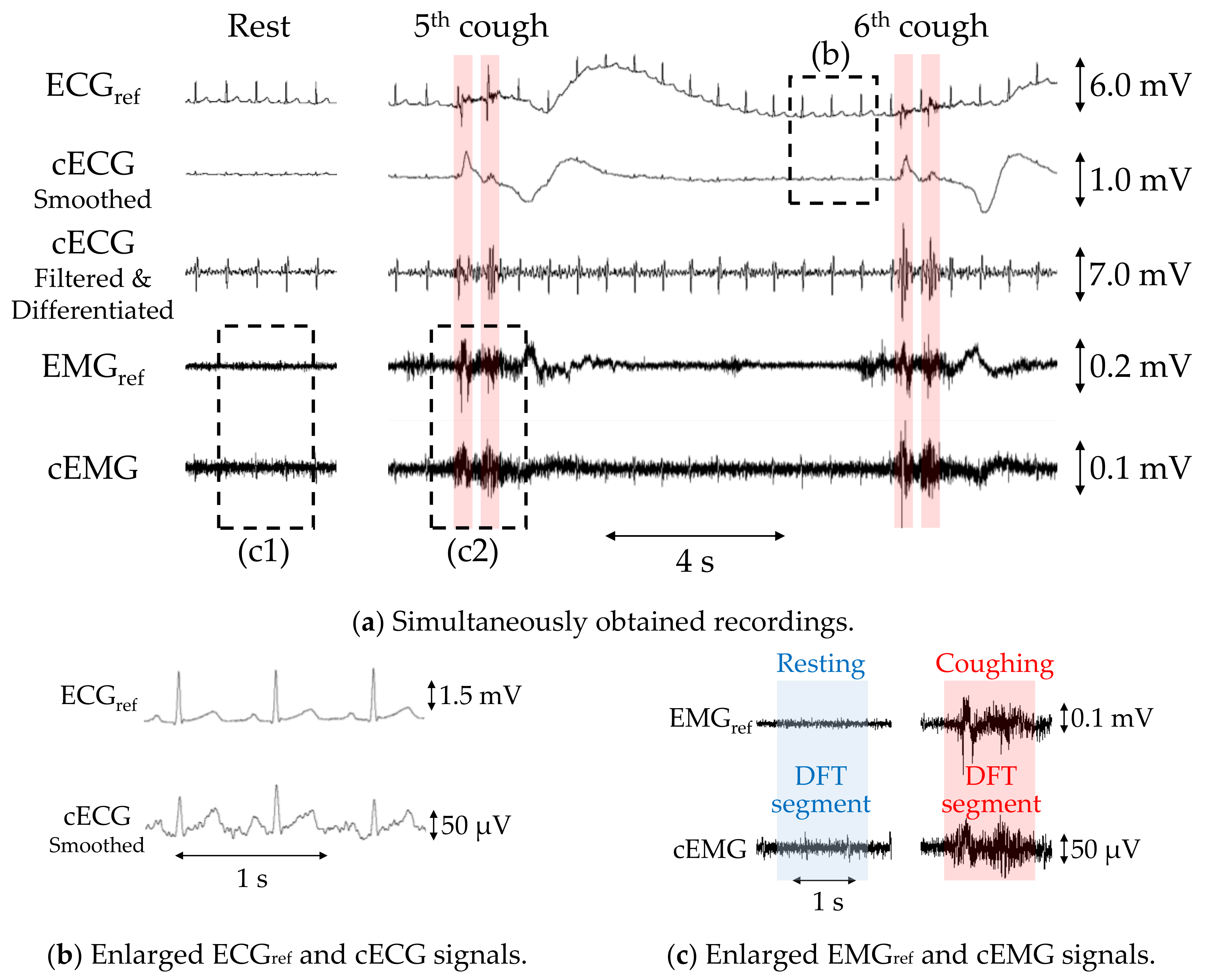
3.1. Simultaneous Measurements of cECG and Cough-Associated cEMG
3.2. Evaluation of cECG and cEMG Signals Measured in the Proposed System
3.2.1. Evaluation of cECG Signals
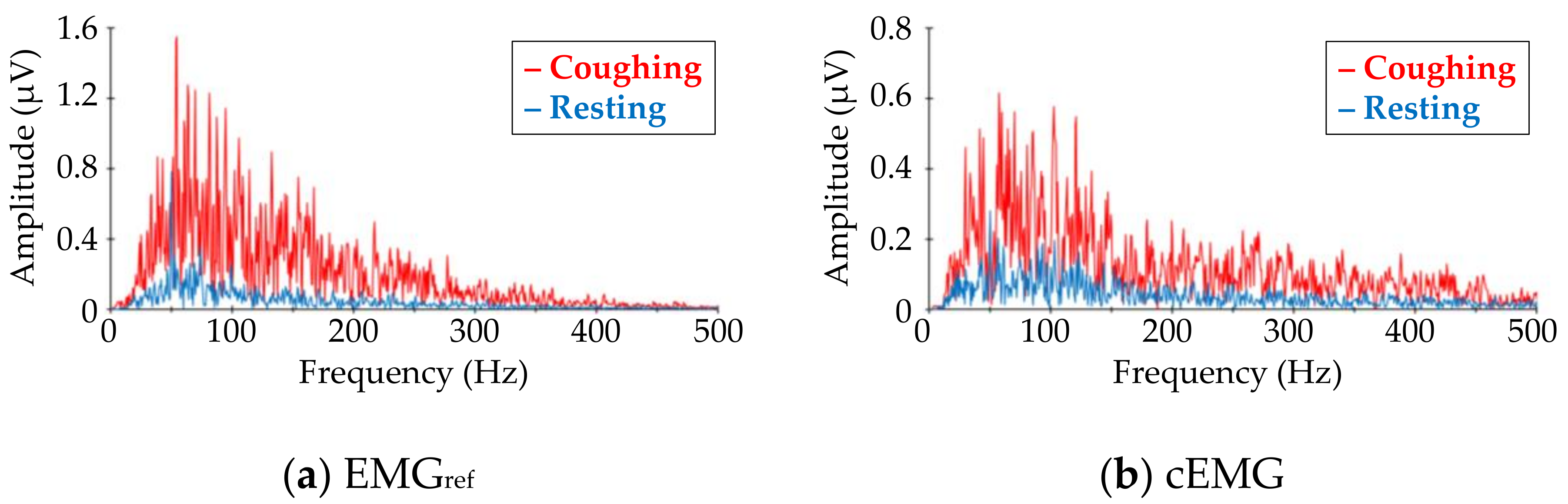
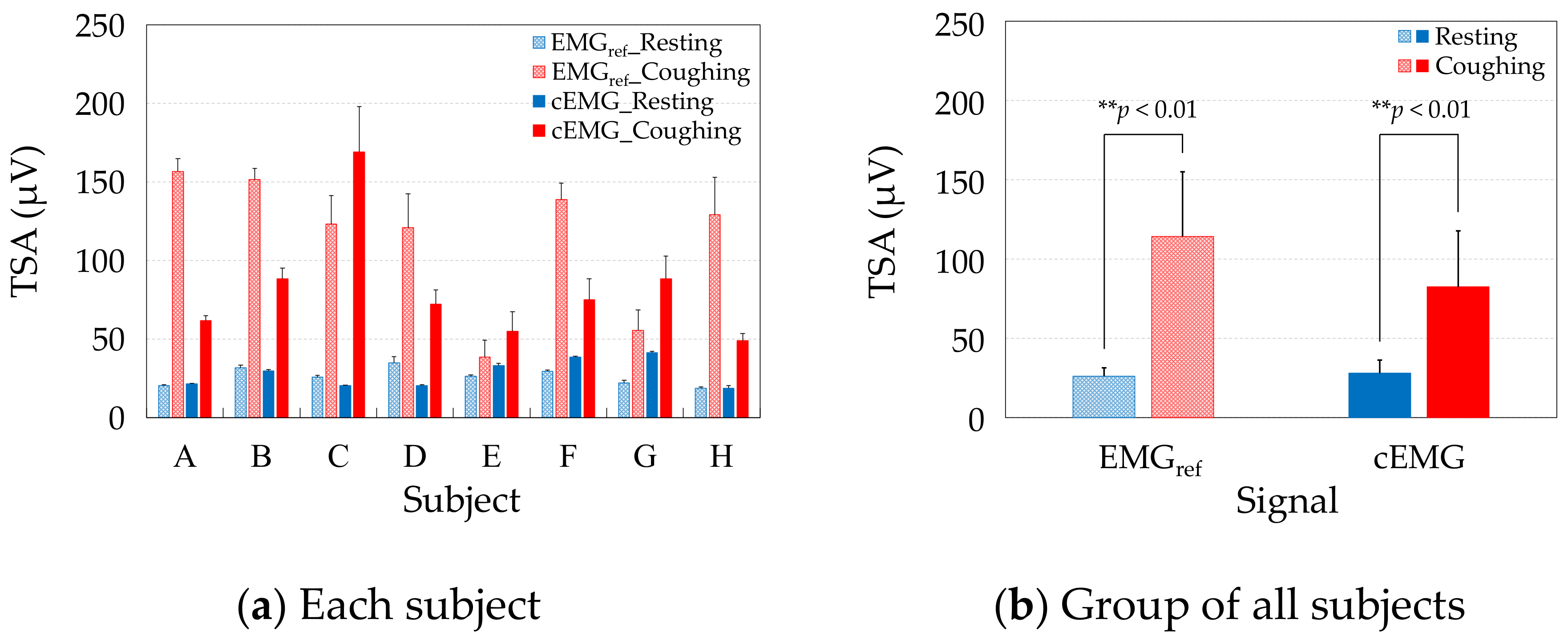
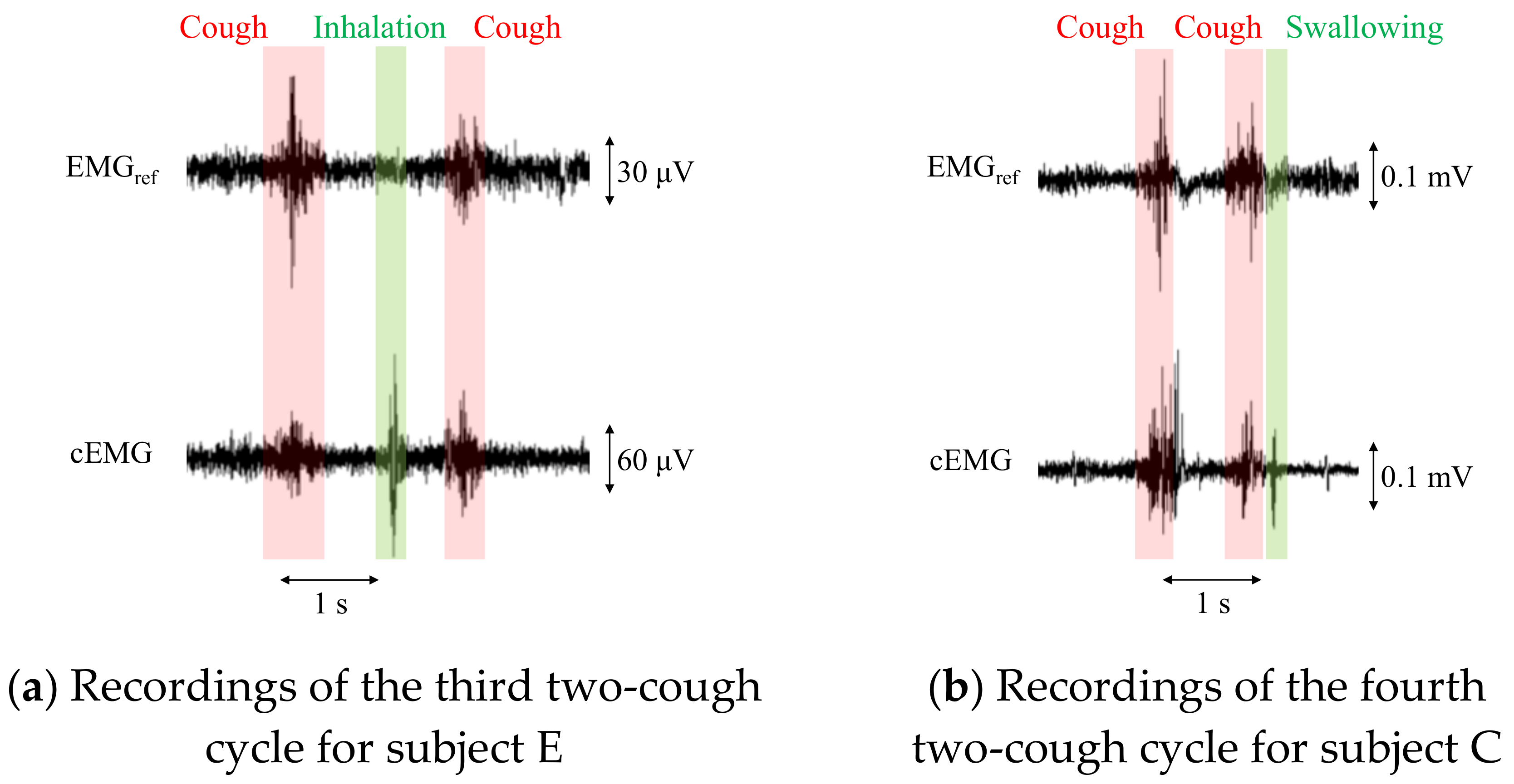
3.2.2. Evaluation of cEMG Signals
4. Discussions
4.1. Advantages of the Adopted Electrode Configuration and Novel FVF
4.2. Comparison of Heart Rate Variability between the Proposed and Commercial Systems
4.3. Challenges to Be Tackled
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Schappert, S.M. National ambulatory medical care survey: 1991 summary. Vital Health Stat13 1993, 116, 1–20. [Google Scholar]
- Irwin, R.S.; Boulet, L.P.; Cloutier, M.M.; Fuller, R.; Gold, P.M.; Hoffstein, V.; Ing, A.J.; McCool, F.D.; O’Byrne, P.; Poe, R.H.; et al. Managing cough as a defense mechanism and as a symptom. A consensus panel report of the American College of Chest Physicians. Chest 1998, 114, 133S–181S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kono, S. Prolusion. In Clinical Practice Guidelines: Cough, 2nd ed.; The Japanese Respiratory Society: Tokyo, Japan, 2012; pp. 2–3, (In Japanese). Available online: https://www.jrs.or.jp/uploads/uploads/files/photos/1048.pdf (accessed on 4 November 2020).
- Brooke, A.M.; Lambert, P.C.; Burton, P.R.; Clarke, C.; Luyt, D.K.; Simpson, H. Night cough in a population-based sample of children: Characteristics, relation to symptoms and associations with measures of asthma severity. Eur. Respir. J. 1996, 9, 65–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bentur, L.; Beck, R.; Shinawi, M.; Naveh, T.; Gavriely, N. Wheeze monitoring in children for assessment of nocturnal asthma and response to therapy. Eur. Respir. J. 2003, 21, 621–626. [Google Scholar] [CrossRef] [Green Version]
- Omachi, T.A.; Blanc, P.D.; Claman, D.M.; Chen, H.; Yelin, E.H.; Julian, L.; Katz, P.P. Disturbed sleep among COPD patients is longitudinally associated with mortality and adverse COPD outcomes. Sleep Med. 2012, 13, 476–483. [Google Scholar] [CrossRef] [Green Version]
- Stephenson, J.J.; Cai, Q.; Mocarski, M.; Tan, H.; Doshi, J.A.; Sullivan, S.D. Impact and factors associated with nighttime and early morning symptoms among patients with chronic obstructive pulmonary disease. Int. J. Chron. Obstruct. Pulmon. Dis. 2015, 10, 577–586. [Google Scholar] [CrossRef] [Green Version]
- Ding, B.; Small, M.; Bergström, G.; Holmgren, U. A cross-sectional survey of night-time symptoms and impact of sleep disturbance on symptoms and health status in patients with COPD. Int. J. Chron. Obstruct. Pulmon. Dis. 2017, 12, 589–599. [Google Scholar] [CrossRef] [Green Version]
- Birring, S.S.; Ing, A.J.; Chan, K.; Cossa, G.; Matos, S.; Morgan, M.D.L.; Pavord, I.D. Obstructive sleep apnoea: A cause of chronic cough. Cough 2007, 3, 7. [Google Scholar] [CrossRef] [Green Version]
- Chan, K.K.Y.; Ing, A.J.; Laks, L.; Cossa, G.; Rogers, P.; Birring, S.S. Chronic cough in patients with sleep-disordered breathing. Eur. Respir. J. 2010, 35, 368–372. [Google Scholar] [CrossRef] [Green Version]
- Chan, K.; Ing, A.; Birring, S.S. Cough in obstructive sleep apnoea. Pulm. Pharmacol. Ther. 2015, 35, 129–131. [Google Scholar] [CrossRef]
- Gaude, G.S. Pulmonary manifestations of gastroesophageal reflux disease. Ann. Thorac. Med. 2009, 4, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Emilsson, Ö.I.; Bengtsson, A.; Franklin, K.A.; Torén, K.; Benediktsdóttir, B.; Farkhooy, A.; Weyler, J.; Dom, S.; Backer, W.D.; Gislason, T.; et al. Nocturnal gastro-oesophageal reflux, asthma and symptoms of OSA: A longitudinal, general population study. Eur. Respir. J. 2013, 41, 1347–1354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cochrane, G.M.; Clark, J.H. A survey of asthma mortality in patients between ages 35 and 64 in the Greater London hospitals in 1971. Thorax 1975, 30, 300–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McNicholas, W.T.; Fitzgerald, M.X. Nocturnal deaths among patients with chronic bronchitis and emphysema. Br. Med. J. (Clin. Res. Ed.) 1984, 289, 878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Owens, R.L.; Macrea, M.M.; Teodorescu, M. The overlaps of asthma or COPD with OSA: A focused review. Respirology 2017, 22, 1073–1083. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orr, W.C. Review article: Sleep-related gastro-oesophageal reflux as a distinct clinical entity. Aliment. Pharmacol. Ther. 2010, 31, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Archer, L.N.J.; Simpson, H. Night cough counts and diary card scores in asthma. Arch. Dis. Child. 1985, 60, 473–474. [Google Scholar] [CrossRef] [Green Version]
- Falconer, A.; Oldman, C.; Helms, P. Poor agreement between reported and recorded nocturnal cough in asthma. Pediatr. Pulmonol. 1993, 15, 209–211. [Google Scholar] [CrossRef]
- Barry, S.J.; Dane, A.D.; Morice, A.H.; Walmsley, A.D. The automatic recognition and counting of cough. Cough 2006, 2, 8. [Google Scholar] [CrossRef] [Green Version]
- Garrard, C.S.; Seidler, A.; McKibben, A.; McAlpine, L.E.; Gordon, D. Spectral analysis of heart rate variability in bronchial asthma. Clin. Auton. Res. 1992, 2, 105–111. [Google Scholar] [CrossRef]
- Jensen, M.T.; Marott, J.L.; Lange, P.; Vestbo, J.; Schnohr, P.; Nielsen, O.W.; Jensen, J.S.; Jensen, G.B. Resting heart rate is a predictor of mortality in COPD. Eur. Respir. J. 2013, 42, 341–349. [Google Scholar] [CrossRef] [PubMed]
- Gula, L.J.; Krahn, A.D.; Skanes, A.; Ferguson, K.A.; George, C.; Yee, R.; Klein, G.J. Heart rate variability in obstructive sleep apnea: A prospective study and frequency domain analysis. Ann. Noninvasive Electrocardiol. 2003, 8, 144–149. [Google Scholar] [CrossRef] [PubMed]
- Lado, M.J.; Vila, X.A.; Rodríguez-Liñares, L.; Méndez, A.J.; Olivieri, D.N.; Félix, P. Detecting sleep apnea by heart rate variability analysis: Assessing the validity of databases and algorithms. J. Med. Syst. 2011, 35, 473–481. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.C.; Wang, H.P.; Lin, L.Y.; Lee, B.C.; Chiu, H.M.; Wu, M.S.; Chen, M.F.; Lin, J.T. Heart rate variability in patients with different manifestations of gastroesophageal reflux disease. Auton. Neurosci. 2004, 116, 39–45. [Google Scholar] [CrossRef]
- Halm, E.A.; Teirstein, A.S. Management of community-acquired pneumonia. N. Engl. J. Med. 2002, 347, 2039–2045. [Google Scholar] [CrossRef]
- Ewig, S.; Bauer, T.; Hasper, E.; Pizzulli, L.; Kubini, R.; Lüderitz, B. Prognostic analysis and predictive rule for outcome of hospital-treated community-acquired pneumonia. Eur. Respir. J. 1995, 8, 392–397. [Google Scholar] [CrossRef]
- Hsu, J.Y.; Stone, R.A.; Sinclair, R.B.L.; Worsdell, M.; Busst, C.M.; Chung, K.F. Coughing frequency in patients with persistent cough: Assessment using a 24 h ambulatory recorder. Eur. Respir. J. 1994, 7, 1246–1253. [Google Scholar] [CrossRef] [Green Version]
- Coyle, M.A.; Keenan, D.B.; Henderson, L.S.; Watkins, M.L.; Haumann, B.K.; Mayleben, D.W.; Wilson, M.G. Evaluation of an ambulatory system for the quantification of cough frequency in patients with chronic obstructive pulmonary disease. Cough 2005, 1, 3. [Google Scholar] [CrossRef] [Green Version]
- Birring, S.S.; Fleming, T.; Matos, S.; Raj, A.A.; Evans, D.H.; Pavord, I.D. The Leicester Cough Monitor: Preliminary validation of an automated cough detection system in chronic cough. Eur. Respir. J. 2008, 31, 1013–1018. [Google Scholar] [CrossRef] [Green Version]
- Vizel, E.; Yigla, M.; Goryachev, Y.; Dekel, E.; Felis, V.; Levi, H.; Kroin, I.; Godfrey, S.; Gavriely, N. Validation of an ambulatory cough detection and counting application using voluntary cough under different conditions. Cough 2010, 6, 3. [Google Scholar] [CrossRef] [Green Version]
- McGuinness, K.; Holt, K.; Dockry, R.; Smith, J. Validation of the vitaloJAK™ 24 h ambulatory cough monitor. Thorax 2012, 67, A131. [Google Scholar] [CrossRef] [Green Version]
- Fischer, P.; Sohrabi, K.; Ashraf, O.; Schneider, H.; Weissflog, A.; Gross, V. Home monitoring of nocturnal cough in COPD patients. Curr. Dir. Biomed. Eng. 2017, 3, 269–271. [Google Scholar] [CrossRef] [Green Version]
- Umayahara, Y.; Soh, Z.; Sekikawa, K.; Kawae, T.; Otsuka, A.; Tsuji, T. Clinical significance of cough peak flow and its non-contact measurement viac sounds: A narrative review. Appl. Sci. 2020, 10, 2782. [Google Scholar] [CrossRef] [Green Version]
- Umayahara, Y.; Soh, Z.; Sekikawa, K.; Kawae, T.; Otsuka, A.; Tsuji, T. Estimation of Cough Peak Flow Using Cough Sounds. Sensors 2018, 18, 2381. [Google Scholar] [CrossRef] [Green Version]
- Umayahara, Y.; Soh, Z.; Sekikawa, K.; Kawae, T.; Otsuka, A.; Tsuji, T. A Mobile Cough Strength Evaluation Device Using Cough Sounds. Sensors 2018, 18, 3810. [Google Scholar] [CrossRef] [Green Version]
- Corrigan, D.L.; Paton, J.Y. Pilot study of objective cough monitoring in infants. Pediatr. Pulmonol. 2003, 35, 350–357. [Google Scholar] [CrossRef]
- Chang, A.B.; Newman, R.G.; Phelan, P.D.; Robertson, C.F. A new use for an old Holter monitor: An ambulatory cough meter. Eur. Respir. J. 1997, 10, 1637–1639. [Google Scholar] [CrossRef] [Green Version]
- Ranjani, S.; Santhiya, V.; Jayapreetha, A. A real time cough monitor for classification of various pulmonary diseases. In Proceedings of the Third International Conference on Emerging Applications of Information Technology, Kolkata, India, 30 November–1 December 2012; pp. 102–105. [Google Scholar]
- Paul, I.M.; Wai, K.; Jewell, S.J.; Shaffer, M.L.; Varadan, V.V. Evaluation of a new self-contained, ambulatory, objective cough monitor. Cough 2006, 2, 7. [Google Scholar] [CrossRef] [Green Version]
- Liaqat, D.; Nemati, E.; Rahman, M.; Kuang, J. A method for preserving privacy during audio recordings by filtering speech. In Proceedings of the IEEE Life Sciences Conference (LSC), Sydney, Australia, 13–15 December 2017; pp. 79–82. [Google Scholar]
- Kato, T.; Ueno, A.; Kataoka, S.; Hoshino, H.; Ishiyama, Y. An application of capacitive electrode for Detecting Electrocardiogram of Neonates and Infants. In Proceedings of the 28th Annual International conference of IEEE EMBS, New York, NY, USA, 31 August–3 September 2006; pp. 916–919. [Google Scholar]
- Ueno, A.; Akabane, Y.; Kato, T.; Hoshino, H.; Kataoka, S.; Ishiyama, Y. Capacitive sensing of electrocardiographic potential through cloth from the dorsal surface of the body in a supine position: A preliminary study. IEEE Trans. Biomed. Eng. 2007, 54, 759–766. [Google Scholar] [CrossRef]
- Ueno, A.; Yamaguchi, T.; Iida, T.; Fukuoka, Y.; Uchikawa, Y.; Noshiro, M. Feasibility of capacitive sensing of surface electromyographic potential through cloth. Sens. Mater. 2012, 24, 335–346. [Google Scholar]
- Borelli, G.; Bonnet, J.J.; Hernandez, Y.R.; Matsuda, K.; Damerau, J. Spectral-distance-based detection of EMG activity from capacitive measurements. IEEE Sens. J. 2018, 18, 8502–8509. [Google Scholar] [CrossRef]
- Fontana, G.A.; Lavorini, F. Cough motor mechanisms. Respir. Physiol. Neurobiol. 2006, 152, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Yoshizumi, N.; Hori, T. Methods for sleep study. In Handbook of Sleep Science and Sleep Medicine; Japanese Society of Sleep Research, Ed.; Asakura Publishing Co.: Tokyo, Japan, 1994; pp. 452–453. (In Japanese) [Google Scholar]
- Walter, M.; Eilebrecht, B.; Wartzek, T.; Leonhardt, S. The smart car seat: Personalized monitoring of vital signs in automotive applications. Pers. Ubiquit. Comput. 2011, 15, 707–715. [Google Scholar] [CrossRef]
- Fukuyama, Y.; Suzuki, R.; Takayama, S.; Ueno, A. Multi-layered fabric electrode for movement artifact reduction in capacitive ECG Measurement. In Proceedings of the 35th Annual International Conference of IEEE (EMBS), Osaka, Japan, 3–7 July 2013; pp. 555–558. [Google Scholar]
- Kato, Y.; Motohara, S.; Omuta, T.; Azran, A.; Ueno, A. Artifact tolerance test for capacitive wearable chest-belt electrocardiograph-effect of electrode configuration. IEEJ Trans. Electron. Inf. Syst. 2017, 137, 607–615. (In Japanese) [Google Scholar]
- Bednar, T.; Babusiak, B.; Smondrk, M.; Cap, I.; Borik, S. The impact of active electrode guard layer in capacitive measurements of bio-signals. Measurement 2020, 171, 108740. [Google Scholar] [CrossRef]
- Ishigami, H.; Tanaka, S.; Ueno, A. Non-contact measurements of blink-associated electrooculogram using in-pillow cloth electrodes: Potential application as a communication aid. In Proceedings of the 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2020; pp. 4147–4150. [Google Scholar]
- Nakamura, H.; Sakajiri, Y.; Ishigami, H.; Ueno, A. A novel analog front end with voltage-dependent input impedance and bandpass amplification for capacitive biopotential measurements. Sensors 2020, 20, 2476. [Google Scholar] [CrossRef]
- Lee, J.S.; Heo, J.; Lee, W.K.; Lim, Y.G.; Kim, Y.H.; Park, K.S. Flexible capacitive electrodes for minimizing motion artifacts in ambulatory electrocardiograms. Sensors 2014, 14, 14732–14743. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.K.; Lim, Y.K.; Park, K.S. Common mode noise cancellation for electrically non-contact ECG measurement system on a chair. In Proceedings of the IEEE Engineering in Medicine and Biology Society 27th Annual Conference, Shanghai, China, 1–4 September 2005; pp. 5881–5883. [Google Scholar]
- The BioSig Project. Available online: http://biosig.sourceforge.net/ (accessed on 5 January 2021).











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject | Weight (kg) | Height (m) | BMI (kg/m2) | Age (yr) | Temp (°C) | RH (%) | VH (g/m3) |
|---|---|---|---|---|---|---|---|
| A | 74 | 1.61 | 28.5 | 23 | 23.5 | 36.0 | 7.62 |
| B | 60 | 1.75 | 19.6 | 23 | 24.0 | 28.0 | 6.10 |
| C | 70 | 1.63 | 26.3 | 23 | 23.8 | 33.0 | 7.11 |
| D | 48 | 1.53 | 20.5 | 20 | 23.8 | 43.8 | 9.44 |
| E | 57 | 1.66 | 20.7 | 24 | 21.8 | 28.0 | 5.38 |
| F | 90 | 1.65 | 33.1 | 23 | 23.6 | 35.0 | 9.34 |
| G | 64 | 1.61 | 24.7 | 23 | 25.2 | 22.0 | 5.13 |
| H | 77 | 1.80 | 23.8 | 21 | 23.5 | 22.0 | 4.66 |
| Mean ± SD | 67.5 ± 13.1 | 1.7 ± 0.1 | 24.6 ± 4.6 | 22.5 ± 1.3 | 23.7 ± 0.9 | 31.0 ± 7.5 | 6.85 ± 1.85 |
| Subject | PSNS (%) | PACC (%) | PPPV (%) | NTP + NFN |
|---|---|---|---|---|
| A | 100 | 100 | 100 | 163 |
| B | 100 | 100 | 100 | 174 |
| C | 100 | 100 | 100 | 172 |
| D | 92.5 | 85.4 | 91.8 | 133 |
| E | 33.1 | 14.3 | 20.2 | 118 |
| F | 100 | 100 | 100 | 141 |
| G | 100 | 100 | 100 | 122 |
| H | 100 | 100 | 100 | 135 |
| Mean ± SD | 90.7 ± 23.4 | 87.5 ± 30.0 | 89.0 ± 27.9 | 145 ± 22 |
| Subject | VLF ×10−4 (s2/Hz) | Error Rate (%) | LF ×10−4 (s2/Hz) | Error Rate (%) | HF ×10−4 (s2/Hz) | Error Rate (%) | VHF ×10−4 (s2/Hz) | Error Rate (%) | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ECGref | cECG | ECGref | cECG | ECGref | cECG | ECGref | cECG | |||||
| A | 8.9283 | 8.9286 | 0.004 | 62.607 | 62.615 | 0.014 | 16.102 | 16.098 | 0.02 | 8.539 | 8.531 | 0.09 |
| B | 8.0537 | 8.0543 | 0.008 | 54.646 | 54.645 | 0.002 | 14.659 | 14.657 | 0.02 | 7.804 | 7.811 | 0.10 |
| C | 8.1603 | 8.1624 | 0.026 | 56.258 | 56.273 | 0.027 | 15.446 | 15.435 | 0.08 | 7.714 | 7.747 | 0.43 |
| F | 11.9863 | 11.986 | 0.002 | 82.874 | 82.879 | 0.006 | 23.857 | 23.815 | 0.17 | 11.395 | 11.415 | 0.17 |
| G | 15.3784 | 15.378 | 0.000 | 105.311 | 105.247 | 0.061 | 29.195 | 29.141 | 0.19 | 15.340 | 15.299 | 0.27 |
| H | 13.2398 | 13.244 | 0.028 | 88.198 | 88.259 | 0.070 | 23.870 | 23.837 | 0.14 | 12.350 | 12.333 | 0.14 |
| Mean | 10.9578 | 10.9589 | 0.011 | 74.982 | 74.986 | 0.030 | 20.521 | 20.497 | 0.10 | 10.524 | 10.523 | 0.20 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takano, A.; Ishigami, H.; Ueno, A. Non-Contact Measurements of Electrocardiogram and Cough-Associated Electromyogram from the Neck Using In-Pillow Common Cloth Electrodes: A Proof-of-Concept Study. Sensors 2021, 21, 812. https://0-doi-org.brum.beds.ac.uk/10.3390/s21030812
Takano A, Ishigami H, Ueno A. Non-Contact Measurements of Electrocardiogram and Cough-Associated Electromyogram from the Neck Using In-Pillow Common Cloth Electrodes: A Proof-of-Concept Study. Sensors. 2021; 21(3):812. https://0-doi-org.brum.beds.ac.uk/10.3390/s21030812
Chicago/Turabian StyleTakano, Akira, Hiroshi Ishigami, and Akinori Ueno. 2021. "Non-Contact Measurements of Electrocardiogram and Cough-Associated Electromyogram from the Neck Using In-Pillow Common Cloth Electrodes: A Proof-of-Concept Study" Sensors 21, no. 3: 812. https://0-doi-org.brum.beds.ac.uk/10.3390/s21030812