
Combined Atlas and Convolutional Neural Network-Based Segmentation of the Hippocampus from MRI According to the ADNI Harmonized Protocol

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Datasets
2.2. Pre-Processing
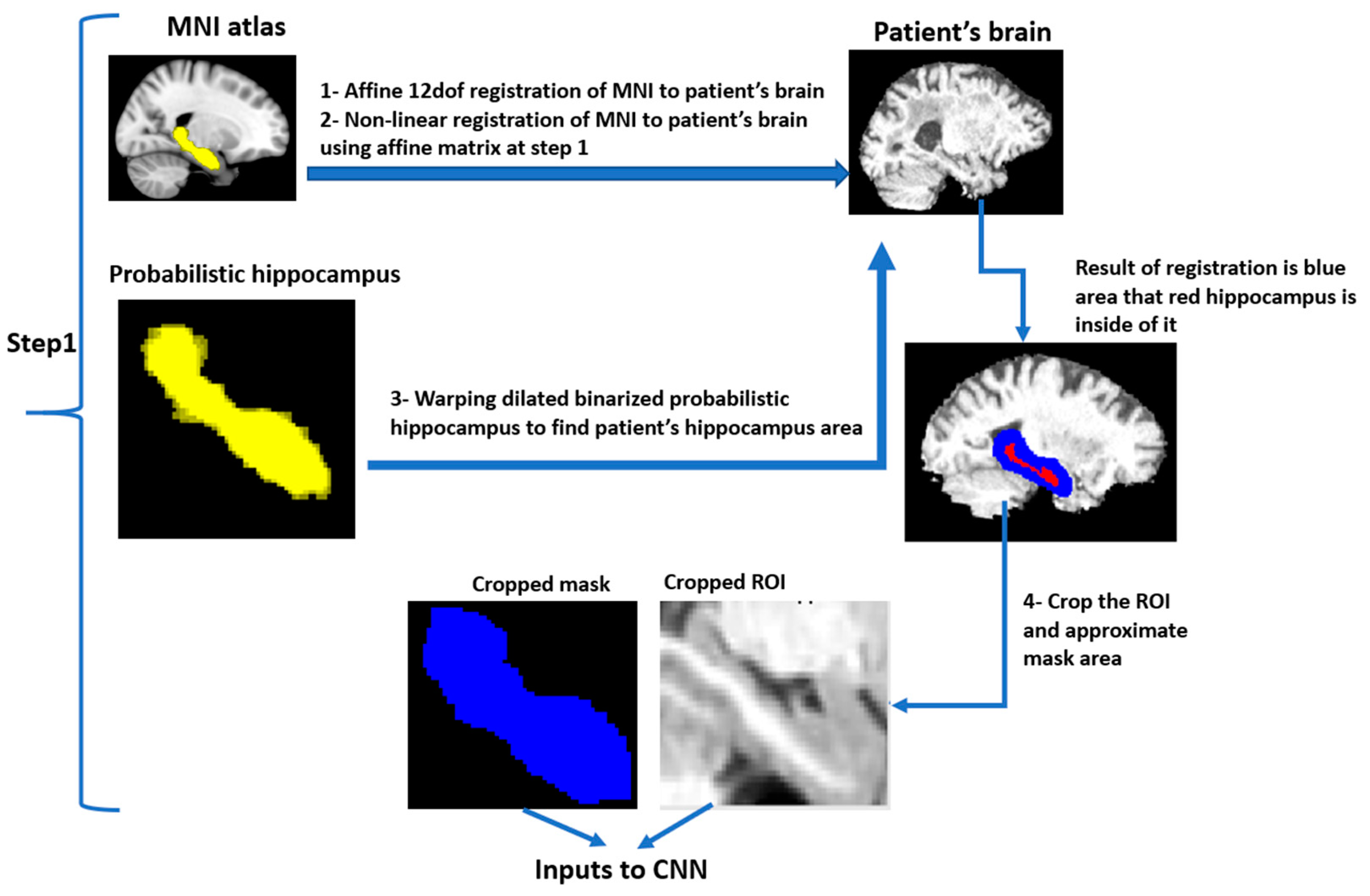
2.3. ROI Identification
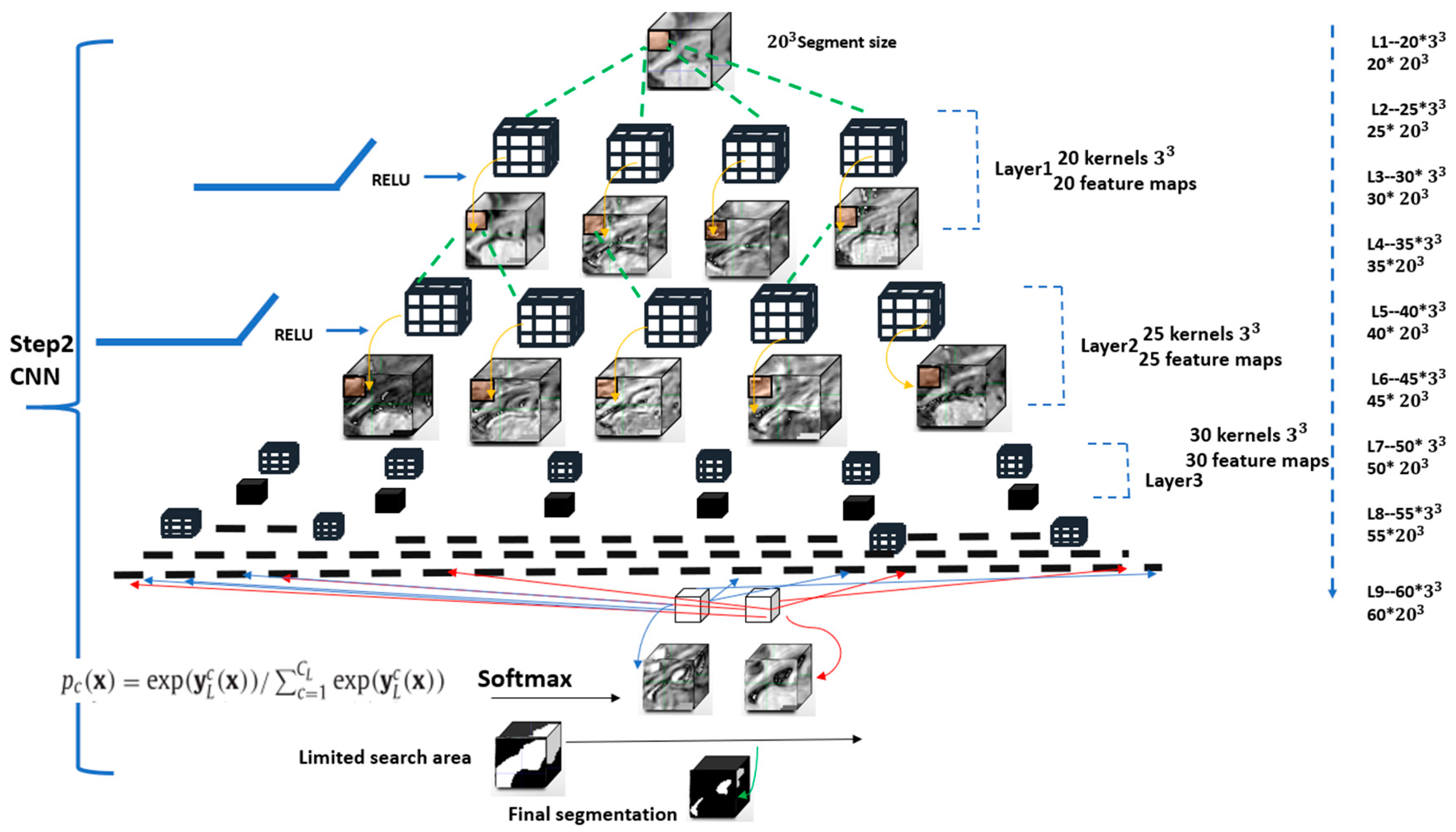
2.4. CNN Algorithm
2.5. Training of DeepHarp
2.6. Evaluation of the DeepHarp Model
2.7. Implementation Details
3. Results
Precision
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Knopman, D.S. Dementia and cerebrovascular disease. Res. Pract. Alzheimers Dis. 2007, 12, 112. [Google Scholar] [CrossRef]
- WHO. Dementia: A Public Health Priority. Available online: https://www.who.int/mental_health/publications/dementia_report_2012/en/ (accessed on 29 December 2020).
- Lista, S.; Garaci, F.G.; Ewers, M.; Teipel, S.; Zetterberg, H.; Blennow, K.; Hampel, H. CSF Aβ1-42 combined with neuroimaging biomarkers in the early detection, diagnosis and prediction of Alzheimer’s disease. Alzheimer’s Dement. 2014, 10, 381–392. [Google Scholar] [CrossRef]
- Tondelli, M.; Wilcock, G.K.; Nichelli, P.; De Jager, C.A.; Jenkinson, M.; Zamboni, G. Structural MRI changes detectable up to ten years before clinical Alzheimer’s disease. Neurobiol. Aging 2012, 33, 825.e25–825.e36. [Google Scholar] [CrossRef] [PubMed]
- Jack, C.R.; Wiste, H.J.; Weigand, S.D.; Knopman, D.S.; Mielke, M.M.; Vemuri, P.; Lowe, V.J.; Senjem, M.L.; Gunter, J.L.; Reyes, A.D.; et al. Different definitions of neurodegeneration produce similar amyloid/neurodegeneration biomarker group findings. Brain 2015, 138, 3747–3759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, P.; Sun, J.; Wolz, R.; Stephenson, D.; Brewer, J.; Fox, N.C.; Cole, P.E.; Jack, C.R., Jr.; Hill, D.L.G.; Schwarz, A.J. Operationalizing hippocampal volume as an enrichment biomarker for amnestic MCI trials: Effect of algorithm, test-retest variability and cut-point on trial cost, duration and sample size. Neurobiol. Aging 2012, 40, 1301–1315. [Google Scholar] [CrossRef]
- Wolz, R.; Schwarz, A.J.; Gray, K.R.; Yu, P.; Hill, D.L.; Initiative, A.D.N. Enrichment of clinical trials in MCI due to AD using markers of amyloid and neurodegeneration. Neurology 2016, 87, 1235–1241. [Google Scholar] [CrossRef] [Green Version]
- Den Heijer, T.; Geerlings, M.I.; Hoebeek, F.E.; Hofman, A.; Koudstaal, P.J.; Breteler, M.M.B. Use of hippocampal and amygdalar volumes on magnetic resonance imaging to predict dementia in cognitively intact elderly people. Arch. Gen. Psychiatry 2006, 63, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Martin, S.B.; Smith, C.D.; Collins, H.R.; Schmitt, F.A.; Gold, B.T. Evidence that volume of anterior medial temporal lobe is reduced in seniors destined for mild cognitive impairment. Neurobiol. Aging 2010, 31, 1099–1106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heijer, T.D.; Van Der Lijn, F.; Koudstaal, P.J.; Hofman, A.; Van Der Lugt, A.; Krestin, G.P.; Niessen, W.J.; Breteler, M.M.B. A 10-year follow-up of hippocampal volume on magnetic resonance imaging in early dementia and cognitive decline. Brain 2010, 133, 1163–1172. [Google Scholar] [CrossRef]
- Jafari-Khouzani, K.; Elisevich, K.V.; Patel, S.; Soltanian-Zadeh, H. Dataset of magnetic resonance images of nonepileptic subjects and temporal lobe epilepsy patients for validation of hippocampal segmentation techniques. Neuroinformatics 2011, 9, 335–346. [Google Scholar] [CrossRef] [Green Version]
- Nestor, S.M.; Gibson, E.; Gao, F.Q.; Kiss, A.; Black, S.E. A direct morphometric comparison of five labeling protocols for multi-atlas driven automatic segmentation of the hippocampus in Alzheimer’s disease. Neuroimage 2013, 66, 50–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thyreau, B.; Sato, K.; Fukuda, H.; Taki, Y. Segmentation of the hippocampus by transferring algorithmic knowledge for large cohort processing. Med. Image Anal. 2018, 43, 214–228. [Google Scholar] [CrossRef]
- Roy, A.G.; Conjeti, S.; Navab, N.; Wachinger, C. QuickNAT: Segmenting MRI Neuroanatomy in 20 seconds. arXiv 2018, arXiv:abs/1801.04161. [Google Scholar]
- Pipitone, J.; Park, M.T.M.; Winterburn, J.; Lett, T.A.; Lerch, J.P.; Pruessner, J.C.; Lepage, M.; Voineskos, A.N.; Chakravarty, M.M. Multi-atlas segmentation of the whole hippocampus and subfields using multiple automatically generated templates. Neuroimage 2014, 101, 494–512. [Google Scholar] [CrossRef] [Green Version]
- Patenaude, B.; Smith, S.M.; Kennedy, D.N.; Jenkinson, M. A Bayesian model of shape and appearance for subcortical brain segmentation. Neuroimage 2011, 56, 907–922. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Géron, A. Hands-On Machine Learning with Scikit-Learn; O’Reilly Media Inc.: Sebastopol, CA, USA, 2017. [Google Scholar]
- Papandreou, G.; Chen, L.-C.; Murphy, K.; Yuille, A.L. Weakly- and Semi-Supervised Learning of a DCNN for Semantic Image Segmentation. arXiv 2015, arXiv:1502.02734. [Google Scholar]
- Fischl, B. FreeSurfer. Neuroimage 2013, 62, 774–781. [Google Scholar] [CrossRef] [Green Version]
- Dolz, J.; Desrosiers, C.; Ben Ayed, I. 3D fully convolutional networks for subcortical segmentation in MRI: A large-scale study. Neuroimage 2018, 170, 456–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duchesne, S.; Valdivia, F.; Robitaille, N.; Mouiha, A.; Bocchetta, M.; Apostolova, L.G.; Ganzola, R.; Preboske, G.; Wolf, D.; Boccardi, M.; et al. Manual segmentation qualification platform for the EADC-ADNI harmonized protocol for hippocampal segmentation project. Alzheimer’s Dement. 2015, 11, 161–174. [Google Scholar] [CrossRef]
- Duchesne, S.; Valdivia, F.; Robitaille, N.; Valdivia, A.; Apostolova, L.; Bocchetta, M.; Ganzola, R.; Preboske, G.; Wolf, D.; Boccardi, M.; et al. Manual segmentation certification platform for the EADC-ADNI harmonized protocol for the hippocampal volumetry project. Alzheimer’s Dement. 2013, 9, 409–410. [Google Scholar] [CrossRef]
- Sun, J.; Yan, S.; Song, C.; Han, B. Dual-functional neural network for bilateral hippocampi segmentation and diagnosis of Alzheimer’s disease. Int. J. Comput. Assist. Radiol. Surg. 2020, 15, 445–455. [Google Scholar] [CrossRef]
- Zhu, H.; Tang, Z.; Cheng, H.; Wu, Y.; Fan, Y. Multi-atlas label fusion with random local binary pattern features: Application to hippocampus segmentation. Sci. Rep. 2019, 9, 1–14. [Google Scholar] [CrossRef]
- Dill, V.; Klein, P.C.; Franco, A.R.; Pinho, M.S. Atlas selection for hippocampus segmentation: Relevance evaluation of three meta-information parameters. Comput. Biol. Med. 2018, 95, 90–98. [Google Scholar] [CrossRef]
- Liu, M.; Li, F.; Yan, H.; Wang, K.; Ma, Y.; Shen, L.; Xu, M. A multi-model deep convolutional neural network for automatic hippocampus segmentation and classification in Alzheimer’s disease. Neuroimage 2020, 208, 116459. [Google Scholar] [CrossRef]
- Ataloglou, D.; Dimou, A.; Zarpalas, D.; Daras, P. Fast and Precise Hippocampus Segmentation through Deep Convolutional Neural Network Ensembles and Transfer Learning. Neuroinformatics 2019, 17, 563–582. [Google Scholar] [CrossRef]
- Pamela, J.; Ls, T.; John, C.; Andrei, G.; Marcus, E. OASIS-3: Longitudinal Neuroimaging, Clinical, and Cognitive Dataset for Normal Aging and Alzheimer Disease. MedRxiv 2019. [Google Scholar] [CrossRef] [Green Version]
- Maclaren, J.; Han, Z.; Vos, S.B.; Fischbein, N.; Bammer, R. Reliability of brain volume measurements: A test-retest dataset. Sci. Data 2014, 1, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Modat, M.; Cash, D.M.; Winston, G.P.; Duncan, J.S. Global image registration using a symmetric block-matching approach. J. Med. Imaging 2014, 1, 024003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamnitsas, K.; Ledig, C.; Newcombe, V.F.; Simpson, J.P.; Kane, A.D.; Menon, D.K.; Rueckert, D.; Glocker, B. Efficient multi-scale 3D CNN with fully connected CRF for accurate brain lesion segmentation. Med. Image Anal. 2017, 36, 61–78. [Google Scholar] [CrossRef] [PubMed]
- Long, J.; Shelhamer, E.; Darrell, T. Fully convolutional networks for semantic segmentation. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Boston, MA, USA, 7–12 June 2015; pp. 3431–3440. [Google Scholar] [CrossRef] [Green Version]
- Bengio, Y. Practical recommendations for gradient-based training of deep architectures. Lect. Notes Comput. Sci. 2012, 7700, 437–478. [Google Scholar] [CrossRef]
- Milletari, F.; Navab, N.; Ahmadi, S.A. V-Net: Fully convolutional neural networks for volumetric medical image segmentation. In Proceedings of the 2016 fourth international conference on 3D vision (3DV), Stanford, CA, USA, 25–28 October 2016; pp. 565–571. [Google Scholar] [CrossRef] [Green Version]
- Ronneberger, O.; Fischer, P.; Brox, T. U-Net: Convolutional Networks for Biomedical Image Segmentation. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Munich, Germany, 5–9 October 2015; pp. 1–8. [Google Scholar]
- He, K.; Gkioxari, G.; Dollár, P.; Girshick, R. Mask, r-cnn. arXiv 2017, arXiv:1703.06870. [Google Scholar]
- van Opbroek, A.; Achterberg, H.C.; Vernooij, M.W.; Arfan Ikram, M.; de Bruijne, M. Transfer learning by feature-space transformation: A method for Hippocampus segmentation across scanners. NeuroImage Clin. 2018, 20, 466–475. [Google Scholar] [CrossRef] [PubMed]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. In Proceedings of the 3rd International Conference on Learning Representations ICLR 2015, San Diego, CA, USA, 7–9 May 2015; pp. 1–14. [Google Scholar]
- Mateen, M.; Wen, J.; Nasrullah Song, S.; Huang, Z. Fundus image classification using VGG-19 architecture with PCA and SVD. Symmetry 2019, 11, 1. [Google Scholar] [CrossRef] [Green Version]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Reco4gnition 2016, Washington, DC, USA, 12 December 2016; pp. 770–778. [Google Scholar] [CrossRef] [Green Version]
- Alex, K.; Sutskever, I. GEH. Advances in Neural Information Processing Systems 25 (NIPS 2012); Morgan Kaufmann Publishers Inc.: San Francisco, CA, USA, 2012. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Datasets | ADNI-HarP Segmentation | Total Sample Size | Training Data | Validation Data | Testing Data | Test-Retest Data |
|---|---|---|---|---|---|---|
| SunnyBrook | no | 50 | 50 | 0 | 0 | 0 |
| OASIS | no | 14 | 14 | 0 | 0 | 0 |
| ADNI-HarP | yes | 130 | 78 | 29 | 23 | 0 |
| Healthy and patients with epilepsy | no | 50 | 50 | 0 | 0 | 0 |
| Test-retest (single subject) | no | 40 | 0 | 0 | 0 | 40 |
| Total | - | 284 | 192 | 29 | 23 | 40 |
| Test Set/Dice Coefficient | Test-Retest Set/Dice Coefficient | |||||||
|---|---|---|---|---|---|---|---|---|
| Left Hippocampus Mean ± SD | Right Hippocampus Mean ± SD | p-Values vs. DeepHarp Left Hippocampus | p-Values vs. DeepHarp Right Hippocampus | Left Hippocampus Mean ± SD | Right Hippocampus Mean ± SD | p-Values vs. DeepHarp Left Hippocampus | p-Values vs. DeepHarp Right Hippocampus | |
| DeepHarp | 0.893 ± 0.017 | 0.889 ± 0.190 | N/A | N/A | 0.95 ± 0.01 | 0.951 ± 0.005 | N/A | N/A |
| HippoDeep | 0.799 ± 0.033 | 0.79 ± 0.049 | <0.001 | <0.001 | 0.957 ± 0.008 | 0.96 ± 0.006 | 0.029 | <0.001 |
| QuickNat | 0.812 ± 0.024 | 0.834 ± 0.023 | <0.001 | <0.001 | 0.948 ± 0.007 | 0.951 ± 0.006 | 0.278 | 0.817 |
| FSL | 0.765 ± 0.025 | 0.759 ± 0.037 | <0.001 | <0.001 | 0.918 ± 0.017 | 0.923 ± 0.012 | <0.001 | <0.001 |
| FreeSurfer | 0.715 ± 0.047 | 0.741 ± 0.033 | <0.001 | <0.001 | 0.91 ± 0.01 | 0.916 ± 0.008 | <0.001 | <0.001 |
| Test-Retest Set/Absolute Volume Differences in Milliliter | Test-Retest Set/Dice Scores | |||||||
|---|---|---|---|---|---|---|---|---|
| Left Hippocampus Mean Volume Difference ± SD | Right Hippocampus Mean Volume Difference ± SD | p-Values vs. DeepHarp Left Hippocampus | p-Values vs. DeepHarp Right Hippocampus | Left Hippocampus Mean Dice ± SD | Right Hippocampus Mean Dice ± SD | p-Values vs. DeepHarp Left Hippocampus | p-Values vs. DeepHarp Right Hippocampus | |
| DeepHarp | 0.080 ± 0.057 | 0.052 ± 0.036 | N/A | N/A | 0.95 ± 0.01 | 0.951 ± 0.005 | N/A | N/A |
| HippoDeep | 0.056 ± 0.050 | 0.044 ± 0.030 | <0.163 | <0.622 | 0.957 ± 0.008 | 0.96 ± 0.006 | 0.029 | <0.001 |
| QuickNat | 0.035 ± 0.021 | 0.055 ± 0.040 | <0.004 | <0.881 | 0.948 ± 0.007 | 0.951 ± 0.006 | 0.278 | 0.817 |
| FSL | 0.174 ± 0.11 | 0.103 ± 0.085 | <0.003 | <0.101 | 0.918 ± 0.017 | 0.923 ± 0.012 | <0.001 | <0.001 |
| FreeSurfer | 0.141 ± 0.113 | 0.114 ± 0.082 | <0.078 | <0.010 | 0.91 ± 0.01 | 0.916 ± 0.008 | <0.001 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nobakht, S.; Schaeffer, M.; Forkert, N.D.; Nestor, S.; E. Black, S.; Barber, P.; the Alzheimer’s Disease Neuroimaging Initiative. Combined Atlas and Convolutional Neural Network-Based Segmentation of the Hippocampus from MRI According to the ADNI Harmonized Protocol. Sensors 2021, 21, 2427. https://0-doi-org.brum.beds.ac.uk/10.3390/s21072427
Nobakht S, Schaeffer M, Forkert ND, Nestor S, E. Black S, Barber P, the Alzheimer’s Disease Neuroimaging Initiative. Combined Atlas and Convolutional Neural Network-Based Segmentation of the Hippocampus from MRI According to the ADNI Harmonized Protocol. Sensors. 2021; 21(7):2427. https://0-doi-org.brum.beds.ac.uk/10.3390/s21072427
Chicago/Turabian StyleNobakht, Samaneh, Morgan Schaeffer, Nils D. Forkert, Sean Nestor, Sandra E. Black, Philip Barber, and the Alzheimer’s Disease Neuroimaging Initiative. 2021. "Combined Atlas and Convolutional Neural Network-Based Segmentation of the Hippocampus from MRI According to the ADNI Harmonized Protocol" Sensors 21, no. 7: 2427. https://0-doi-org.brum.beds.ac.uk/10.3390/s21072427