
The Development of an Automatic Rib Sequence Labeling System on Axial Computed Tomography Images with 3-Dimensional Region Growing

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Data
2.3. Experiment Environment
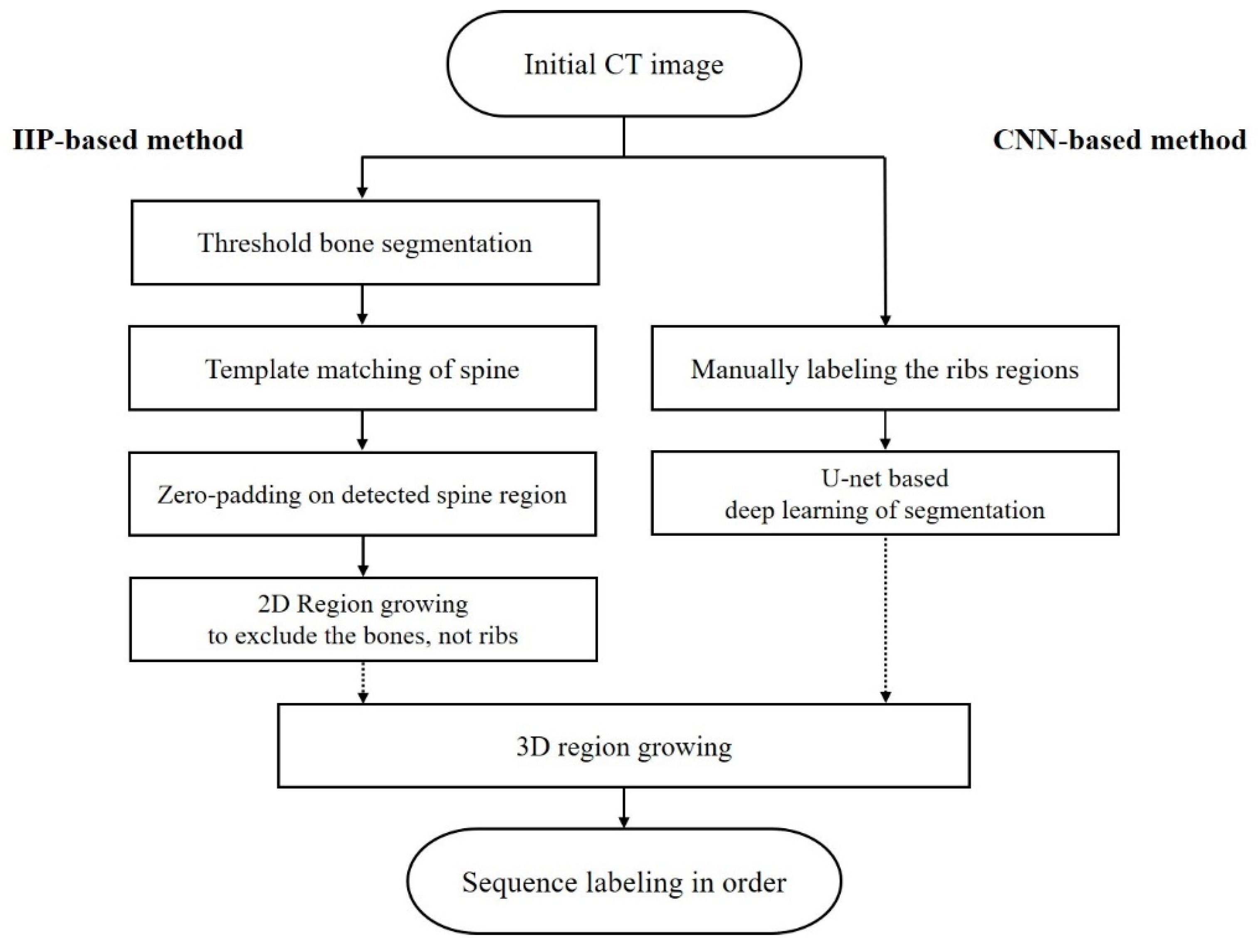
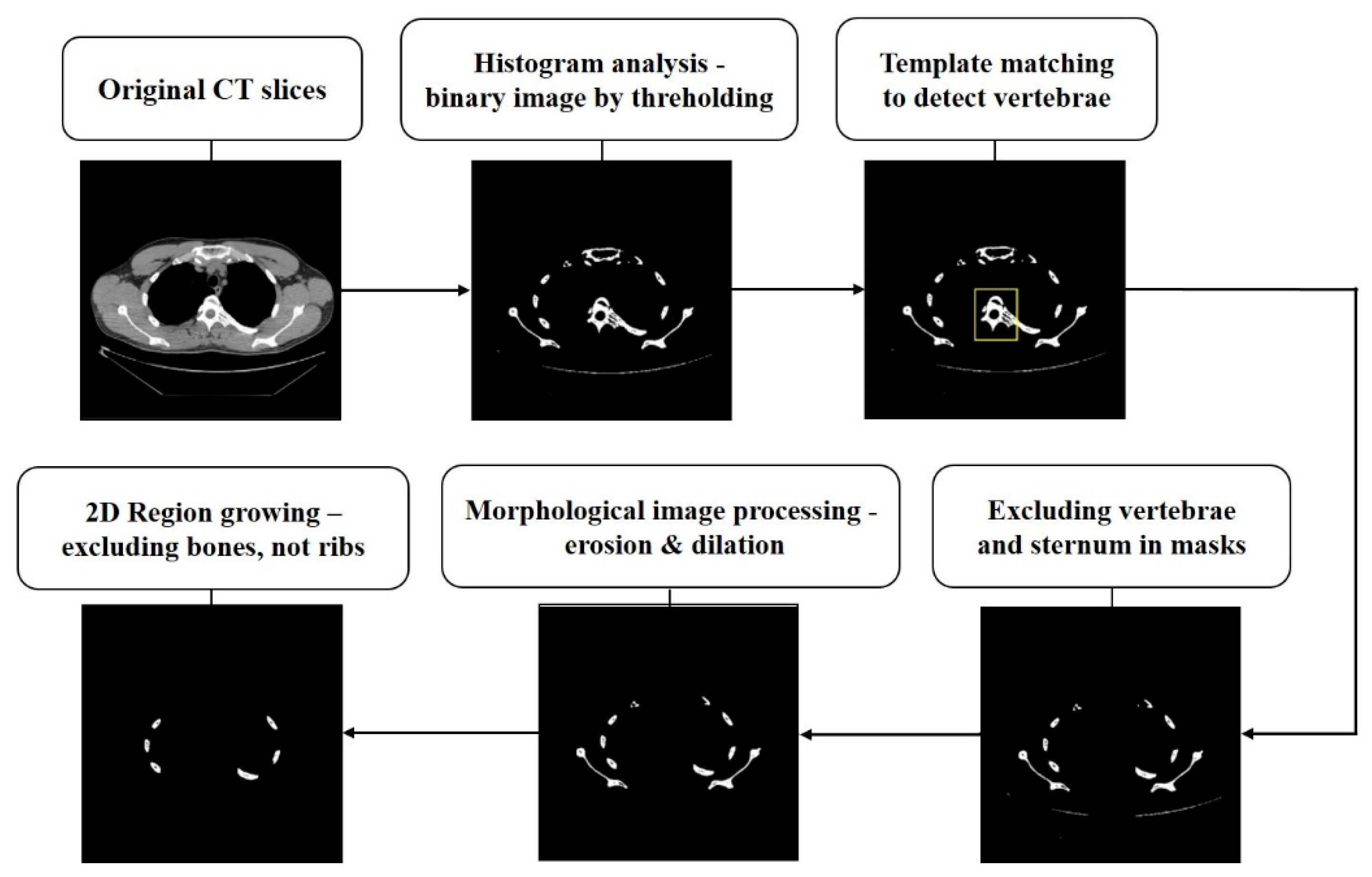
2.4. Processing to Generate Masks of Interesting Rib Regions
2.4.1. IIP-Based Method
2.4.2. CNN-Based Method
2.5. 3D-Region Growing for Sequence Labeling
2.6. Statistical Analysis-Based Performance Evaluation
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CT | computed tomography |
| IIP | intensity-based image processing |
| CNN | convolutional neural network |
| 3D | 3-dimensional |
| DSC | dice similarity coefficient |
| SAD | the sum of absolute differences |
| TP | true-positive |
| FP | false-positive |
| TN | true-negative |
| FN | false-negative |
| CI | confidence interval |
References
- Sunshine, J.H.; Maynard, C.D.; Paros, J.; Forman, H.P. Update on the diagnostic radiologist shortage. AJR Am. J. Roentgenol. 2004, 182, 301–305. [Google Scholar] [CrossRef] [PubMed]
- Do, H.M.; Spear, L.G.; Nikpanah, M.; Mirmomen, S.M.; Machado, L.B.; Folio, L.R. Augmented Radiologist Workflow Improves Report Value and Saves Time: A Potential Model for Implementation of Artificial Intelligence. Acad. Radiol. 2020, 27, 96–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, D.; Hwang, W.; Bae, J.; Park, H.; Kim, K. Video Archiving and Communication System (VACS): A Progressive Approach, Design, Implementation, and Benefits for Surgical Videos. Healthc. Inform. Res. 2021, 27, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Kim, Y.; Kim, K. Bone age estimation using deep learning and hand X-ray images. Biomed. Eng. Lett. 2020, 10, 323–331. [Google Scholar] [CrossRef]
- Buzug, T.M. Computed tomography. In Springer Handbook of Medical Technology; Springer: Berlin/Heidelberg, Germany; New York, NY, USA, 2011; pp. 311–342. [Google Scholar]
- Pinto, A.; Brunese, L. Spectrum of diagnostic errors in radiology. World J. Radiol. 2010, 2, 377–383. [Google Scholar] [CrossRef]
- Jones, F.W. The Anatomy of Cervical Ribs; SAGE Publications: New York, NY, USA, 1913. [Google Scholar]
- Graeber, G.M.; Nazim, M. The anatomy of the ribs and the sternum and their relationship to chest wall structure and function. Thorac. Surg. Clin. 2007, 17, 473–489. [Google Scholar] [CrossRef]
- Bhalla, M.; McCauley, D.I.; Golimbu, C.; Leitman, B.S.; Naidich, D.P. Counting ribs on chest CT. J. Comput. Assist. Tomogr. 1990, 14, 590–594. [Google Scholar] [CrossRef]
- Kurihara, Y.; Yakushiji, Y.K.; Matsumoto, J.; Ishikawa, T.; Hirata, K. The ribs: Anatomic and radiologic considerations. Radiographics 1999, 19, 105–119. [Google Scholar] [CrossRef]
- Wu, M.; Chai, Z.; Qian, G.; Lin, H.; Wang, Q.; Wang, L.; Chen, H. Development and Evaluation of a Deep Learning Algorithm for Rib Segmentation and Fracture Detection from Multicenter Chest CT Images. Radiol. Artif. Intell. 2021, 3, e200248. [Google Scholar] [CrossRef]
- Jin, L.; Yang, J.; Kuang, K.; Ni, B.; Gao, Y.; Li, M. Deep-learning-assisted detection and segmentation of rib fractures from CT scans: Development and validation of FracNet. EBioMedicine 2020, 62, 103106. [Google Scholar] [CrossRef]
- Weikert, T.; Noordtzij, L.A.; Bremerich, J.; Stieltjes, B.; Parmar, V.; Sauter, A.W. Assessment of a Deep Learning Algorithm for the Detection of Rib Fractures on Whole-Body Trauma Computed Tomography. Korean J. Radiol. 2020, 21, 891–899. [Google Scholar] [CrossRef] [PubMed]
- Staal, J.; van Ginneken, B.; Viergever, M.A. Automatic rib segmentation and labeling in computed tomography scans using a general framework for detection, recognition and segmentation of objects in volumetric data. Med. Image Anal. 2007, 11, 35–46. [Google Scholar] [CrossRef] [PubMed]
- Wessel, J.; Heinrich, M.P.; von Berg, J.; Franz, A.; Saalbach, A. Sequential rib labeling and segmentation in chest X-ray using Mask R-CNN. arXiv 2019, arXiv:1908.08329. [Google Scholar]
- Klein, S.; Staring, M.; Murphy, K.; Viergever, M.A.; Pluim, J.P. Elastix: A toolbox for intensity-based medical image registration. IEEE Trans. Med. Imaging 2010, 29, 196–205. [Google Scholar] [CrossRef] [PubMed]
- Petrou, M.M.; Petrou, C. Image Processing: The fundamentals; John Wiley & Sons: Hoboken, NJ, USA, 2010. [Google Scholar]
- Guo, Z.; Li, X.; Huang, H.; Guo, N.; Li, Q. Learning-Based Image Segmentation on Multimodal Medical Imaging. IEEE Trans. Radiat. Plasma Med. Sci. 2019, 3, 162–169. [Google Scholar] [CrossRef]
- Roth, H.R.; Farag, A.; Lu, L.; Turkbey, E.B.; Summers, R.M. Deep convolutional networks for pancreas segmentation in CT imaging. In Proceedings of the Medical Imaging 2015: Image Processing, Orlando, FL, USA, 13 May 2015; Volume 9413, p. 94131G. [Google Scholar]
- Ronneberger, O.; Fischer, P.; Brox, T. U-net: Convolutional networks for biomedical image segmentation. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Munich, Germany, 5–9 October 2015; Springer: Cham, Switzerland; pp. 234–241. [Google Scholar]
- Alom, M.Z.; Yakopcic, C.; Hasan, M.; Taha, T.M.; Asari, V.K. Recurrent residual U-Net for medical image segmentation. J. Med. Imaging 2019, 6, 014006. [Google Scholar] [CrossRef]
- Shen, W.; Xu, W.; Zhang, H.; Sun, Z.; Ma, J.; Wang, Y. Automatic segmentation of the femur and tibia bones from X-ray images based on pure dilated residual U-Net. Inverse Probl. Imaging 2011, 15, 1333. [Google Scholar] [CrossRef]
- Ding, L.; Zhao, K.; Zhang, X.; Wang, X.; Zhang, J. A lightweight U-Net architecture multi-scale convolutional network for pediatric hand bone segmentation in X-ray image. IEEE Access 2019, 7, 68436–68445. [Google Scholar] [CrossRef]
- Sánchez, J.C.G.; Magnusson, M.; Sandborg, M.; Tedgren, Å.C.; Malusek, A. Segmentation of bones in medical dual-energy computed tomography volumes using the 3D U-Net. Phys. Med. 2020, 69, 241–247. [Google Scholar] [CrossRef]
- Brunelli, R. Template Matching Techniques in Computer Vision: Theory and Practice; John Wiley & Sons: Hoboken, NJ, USA, 2009. [Google Scholar]
- Sarvaiya, J.N.; Patnaik, S.; Bombaywala, S. Image registration by template matching using normalized cross-correlation. In Proceedings of the 2009 International Conference on Advances in Computing, Control, and Telecommunication Technologies, IEEE, Kerala, India, 28–29 December 2009. [Google Scholar]
- Dawoud, N.N.; Samir, B.B.; Janier, J. Fast template matching method based optimized sum of absolute difference algorithm for face localization. Int. J. Comput. Appl. 2011, 18, 30–34. [Google Scholar]
- Korman, S.; Reichman, D.; Tsur, G.; Avidan, S. Fast-match: Fast affine template matching. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Portland, OR, USA, 23–28 June 2013; pp. 2331–2338. [Google Scholar]
- Wei, S.D.; Lai, S.H. Fast template matching based on normalized cross correlation with adaptive multilevel winner update. IEEE Trans Image Process 2008, 17, 2227–2235. [Google Scholar] [CrossRef] [PubMed]
- Adams, R.; Bischof, L. Seeded region growing. IEEE Trans. Pattern Anal. Mach. Intell. 1994, 16, 641–647. [Google Scholar] [CrossRef] [Green Version]
- Pohle, R.; Toennies, K.D. Segmentation of medical images using adaptive region growing. Med. Imaging 2001 Image Processing 2001, 4322, 1337–1346. [Google Scholar]
- Von Eicken, T.; Basu, A.; Buch, V.; Vogels, W. U-Net: A user-level network interface for parallel and distributed computing. ACM SIGOPS Oper. Syst. Rev. 1995, 29, 40–53. [Google Scholar] [CrossRef]
- Du, G.; Cao, X.; Liang, J.; Chen, X.; Zhan, Y. Medical image segmentation based on u-net: A review. J. Imaging Sci. Technol. 2020, 64, 20508-1–20508-12. [Google Scholar] [CrossRef]
- da Nóbrega, R.V.M.; Rodrigues, M.B.; Rebouças Filho, P.P. Segmentation and visualization of the lungs in three dimensions using 3D Region Growing and Visualization Toolkit in CT examinations of the chest. In Proceedings of the 2017 IEEE 30th International Symposium on Computer-Based Medical Systems (CBMS), Thessaloniki, Greece, 22–24 June 2017; pp. 397–402. [Google Scholar]
- Revol-Muller, C.; Peyrin, F.; Carrillon, Y.; Odet, C. Automated 3D region growing algorithm based on an assessment function. Pattern Recognit. Lett. 2002, 23, 137–150. [Google Scholar] [CrossRef]
- Justice, R.K.; Stokely, E.M.; Strobel, J.S.; Ideker, R.E.; Smith, W.M. Medical image segmentation using 3D seeded region growing. Med. Imaging 1997 Image Processing 1997, 3034, 900–910. [Google Scholar]
- Yang, Z.; Zhao, Y.Q.; Liao, M.; Di, S.H.; Zeng, Y.Z. Semi-automatic liver tumor segmentation with adaptive region growing and graph cuts. Biomed. Signal Processing Control. 2021, 68, 102670. [Google Scholar] [CrossRef]
- Ko, S.; Yi, J.; Lim, J.E.; Ra, J.B. Efficient segmentation algorithm for 3D medical image data using a region-growing-based tracking. In Proceedings of the Medical Imaging 2000: Image Processing, San Diego, CA, USA, 12–18 February 2000. [Google Scholar]
- Kato, H.; Kiyokawa, H.; Inoue, H.; Kobayashi, S.; Nishizawa, O. Anatomical reconsideration to renal area: Lessons learned from radical nephrectomy or adrenalectomy through a minimal incision over the 12th rib. Int. J. Urol. 2004, 11, 709–713. [Google Scholar] [CrossRef]
- De Cicco, G.; Tosi, D.; Crisci, R.; Bortolami, A.; Aquino, T.M.; Benussi, S. Use of new cannulated screws for primary sternal closure in high risk patients for sternal dehiscence. J. Thorac. Dis. 2019, 11, 4538. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| U-Net (CNN) | |||||
|---|---|---|---|---|---|
| Recall (%) | Precision (%) | Specificity (%) | Accuracy (%) | DSC | |
| Average | 91.99 | 90.61 | 98.33 | 97.91 | 0.89 |
| (95% CI) | (90.83–93.15) | (89.26–91.96) | (97.87–98.79) | (97.42–98.40) | (0.87–0.91) |
| Min | 90.23 | 88.91 | 97.88 | 97.44 | 0.87 |
| Max | 93.31 | 91.87 | 98.91 | 98.82 | 0.92 |
| Labeling | p-Value | ||
|---|---|---|---|
| No. (Out of 50 cases in total) (Success cases Nr./Total cases Nr.) | Successful sequence labeling rate on all ribs (%) (95% CI) | p < 0.05 | |
| IIP-based | 46/50 | 92.0% (85.4–98.6%) | |
| CNN-based | 49/50 | 98.0% (94.5–100.0%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seol, Y.J.; Park, S.H.; Kim, Y.J.; Park, Y.-T.; Lee, H.Y.; Kim, K.G. The Development of an Automatic Rib Sequence Labeling System on Axial Computed Tomography Images with 3-Dimensional Region Growing. Sensors 2022, 22, 4530. https://0-doi-org.brum.beds.ac.uk/10.3390/s22124530
Seol YJ, Park SH, Kim YJ, Park Y-T, Lee HY, Kim KG. The Development of an Automatic Rib Sequence Labeling System on Axial Computed Tomography Images with 3-Dimensional Region Growing. Sensors. 2022; 22(12):4530. https://0-doi-org.brum.beds.ac.uk/10.3390/s22124530
Chicago/Turabian StyleSeol, Yu Jin, So Hyun Park, Young Jae Kim, Young-Taek Park, Hee Young Lee, and Kwang Gi Kim. 2022. "The Development of an Automatic Rib Sequence Labeling System on Axial Computed Tomography Images with 3-Dimensional Region Growing" Sensors 22, no. 12: 4530. https://0-doi-org.brum.beds.ac.uk/10.3390/s22124530