
Assessment of a Therapeutic X-ray Radiation Dose Measurement System Based on a Flexible Copper Indium Gallium Selenide Solar Cell

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
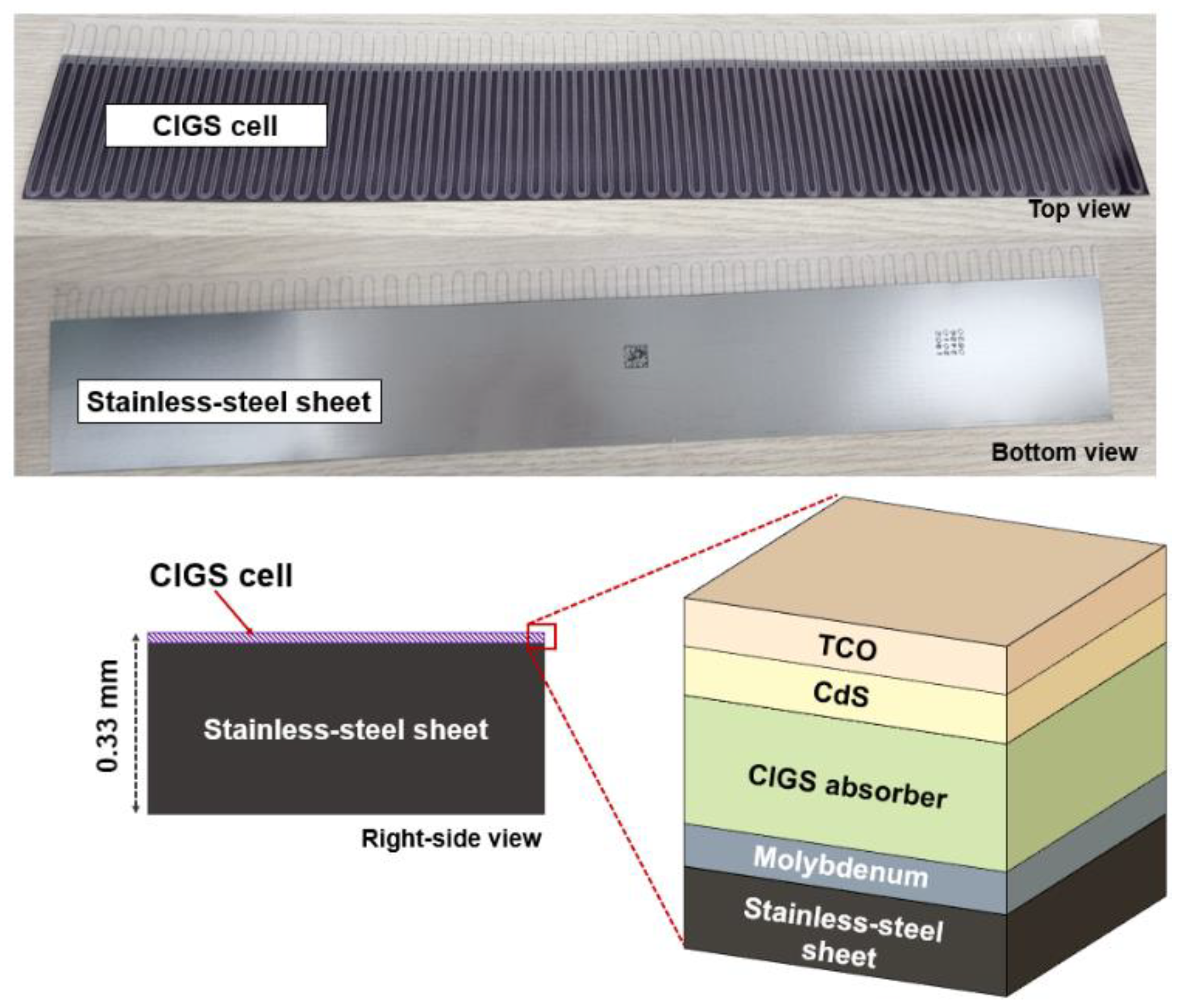
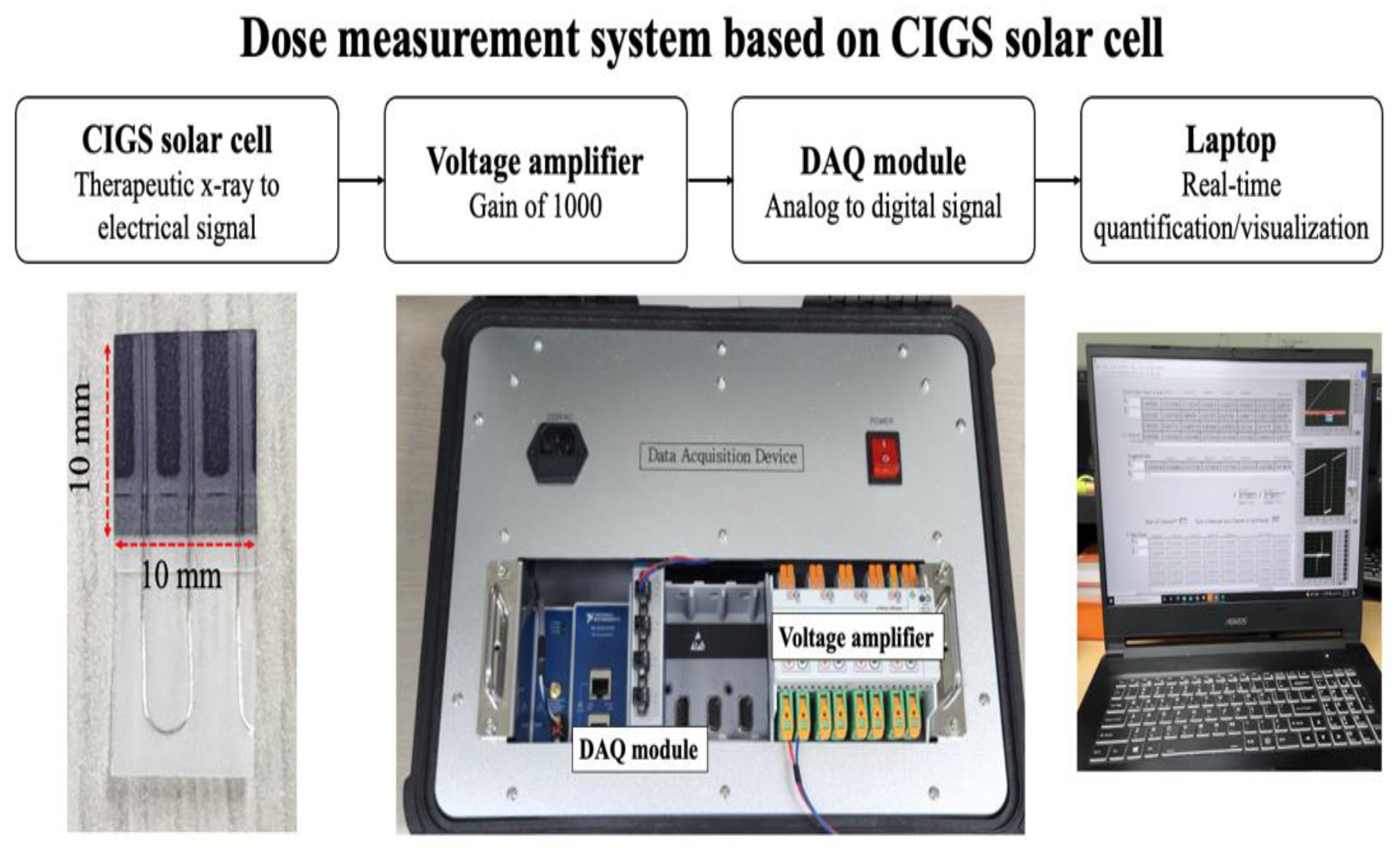
2.1. System Configuration
2.2. Quantifications and Evalutions of Dosimetric Characteristics
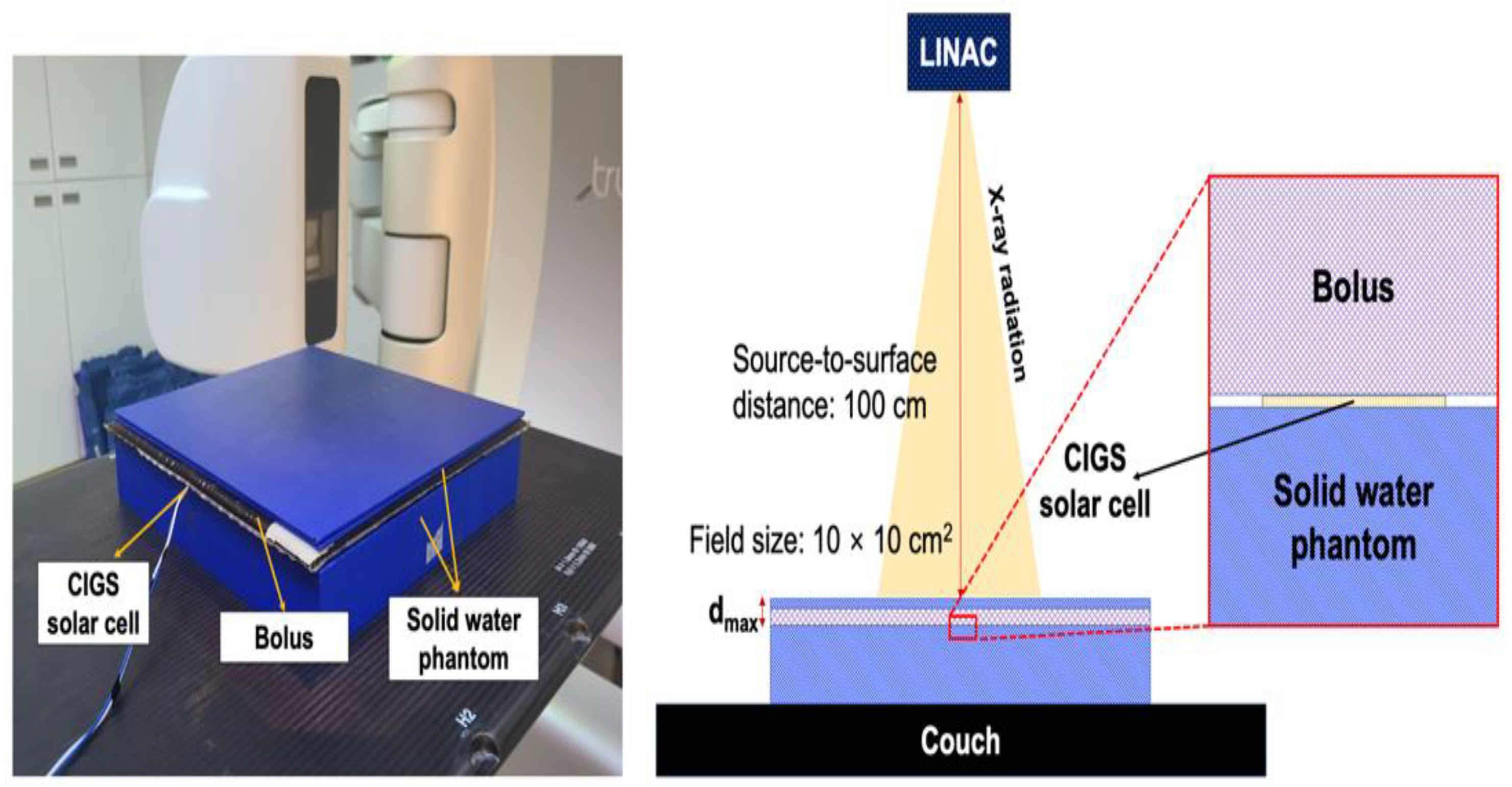
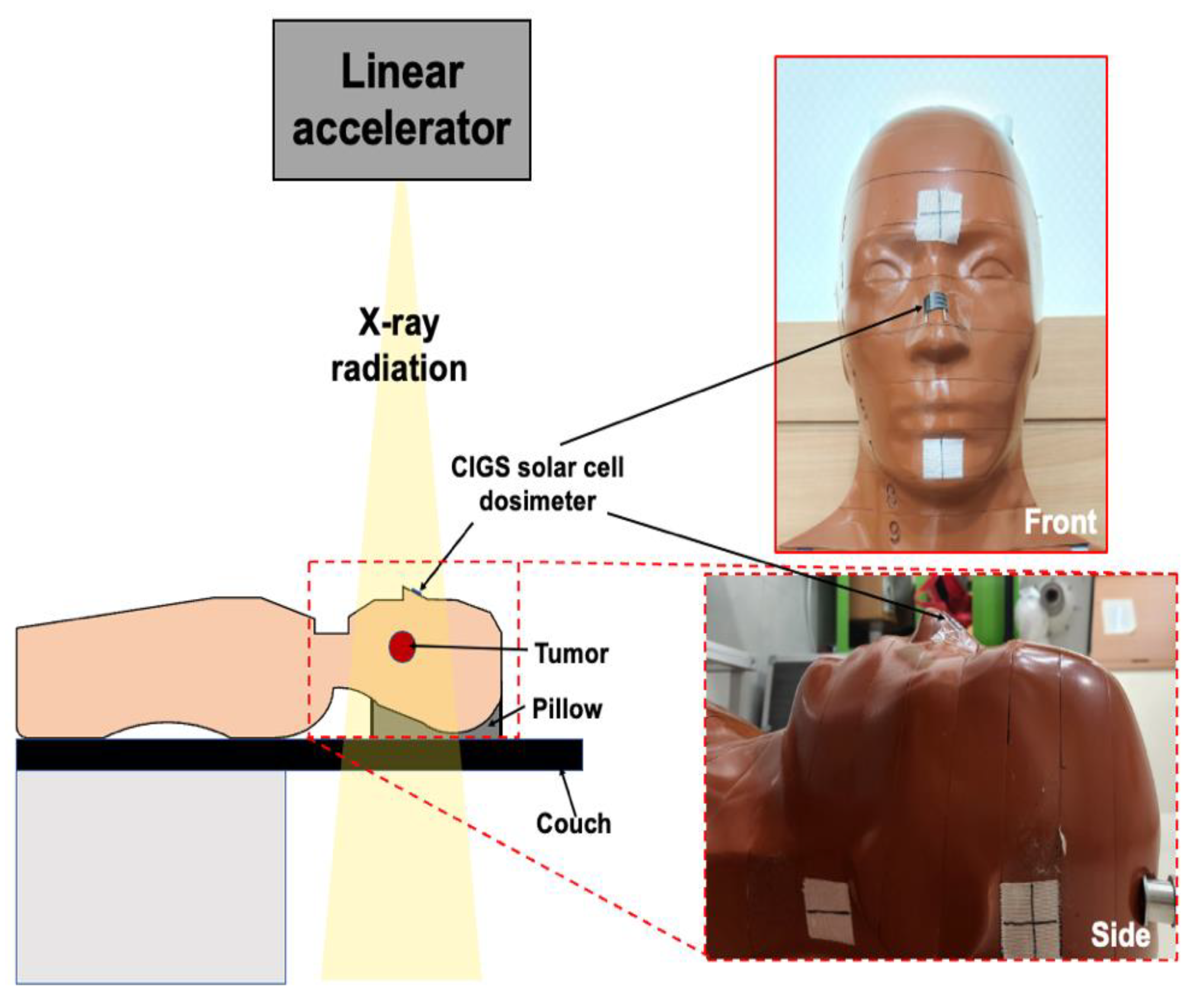
2.2.1. Experimental Setup
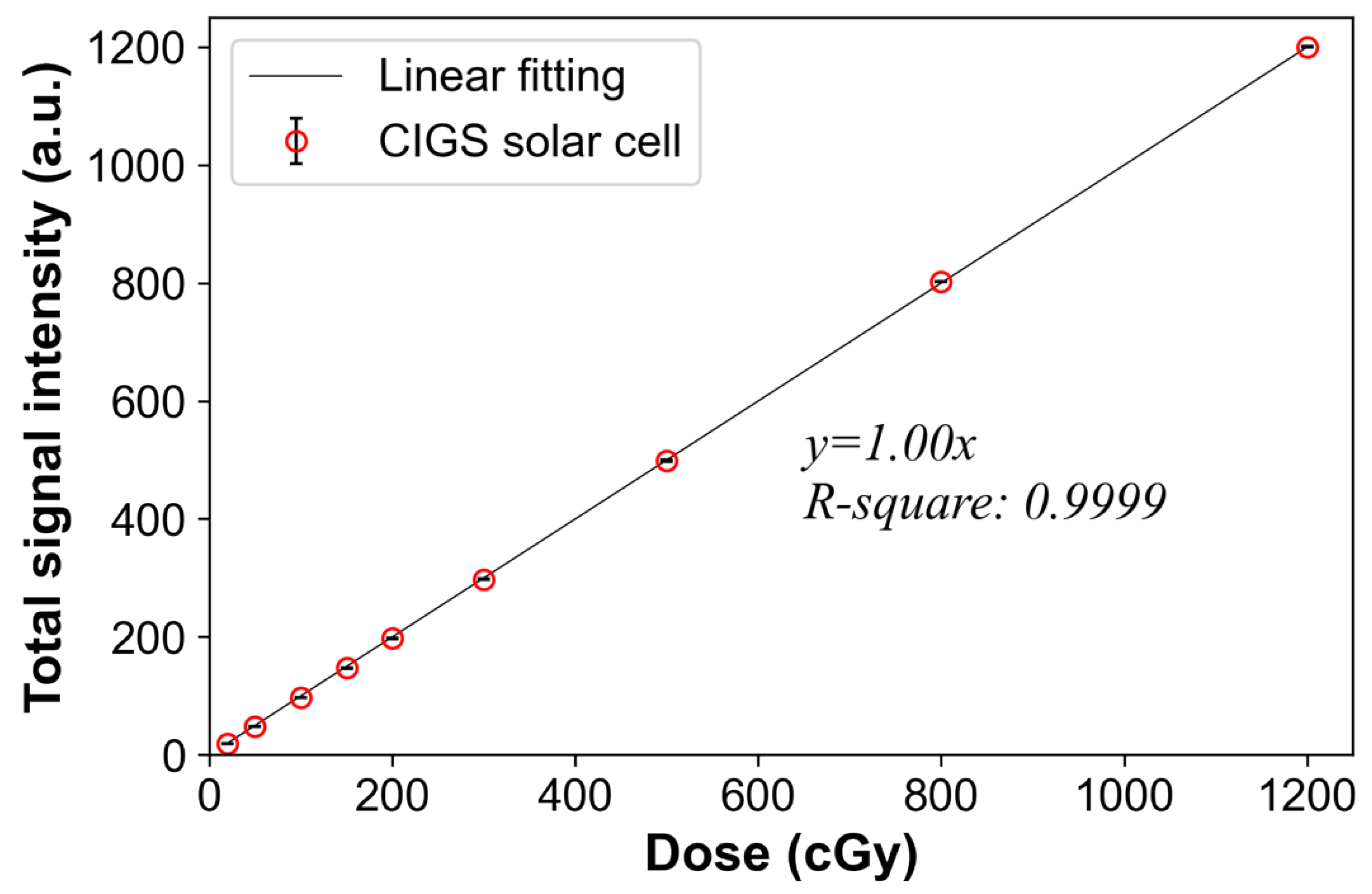
2.2.2. Dose Linearity
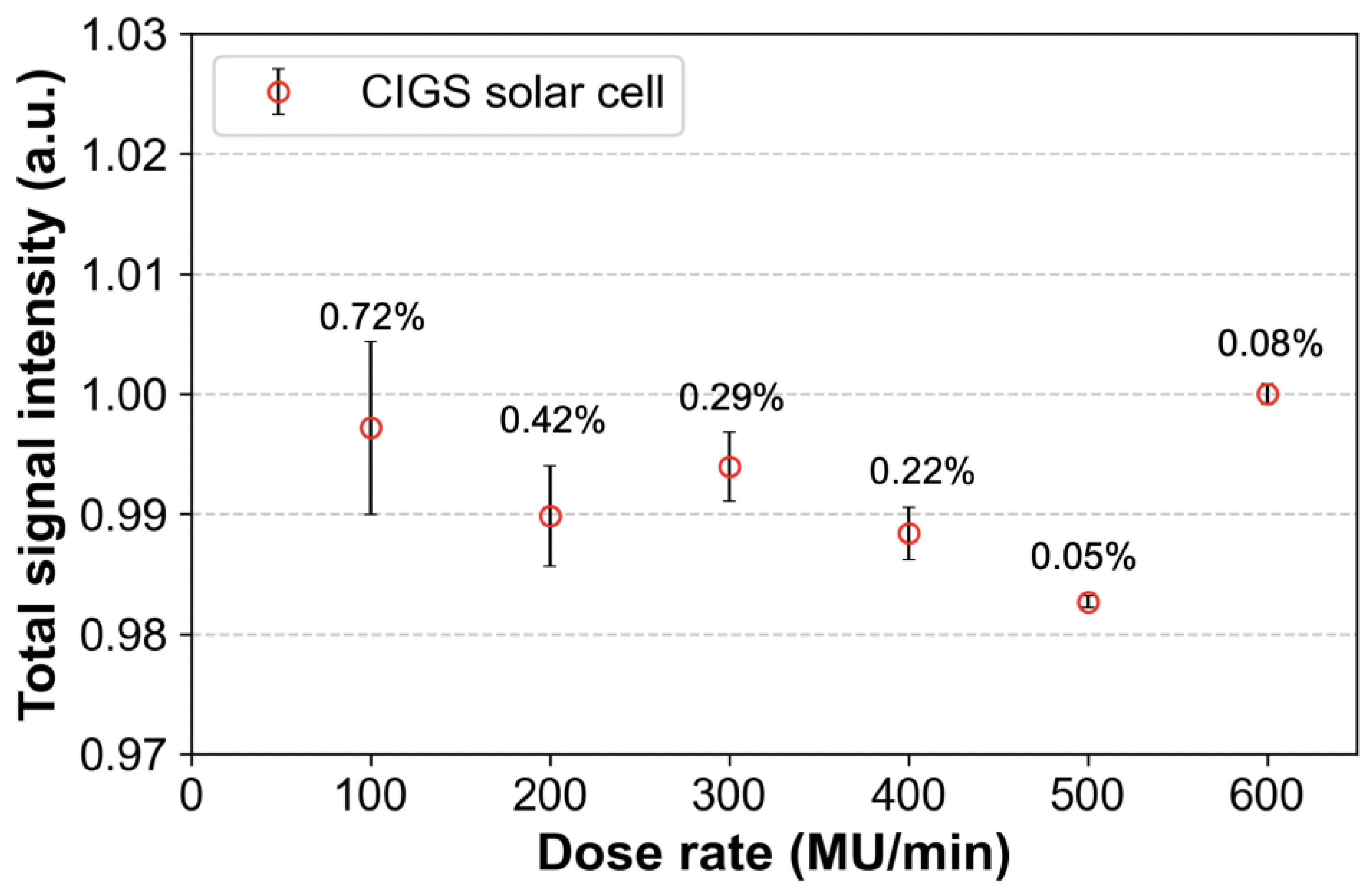
2.2.3. Dose Rate Independence
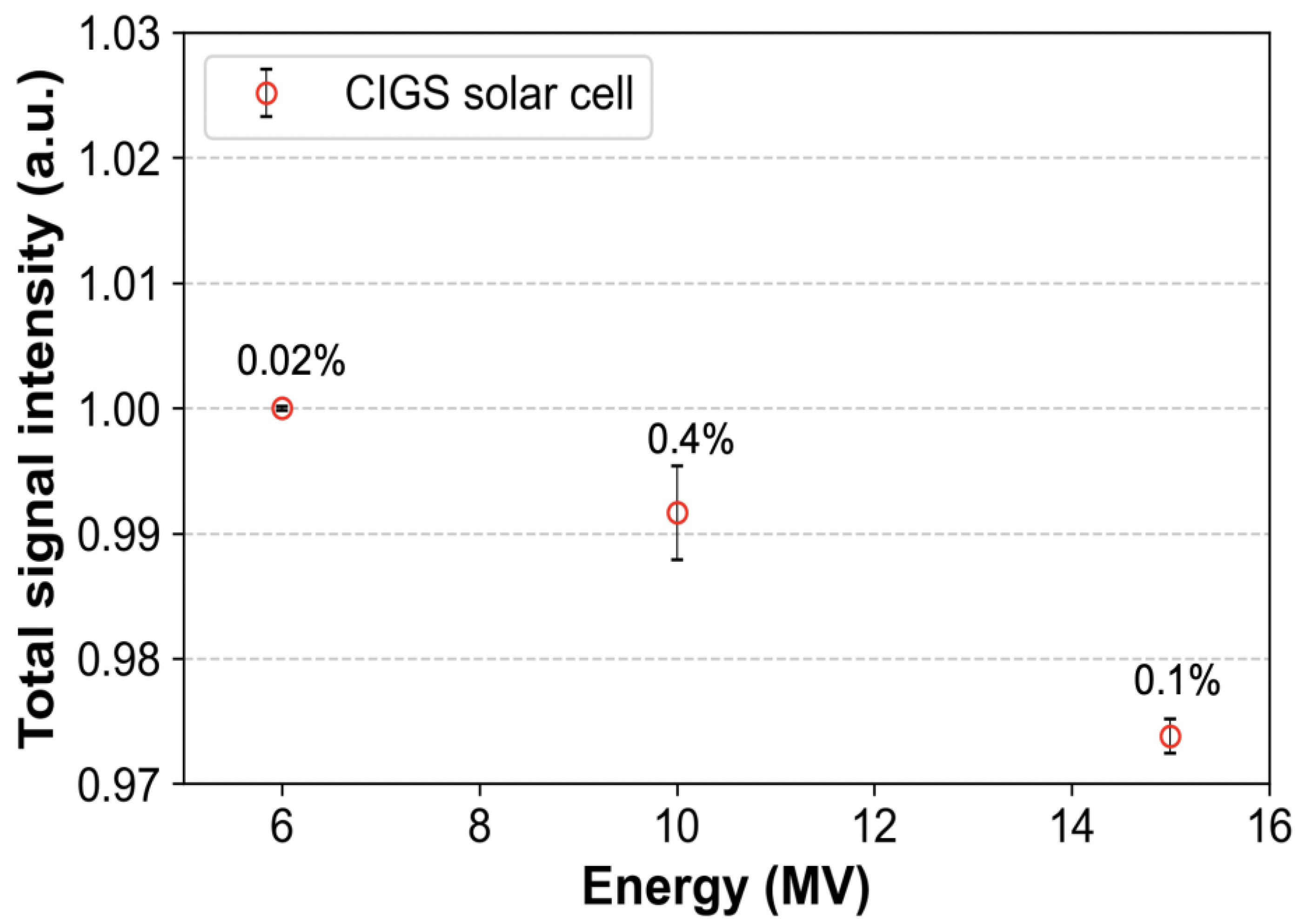
2.2.4. Energy Independence
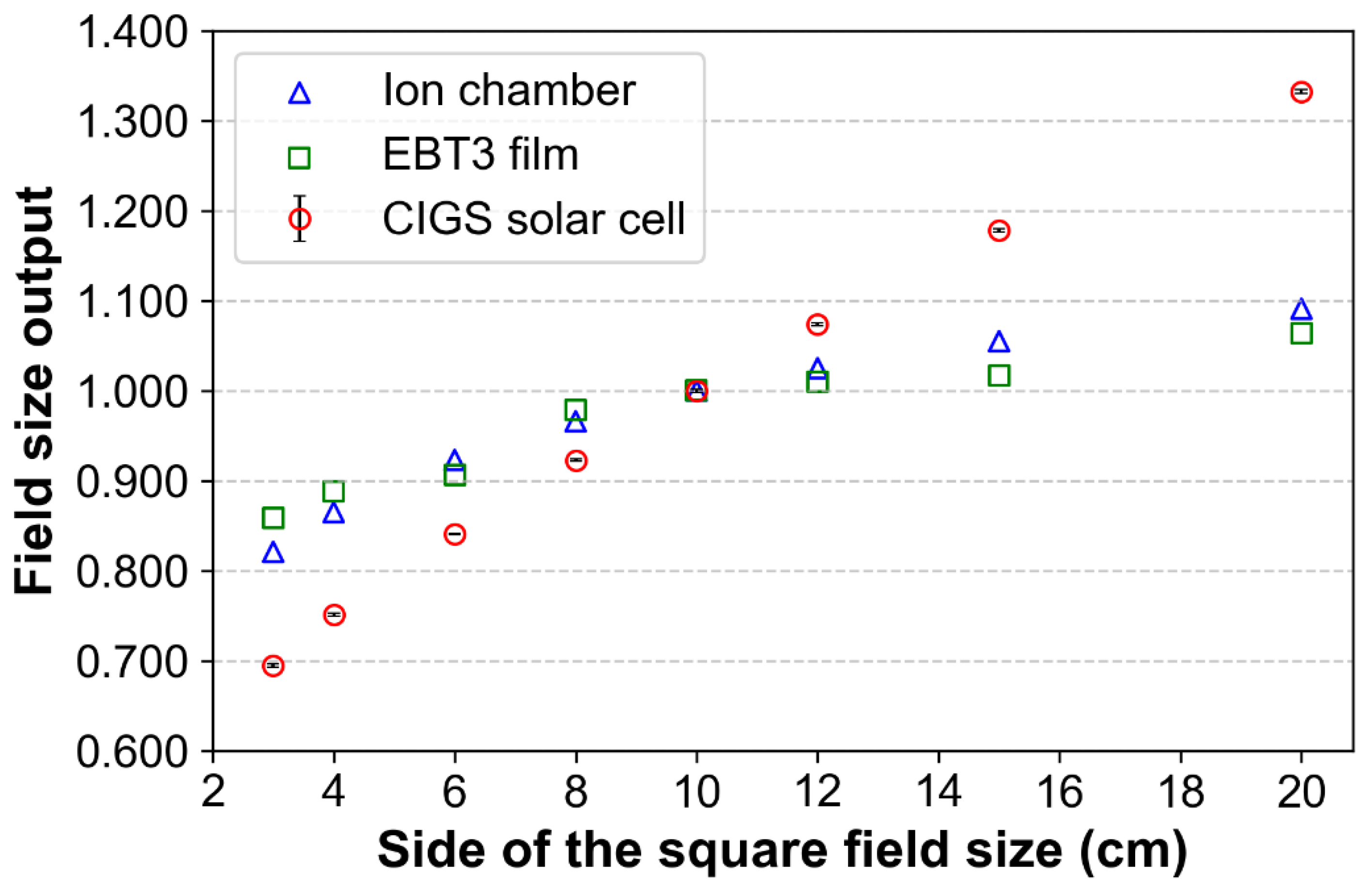
2.2.5. Field Size Output
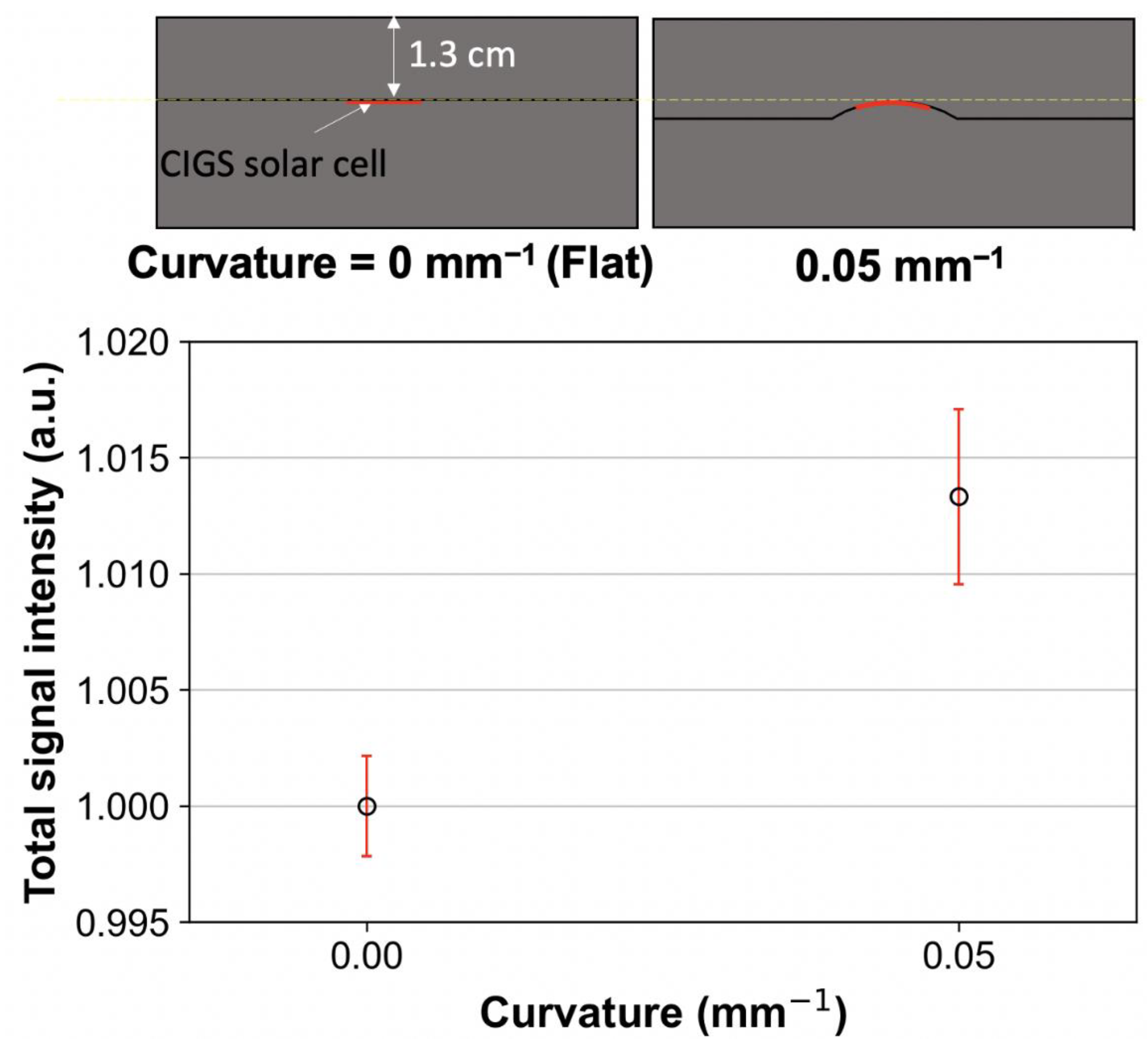
2.2.6. Flexibility Test
3. Results
3.1. Dose Linearity
3.2. Dose Rate Independence
3.3. Energy Independence
3.4. Field Size Output
3.5. Flexibility Test
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Berlangieri, A.; Elliott, S.; Wasiak, J.; Chao, M.; Foroudi, F. Use of magnetic resonance image-guided radiotherapy for breast cancer: A scoping review. J. Med. Radiat. Sci. 2022, 69, 122–133. [Google Scholar] [CrossRef] [PubMed]
- Bryce-Atkinson, A.; De Jong, R.; Marchant, T.; Whitfield, G.; Aznar, M.C.; Bel, A.; van Herk, M. Low dose cone beam CT for paediatric image-guided radiotherapy: Image quality and practical recommendations. Radiother. Oncol. 2021, 163, 68–75. [Google Scholar] [CrossRef] [PubMed]
- De Ridder, M.; Raaijmakers, C.P.J.; Pameijer, F.A.; de Bree, R.; Reinders, F.C.J.; Doornaert, P.A.H.; Terhaard, C.H.J.; Philippens, M.E.P. Target Definition in MR-Guided Adaptive Radiotherapy for Head and Neck Cancer. Cancers 2022, 14, 3027. [Google Scholar] [CrossRef] [PubMed]
- Christiansen, R.L.; Dysager, L.; Hansen, C.R.; Jensen, H.R.; Schytte, T.; Nyborg, C.J.; Bertelsen, A.S.; Agergaard, S.N.; Mahmood, F.; Hansen, S.; et al. Online adaptive radiotherapy potentially reduces toxicity for high-risk prostate cancer treatment. Radiother. Oncol. 2022, 167, 165–171. [Google Scholar] [CrossRef]
- Williams, M.V. Radiotherapy Near Misses, Incidents and Errors: Radiotherapy Incident at Glasgow. Clin. Oncol. 2007, 19, 1–3. [Google Scholar] [CrossRef]
- PSRT. Data Report on Radiotherapy Errors and Near Misses. Available online: www.gov.uk/government/publications/radiotherapy-errors-and-near-misses-data-report (accessed on 22 July 2022).
- Azzam, P.; Mroueh, M.; Francis, M.; Daher, A.A.; Zeidan, Y.H. Radiation-induced neuropathies in head and neck cancer: Prevention and treatment modalities. Ecancermedicalscience 2020, 14, 1133. [Google Scholar] [CrossRef]
- Barazzuol, L.; Coppes, R.P.; van Luijk, P. Prevention and treatment of radiotherapy-induced side effects. Mol. Oncol. 2020, 14, 1538–1554. [Google Scholar] [CrossRef]
- Voshart, D.C.; Wiedemann, J.; van Luijk, P.; Barazzuol, L. Regional Responses in Radiation-Induced Normal Tissue Damage. Cancers 2021, 13, 367. [Google Scholar] [CrossRef]
- Essers, M.; Mijnheer, B. In vivo dosimetry during external photon beam radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 1999, 43, 245–259. [Google Scholar] [CrossRef]
- Mijnheer, B.; Beddar, S.; Izewska, J.; Reft, C. In vivo dosimetry in external beam radiotherapy. Med. Phys. 2013, 40, 070903. [Google Scholar] [CrossRef]
- MacDougall, N.D.; Graveling, M.; Hansen, V.N.; Brownsword, K.; Morgan, A. In vivo dosimetry in UK external beam radiotherapy: Current and future usage. Br. J. Radiol. 2017, 90, 20160915. [Google Scholar] [CrossRef] [Green Version]
- Olaciregui-Ruiz, I.; Beddar, S.; Greer, P.; Jornet, N.; McCurdy, B.; Paiva-Fonseca, G.; Mijnheer, B.; Verhaegen, F. In vivo dosimetry in external beam photon radiotherapy: Requirements and future directions for research, development, and clinical practice. Phys. Imaging Radiat. Oncol. 2020, 15, 108–116. [Google Scholar] [CrossRef] [PubMed]
- Hwang, U.-J.; Baek, T.S.; Yoon, M. Development of Dose Verification Method for In vivo Dosimetry in External Radiotherapy. Prog. Med. Phys. 2014, 25, 23–29. [Google Scholar] [CrossRef]
- Kron, T.; Clements, N.; Aarons, Y.; Dunn, L.; Chesson, B.; Miller, J.; Roozen, K.; Ball, D. Radiochromic film for individual patient QA in extracranial stereotactic lung radiotherapy. Radiat. Meas. 2011, 46, 1920–1923. [Google Scholar] [CrossRef]
- Li, J.G.; Yan, G.; Liu, C. Comparison of two commercial detector arrays for IMRT quality assurance. J. Appl. Clin. Med. Phys. 2009, 10, 62–74. [Google Scholar] [CrossRef] [PubMed]
- Sarvari, A.; Peterlin, P.; Pernek, T. [P170] Influence of detector selection for VMAT patient QA on a gamma analysis result. Phys. Med. 2018, 52, 148. [Google Scholar] [CrossRef]
- Zhou, Y.; Sang, J.; Chen, H.; Zhu, M.; Wang, H.; Zhai, S.; Lu, L.; Liu, H.; Zhu, Z.; Hui, Z.; et al. A novel angular dependency model for MatriXX response and its application to true composite dose verification for IMRT plans. J. Appl. Clin. Med. Phys. 2021, 22, 120–135. [Google Scholar] [CrossRef]
- Guillot, M.; Beaulieu, L.; Archambault, L.; Beddar, S.; Gingras, L. A new water-equivalent 2D plastic scintillation detectors array for the dosimetry of megavoltage energy photon beams in radiation therapy. Med. Phys. 2011, 38, 6763–6774. [Google Scholar] [CrossRef]
- Son, J.; Lee, S.B.; Lim, Y.; Park, S.Y.; Cho, K.; Yoon, M.; Shin, D. Development of Optical Fiber Based Measurement System for the Verification of Entrance Dose Map in Pencil Beam Scanning Proton Beam. Sensors 2018, 18, 227. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, Y.; Warmington, L.; Gopishankar, N. Three-dimensional radiation dosimetry using polymer gel and solid radiochromic polymer: From basics to clinical applications. World J. Radiol. 2017, 9, 112–125. [Google Scholar] [CrossRef]
- Venning, A.; Mundayadan Chandroth, M.; Morgan, C.; Roberts, M. Investigation of target dose conformity using normoxic polymer gel dosimetry techniques: A clinical example of 12th thoracic vertebrae SBRT treatment with VMAT. J. Phys. Conf. Ser. 2022, 2167, 012016. [Google Scholar] [CrossRef]
- Bresciani, S.; Poli, M.; Miranti, A.; Maggio, A.; Di Dia, A.; Bracco, C.; Gabriele, P.; Stasi, M. Comparison of two different EPID-based solutions performing pretreatment quality assurance: 2D portal dosimetry versus 3D forward projection method. Phys. Med. 2018, 52, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Defoor, D.L.; Vazquez-Quino, L.A.; Mavroidis, P.; Papanikolaou, N.; Stathakis, S. Anatomy-based, patient-specific VMAT QA using EPID or MLC log files. J. Appl. Clin. Med. Phys. 2015, 16, 206–215. [Google Scholar] [CrossRef]
- Almond, P.R.; Biggs, P.J.; Coursey, B.M.; Hanson, W.F.; Huq, M.S.; Nath, R.; Rogers, D.W.O. AAPM’s TG-51 protocol for clinical reference dosimetry of high-energy photon and electron beams. Med. Phys. 1999, 26, 1847–1870. [Google Scholar] [CrossRef] [Green Version]
- IAEA TRS 398. Absorbed Dose Determination in External Beam Radiotherapy; Absorbed Dose Water IAEA: Vienna, Austria, 2000. [Google Scholar]
- Li, T.; Wu, Q.J.; Matzen, T.; Yin, F.-F.; O’Daniel, J.C. Diode-based transmission detector for IMRT delivery monitoring: A validation study. J. Appl. Clin. Med. Phys. 2016, 17, 235–244. [Google Scholar] [CrossRef] [PubMed]
- Martin, T.; Koch, A.; Nikl, M. Scintillator materials for x-ray detectors and beam monitors. MRS Bull. 2017, 42, 451–457. [Google Scholar] [CrossRef]
- Nascimento, L.F.; Verellen, D.; Goossens, J.; Struelens, L.; Vanhavere, F.; Leblans, P.; Akselrod, M. Two-dimensional real-time quality assurance dosimetry system using μ-Al2O3:C,Mg radioluminescence films. Phys. Imaging Radiat. Oncol. 2020, 16, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Kron, T.; Elliot, A.; Wong, T.; Showell, G.; Clubb, B.; Metcalfe, P. X-ray surface dose measurements using TLD extrapolation. Med. Phys. 1993, 20, 703–711. [Google Scholar] [CrossRef] [PubMed]
- Rivera, T. Thermoluminescence in medical dosimetry. Appl. Radiat. Isot. 2012, 71, 30–34. [Google Scholar] [CrossRef]
- Park, S.-Y.; Choi, C.H.; Park, J.M.; Chun, M.; Han, J.H.; Kim, J.-i. Sensitivity and stability of optically stimulated luminescence dosimeters with filled deep electron/hole traps under pre-irradiation and bleaching conditions. Phys. Med. 2017, 38, 81–87. [Google Scholar] [CrossRef]
- Jursinic, P.A. Characterization of optically stimulated luminescent dosimeters, OSLDs, for clinical dosimetric measurements. Med. Phys. 2007, 34, 4594–4604. [Google Scholar] [CrossRef] [PubMed]
- McKeever, S.W.S.; Moscovitch, M. On the advantages and disadvantages of optically stimulated luminescence dosimetry and thermoluminescence dosimetry. Radiat. Prot. Dosim. 2003, 104, 263–270. [Google Scholar] [CrossRef]
- Okazaki, T.; Hayashi, H.; Takegami, K.; Okino, H.; Kimoto, N.; Maehata, I.; Kobayashi, I. Fundamental Study of nanoDot OSL Dosimeters for Entrance Skin Dose Measurement in Diagnostic X-ray Examinations. J. Radiat. Prot. Res. 2016, 41, 229–236. [Google Scholar] [CrossRef]
- Kwan, I.S.; Rosenfeld, A.B.; Qi, Z.Y.; Wilkinson, D.; Lerch, M.L.F.; Cutajar, D.L.; Safavi-Naeni, M.; Butson, M.; Bucci, J.A.; Chin, Y.; et al. Skin dosimetry with new MOSFET detectors. Radiat. Meas. 2008, 43, 929–932. [Google Scholar] [CrossRef]
- Jong, W.L.; Wong, J.H.D.; Ung, N.M.; Ng, K.H.; Ho, G.F.; Cutajar, D.L.; Rosenfeld, A.B. Characterization of MOSkin detector for in vivo skin dose measurement during megavoltage radiotherapy. J. Appl. Clin. Med. Phys. 2014, 15, 120–132. [Google Scholar] [CrossRef]
- Kinhikar, R.A.; Murthy, V.; Goel, V.; Tambe, C.M.; Dhote, D.S.; Deshpande, D.D. Skin dose measurements using MOSFET and TLD for head and neck patients treated with tomotherapy. Appl. Radiat. Isot. 2009, 67, 1683–1685. [Google Scholar] [CrossRef]
- Choi, J.H.; Cutajar, D.; Metcalfe, P.; Downes, S. Application of MOSkin detector for in vivo dosimetry on total skin electron therapy (TSET). Biomed. Phys. Eng. Express 2018, 4, 024002. [Google Scholar] [CrossRef]
- Jornet, N.; Carrasco, P.; Jurado, D.; Ruiz, A.; Eudaldo, T.; Ribas, M. Comparison study of MOSFET detectors and diodes for entrance in vivo dosimetry in 18 MV X-ray beams. Med. Phys. 2004, 31, 2534–2542. [Google Scholar] [CrossRef] [PubMed]
- Nakano, M.; Hill, R.F.; Whitaker, M.; Kim, J.-H.; Kuncic, Z. A study of surface dosimetry for breast cancer radiotherapy treatments using Gafchromic EBT2 film. J. Appl. Clin. Med. Phys. 2012, 13, 83–97. [Google Scholar] [CrossRef]
- Devic, S.; Seuntjens, J.; Sham, E.; Podgorsak, E.B.; Schmidtlein, C.R.; Kirov, A.S.; Soares, C.G. Precise radiochromic film dosimetry using a flat-bed document scanner. Med. Phys. 2005, 32, 2245–2253. [Google Scholar] [CrossRef]
- Mijnheer, B.; Olaciregui-Ruiz, I.; Rozendaal, R.; Sonke, J.J.; Spreeuw, H.; Tielenburg, R.; van Herk, M.; Vijlbrief, R.; Mans, A. 3D EPID-based in vivo dosimetry for IMRT and VMAT. J. Phys. Conf. Ser. 2013, 444, 012011. [Google Scholar] [CrossRef]
- Celi, S.; Costa, E.; Wessels, C.; Mazal, A.; Fourquet, A.; Francois, P. EPID based in vivo dosimetry system: Clinical experience and results. J. Appl. Clin. Med. Phys. 2016, 17, 262–276. [Google Scholar] [CrossRef] [PubMed]
- Quast, U. Total body irradiation—review of treatment techniquesin Europe. Radiother. Oncol. 1987, 9, 91–106. [Google Scholar] [CrossRef]
- Chaffey, J.T.; Rosenthal, D.S.; Moloney, W.C.; Hellman, S. Total body irradiation as treatment for lymphosarcoma. Int. J. Radiat. Oncol. Biol. Phys. 1976, 1, 399–405. [Google Scholar] [CrossRef]
- Barrett, A. Total body irradiation before bone marrow transplantation: A review. Clin. Radiol. 1982, 33, 131–135. [Google Scholar] [CrossRef]
- Ramanujam, J.; Bishop, D.M.; Todorov, T.K.; Gunawan, O.; Rath, J.; Nekovei, R.; Artegiani, E.; Romeo, A. Flexible CIGS, CdTe and a-Si:H based thin film solar cells: A review. Prog. Mater. Sci. 2020, 110, 100619. [Google Scholar] [CrossRef]
- Zygmanski, P.; Abkai, C.; Han, Z.; Shulevich, Y.; Menichelli, D.; Hesser, J. Low-cost flexible thin-film detector for medical dosimetry applications. J. Appl. Clin. Med. Phys. 2014, 15, 311–326. [Google Scholar] [CrossRef]
- Jeong, S.; Cheon, W.; Shin, D.; Lim, Y.K.; Jeong, J.; Kim, H.; Yoon, M.; Lee, S.B. Development of a dosimetry system for therapeutic X-rays using a flexible amorphous silicon thin-film solar cell with a scintillator screen. Med. Phys. 2022, 49, 4768–4779. [Google Scholar] [CrossRef]
- Parsai, E.I.; Shvydka, D.; Kang, J. Design and optimization of large area thin-film CdTe detector for radiation therapy imaging applications. Med. Phys. 2010, 37, 3980–3994. [Google Scholar] [CrossRef]
- Gill, H.S.; Elshahat, B.; Kokil, A.; Li, L.; Mosurkal, R.; Zygmanski, P.; Sajo, E.; Kumar, J. Flexible perovskite based X-ray detectors for dose monitoring in medical imaging applications. Phys. Med. 2018, 5, 20–23. [Google Scholar] [CrossRef]
- Green, M.A.; Dunlop, E.D.; Hohl-Ebinger, J.; Yoshita, M.; Kopidakis, N.; Hao, X. Solar Cell Efficiency Tables (Version 58). Prog. Photovolt. 2021, 29, 657–667. [Google Scholar] [CrossRef]
- Mishra, A.K.; Shukla, R.K. Effect of humidity in the perovskite solar cell. Mater Today Proc. 2020, 29, 836–838. [Google Scholar] [CrossRef]
- Dabbabi, S.; Ben Nasr, T.; Turki Kamoun, N. CIGS Solar Cells for Space Applications: Numerical Simulation of the Effect of Traps Created by High-Energy Electron and Proton Irradiation on the Performance of Solar Cells. JOM 2019, 71, 602–607. [Google Scholar] [CrossRef]
- Jasenek, A.; Rau, U.; Weinert, K.; Kötschau, I.M.; Hanna, G.; Voorwinden, G.; Powalla, M.; Schock, H.W.; Werner, J.H. Radiation resistance of Cu(In,Ga)Se2 solar cells under 1-MeV electron irradiation. Thin Solid Film. 2001, 387, 228–230. [Google Scholar] [CrossRef]
- Weinert, K.; Jasenek, A.; Rau, U. Consequence of 3-MeV electron irradiation on the photovoltaic output parameters of Cu(In,Ga)Se2 solar cells. Thin Solid Films 2003, 431–432, 453–456. [Google Scholar] [CrossRef]
- MiaSolé Hi-Tech Corp. Flexible Solar Cell Datasheet. Available online: https://miasole.com/wp-content/uploads/2014/09/SolarCell_Datasheet_5.pdf (accessed on 24 June 2022).
- Imaizumi, M.; Okuno, Y.; Sato, S.-i.; Ohshima, T. Displacement Damage Dose Analysis on Alfa-ray Degradation of Output of a CIGS Solar Cell. In Proceedings of the 2021 IEEE 48th Photovoltaic Specialists Conference (PVSC), Online, 20–25 June 2021; pp. 1876–1879. [Google Scholar]
- Imaizumi, M.; Okuno, Y.; Takamoto, T.; Sato, S.-i.; Ohshima, T. Displacement damage dose analysis of the output characteristics of In0.5Ga0.5P and Cu(In,Ga)(S,Se)2 solar cells irradiated with alpha ray simulated helium ions. Jpn. J. Appl. Phys. 2022, 61, 044002. [Google Scholar] [CrossRef]
- Kawahara, D.; Ozawa, S.; Kimura, T.; Saito, A.; Nakashima, T.; Ohno, Y.; Murakami, Y.; Nagata, Y.; Shiinoki, T. Photon and electron backscatter dose and energy spectrum analysis around Lipiodol using flattened and unflattened beams. J. Appl. Clin. Med. Phys. 2019, 20, 178–183. [Google Scholar] [CrossRef] [PubMed]
- Khan, F.M.; Gibbons, J.P. Chapter 5: Interaction of Ionizing Radiation. In Khan’s the Physics of Radiation Therapy, 5th ed.; Wolters Kluwer: Alphen and den Rijn, The Netherlands, 2014; p. 67. [Google Scholar]
- Khan, F.M.; Gibbons, J.P. Chapter 10: A System of Dosimetric Calculations. In Khan’s the Physics of Radiation Therapy, 5th ed.; Wolters Kluwer: Alphen and den Rijn, The Netherlands, 2014; p. 152. [Google Scholar]
- Pushpavanam, K.; Narayanan, E.; Chang, J.; Sapareto, S.; Rege, K. A Colorimetric Plasmonic Nanosensor for Dosimetry of Therapeutic Levels of Ionizing Radiation. ACS Nano 2015, 9, 11540–11550. [Google Scholar] [CrossRef]
- Pushpavanam, K.; Inamdar, S.; Dutta, S.; Bista, T.; Sokolowski, T.; Boshoven, E.; Sapareto, S.; Rege, K. Determination of topographical radiation dose profiles using gel nanosensors. Sci. Adv. 2019, 5, eaaw8704. [Google Scholar] [CrossRef] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Evaluations | Experimental Variables | ||||
|---|---|---|---|---|---|
| Energy (MV) | Field Size (cm2) | Dose Rate (MU/min) | Irradiated Dose (cGy) | Measurement Depth (cm) | |
| Dose linearity | 6 | 10 × 10 | 600 | 20, 50, 100, 150, 200, 300, 500, 800, and 1200 | dmax |
| Dose rate independence | 6 | 10 × 10 | 100–600 | 100 | dmax |
| Energy independence | 6, 10, and 15 | 10 × 10 | 600 | 100 | dmax |
| Field size output | 6 | From 3 × 3 to 20 × 20 | 600 | 100 | 10 |
| Flexibility test | 6 | 10 × 10 | 600 | 100 | 1.3 (in HIPS material) |
| Delivered dose (cGy) | 20 | 50 | 100 | 150 | 200 | 300 | 500 | 800 | 1200 |
| Standard deviation (cGy) | 0.01 | 0.07 | 0.08 | 0.30 | 0.33 | 0.80 | 1.07 | 0.10 | 0.70 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shin, D.-S.; Kim, T.-H.; Rah, J.-E.; Kim, D.; Yang, H.J.; Lee, S.B.; Lim, Y.K.; Jeong, J.; Kim, H.; Shin, D.; et al. Assessment of a Therapeutic X-ray Radiation Dose Measurement System Based on a Flexible Copper Indium Gallium Selenide Solar Cell. Sensors 2022, 22, 5819. https://0-doi-org.brum.beds.ac.uk/10.3390/s22155819
Shin D-S, Kim T-H, Rah J-E, Kim D, Yang HJ, Lee SB, Lim YK, Jeong J, Kim H, Shin D, et al. Assessment of a Therapeutic X-ray Radiation Dose Measurement System Based on a Flexible Copper Indium Gallium Selenide Solar Cell. Sensors. 2022; 22(15):5819. https://0-doi-org.brum.beds.ac.uk/10.3390/s22155819
Chicago/Turabian StyleShin, Dong-Seok, Tae-Ho Kim, Jeong-Eun Rah, Dohyeon Kim, Hye Jeong Yang, Se Byeong Lee, Young Kyung Lim, Jonghwi Jeong, Haksoo Kim, Dongho Shin, and et al. 2022. "Assessment of a Therapeutic X-ray Radiation Dose Measurement System Based on a Flexible Copper Indium Gallium Selenide Solar Cell" Sensors 22, no. 15: 5819. https://0-doi-org.brum.beds.ac.uk/10.3390/s22155819