
Feasibility and Effects of an Immersive Virtual Reality Exergame Program on Physical Functions in Institutionalized Older Adults: A Randomized Clinical Trial



Abstract
:1. Introduction
2. Materials and Methods
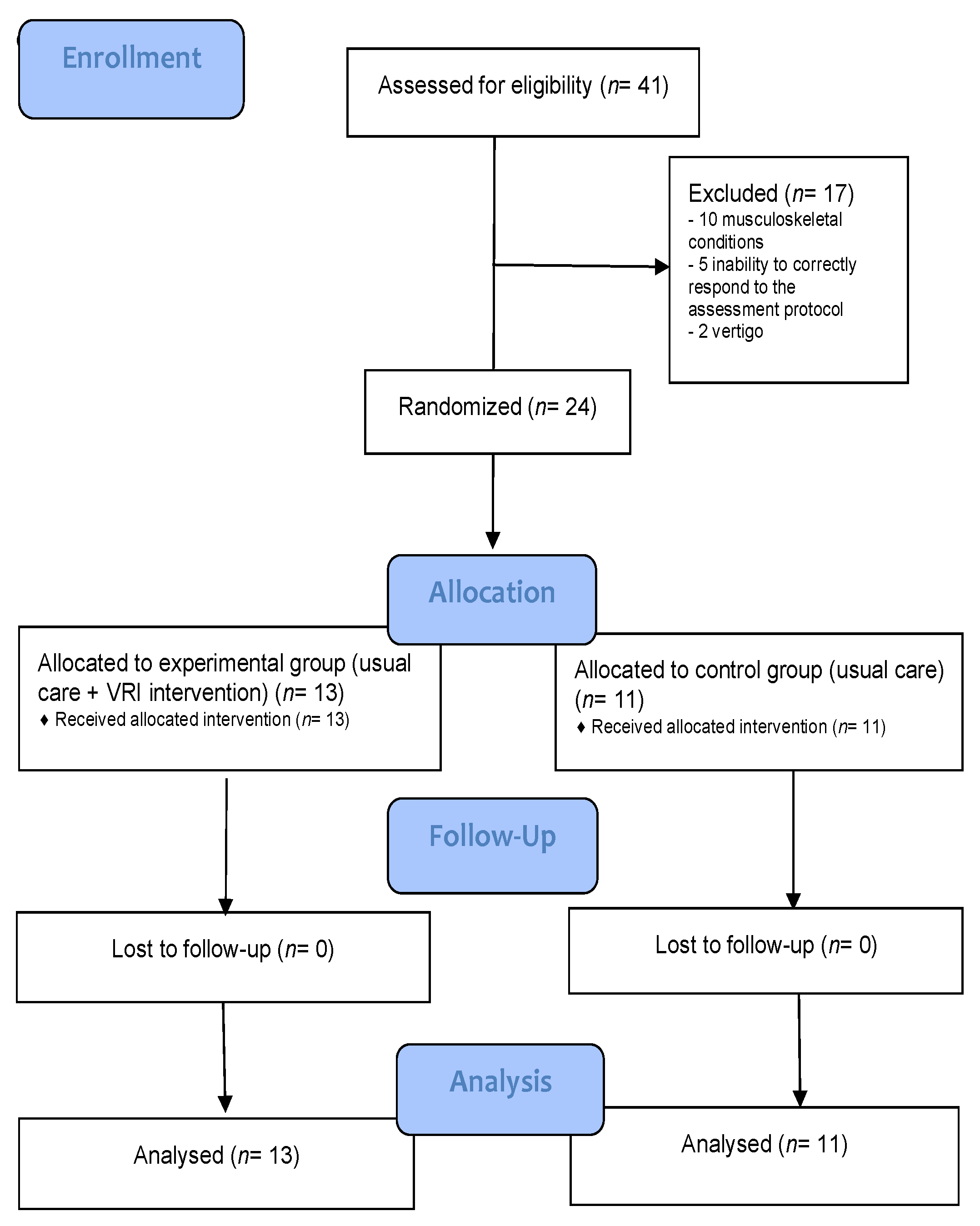
2.1. Study Design
2.2. Participants
2.3. Pre-Intervention
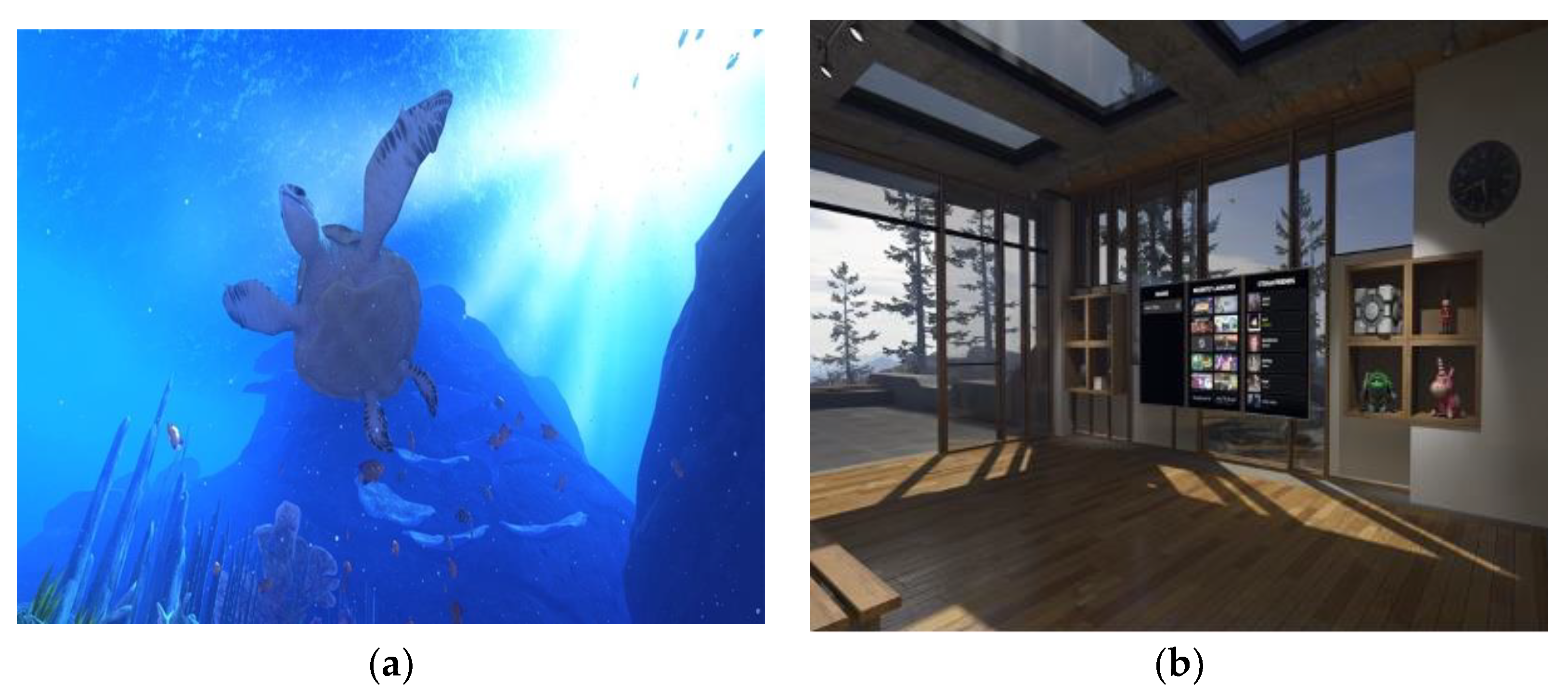
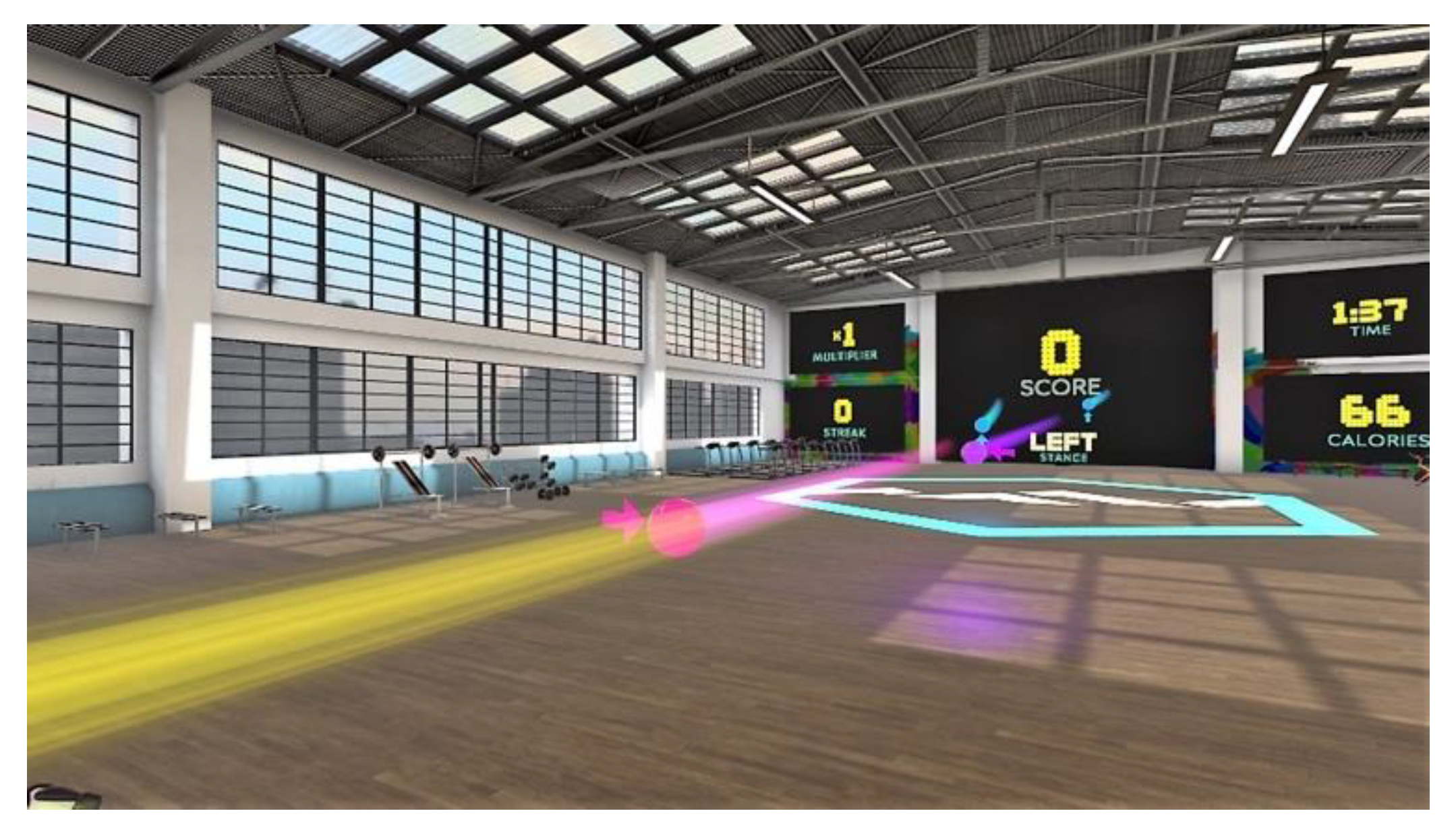
2.4. IVR Intervention
2.5. Assessments
- Physical function was assessed by balance and gait, mobility, lower limb function and handgrip strength. The balance and gait were evaluated by the Tinetti test [26]. Functional mobility and lower limb function were measured by the Timed Up and Go (TUG) test [27] and the Five times sit-to-stand test (FTSTS) [28]. Handgrip strength (HGS) was measured with an analog hand dynamometer. To perform the measurement, the participants in the stand position held the dynamometer with their dominant hand and performed the test with their elbows bent at 90 degrees. These data were collected in both groups in the pre-, post-, and follow-up evaluations.
- Quality of life (QoL) was assessed by the 12-Item Short Form Survey (SF-12), Spanish version 2 [29]. These data were collected in both groups in the pre- and post-evaluations;
- Parameters related to IVR exposure training were assessed for cybersickness, usability, post-gaming experiences, and VR sessions. Cybersickness was evaluated by the Simulator Sickness Questionnaire (SSQ), translated into and adapted for Spanish [30,31,32], usability was measured by the System Usability Scale (SUS) [33], post-gaming experiences were evaluated by Game Experience Questionnaire (GEQ-post game module) [34] and an ad hoc satisfaction questionnaire. Its development is based on the information extracted in our two published systematic reviews [35,36] It has been used in the evaluation of our previous research experiences [20,21,24,25] and was intended to assess the satisfaction of using exercise based IVR in the elderly population. Finally, the VR sessions were evaluated by the number of BOX VR sessions completed and their scores. These data were collected in the EG in intermediate and post evaluations.
2.6. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lutz, W.; Sanderson, W.; Scherbov, S.; Asia, S. The coming acceleration of global population ageing. Nature 2008, 451, 716–719. [Google Scholar] [CrossRef]
- World Health Organization. Active Ageing: A Policy Framework. 2002. Available online: https://apps.who.int/iris/handle/10.665/67215 (accessed on 25 April 2022).
- Flatt, T. A new definition of aging? Front. Genet. 2012, 3, 148. [Google Scholar] [CrossRef] [PubMed]
- Bherer, L.; Erickson, K.I.; Liu-Ambrose, T. A review of the effects of physical activity and exercise on cognitive and brain functions in older adults. J. Aging Res. 2013, 2013, 657508. [Google Scholar] [CrossRef]
- World Health Organization. World Report on Ageing and Health. 2015. Available online: https://apps.who.int/iris/handle/10.665/186463 (accessed on 25 April 2022).
- Fernández-Ballesteros, R.; Caprara, M.G.; Iñiguez, J.; García, L.F. Promoting active ageing: Effects of the “Vital living” programme. Rev. Esp. Geriatría Gerontol. 2005, 40, 92–103. [Google Scholar] [CrossRef]
- Granacher, U.; Muehlbauer, T.; Gruber, M. A qualitative review of balance and strength performance in healthy older adults: Impact for testing and training. J. Aging Res. 2012, 2012, 708905. [Google Scholar] [CrossRef]
- Gillespie, L.D.; Robertson, M.C.; Gillespie, W.J.; Sherrington, C.; Gates, S.; Clemson, L.M.; Lamb, S.E. Interventions for preventing falls in older people living in the community. Cochrane Database Syst. Rev. 2012, 9, CD007146. [Google Scholar] [CrossRef]
- Granacher, U.; Muehlbauer, T.; Zahner, L.; Gollhofer, A.; Kressig, R.W. Comparison of traditional and recent approaches in the promotion of balance and strength in older adults. Sports Med. 2011, 41, 377–400. [Google Scholar] [CrossRef]
- Donath, L.; van Dieen, J.H.; Faude, O. Exercise-based fall prevention in the elderly: What about agility? Sports Med. 2016, 46, 143–149. [Google Scholar] [CrossRef]
- Bergmann, J.; Krewer, C.; Bauer, P.; Koenig, A.; Riener, R.; Müller, F. Virtual reality to augment robot-assisted gait training in nonambulatory patients with a subacute stroke: A pilot randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2018, 54, 397–407. [Google Scholar] [CrossRef]
- Mujber, T.S.; Szecsi, T.; Hashmi, M.S.J. Virtual reality applications in manufacturing process simulation. J. Mat. Process. Technol. 2004, 156, 1834–1838. [Google Scholar] [CrossRef]
- Milgram, P.; Takemura, H.; Utsumi, A.; Kishino, F. Augmented reality: A class of displays on the reality-virtuality continuum. Telemanipulator Telepresence Technol. 1995, 2351, 282–292. [Google Scholar]
- Benham, S.; Kang, M.; Grampurohit, N. Immersive virtual reality for the management of pain in community-dwelling older adults. OTJR Occup. Particip. Health 2019, 39, 90–96. [Google Scholar] [CrossRef]
- Mora, J.C.; Valencia, W.M. Exercise and Older Adults. Clin. Geriatr. Med. 2017, 34, 145–162. [Google Scholar] [CrossRef]
- Boulos, M.N.; Yang, S.P. Exergames for health and fitness: The roles of GPS and geosocial apps. Int. J. Health Geogr. 2013, 12, 18. [Google Scholar] [CrossRef]
- Ruivo, J.A. Exergames and cardiac rehabilitation: A review. Cardiopulm. Rehabil. Prev. 2014, 34, 2–20. [Google Scholar] [CrossRef]
- Lange, B.; Koenig, S.; Chang, C.Y.; McConnell, E.; Suma, E.; Bolas, M.; Rizzo, A. Designing informed game-based rehabilitation tasks leveraging advances in virtual reality. Disabil. Rehabil. 2012, 34, 1863–1870. [Google Scholar] [CrossRef]
- Duque, G.; Boersma, D.; Loza-Diaz, G.; Hassan, S.; Suarez, H.; Geisinger, D.; Suriyaarachchi, P.; Sharma, A.; Demontiero, O. Effects of balance training using a virtual-reality system in older fallers. Clin. Interv. Aging 2013, 8, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Campo-Prieto, P.; Carral, J.M.C.; Oliveira, I.; Rodríguez-Fuentes, G. Immersive virtual reality in older people: A case study. Retos 2021, 39, 1001–1005. [Google Scholar] [CrossRef]
- Campo-Prieto, P.; Rodríguez-Fuentes, G.; Cancela-Carral, J.M. Immersive Virtual Reality Exergame Promotes the Practice of Physical Activity in Older People: An Opportunity during COVID-19. Mutimodal. Technol. Interact. 2021, 5, 52. [Google Scholar] [CrossRef]
- Cikajlo, I.; Peterlin Potisk, K. Advantages of using virtual reality based training in persons with Parkinson’s disease: A parallel study. J. NeuroEngineering Rehabil. 2019, 16, 119. [Google Scholar] [CrossRef]
- Brett, L.; Noblet, T.; Jorgensen, M.; Georgiou, A. The use of physiotherapy in nursing homes internationally: A systematic review. PLoS ONE 2019, 14, e0219488. [Google Scholar] [CrossRef]
- Campo-Prieto, P.; Rodríguez-Fuentes, G.; Cancela-Carral, J.M. Can Immersive Virtual Reality Videogames Help Parkinson’s Disease Patients? A Case Study. Sensors 2021, 21, 4825. [Google Scholar] [CrossRef]
- Campo-Prieto, P.; Cancela-Carral, J.M.; Rodríguez-Fuentes, G. Wearable Immersive Virtual Reality Device for Promoting Physical Activity in Parkinson’s Disease Patients. Sensors 2022, 22, 3302. [Google Scholar] [CrossRef] [PubMed]
- Tinetti, M.E.; Williams, T.F.; Mayewski, R. Fall risk index for elderly patients based on number of chronic disabilities. Am. J. Med. 1986, 80, 429–434. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A short physical performance battery assessing lower extremity function: Association with self-reported disability and prediction of mortality and nursing home admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef]
- Ware, J.E.; Kosinski, M.; Keller, S.D. A 12-item short form health survey. Med. Care. 1996, 34, 220–223. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, R.S.; Lane, N.E.; Berbaum, K.S.; Lilienthal, M.G. Simulator sickness questionnaire: An enhanced method for quantifying simulator sickness. Int. J. Aviat. Psychol. 1993, 3, 203–220. [Google Scholar] [CrossRef]
- Kennedy, R.S.; Drexler, J.; Kennedy, R.C. Research in visually induced motion sickness. Appl. Ergon. 2010, 41, 494–503. [Google Scholar] [CrossRef] [PubMed]
- Campo-Prieto, P.; Rodríguez-Fuentes, G.; Cancela-Carral, J.M. Translation and cross-cultural adaptation to Spanish of the Simulator Sickness Questionnaire. Retos 2021, 43, 503–509. [Google Scholar] [CrossRef]
- Brooke, J. SUS: A quick and dirty usability scale. Usability Eval. Ind. 1995, 189, 4–7. [Google Scholar]
- Ijsselsteijn, W.A.; de Kort, Y.A.W.; Poels, K. The Game Experience Questionnaire; Eindh Tech Univ Eindh: Eindhoven, The Netherlands, 2013. [Google Scholar]
- Campo-Prieto, P.; Cancela, J.M.C.; Rodríguez-Fuentes, G. Immersive virtual reality as physical therapy in older adults: Present or future (systematic review). Virtual Real. 2021, 25, 801–817. [Google Scholar] [CrossRef]
- Campo-Prieto, P.; Santos-García, D.; Cancela-Carral, J.; Rodríguez-Fuentes, G. Estado actual de la realidad virtual inmersiva como herramienta de rehabilitación física y funcional en pacientes con enfermedad de Parkinson: Revisión sistemática. Rev. Neurol. 2021, 73, 358–367. [Google Scholar] [CrossRef]
- Borg, G.A.V. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Davis, S.; Nesbitt, K.; Nalivaiko, E. A Systematic Review of Cybersickness. In Proceedings of the 2014 Conference on Interactive Entertainment-IE2014, Newcastle, Australia, 2–3 December 2014; pp. 1–9. [Google Scholar] [CrossRef]
- Mollinedo Cardalda, I.; López, A.; Cancela Carral, J.M. The effects of different types of physical exercise on physical and cognitive function in frail institutionalized older adults with mild to moderate cognitive impairment. A randomized controlled trial. Arch. Gerontol. Geriatr. 2019, 83, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Thapa, N.; Park, H.J.; Yang, J.G.; Son, H.; Jang, M.; Lee, J.; Kang, S.W.; Park, K.W.; Park, H. The Effect of a Virtual Reality-Based Intervention Program on Cognition in Older Adults with Mild Cognitive Impairment: A Randomized Control Trial. J. Clin. Med. 2020, 9, 1283. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Niksirat, K.S.; Chen, S.; Weng, D.; Sarcar, S.; Ren, X. The Impact of a Multitasking-Based Virtual Reality Motion Video Game on the Cognitive and Physical Abilities of Older Adults. Sustainability 2020, 12, 9106. [Google Scholar] [CrossRef]
- Park, J.; Yim, J. A new approach to improve cognition, muscle strength, and postural balance in community-dwelling elderly with a 3-D virtual reality kayak program. Tohoku J. Exp. Med. 2016, 238, 1. [Google Scholar] [CrossRef]
- Bohil, C.J.; Alicea, B.; Biocca, F.A. Virtual reality in neuroscience research and therapy. Nat. Rev. Neurosci. 2011, 12, 752–762. [Google Scholar] [CrossRef] [PubMed]
- Arroyo, A.; Periáñez, J.A.; Ríos-Lago, M.; Lubrini, G.; Andreo, J.; Benito-León, J.; Louis, E.D.; Romero, J.P. Components determining the slowness of information processing in parkinson’s disease. Brain Behav. 2021, 11, e02031. [Google Scholar] [CrossRef] [PubMed]
- Arroyo-Ferrer, A.; Andreo, J.; Periáñez, J.A.; Ríos-Lago, M.; Lubrini, G.; Herreros-Rodríguez, J.; García-Caldentey, J.; Romero, J.P. Computerized Simple Reaction Time and Balance in Nondemented Parkinson’s Patients. Neurodegener. Dis. 2020, 20, 193–199. [Google Scholar] [CrossRef]
- Arroyo-Ferrer, A.; Sánchez-Cuesta, F.J.; González-Zamorano, Y.; Del Castillo, M.D.; Sastre-Barrios, C.; Ríos-Lago, M.; Romero, J.P. Validation of Cognitive Rehabilitation as a Balance Rehabilitation Strategy in Patients with Parkinson’s Disease: Study Protocol for a Randomized Controlled Trial. Medicina 2021, 57, 314. [Google Scholar] [CrossRef] [PubMed]
- Cacciata, M.; Stromberg, A.; Lee, J.-A.; Sorkin, D.; Lombardo, D.; Clancy, S.; Nyamathi, A.; Evangelista, L.S. Effect of exergaming on health-related quality of life in older adults: A systematic review. Int. J. Nurs. 2019, 93, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Barsasella, D.; Liu, M.F.; Malwade, S.; Galvin, C.J.; Dhar, E.; Chang, C.C.; Li, Y.J.; Syed-Abdul, S. Effects of virtual reality sessions on the quality of life, happiness, and functional fitness among the older people: A randomized controlled trial from Taiwan. Comput Methods Programs Biomed. 2021, 200, 105892. [Google Scholar] [CrossRef] [PubMed]
- Liao, Y.Y.; Tseng, H.Y.; Lin, Y.J.; Wang, C.J.; Hsu, W.C. Using virtual reality-based training to improve cognitive function, instrumental activities of daily living and neural efficiency in older adults with mild cognitive impairment. Eur. J. Phys. Rehabil. Med. 2020, 56, 47–57. [Google Scholar] [CrossRef]
- Kim, A.; Darakjian, N.; Finley, J.M. Walking in fully immersive virtual environments: An evaluation of potential adverse effects in older adults and individuals with Parkinson’s disease. J. Neuroeng. Rehabil. 2017, 14, 16. [Google Scholar] [CrossRef]
- Trombetta, M.; Bazzanello Henrique, P.P.; Brum, M.R.; Colussi, E.L.; De Marchi, A.C.B.; Rieder RMotion Rehab, A.V.E. 3D: A VRbasedexergame for post-stroke rehabilitation. Comput. Methods Programs Biomed. 2017, 151, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Roberts, A.R.; De Schutter, B.; Franks, K.; Radina, M.E. Older adults’ experiences with audiovisual virtual reality: Perceived usefulness and other factors influencing technology acceptance. Clin. Gerontol. 2019, 42, 27–33. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Experimental Group (n = 13) | Control Group (n = 11) | ||
|---|---|---|---|
| Age (Years) | 85.08 ± 8.48 | 84.82 ± 8.10 | |
| Sex | Female (%) | 84.61 | 90.90 |
| Height (m) | 1.55 ± 0.09 | 1.49 ± 0.08 | |
| Weight (Kg) | 60.32 ± 10.53 | 61.60 ± 11.75 | |
| BMI (Kg/m2) | 25.25 ± 5.13 | 27.86 ± 4.09 | |
| Pre | Post | Follow Up | |||||
|---|---|---|---|---|---|---|---|
| EG (n = 13) | CG (n = 11) | EG (n = 13) | CG (n = 11) | EG (n = 13) | CG (n = 11) | ||
| FTSTS | 5 Sit to Stand (s) | 15.56 ± 4.52 | 21.19 ± 12.63 | 13.81 ± 3.46 | 25.57 ± 14.15 * | 17.16 ± 3.88 | 21.67 ± 10.70 |
| TINETTI | Balance | 12.38 ± 1.26 | 12.27 ± 1.95 | 14.23 ± 1.09 | 11.45 ± 1.96 * | 13.42 ± 1.44 | 12.00 ± 1.83 * |
| Gait | 10.08 ± 1.50 | 9.09 ± 2.02 | 11.07 ± 0.86 | 9.09 ± 1.57 * | 10.50 ± 1.17 | 9.10 ± 1.73 * | |
| TOTAL | 22.46 ± 2.15 | 21.36 ± 3.59 | 25.30 ± 1.65 | 20.54 ± 3.35 * | 23.92 ± 2.35 | 21.10 ± 3.38 * | |
| HGS | Handgrip (kg) | 15.54 ± 7.13 | 15.00 ± 6.35 | 20.50 ± 6.18 | 16.95 ± 5.97 | 21.08 ± 4.98 | 16.70 ± 7.09 |
| TUG | Sit to stand (s) | 2.80 ± 1.20 | 4.87 ± 2.20 * | 3.16 ± 1.88 | 5.02 ± 3.97 | 2.64 ± 1.59 | 3.79 ± 1.93 |
| Gait (s) | 4.94 ± 2.51 | 5.69 ± 3.31 | 4.77 ± 0.92 | 6.49 ± 3.30 * | 5.44 ± 3.71 | 6.45 ± 3.05 | |
| Turning (s) | 1.73 ± 0.53 | 2.46 ± 0.87 * | 2.31 ± 1.05 | 3.61 ± 3.88 | 1.88 ± 1.80 | 3.02 ± 1.34 | |
| Return Gait (s) | 4.57 ± 2.63 | 5.51 ± 2.82 | 4.87 ± 2.62 | 5.85 ± 2.17 | 4.88 ± 3.49 | 5.56 ± 3.20 | |
| Stand_to_sit (s) | 3.90 ± 1.01 | 4.71 ± 2.14 | 4.51 ± 1.79 | 5.02 ± 2.71 | 4.04 ± 1.13 | 6.54 ± 3.68 * | |
| TOTAL (s) | 17.93 ± 6.37 | 23.23 ± 9.25 | 19.00 ± 6.58 | 26.27 ± 11.77 * | 18.88 ± 9.12 | 25.36 ± 11.01 | |
| Differences between Moments (Post-Pre) | Differences between Moments (Post-Follow) | ||||||
|---|---|---|---|---|---|---|---|
| EG (n = 13) | CG (n = 11) | Manova 2 × 2 | EG (n = 13) | CG (n = 11) | Manova 2 × 2 | ||
| Dif. Post-Pre | Dif. Post-Pre | Dif. Post-Follow | Dif. Post-Follow | ||||
| FTSTS | 5 Sit to Stand (s) | 1.75 ± 3.63 | −4.38 ± 7.44 ** | F = 0.544 Sig = 0.465 | −3.96 ± 3.87 | 3.50 ± 9.53 | F = 0.016 Sig = 0.901 |
| TINETTI | Balance | 1.84 ± 1.06 ** | −0.81 ± 1.53 | F = 2.064 Sig = 0.048 | −0.75 ± 0.86 | 0.40 ± 1.17 | F = 0.503 Sig = 0.482 |
| Gait | 1.00 ± 1.08 ** | 0.01 ± 0.89 | F = 0.125 Sig = 0.725 | 0.58 ± 0.66 | 0.30 ± 1.05 | F = 0.462 Sig = 0.500 | |
| TOTAL | 2.84 ± 1.67 ** | −0.81 ± 1.99 | F = 0.397 Sig = 0.532 | −1.33 ± 1.30 | 0.10 ± 1.66 | F = 0.534 Sig = 0.469 | |
| HGS | Handgrip (kg) | 4.96 ± 4.22 ** | 1.95 ± 2.91 | F = 0.161 Sig = 0.691 | 0.33 ± 2.17 | −0.55 ± 2.43 | F = 0.930 Sig = 0.340 |
| TUG | Sit to stand (s) | −0.36 ± 1.31 | −0.15 ± 3.04 | F = 3.571 Sig = 0.045 | 0.46 ± 0.74 | 0.44 ± 2.45 | F = 0.048 Sig = 0.828 |
| Gait (s) | 0.16 ± 2.52 | −0.79 ± 4.05 | F = 0.248 Sig = 0.621 | −0.67 ± 3.55 | 0.43 ± 1.75 | F = 0.461 Sig = 0.501 | |
| Turning (s) | −0.58 ± 1.27 | −1.15 ± 3.48 | F = 0.340 Sig = 0.563 | 0.47 ± 2.05 | 0.50 ± 1.45 | F = 1.349 Sig = 0.252 | |
| Return Gait (s) | −0.29 ± 1.63 | −0.33 ± 1.71 | F = 0.928 Sig = 0.341 | −0.08 ± 2.08 | 0.072 ± 1.88 | F = 0.261 Sig = 0.612 | |
| Stand_to_sit (s) | −0.60 ± 1.77 | −0.31 ± 2.43 | F = 0.428 Sig = 0.516 | 0.32 ± 1.37 | −2.15 ± 2.54 | F = 0.519 Sig = 0.475 | |
| TOTAL (s) | −1.06 ± 4.23 | −3.03 ± 4.62 | F = 0.753 Sig = 0.390 | −0.17 ± 5.62 | 1.56 ± 5.42 | F = 0.203 Sig = 0.655 | |
| Pre | Post | ||||
|---|---|---|---|---|---|
| EG (n = 13) | CG (n = 11) | EG (n = 13) | CG (n = 11) | ||
| SF-12 | Physical Score | 48.81 ± 9.45 | 42.06 ± 12.71 | 48.52 ± 9.01 | 44.41 ± 9.88 |
| Mental Score | 48.81 ± 8.70 | 50.39 ± 10.47 | 53.41 ± 8.65 | 55.16 ± 9.53 | |
| Differences between Moments (Post-Pre) | ||||
|---|---|---|---|---|
| EG (n = 13) | CG (n = 11) | Manova 2 × 2 | ||
| Dif. Post-Pre | Dif. Post-Pre | |||
| SF-12 | Physical Score | −0.29 ± 6.26 | 2.34 ± 13.09 | F = 2.677 Sig = 0.019 |
| Mental Score | 4.60 ± 8.38 | 4.76 ± 13.95 | F = 0.114 Sig = 0.738 | |
| EG (n = 13) | |||
|---|---|---|---|
| Intermediate | Post | ||
| Simulator Sickness Questionnaire | No symptoms | No symptoms | |
| System Usability Scale | 76.73 ± 10.77 | 73.96 ± 16.77 | |
| Game Experience Questionnaire (post game module) | PE (0–4) | 2.77 ± 0.68 | 2.87 ± 0.86 |
| NE (0–4) | 0.15 ± 0.29 | 0.22 ± 0.21 | |
| T (0–4) | 0.35 ± 0.37 | 0.37 ± 0.43 | |
| RR (0–4) | 0.33 ± 0.45 | 0.19 ± 0.33 | |
| Experimental Group (n = 13) | |||
|---|---|---|---|
| n | % | ||
| How did you find the experience? | Good or very good | 13 | 100% |
| What did you like the most? | Everything | 6 | 54.54% |
| The exercise I did without realizing | 2 | 18.18% | |
| What I saw in the virtual world | 2 | 18.18% | |
| Nothing in particular | 1 | 9.09% | |
| Following a routine | 1 | 9.09% | |
| Completing the program | 1 | 9.09% | |
| Was there anything you did not like? | No | 10 | 72.73% |
| Initial fear due to not knowing what to expect | 2 | 18.18% | |
| Difficulties in use | 1 | 9.09% | |
| Would you recommend the IVR experience? | Yes | 11 | 81.82% |
| No | 2 | 18.18% | |
| Do you think this could be useful for people of your age? Why? | Yes “You exercise your mental agility and many other things that we need” ”It is energizing” “It is fundamental to remain active” “To do exercise” “It´s important for people of my age to move” “You get more agile, amongst other benefits” “You learn new things” “It encourages you to do exercise” “It helps you see and feel things that you would not feel on your own” “It is a good way to exercise, even if it is a little difficult at first” | 11 | 81.82% |
| No “I don´t find it interesting” “I don´t find it useful” | 2 | 18.18% | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campo-Prieto, P.; Cancela-Carral, J.M.; Rodríguez-Fuentes, G. Feasibility and Effects of an Immersive Virtual Reality Exergame Program on Physical Functions in Institutionalized Older Adults: A Randomized Clinical Trial. Sensors 2022, 22, 6742. https://0-doi-org.brum.beds.ac.uk/10.3390/s22186742
Campo-Prieto P, Cancela-Carral JM, Rodríguez-Fuentes G. Feasibility and Effects of an Immersive Virtual Reality Exergame Program on Physical Functions in Institutionalized Older Adults: A Randomized Clinical Trial. Sensors. 2022; 22(18):6742. https://0-doi-org.brum.beds.ac.uk/10.3390/s22186742
Chicago/Turabian StyleCampo-Prieto, Pablo, José Mª Cancela-Carral, and Gustavo Rodríguez-Fuentes. 2022. "Feasibility and Effects of an Immersive Virtual Reality Exergame Program on Physical Functions in Institutionalized Older Adults: A Randomized Clinical Trial" Sensors 22, no. 18: 6742. https://0-doi-org.brum.beds.ac.uk/10.3390/s22186742