
Caregivers’ Profiles Based on the Canadian Occupational Performance Measure for the Adoption of Assistive Technologies
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure and Ethics
2.3. Materials
2.4. Design
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gallego-Alberto, L.; Losada, A.; Cabrera, I.; Romero-Moreno, R.; Pérez-Miguel, A.; Pedroso-Chaparro, M.D.S.; Márquez-González, M. “I Feel Guilty”. Exploring Guilt-Related Dynamics in Family Caregivers of People with Dementia. Clin. Gerontol. 2020, 45, 1–10. [Google Scholar] [CrossRef]
- Wells, J.L.; Hua, A.Y.; Levenson, R.W. Poor Disgust Suppression Is Associated with Increased Anxiety in Caregivers of People with Neurodegenerative Disease. J. Gerontol. Ser. B 2020, 76, gbaa056. [Google Scholar] [CrossRef]
- Hu, P.; Yang, Q.; Kong, L.; Hu, L.; Zeng, L. Relationship between the Anxiety/Depression and Care Burden of the Major Caregiver of Stroke Patients. Medicine (Baltimore) 2018, 97, e12638. [Google Scholar] [CrossRef]
- del-Pino-Casado, R.; Espinosa-Medina, A.; López-Martínez, C.; Orgeta, V. Sense of Coherence, Burden and Mental Health in Caregiving: A Systematic Review and Meta-Analysis. J. Affect. Disord. 2019, 242, 14–21. [Google Scholar] [CrossRef]
- Behera, C.K.; Condell, J.; Dora, S.; Gibson, D.S.; Leavey, G. State-of-the-Art Sensors for Remote Care of People with Dementia during a Pandemic: A Systematic Review. Sensors 2021, 21, 4688. [Google Scholar] [CrossRef]
- Stavropoulos, T.G.; Papastergiou, A.; Mpaltadoros, L.; Nikolopoulos, S.; Kompatsiaris, I. IoT Wearable Sensors and Devices in Elderly Care: A Literature Review. Sensors 2020, 20, 2826. [Google Scholar] [CrossRef]
- Sardella, A.; Lenzo, V.; Alibrandi, A.; Catalano, A.; Corica, F.; Quattropani, M.C.; Basile, G. A Clinical Bridge between Family Caregivers and Older Adults: The Contribution of Patients’ Frailty and Optimism on Caregiver Burden. Int. J. Environ. Res. Public Health 2021, 18, 3406. [Google Scholar] [CrossRef]
- Edwards, M. Family Caregivers for People with Dementia and the Role of Occupational Therapy. Phys. Occup. Ther. Geriatr. 2015, 33, 220–232. [Google Scholar] [CrossRef]
- Cohen, C.A.; Colantonio, A.; Vernich, L. Positive Aspects of Caregiving: Rounding out the Caregiver Experience. Int. J. Geriatr. Psychiatry 2002, 17, 184–188. [Google Scholar] [CrossRef]
- Moret-Tatay, C.; Beneyto-Arrojo, M.J.; Gutierrez, E.; Boot, W.R.; Charness, N. A Spanish Adaptation of the Computer and Mobile Device Proficiency Questionnaires (CPQ and MDPQ) for Older Adults. Front. Psychol. 2019, 10, 1165. [Google Scholar] [CrossRef]
- Mitchell, L.A.; Hirdes, J.; Poss, J.W.; Slegers-Boyd, C.; Caldarelli, H.; Martin, L. Informal Caregivers of Clients with Neurological Conditions: Profiles, Patterns and Risk Factors for Distress from a Home Care Prevalence Study. BMC Health Serv. Res. 2015, 15, 350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Czaja, S.J.; Lee, C.C.; Nair, S.N.; Sharit, J. Older Adults and Technology Adoption. Proc. Hum. Factors Ergon. Soc. Annu. Meet. 2008, 52, 139–143. [Google Scholar] [CrossRef]
- University of Michigan; Bagozzi, R. The Legacy of the Technology Acceptance Model and a Proposal for a Paradigm Shift. J. Assoc. Inf. Syst. 2007, 8, 244–254. [Google Scholar] [CrossRef]
- Venkatesh, V.; Morris, M.G.; Davis, G.B.; Davis, F.D. Davis User Acceptance of Information Technology: Toward a Unified View. MIS Q. 2003, 27, 425. [Google Scholar] [CrossRef] [Green Version]
- Chi, N.-C.; Demiris, G. A Systematic Review of Telehealth Tools and Interventions to Support Family Caregivers. J. Telemed. Telecare 2015, 21, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Dai, B.; Larnyo, E.; Tetteh, E.A.; Aboagye, A.K.; Musah, A.-A.I. Factors Affecting Caregivers’ Acceptance of the Use of Wearable Devices by Patients With Dementia: An Extension of the Unified Theory of Acceptance and Use of Technology Model. Am. J. Alzheimer’s Dis. Other Dement. 2020, 35, 153331751988349. [Google Scholar] [CrossRef] [Green Version]
- Dauphinot, V.; Delphin-Combe, F.; Mouchoux, C.; Dorey, A.; Bathsavanis, A.; Makaroff, Z.; Rouch, I.; Krolak-Salmon, P. Risk Factors of Caregiver Burden Among Patients with Alzheimer’s Disease or Related Disorders: A Cross-Sectional Study. J. Alzheimers Dis. 2015, 44, 907–916. [Google Scholar] [CrossRef] [Green Version]
- Ferrara, M.; Langiano, E.; Di Brango, T.; De Vito, E.; Di Cioccio, L.; Bauco, C. Prevalence of Stress, Anxiety and Depression in with Alzheimer Caregivers. Health Qual. Life Outcomes 2008, 6, 93. [Google Scholar] [CrossRef] [Green Version]
- Carswell, A.; McColl, M.A.; Baptiste, S.; Law, M.; Polatajko, H.; Pollock, N. The Canadian Occupational Performance Measure: A Research and Clinical Literature Review. Can. J. Occup. Ther. 2004, 71, 210–222. [Google Scholar] [CrossRef]
- McColl, M.A.; Law, M.; Baptiste, S.; Pollock, N.; Carswell, A.; Polatajko, H.J. Targeted Applications of the Canadian Occupational Performance Measure. Can. J. Occup. Ther. 2005, 72, 298–300. [Google Scholar] [CrossRef]
- Vollmer Dahlke, D.; Ory, M.G. Emerging Issues of Intelligent Assistive Technology Use Among People With Dementia and Their Caregivers: A U.S. Perspective. Front. Public Health 2020, 8, 191. [Google Scholar] [CrossRef] [PubMed]
- Graff, M.J.L.; Vernooij-Dassen, M.J.M.; Zajec, J.; Olde-Rikkert, M.G.M.; Hoefnagels, W.H.L.; Dekker, J. How Can Occupational Therapy Improve the Daily Performance and Communication of an Older Patient with Dementia and His Primary Caregiver?: A Case Study. Dementia 2006, 5, 503–532. [Google Scholar] [CrossRef]
- Demers, L.; Fuhrer, M.J.; Jutai, J.; Lenker, J.; Depa, M.; De Ruyter, F. A Conceptual Framework of Outcomes for Caregivers of Assistive Technology Users. Am. J. Phys. Med. Rehabil. 2009, 88, 645–655. [Google Scholar] [CrossRef] [PubMed]
- García-Mochón, L.; Peña-Longobardo, L.M.; del Río-Lozano, M.; Oliva-Moreno, J.; Larrañaga-Padilla, I.; García-Calvente, M.D.M. Determinants of Burden and Satisfaction in Informal Caregivers: Two Sides of the Same Coin? The CUIDAR-SE Study. Int. J. Environ. Res. Public Health 2019, 16, 4378. [Google Scholar] [CrossRef] [Green Version]
- Vázquez-Sánchez, M.Á.; Aguilar-Trujillo, M.P.; Estébanez-Carvajal, F.M.; Casals-Vázquez, C.; Casals-Sánchez, J.L.; Heras-Pérez, M.C. Influencia de los pensamientos disfuncionales en la sobrecarga de los cuidadores de personas dependientes. Enferm. Clínica 2012, 22, 11–17. [Google Scholar] [CrossRef]
- Dombestein, H.; Norheim, A.; Lunde Husebø, A.M. Understanding Informal Caregivers’ Motivation from the Perspective of Self-determination Theory: An Integrative Review. Scand. J. Caring Sci. 2020, 34, 267–279. [Google Scholar] [CrossRef]
- Park, M.; Choi, S.; Lee, S.J.; Kim, S.H.; Kim, J.; Go, Y.; Lee, D.Y. The Roles of Unmet Needs and Formal Support in the Caregiving Satisfaction and Caregiving Burden of Family Caregivers for Persons with Dementia. Int. Psychogeriatr. 2018, 30, 557–567. [Google Scholar] [CrossRef]
- Fergusson, D.M.; McLeod, G.F.H.; Horwood, L.J.; Swain, N.R.; Chapple, S.; Poulton, R. Life Satisfaction and Mental Health Problems (18 to 35 Years). Psychol. Med. 2015, 45, 2427–2436. [Google Scholar] [CrossRef] [PubMed]
- Abrahamson, K.; Myers, J.; Nazir, A. Implementation of a Person-Centered Medical Care Model in a Skilled Nursing Facility: A Pilot Evaluation. J. Am. Med. Dir. Assoc. 2017, 18, 539–543. [Google Scholar] [CrossRef]
- Etemadifar, S.; Heidari, M.; Jivad, N.; Masoudi, R. Effects of Family-Centered Empowerment Intervention on Stress, Anxiety, and Depression among Family Caregivers of Patients with Epilepsy. Epilepsy Behav. 2018, 88, 106–112. [Google Scholar] [CrossRef]
- Corvol, A.; Netter, A.; Campeon, A.; Somme, D. Implementation of an Occupational Therapy Program for Alzheimer’s Disease Patients in France: Patients’ and Caregivers’ Perspectives. J. Alzheimers Dis. 2018, 62, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Bianchini, E.; Della Gatta, F.; Virgilio, M.; Alborghetti, M.; Salvetti, M.; Giubilei, F.; Pontieri, F.E. Validation of the Canadian Occupational Performance Measure in Italian Parkinson’s Disease Clients. Phys. Occup. Ther. Geriatr. 2021, 40, 1–12. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
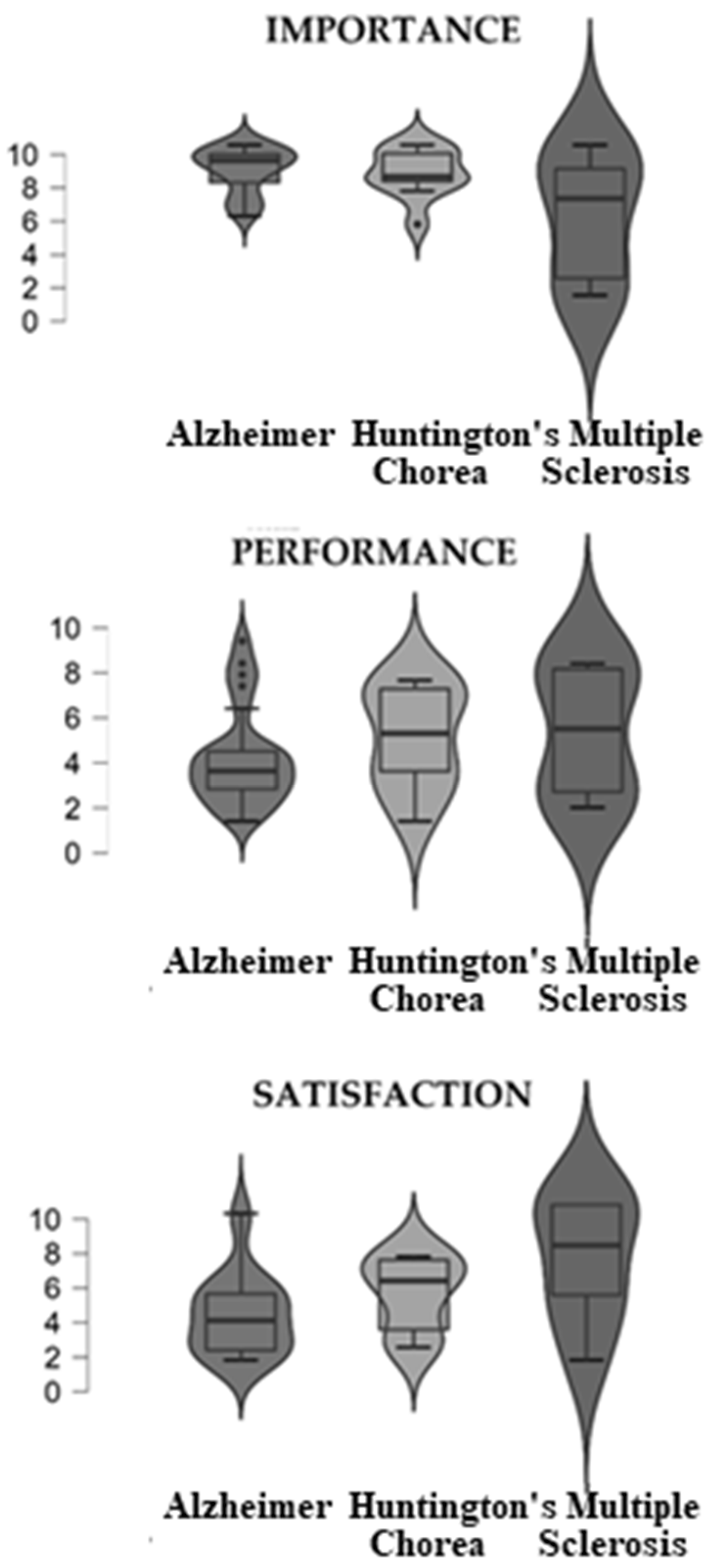
| COPM | Pathology | Mean | SD | p |
|---|---|---|---|---|
| Importance | Alzheimer | 8.52 | 1.37 | 0.29 |
| Huntington’s Chorea | 8.34 | 1.46 | ||
| Multiple Sclerosis | 5.70 | 4.00 | ||
| Total | 7.70 | 2.12 | ||
| Performance | Alzheimer | 3.82 | 2.18 | 0.55 |
| Huntington’s Chorea | 4.72 | 2.27 | ||
| Multiple Sclerosis | 4.97 | 3.03 | ||
| Total | 4.74 | 2.36 | ||
| Satisfaction | Alzheimer | 3.64 | 2.36 | 0.04 |
| Huntington’s Chorea | 4.89 | 2.16 | ||
| Multiple Sclerosis | 6.82 | 3.78 | ||
| Total | 4.90 | 2.51 |
| Comparison | z | Wi | Wj | p | pbonf | pholm |
|---|---|---|---|---|---|---|
| 1–2 | −1.686 | 16.938 | 24.350 | 0.046 | 0.138 | 0.092 |
| 1–3 | −2.138 | 16.938 | 28.333 | 0.016 | 0.049 | 0.049 |
| 2–3 | −0.661 | 24.350 | 28.333 | 0.254 | 0.763 | 0.254 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gatta, F.D.; Fabrizi, E.; Giubilei, F.; Grau, M.D.; Moret-Tatay, C. Caregivers’ Profiles Based on the Canadian Occupational Performance Measure for the Adoption of Assistive Technologies. Sensors 2022, 22, 7500. https://0-doi-org.brum.beds.ac.uk/10.3390/s22197500
Gatta FD, Fabrizi E, Giubilei F, Grau MD, Moret-Tatay C. Caregivers’ Profiles Based on the Canadian Occupational Performance Measure for the Adoption of Assistive Technologies. Sensors. 2022; 22(19):7500. https://0-doi-org.brum.beds.ac.uk/10.3390/s22197500
Chicago/Turabian StyleGatta, Francesco Della, Elisa Fabrizi, Franco Giubilei, María Dolores Grau, and Carmen Moret-Tatay. 2022. "Caregivers’ Profiles Based on the Canadian Occupational Performance Measure for the Adoption of Assistive Technologies" Sensors 22, no. 19: 7500. https://0-doi-org.brum.beds.ac.uk/10.3390/s22197500