
Hybrid-Pattern Recognition Modeling with Arrhythmia Signal Processing for Ubiquitous Health Management

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Data Sampling
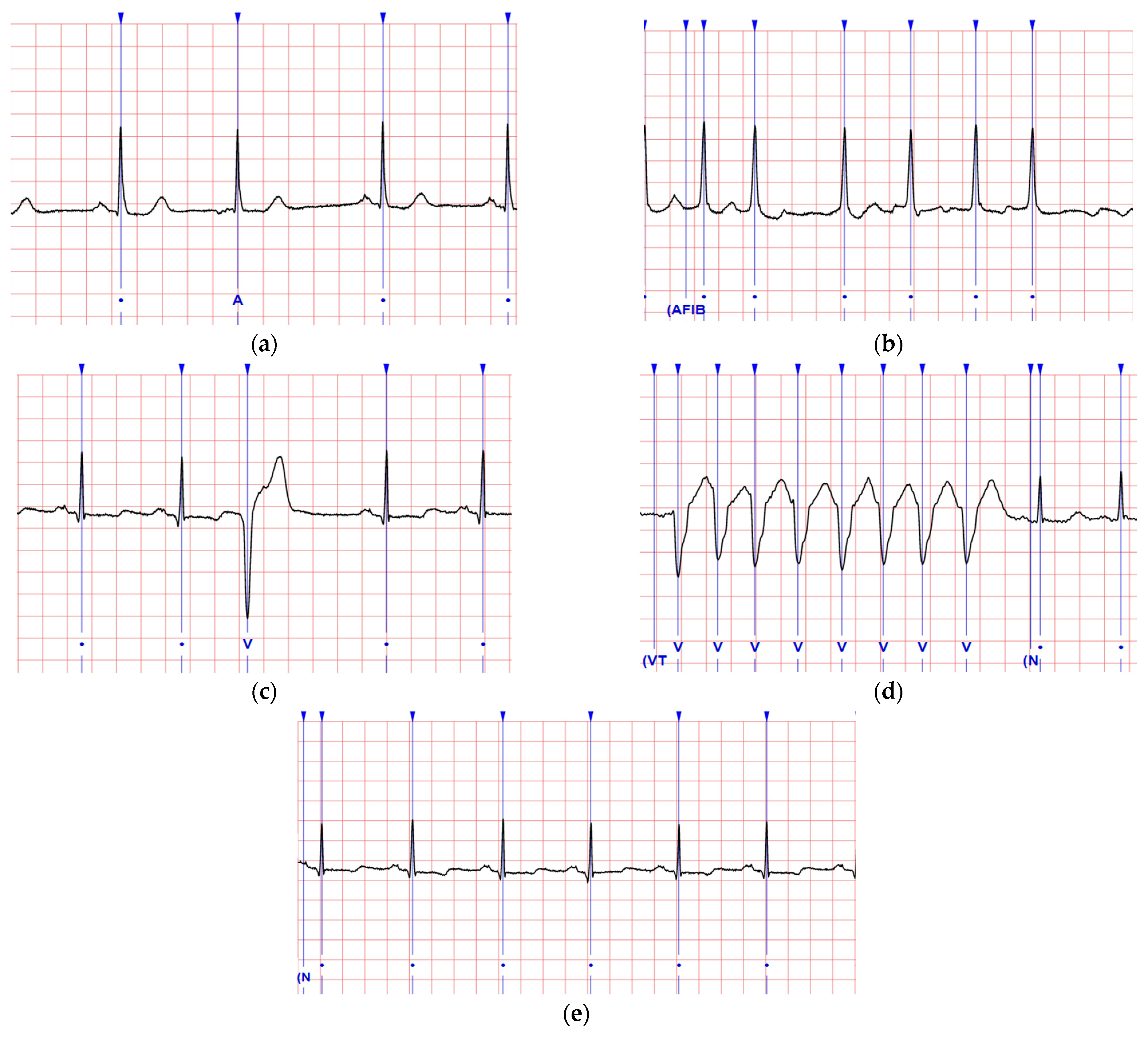
2.1.1. Normal Rhythm and Arrhythmia Symptoms
2.1.2. ECG Waveform Patterns
2.1.3. Sample Data Sets
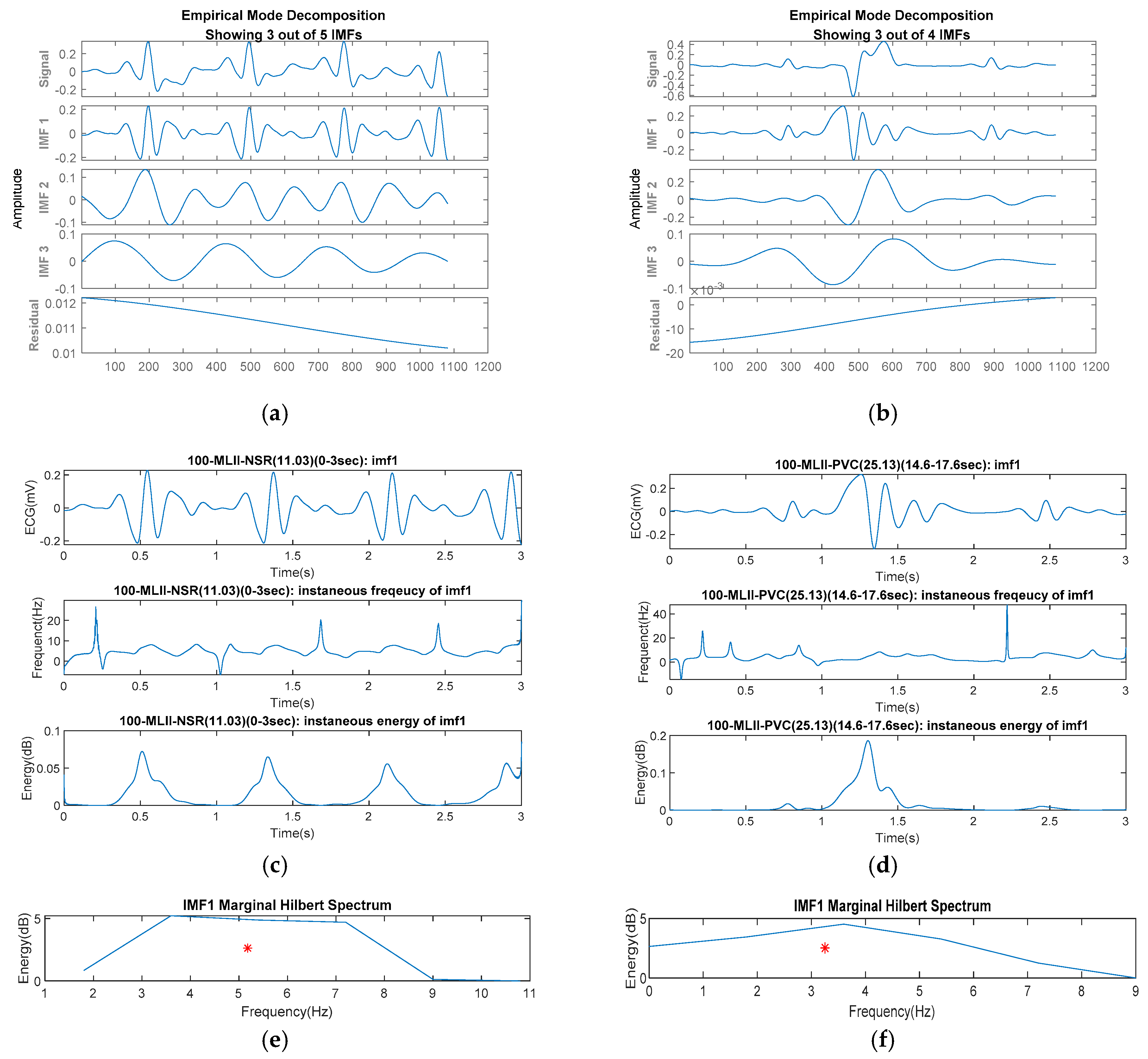
2.2. Featuring by Marginal Hilbert Spectrum
2.3. Comprehensive Machine Learning Models
2.3.1. Multiple Layer Perceptron (MLP)
2.3.2. Random Forest (RF)
2.3.3. Support Vector Machine (SVM)
2.3.4. Naive Bayes (NB)
2.4. UHMS Infrastructure
2.4.1. Runtime Server Architecture in Modeling Tier
2.4.2. Pattern Repository Design in Recognition Tier
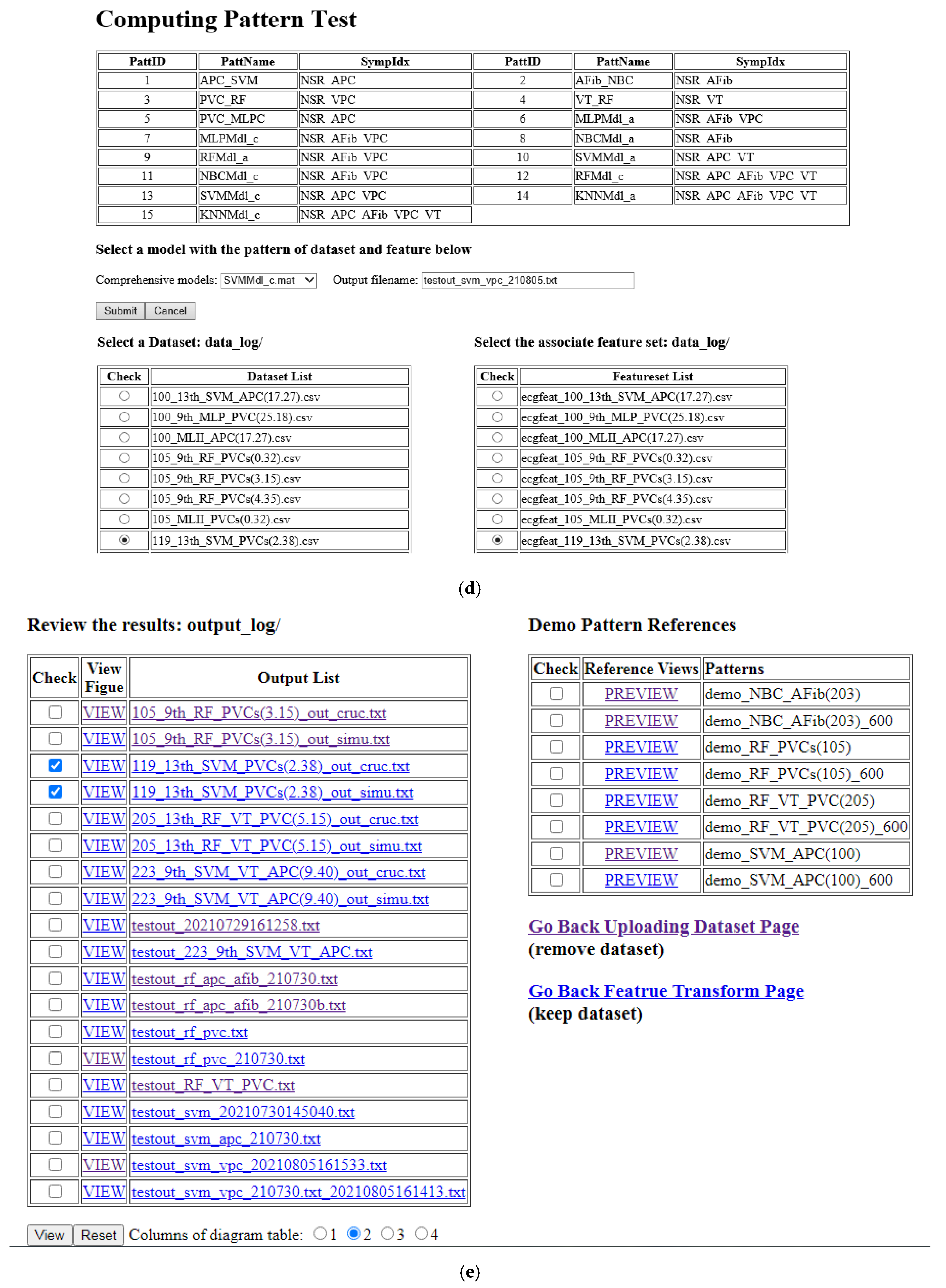
2.4.3. UHM Portals in Management Tier
3. Results
3.1. Pre-Processing Analysis
3.2. Modeling Evaluation
Sensitivity = TP/(TP + FN) = TPR (i.e., true positive rate)
Specificity = 1 − FP/(FP + TN) = 1 − FPR (i.e., false positive rate)
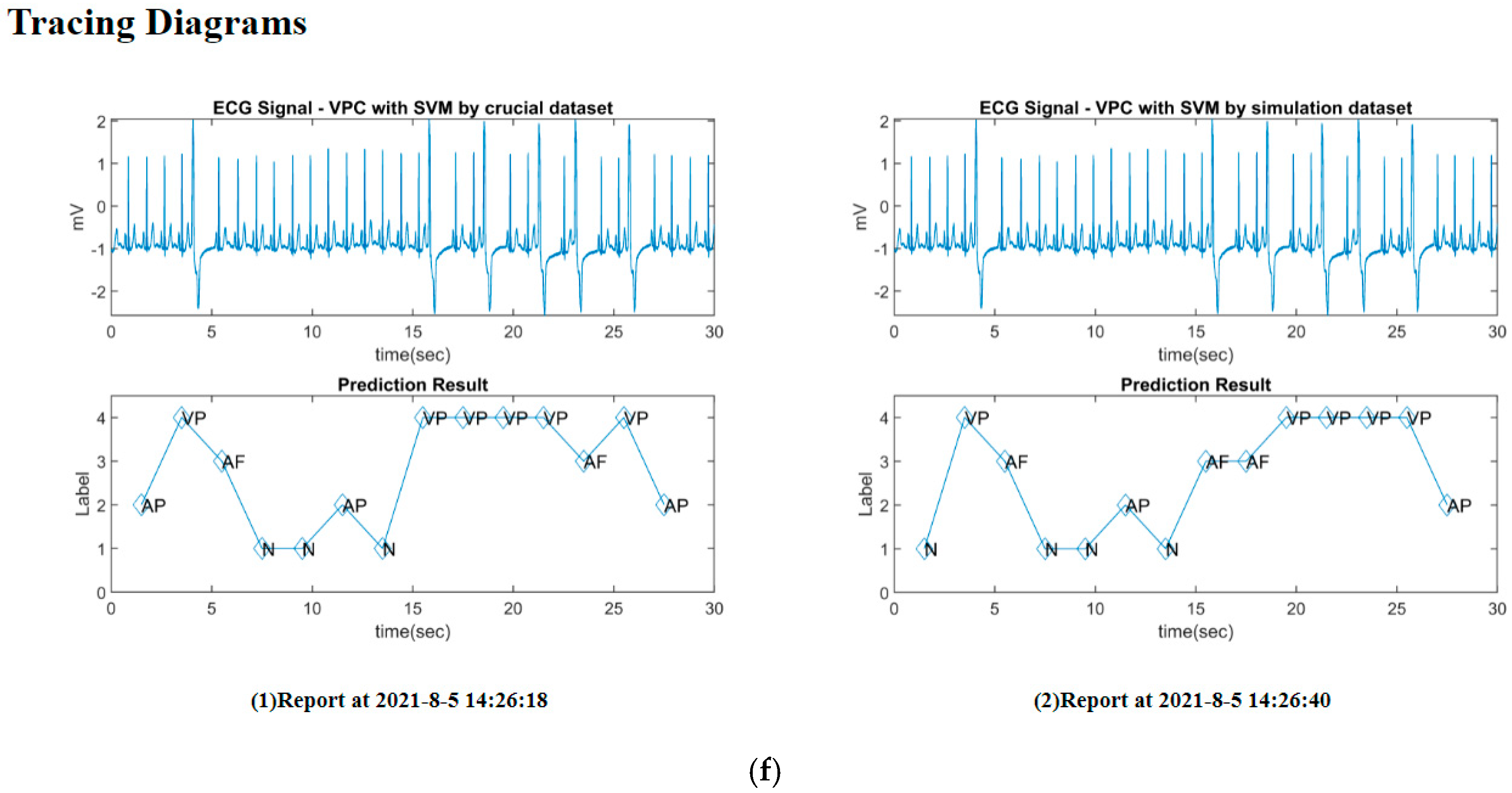
3.3. Implementation
4. Discussion
4.1. Principal Finding
- (1)
- Candidate features can be extracted from the first three-order IMFs. In the analysis, we used the low-pass filter to remove noises from the ECG signals before the EMD process. The past study employed this process with the SVM to achieve good performance for recognizing the APC and VPC [20]. As inspecting the decomposed IMFs of the AFib and VT samples, the IMF1 showed the major features of the frequency and power due to the MHS-area centroid in a significant range. At the same time, IMF2 and IMF3 contributed minor characteristics with a dispersed distribution. The MHS-area centroids for the latter-order IMFs were similar for all symptoms. Therefore, the first three-order IMFs, which used to include the hybrid patterns’ recognizable features, are suggested for the candidate features.
- (2)
- Symptomatic waveforms should be wholly involved in the featuring frame. The timestamps of the arrhythmia symptoms’ interest points were annotated on the official web page [18], but they mixed with the NSR or other symptoms in a featuring frame. The impure waveforms of the symptoms may affect the features of the observed databases in this study. Therefore, the appropriate sample should involve the complete waveform of the specific symptom in the frame, which allows some NSRs to fill up the frame size and reduce the bias.
- (3)
- HHT-based data pre-processing can imply innovative features in the ML model. With EMD in the HHT, the features (i.e., MHS-area centroids for various IMFs) of the multiclass symptoms due to the limited samples were observed to scatter in a separable distribution. The simulative features can be supplemented following the mean and deviation of the observed samples for data training. The evaluation showed similar performances for AFib and VPC corresponding to NSR using the simulative data set compared to the crucial data set. However, the VPC versus AFib and VT did not reach acceptable results, since they lacked enough samples with reliable means and standard deviations for simulation. Various models with ensemble analysis can be pipelined in a suitable pattern for the diverse symptoms to achieve a good recognition in practice. Proper feature pre-processing with validation can avoid unbalanced or insufficient samples and improve training efficacy before constructing the reliable recognition model. This approach revealed the requirement of conventional AI-based analysis in which the significant features can enhance the various machine learning methods to reach good results in classification [44,45,46].
- (4)
- The coupling ML models can customize the UHMS to recognize hybrid arrhythmia patterns. The model’s parameters are adjustable for the specific feature set. The current prototype could recognize four arrhythmia symptoms for application and suggest the suitable ML models with respect to the hybrid patterns for the frequency–domain features. The user can determine the most possible symptom based on the models’ suggestion. In advance, we suggested the features in the HS for recognizing more arrhythmia diseases. The HS offers the instantaneous energy and frequency in the time–frequency domain, which also implies the time-dependent characteristics of the HRV symptoms with noticeable phase changes in the wave period. The previous study selected the features in both domains to avoid ambiguous identification for the similar waveform of ventricular arrhythmia [47]. The HS can be reflected as more features when the MHS-area centroids are not apparent than other symptoms [48].
4.2. Study Limitation
4.3. Comparison with Prior Work
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AFib | atrial fibrillation |
| APC | atrial premature atrial complex |
| AUC | area under the curve of receiver operating characteristics |
| HHT | Hilbert–Huang transform |
| MHS | marginal Hilbert spectrum |
| MLP | multiple layer perceptron |
| NB | naive Bayes |
| NSR | normal sinus rhythm |
| RF | random forest |
| ROC | receiver operating characteristics |
| SVM | support vector machine |
| VPC | ventricular premature complex |
| VT | ventricular tachycardia |
References
- Maramba, I.; Chatterjee, A.; Newman, C. Methods of usability testing in the development of eHealth applications: A scoping review. Int. J. Med. Inform. 2019, 126, 95–104. [Google Scholar] [CrossRef]
- Yang, H.; Jung, C.; Yang, S.; Kim, M.; Shim, S.; Lee, K.; Lee, H. Development and Validation of an Arterial Pressure-Based Cardiac Output Algorithm Using a Convolutional Neural Network: Retrospective Study Based on Prospective Registry Data. JMIR Med. Inf. 2021, 9, e24762. [Google Scholar] [CrossRef]
- Chu, Y.H.; Hsieh, Y.C.; Wang, C.H.; Pan, Y.C.; Chang, R.I. UPHSM: Ubiquitous personal health surveillance and management system via WSN agent on open source smartphone. In Proceedings of the 13th IEEE International Conference on e-Health Networking Applications and Services (Healthcom), Columbia, MI, USA, 13–15 June 2011; pp. 60–63. [Google Scholar] [CrossRef]
- Otto, C.; Milenkovic, A.; Sanders, C.; Jovanov, E. System architecture of a wireless body area sensor network for ubiquitous health monitoring. J. Mob. Multimed. 2006, 1, 307–326. [Google Scholar]
- Lai, Y.-C.; Kan, Y.-C.; Lin, Y.-C.; Lin, H.-C. AIoT-Enabled Rehabilitation Recognition System—Exemplified by Hybrid Lower-Limb Exercises. Sensors 2021, 21, 4761. [Google Scholar] [CrossRef] [PubMed]
- Shukla, S.; Lakhmani, A.; Agarwal, A.K. Approaches of artificial intelligence in biomedical image processing: A leading tool between computer vision & biological vision. In Proceedings of the 2016 International Conference on Advances in Computing, Communication, & Automation (ICACCA), Dehradun, India, 8–9 April 2016. [Google Scholar]
- Kotsiantis, S.B. Supervised Machine Learning: A Review of Classification Techniques. Information 2007, 31, 249–268. [Google Scholar]
- Alkeem, E.A.; Kim, S.K.; Yeun, C.Y.; Zemerly, M.J.; Poon, K.F.; Gianini, G.; Yoo, P.D. An Enhanced Electrocardiogram Biometric Authentication System Using Machine Learning. IEEE Access 2019, 7, 123069–123075. [Google Scholar] [CrossRef]
- Naghsh-Nilchi, A.R.; Aghashahi, M. Epilepsy seizure detection using eigen-system spectral estimation and Multiple Layer Perceptron neural network. Biomed. Signal Process. Control 2010, 5, 147–157. [Google Scholar] [CrossRef]
- Mohammadzadeh Asl, B.; Kamaledin Setarehdan, S.; Mohebbi, M. Support vector machine-based arrhythmia classification using reduced features of heart rate variability signal. Artif. Intell. Med. 2008, 44, 51–64. [Google Scholar]
- Breiman, L. Random Forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef] [Green Version]
- Da Luz, S.E.J.; Schwartz, W.R.; Cemara-Chevez, G.; Menottia, D. ECG-based heartbeat classification for arrhythmia detection: A survey. Comput. Methods Programs Biomed. 2016, 127, 144–164. [Google Scholar] [CrossRef]
- Chou, E.-F.; Khine, M.; Lockhart, T.; Soangra, R. Effects of ECG Data Length on Heart Rate Variability among Young Healthy Adults. Sensors 2021, 21, 6286. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.S.; Correia, M.V.; Silva, H.P. Invisible ECG for High Throughput Screening in eSports. Sensors 2021, 21, 7601. [Google Scholar] [CrossRef]
- Kim, J.; Yang, G.; Kim, J.; Lee, S.; Kim, K.K.; Park, C. Efficiently Updating ECG-Based Biometric Authentication Based on Incremental Learning. Sensors 2021, 21, 1568. [Google Scholar] [CrossRef] [PubMed]
- Jayaraman, S.; Sangareddi, V.; Periyasamy, R.; Joseph, J.; Shanmugam, R.M. Modified limb lead ECG system effects on electrocardiographic wave amplitudes and frontal plane axis in sinus rhythm subjects. Anatol. J. Cardiol. 2017, 17, 46–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McSharry, P.E.; Clifford, G.; Tarassenko, L.; Smith, L.A. A dynamical model for generating synthetic electrocardiogram signals. IEEE Trans. Biomed. Eng. 2003, 50, 289–294. [Google Scholar] [CrossRef] [Green Version]
- Moody, G.B.; Mark, R.G. The impact of the MIT-BIH Arrhythmia Database. IEEE Eng. Med. Biol. 2001, 20, 45–50. Available online: https://physionet.org/physiobank/database/mitdb/ (accessed on 12 January 2022). [CrossRef]
- Goldberger, A.L.; Amaral, L.A.N.; Glass, L.; Hausdorff, J.M.; Ivanov, P.C.; Mark, R.G.; Mietus, J.E.; Moody, G.B.; Peng, C.K.; Stanley, H.E. PhysioBank, PhysioToolkit, and PhysioNet: Components of a New Research Resource for Complex Physiologic Signals. Circulation 2003, 101, e215–e220. [Google Scholar] [CrossRef] [Green Version]
- Sahoo, S.; Mohanty, M.; Behera, S.; Sabut, S.K. ECG beat classification using empirical mode decomposition and mixture of features. J. Med. Eng. Technol. 2017, 41, 652–661. [Google Scholar] [CrossRef] [PubMed]
- Yildirim, O.; Talo, M.; Ciaccio, E.J.; Tan, R.S.; Acharya, U.R. Accurate deep neural network model to detect cardiac arrhythmia on more than 10,000 individual subject ECG records. Comput. Methods Programs Biomed. 2020, 197, 105740. [Google Scholar] [CrossRef]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [Green Version]
- Pichon, A.; Roulaud, M.; Antoine-Jonville, S.; Bisschop, C.; Denjean, A. Spectral analysis of heart rate variability: Interchangeability between autoregressive analysis and fast Fourier transform. J. Electrocardiol. 2006, 39, 31–37. [Google Scholar] [CrossRef]
- Mian Qaisar, S.; Fawad Hussain, S. Arrhythmia Diagnosis by Using Level-Crossing ECG Sampling and Sub-Bands Features Extraction for Mobile Healthcare. Sensors 2020, 20, 2252. [Google Scholar] [CrossRef] [Green Version]
- Szczepański, A.; Saeed, K. A Mobile Device System for Early Warning of ECG Anomalies. Sensors 2014, 14, 11031–11044. [Google Scholar] [CrossRef]
- Serhani, M.A.; El Kassabi, H.T.; Ismail, H.; Nujum Navaz, A. ECG Monitoring Systems: Review, Architecture, Processes, and Key Challenges. Sensors 2020, 20, 1796. [Google Scholar] [CrossRef] [Green Version]
- Huang, N.E.; Shen, S.S.P. Hilbert-Huang Transform and Its Applications; Interdisciplinary Mathematical Sciences; World Scientific: Taipei, Taiwan, 2014; Volume 16. [Google Scholar] [CrossRef]
- Wang, Y.H.; Yeh, C.H.; Young, H.W.V.; Hu, K.; Lo, M.T. On the computational complexity of the empirical mode decomposition algorithm. Phys. A Stat. Mech. Its Appl. 2014, 400, 159–167. [Google Scholar] [CrossRef]
- Hadj Slimane, Z.E.; Naet-Alib, A. QRS complex detection using Empirical Mode Decomposition. Digit. Signal. Process. 2010, 20, 1221–1228. [Google Scholar] [CrossRef]
- Hossain, M.B.; Bashar, S.K.; Walkey, A.J.; McManus, D.D.; Chon, K.H. An Accurate QRS Complex and P Wave Detection in ECG Signals Using Complete Ensemble Empirical Mode Decomposition with Adaptive Noise Approach. IEEE Access 2019, 7, 128869–128880. [Google Scholar] [CrossRef]
- Li, H.; Kwong, S.; Yang, L.; Huang, D.; Xiao, D. Hilbert-Huang Transform for analysis of heart rate variability in cardiac health. IEEE/ACM Trans. Comput. Biol. Bioinform. 2011, 8, 1557–1567. [Google Scholar] [CrossRef]
- Kuo, T.B.J.; Yang, C.C.H.; Huang, N.E. Quantification of Respiratory Sinus Arrhythmia Using Hilbert-Huang Transform. Adv. Adapt. Data Anal. 2009, 1, 295–307. [Google Scholar] [CrossRef]
- Marcus, G.M. Evaluation and management of premature ventricular complexes. Circulation 2020, 141, 1404–1408. [Google Scholar] [CrossRef]
- Parsi, A.; O’Loughlin, D.; Glavin, M.; Jones, E. Prediction of Sudden Cardiac Death in Implantable Cardioverter Defibrillators: A Review and Comparative Study of Heart Rate Variability Features. IEEE Rev. Biomed. Eng. 2020, 13, 5–16. [Google Scholar] [CrossRef]
- Segismundo, M.J.; Villanueva, M.M.F.; Zaldua, A.; Lee-Ramos, C.M. Spectrogram analysis of electrocardiogram with Normal Sinus Rhythm, Arrhythmia and Atrial Fibrillation. In Proceedings of the TENCON 2012 IEEE Region 10 Conference, Cebu, Philippine, 19–22 November 2012; pp. 1–5. [Google Scholar] [CrossRef]
- Basu, S.; Mamud, S. Comparative Study on the Effect of Order and Cut off Frequency of Butterworth Low Pass Filter for Removal of Noise in ECG Signal. In Proceedings of the 2020 IEEE 1st International Conference for Convergence in Engineering (ICCE), Kolkata, India, 5–6 September 2020; pp. 156–160. [Google Scholar] [CrossRef]
- Bertolazzi, P.; Felici, G.; Festa, P.; Fiscon, G.; Weitschek, E. Integer programming models for feature selection: New extensions and a randomized solution algorithm. Eur. J. Oper. Res. 2016, 250, 389–399. [Google Scholar] [CrossRef]
- Suykens, J.A.K.; Vandewalle, J. Least Squares Support Vector Machine Classifiers. Neural Process. Lett. 1999, 9, 293–300. [Google Scholar] [CrossRef]
- Jin, B.; Tang, Y.C.; Zhang, Y.Q. Support vector machines with genetic fuzzy feature transformation for biomedical data classification. Inf. Sci. 2007, 177, 476–489. [Google Scholar] [CrossRef]
- Ge, D.; Srinivasan, N.; Krishnan, S.M. Cardiac Arrhythmia Classification Using Autoregressive Modeling. Biomed. Eng. Online 2003, 1, 5. [Google Scholar] [CrossRef] [Green Version]
- Unal, I. Defining an Optimal Cut-Point Value in ROC Analysis: An Alternative Approach. Comput. Math. Methods Med. 2017, 2017, 3762651. [Google Scholar] [CrossRef]
- Massimo Buscema, P.; Grossi, E.; Massini, G.; Breda, M.; Dell Torre, F. Computer aided diagnosis for atrial fibrillation based on new artificial adaptive systems. Comput. Methods Programs Biomed. 2020, 191, 105401. [Google Scholar] [CrossRef]
- Alonso, E.; Eftestel, T.; Aramendi, E.; Kramer-Johansen, J.; Skogvoll, E.; Nordseth, T. Beyond ventricular fibrillation analysis: Comprehensive waveform analysis for all cardiac rhythms occurring during resuscitation. Resuscitation 2014, 85, 1541–1548. [Google Scholar] [CrossRef]
- Sun, Y.; Wing, A.K.C.; Kamel, M.S. Classification of Imbalanced Data: A Review. Int. J. Pattern Recognit. Artif. Intell. 2009, 23, 687–719. [Google Scholar] [CrossRef]
- Qiao, F.; Li, B.; Zhang, Y.; Guo, H.; Li, W.; Zhou, S. A Fast and Accurate Recognition of ECG Signals Based on ELM-LRF and BLSTM Algorithm. IEEE Access 2020, 8, 71189–71198. [Google Scholar] [CrossRef]
- Choa, B.H.; Yu, H.; Kim, K.W.; Kim, T.H.; Kim, I.Y.; Kim, S.I. Application of irregular and unbalanced data to predict diabetic nephropathy using visualization and feature selection methods. Artif. Intell. Med. 2008, 42, 37–53. [Google Scholar] [CrossRef]
- Weixin, N. A novel algorithm for ventricular arrhythmia classification using a fuzzy logic approach. Australas. Phys. Eng. Sci. Med. 2016, 39, 903–912. [Google Scholar] [CrossRef]
- Hajeb-Mohammadalipour, S.; Ahmadi, M.; Shahghadami, R.; Chon, K.H. Automated Method for Discrimination of Arrhythmias Using Time, Frequency, and Nonlinear Features of Electrocardiogram Signals. Sensors 2018, 18, 2090. [Google Scholar] [CrossRef] [Green Version]
- Ghaddar, B.; Naoum-Sawaya, J. High dimensional data classification and feature selection using support vector machines. Eur. J. Oper. Res. 2018, 265, 993–1004. [Google Scholar] [CrossRef]
- Jin, Y. Fuzzy modeling of high-dimensional systems: Complexity reduction and interpretability improvement. IEEE Trans. Fuzzy Syst. 2000, 8, 212–221. [Google Scholar] [CrossRef] [Green Version]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Symptoms | NSR | APC | AFib | VPC | VT |
|---|---|---|---|---|---|
| Features | IMF1 (μ, σ) | ||||
| Frequency | 4.772, 0.787 | 4.241, 0.798 | 3.571, 0.558 | 3.283, 0.973 | 3.120, 1.123 |
| Power | 1.167, 0.864 | 0.791, 0.567 | 2.683, 1.214 | 3.196, 2.170 | 6.504, 6.250 |
| Features | IMF2 (μ, σ) | ||||
| Frequency | 1.478, 0.527 | 0.932, 0.504 | 1.049, 0.455 | 0.993, 0.503 | 1.013, 0.489 |
| Power | 1.344, 1.605 | 1.223, 1.294 | 2.824, 2.053 | 4.548, 3.909 | 6.923, 7.274 |
| Features | IMF3 (μ, σ) | ||||
| Frequency | 0.288, 0.261 | 0.378, 0.257 | 0.327, 0.263 | 0.340, 0.264 | 0.315, 0.265 |
| Power | 0.645, 1.997 | 1.461, 2.762 | 1.183, 2.024 | 1.449, 2.011 | 1.184, 1.070 |
| IMF1’s Frequency | IMF2’s Frequency | IMF3’s Frequency | |||
| Pattern | p-Value | Patterns | p-Value | Pattern | p-Value |
| NSR–APC | <0.001 | NSR–APC | <0.001 | NSR–APC | 0.0003 |
| NSR–AFib | <0.001 | NSR–AFib | <0.001 | NSR–AFib | 0.0009 |
| NSR–VPC | <0.001 | NSR–VPC | <0.001 | NSR–VPC | 0.006 |
| NSR–VT | <0.001 | NSR–VT | <0.001 | NSR–VT | 0.3482 |
| APC–AFib | <0.001 | APC–AFib | 0.0286 | APC–AFib | 0.037 |
| APC–VPC | <0.001 | APC–VPC | 0.3926 | APC–VPC | 0.1081 |
| APC–VT | <0.001 | APC–VT | 0.2015 | APC–VT | 0.0407 |
| AFib–VPC | <0.001 | AFib–VPC | 0.0871 | AFib–VPC | 0.6571 |
| AFib–VT | <0.001 | AFib–VT | 0.5691 | AFib–VT | 0.6032 |
| VPC-VT | 0.0302 | VPC-VT | 0.6266 | VPC-VT | 0.4894 |
| IMF1’s Power | IMF2’s Power | IMF3’s Power | |||
| Pattern | p-Value | Pattern | p-Value | Pattern | p-Value |
| NSR–APC | <0.001 | NSR–APC | 0.4453 | NSR–APC | <0.001 |
| NSR–AFib | <0.001 | NSR–AFib | <0.001 | NSR–AFib | <0.001 |
| NSR–VPC | <0.001 | NSR–VPC | <0.001 | NSR–VPC | <0.001 |
| NSR–VT | <0.001 | NSR–VT | <0.001 | NSR–VT | <0.001 |
| APC–AFib | <0.001 | APC–AFib | <0.001 | APC–AFib | 0.0024 |
| APC–VPC | <0.001 | APC–VPC | <0.001 | APC–VPC | 0.0024 |
| APC–VT | <0.001 | APC–VT | <0.001 | APC–VT | 0.0052 |
| AFib–VPC | 0.3851 | AFib–VPC | <0.001 | AFib–VPC | 0.4177 |
| AFib–VT | <0.001 | AFib–VT | <0.001 | AFib–VT | 0.3471 |
| VPC-VT | <0.001 | VPC-VT | 0.0028 | VPC-VT | 0.7985 |
| ML Model | Parameter | Value |
|---|---|---|
| MLP | hidden layer size | 10 |
| backpropagation training function | scaled conjugate gradient | |
| performance validation function | cross entropy | |
| RF | ensemble aggregation method | adaptive boosting |
| learning cycles | 100 | |
| nodes in trees | 10 | |
| SVM | kernel function | linear |
| coding design | OVO | |
| estimation output | posterior probability | |
| kernel scale parameter | 1 | |
| NB | distribution for the nodes | Gaussian distribution |
| smoothing density support | real values |
| Pattern | ROC | MLP | RF | SVM | NB |
|---|---|---|---|---|---|
| NSR–APC | Sensitivity | 0.842 | 0.782 | 0.774 | 0.815 |
| Specificity | 0.857 | 0.837 | 0.907 | 0.889 | |
| Accuracy | 0.842 | 0.783 | 0.777 | 0.816 | |
| AUC | 0.85 | 0.81 | 0.84 | 0.85 | |
| NSR–AFib | Sensitivity | 0.913 | 0.916 | 0.941 | 0.812 |
| Specificity | 0.918 | 0.931 | 0.861 | 0.91 | |
| Accuracy | 0.913 | 0.919 | 0.929 | 0.83 | |
| AUC | 0.92 | 0.92 | 0.9 | 0.86 | |
| NSR–VPC | Sensitivity | 0.9 | 0.927 | 0.953 | 0.958 |
| Specificity | 0.673 | 0.901 | 0.683 | 0.657 | |
| Accuracy | 0.89 | 0.925 | 0.936 | 0.943 | |
| AUC | 0.79 | 0.91 | 0.82 | 0.81 | |
| NSR–VT | Sensitivity | 0.959 | 0.986 | 0.989 | 0.997 |
| Specificity | 0.857 | 0.96 | 0.8 | 0.955 | |
| Accuracy | 0.957 | 0.985 | 0.986 | 0.996 | |
| AUC | 0.91 | 0.97 | 0.89 | 0.98 | |
| APC–AFib | Sensitivity | 0.882 | 0.878 | 0.907 | 0.78 |
| Specificity | 0.844 | 0.929 | 0.89 | 0.957 | |
| Accuracy | 0.847 | 0.925 | 0.982 | 0.943 | |
| AUC | 0.86 | 0.9 | 0.9 | 0.87 | |
| APC–AFib | Sensitivity | 0.769 | 1 | 0.975 | 0.914 |
| Specificity | 0.826 | 0.862 | 0.826 | 0.784 | |
| Accuracy | 0.809 | 0.895 | 0.865 | 0.821 | |
| AUC | 0.8 | 0.93 | 0.9 | 0.85 | |
| APC–VT | Sensitivity | 1 | 1 | 1 | 1 |
| Specificity | 0.923 | 1 | 0.96 | 0.778 | |
| Accuracy | 0.964 | 1 | 0.984 | 0.898 | |
| AUC | 0.96 | 1 | 0.98 | 0.89 | |
| AFib–VPC | Sensitivity | 0.724 | 0.793 | 0.742 | 0.863 |
| Specificity | 0.521 | 0.613 | 0.714 | 0.445 | |
| Accuracy | 0.676 | 0.75 | 0.736 | 0.77 | |
| AUC | 0.62 | 0.7 | 0.73 | 0.65 | |
| AFib–VT | Sensitivity | 0.899 | 0.915 | 0.888 | 0.992 |
| Specificity | 0.667 | 0.828 | 0.889 | 0.656 | |
| Accuracy | 0.879 | 0.909 | 0.888 | 0.97 | |
| AUC | 0.78 | 0.87 | 0.89 | 0.82 | |
| VPC–VT | Sensitivity | 0.673 | 0.685 | 0.709 | 0.726 |
| Specificity | 0.649 | 0.490 | 0.533 | 0.568 | |
| Accuracy | 0.667 | 0.636 | 0.665 | 0.682 | |
| AUC | 0.66 | 0.59 | 0.62 | 0.65 |
| Pattern | ROC | MLP | RF | SVM | NB |
|---|---|---|---|---|---|
| NSR–APC | Sensitivity | 0.917 | 0.819 | 0.903 | 0.859 |
| Specificity | 0.789 | 0.833 | 0.821 | 0.825 | |
| Accuracy | 0.917 | 0.819 | 0.902 | 0.859 | |
| AUC | 0.85 | 0.83 | 0.86 | 0.84 | |
| NSR–AFib | Sensitivity | 0.887 | 0.907 | 0.905 | 0.906 |
| Specificity | 0.815 | 0.82 | 0.787 | 0.808 | |
| Accuracy | 0.876 | 0.895 | 0.888 | 0.889 | |
| AUC | 0.85 | 0.86 | 0.85 | 0.86 | |
| NSR–VPC | Sensitivity | 0.961 | 0.97 | 0.932 | 0.969 |
| Specificity | 0.629 | 0.65 | 0.652 | 0.595 | |
| Accuracy | 0.945 | 0.953 | 0.918 | 0.951 | |
| AUC | 0.8 | 0.81 | 0.79 | 0.78 | |
| NSR–VT | Sensitivity | 0.994 | 0.995 | 0.994 | 0.996 |
| Specificity | 0.793 | 0.84 | 0.806 | 0.786 | |
| Accuracy | 0.992 | 0.994 | 0.992 | 0.993 | |
| AUC | 0.89 | 0.92 | 0.9 | 0.89 | |
| APC–AFib | Sensitivity | 0.811 | 0.921 | 0.842 | 0.868 |
| Specificity | 0.952 | 0.722 | 0.929 | 0.913 | |
| Accuracy | 0.94 | 0.738 | 0.92 | 0.909 | |
| AUC | 0.88 | 0.82 | 0.89 | 0.89 | |
| APC–AFib | Sensitivity | 0.909 | 0.921 | 0.914 | 0.917 |
| Specificity | 0.886 | 0.757 | 0.898 | 0.821 | |
| Accuracy | 0.893 | 0.801 | 0.9 | 0.85 | |
| AUC | 0.9 | 0.84 | 0.91 | 0.87 | |
| APC–VT | Sensitivity | 1 | 1 | 1 | 1 |
| Specificity | 1 | 0.875 | 0.962 | 0.957 | |
| Accuracy | 1 | 0.949 | 0.983 | 0.982 | |
| AUC | 1 | 0.94 | 0.98 | 0.98 | |
| AFib–VPC | Sensitivity | 0.805 | 0.776 | 0.692 | 0.849 |
| Specificity | 0.527 | 0.553 | 0.662 | 0.473 | |
| Accuracy | 0.741 | 0.719 | 0.685 | 0.759 | |
| AUC | 0.67 | 0.66 | 0.68 | 0.66 | |
| AFib–VT | Sensitivity | 0.963 | 0.976 | 0.921 | 0.978 |
| Specificity | 0.719 | 0.75 | 0.735 | 0.667 | |
| Accuracy | 0.945 | 0.958 | 0.905 | 0.955 | |
| AUC | 0.84 | 0.86 | 0.83 | 0.82 | |
| VPC–VT | Sensitivity | 0.673 | 0.685 | 0.709 | 0.726 |
| Specificity | 0.649 | 0.490 | 0.533 | 0.568 | |
| Accuracy | 0.667 | 0.636 | 0.665 | 0.682 | |
| AUC | 0.66 | 0.59 | 0.62 | 0.65 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsiao, W.-T.; Kan, Y.-C.; Kuo, C.-C.; Kuo, Y.-C.; Chai, S.-K.; Lin, H.-C. Hybrid-Pattern Recognition Modeling with Arrhythmia Signal Processing for Ubiquitous Health Management. Sensors 2022, 22, 689. https://0-doi-org.brum.beds.ac.uk/10.3390/s22020689
Hsiao W-T, Kan Y-C, Kuo C-C, Kuo Y-C, Chai S-K, Lin H-C. Hybrid-Pattern Recognition Modeling with Arrhythmia Signal Processing for Ubiquitous Health Management. Sensors. 2022; 22(2):689. https://0-doi-org.brum.beds.ac.uk/10.3390/s22020689
Chicago/Turabian StyleHsiao, Wei-Ting, Yao-Chiang Kan, Chin-Chi Kuo, Yu-Chieh Kuo, Sin-Kuo Chai, and Hsueh-Chun Lin. 2022. "Hybrid-Pattern Recognition Modeling with Arrhythmia Signal Processing for Ubiquitous Health Management" Sensors 22, no. 2: 689. https://0-doi-org.brum.beds.ac.uk/10.3390/s22020689