
Healing Hands: The Tactile Internet in Future Tele-Healthcare

 , , , , , ,
, , , , , ,  and
and 
Abstract
:1. Introduction
2. The Tactile Internet
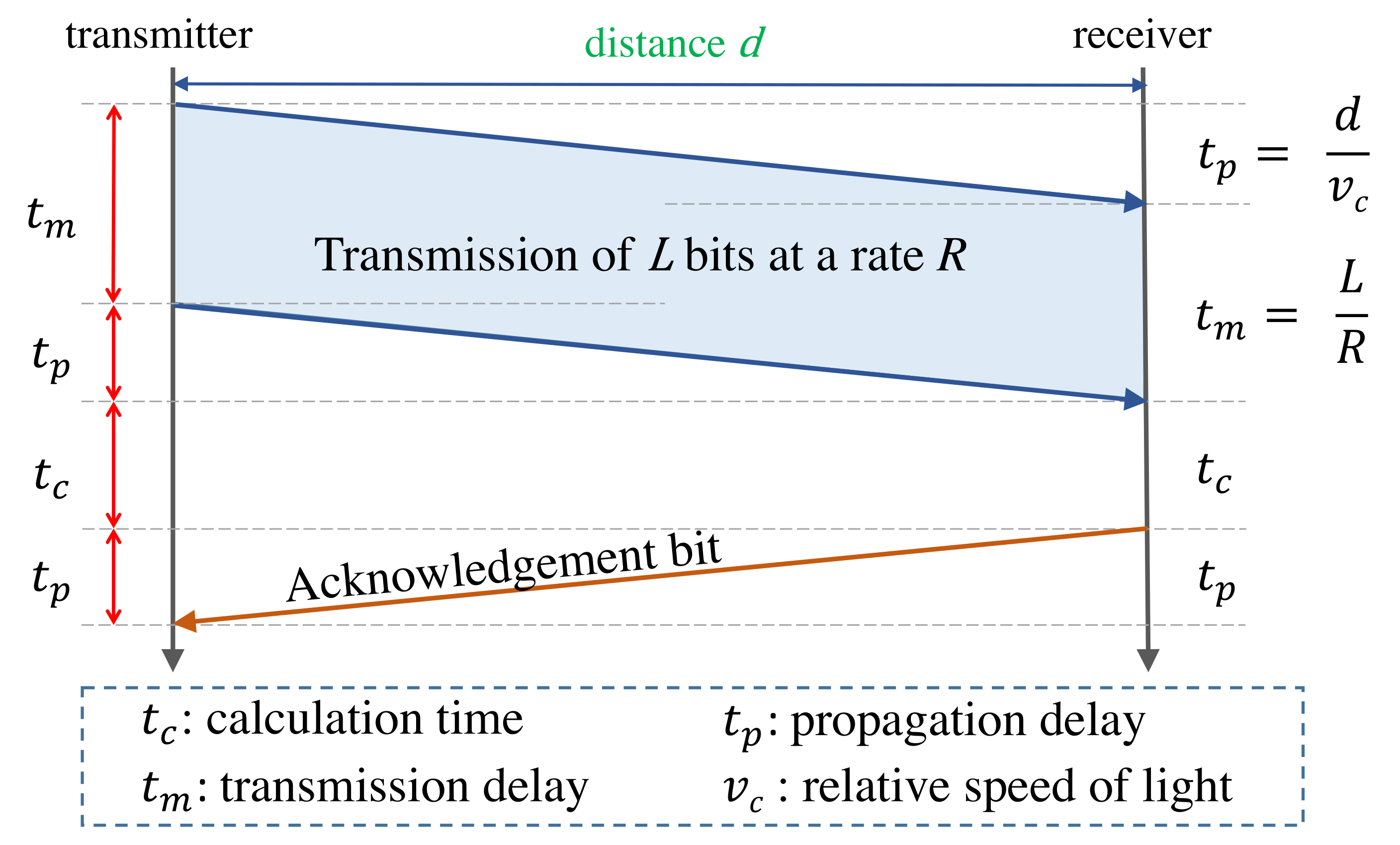
2.1. Latency Requirements
2.2. Current Latency Limitations
3. Tele-Healthcare Latency in the Real World
3.1. Surgery
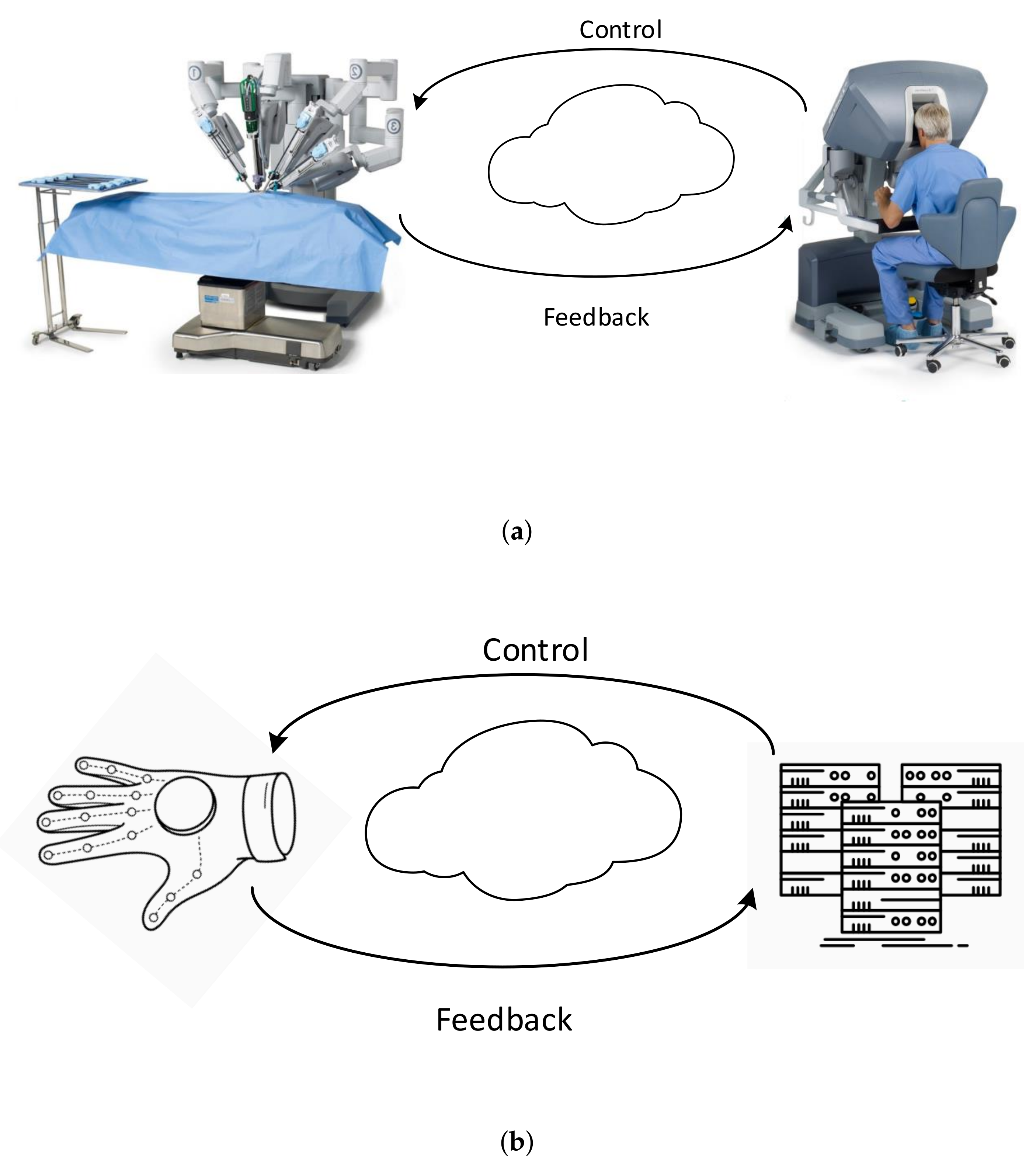
3.1.1. Remote Surgery
3.1.2. Intuitive Human–Machine Coworking
3.2. Rehabilitation
3.2.1. Independent Rehabilitation at Home
3.2.2. Intuitive Machine-Guided Human Rehabilitation
4. Latency and the Problem of Net-Neutrality
4.1. Evaluation Setup and Experimentation
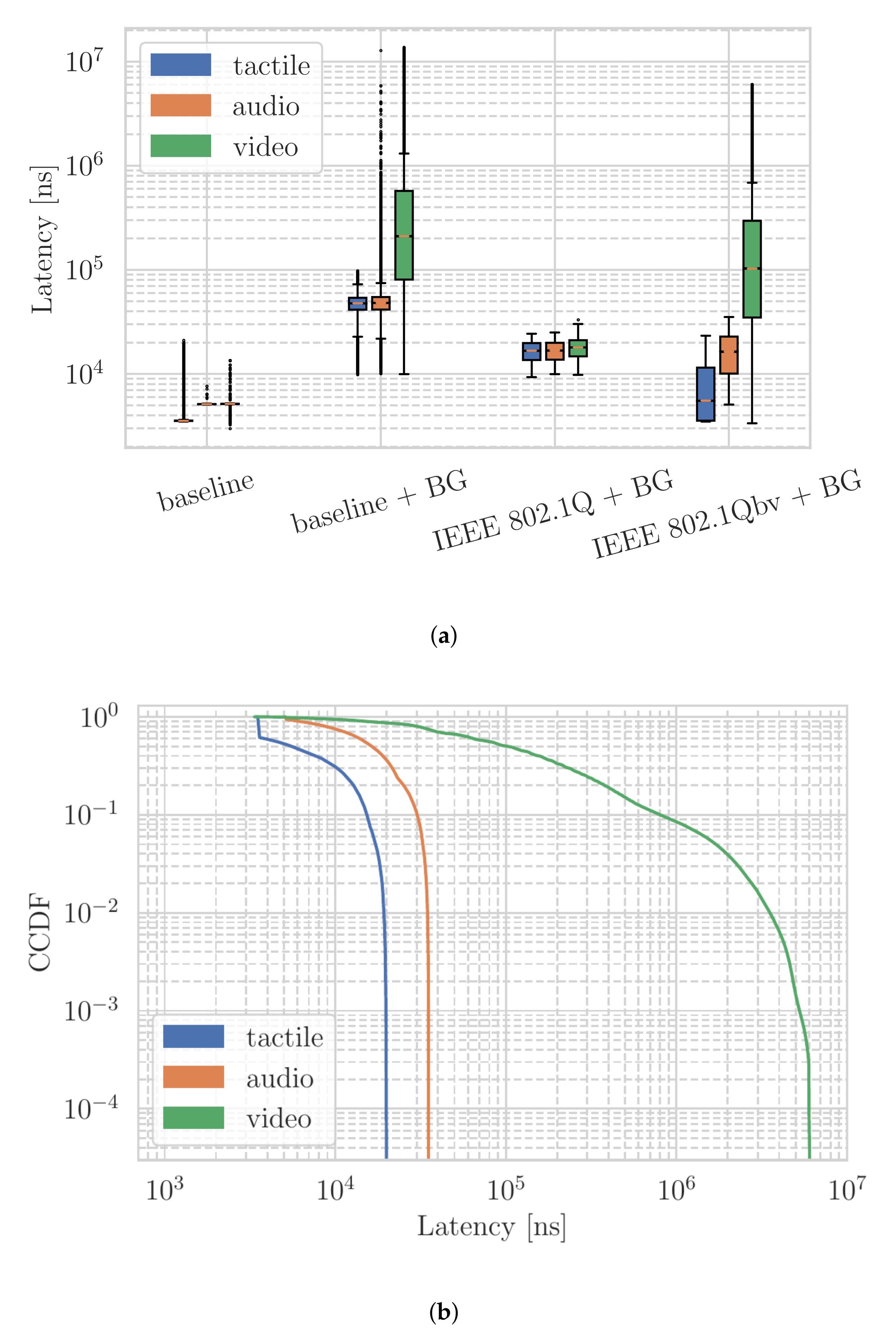
4.2. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Sanders, C.; Rogers, A.; Bowen, R.; Bower, P.; Hirani, S.; Cartwright, M.; Fitzpatrick, R.; Knapp, M.; Barlow, J.; Hendy, J.; et al. Exploring barriers to participation and adoption of telehealth and telecare within the Whole System Demonstrator trial: A qualitative study. BMC Health Serv. Res. 2012, 12, 220. [Google Scholar] [CrossRef]
- Moore, M.A.; Coffman, M.; Jetty, A.; Klink, K.; Petterson, S.; Bazemore, A. Family Physicians Report Considerable Interest in, but Limited Use of, Telehealth Services. J. Am. Board Fam. Med. 2017, 30, 320–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.; Amaize, A.; Barath, D. Evaluating Telehealth Adoption and Related Barriers Among Hospitals Located in Rural and Urban Areas. J. Rural. Health 2020, 37, 801–811. [Google Scholar] [CrossRef] [PubMed]
- Tuckson, R.V.; Edmunds, M.; Hodgkins, M.L. Telehealth. N. Engl. J. Med. 2017, 377, 1585–1592. [Google Scholar] [CrossRef] [PubMed]
- Dorsey, E.R.; Topol, E.J. State of telehealth. N. Engl. J. Med. 2016, 375, 154–161. [Google Scholar] [CrossRef] [Green Version]
- Popescu, V.G.; Burdea, G.C.; Bouzit, M.; Hentz, V.R. A virtual-reality-based telerehabilitation system with force feedback. IEEE Trans. Inf. Technol. Biomed. 2000, 4, 45–51. [Google Scholar] [CrossRef]
- Hernandez, A.I.; Mora, F.; Villegas, M.; Passariello, G.; Carrault, G. Real-time ECG transmission via Internet for nonclinical applications. IEEE Trans. Inf. Technol. Biomed. 2001, 5, 253–257. [Google Scholar] [CrossRef]
- Tousignant, M.; Mampuya, W.M.; Bissonnette, J.; Guillemette, E.; Lauriault, F.; Lavoie, J.; St-Laurent, M.E.; Pagé, C. Telerehabilitation with live-feed biomedical sensor signals for patients with heart failure: A pilot study. Cardiovasc. Diagn. Ther. 2019, 9, 319. [Google Scholar] [CrossRef]
- Aileni, R.M.; Suciu, G.; Suciu, V.; Pasca, S.; Ciurea, J. Smart Systems to Improve the Mobility of People with Visual Impairment 25 through IoM and IoMT. In Technological Trends in Improved Mobility of the Visually Impaired; Springer International Publishing: Cham, Switzerland, 2020; pp. 65–84. [Google Scholar] [CrossRef]
- Ding, X.; Clifton, D.; Ji, N.; Lovell, N.H.; Bonato, P.; Chen, W.; Yu, X.; Xue, Z.; Xiang, T.; Long, X.; et al. Wearable Sensing and Telehealth Technology with Potential Applications in the Coronavirus Pandemic. IEEE Rev. Biomed. Eng. 2021, 14, 48–70. [Google Scholar] [CrossRef]
- Shen, Y.; Guo, D.; Long, F.; Mateos, L.A.; Ding, H.; Xiu, Z.; Hellman, R.B.; King, A.; Chen, S.; Zhang, C.; et al. Robots Under COVID-19 Pandemic: A Comprehensive Survey. IEEE Access 2021, 9, 1590–1615. [Google Scholar] [CrossRef]
- Nepogodiev, D.; Martin, J.; Biccard, B.; Makupe, A.; Bhangu, A.; Ademuyiwa, A. Global burden of postoperative death. Lancet 2019, 393, 401. [Google Scholar] [CrossRef] [Green Version]
- Weiser, T.G.; Regenbogen, S.E.; Thompson, K.D.; Haynes, A.B.; Lipsitz, S.R.; Berry, W.R.; Gawande, A.A. An estimation of the global volume of surgery: A modelling strategy based on available data. Lancet 2008, 372, 139–144. [Google Scholar] [CrossRef]
- Birkmeyer, J.D.; Finks, J.F.; O’Reilly, A.; Oerline, M.; Carlin, A.M.; Nunn, A.R.; Dimick, J.; Banerjee, M.; Birkmeyer, N.J. Surgical skill and complication rates after bariatric surgery. N. Engl. J. Med. 2013, 369, 1434–1442. [Google Scholar] [CrossRef] [PubMed]
- Birkmeyer, J.D.; Siewers, A.E.; Finlayson, E.V.; Stukel, T.A.; Lucas, F.L.; Batista, I.; Welch, H.G.; Wennberg, D.E. Hospital volume and surgical mortality in the United States. N. Engl. J. Med. 2002, 346, 1128–1137. [Google Scholar] [CrossRef] [PubMed]
- Maier-Hein, L.; Vedula, S.S.; Speidel, S.; Navab, N.; Kikinis, R.; Park, A.; Eisenmann, M.; Feussner, H.; Forestier, G.; Giannarou, S.; et al. Surgical data science for next-generation interventions. Nat. Biomed. Eng. 2017, 1, 691. [Google Scholar] [CrossRef]
- Fitzek, F.; Li, S.C.; Speidel, S.; Thorsten, S.; Simsek, M.; Reisslein, M. (Eds.) Tactile Internet with Human-in-the-Loop, 1st ed.; Academic Press: New York, NY, USA, 2021. [Google Scholar] [CrossRef]
- Fettweis, G.P. The tactile internet: Applications and challenges. IEEE Veh. Technol. Mag. 2014, 9, 64–70. [Google Scholar] [CrossRef]
- Dohler, M.; Mahmoodi, T.; Lema, M.A.; Condoluci, M.; Sardis, F.; Antonakoglou, K.; Aghvami, H. Internet of skills, where robotics meets AI, 5G and the Tactile Internet. In Proceedings of the 2017 European Conference on Networks and Communications (EuCNC), Oulu, Finland, 12–15 June 2017; pp. 1–5. [Google Scholar] [CrossRef] [Green Version]
- Li, S.C.; Muschter, E.; Limanowski, J.; Hatzipanayioti, A. Human perception and neurocognitive development across the lifespan. In Tactile Internet; Fitzek, F.H., Li, S.C., Speidel, S., Strufe, T., Simsek, M., Reisslein, M., Eds.; Academic Press: Cambridge, MA, USA, 2021; pp. 199–221. [Google Scholar] [CrossRef]
- Yang, Y.; Zador, A.M. Differences in Sensitivity to Neural Timing among Cortical Areas. J. Neurosci. 2012, 32, 15142–15147. [Google Scholar] [CrossRef] [Green Version]
- 3GPP. Study on Communication for Automation in Vertical Domains (CAV). Technical Report (TR) 22.804, 3rd Generation Partnership Project (3GPP), Version 16.3.0. 2020. Available online: https://portal.3gpp.org/desktopmodules/Specifications/SpecificationDetails.aspx?specificationId=3187 (accessed on 29 November 2021).
- Stein, B.E. The New Handbook of Multisensory Processing; MIT Press: Cambridge, MA, USA, 2012. [Google Scholar]
- Ernst, M.O.; Bulthoff, H.H. Merging the senses into a robust percept. Trends. Cogn. Sci. 2004, 8, 162–169. [Google Scholar] [CrossRef]
- Knill, D.C.; Pouget, A. The Bayesian brain: The role of uncertainty in neural coding and computation. Trends. Neurosci. 2004, 27, 712–719. [Google Scholar] [CrossRef]
- Macaluso, E.; Driver, J. Multisensory spatial interactions: A window onto functional integration in the human brain. Trends. Neurosci. 2005, 28, 264–271. [Google Scholar] [CrossRef]
- Stein, B.E.; Stanford, T.R.; Rowland, B.A. Development of multisensory integration from the perspective of the individual neuron. Nat. Rev. Neurosci. 2014, 15, 520–535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grady, C. Trends in neurocognitive aging. Nat. Reviews. Neurosci. 2012, 13, 491. [Google Scholar] [CrossRef] [PubMed]
- Li, S.C.; Rieckmann, A. Neuromodulation and aging: Implications of aging neuronal gain control on cognition. Curr. Opin. Neurobiol. 2014, 29, 148–158. [Google Scholar] [CrossRef] [PubMed]
- Li, S.C.; Lindenberger, U.; Hommel, B.; Aschersleben, G.; Prinz, W.; Baltes, P.B. Transformations in the couplings among intellectual abilities and constituent cognitive processes across the life span. Psychol. Sci. 2004, 15, 155–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papenberg, G.; Hammerer, D.; Muller, V.; Lindenberger, U.; Li, S.C. Lower theta inter-trial phase coherence during performance monitoring is related to higher reaction time variability: A lifespan study. Neuroimage 2013, 83, 912–920. [Google Scholar] [CrossRef]
- Ghosh, S.; Mukherjee, A.; Ghosh, S.K.; Buyya, R. Mobi-IoST: Mobility-Aware Cloud-Fog-Edge-IoT Collaborative Framework for Time-Critical Applications. IEEE Trans. Netw. Sci. Eng. 2020, 7, 2271–2285. [Google Scholar] [CrossRef] [Green Version]
- Štefanič, P.; Cigale, M.; Jones, A.C.; Knight, L.; Taylor, I.; Istrate, C.; Suciu, G.; Ulisses, A.; Stankovski, V.; Taherizadeh, S.; et al. SWITCH workbench: A novel approach for the development and deployment of time-critical microservice-based cloud-native applications. Future Gener. Comput. Syst. 2019, 99, 197–212. [Google Scholar] [CrossRef]
- Xiang, Z.; Gabriel, F.; Urbano, E.; Nguyen, G.T.; Reisslein, M.; Fitzek, F.H.P. Reducing Latency in Virtual Machines Enabling Tactile Internet for Human Machine Co-working. IEEE J. Sel. Areas Commun. 2019, 37, 1098–1116. [Google Scholar] [CrossRef]
- Tsokalo, I.A.; Kuss, D.; Kharabet, I.; Fitzek, F.H.P.; Reisslein, M. Remote Robot Control with Human-in-the-Loop over Long Distances Using Digital Twins. In Proceedings of the 2019 IEEE Global Communications Conference (GLOBECOM), Waikoloa, HI, USA, 9–13 December 2019; pp. 1–6. [Google Scholar] [CrossRef]
- Son, G.M.; Kim, J.G.; Lee, J.C.; Suh, Y.J.; Cho, H.M.; Lee, Y.S.; Lee, I.K.; Chun, C.S. Multidimensional analysis of the learning curve for laparoscopic rectal cancer surgery. J. Laparoendosc. Adv. Surg. Tech. 2010, 20, 609–617. [Google Scholar] [CrossRef]
- Andolfi, C.; Umanskiy, K. Mastering robotic surgery: Where does the learning curve lead us? J. Laparoendosc. Adv. Surg. Tech. 2017, 27, 470–474. [Google Scholar] [CrossRef]
- Marescaux, J.; Leroy, J.; Rubino, F.; Smith, M.; Vix, M.; Simone, M.; Mutter, D. Transcontinental robot-assisted remote telesurgery: Feasibility and potential applications. Ann. Surg. 2002, 235, 487. [Google Scholar] [CrossRef] [PubMed]
- Gupta, R.; Tanwar, S.; Tyagi, S.; Kumar, N. Tactile-internet-based telesurgery system for healthcare 4.0: An architecture, research challenges, and future directions. IEEE Netw. 2019, 33, 22–29. [Google Scholar] [CrossRef]
- Hung, A.J.; Chen, J.; Shah, A.; Gill, I.S. Telementoring and telesurgery for minimally invasive procedures. J. Urol. 2018, 199, 355–369. [Google Scholar] [CrossRef] [PubMed]
- Lacy, A.; Bravo, R.; Otero-Piñeiro, A.; Pena, R.; De Lacy, F.; Menchaca, R.; Balibrea, J. 5G-assisted telementored surgery. Br. J. Surg. 2019, 106, 1576–1579. [Google Scholar] [CrossRef] [Green Version]
- Rojas-Muñoz, E.; Cabrera, M.E.; Lin, C.; Andersen, D.; Popescu, V.; Anderson, K.; Zarzaur, B.L.; Mullis, B.; Wachs, J.P. The System for Telementoring with Augmented Reality (STAR): A head-mounted display to improve surgical coaching and confidence in remote areas. Surgery 2020, 167, 724–731. [Google Scholar] [CrossRef]
- Huang, E.Y.; Knight, S.; Guetter, C.R.; Davis, C.H.; Moller, M.; Slama, E.; Crandall, M. Telemedicine and telementoring in the surgical specialties: A narrative review. Am. J. Surg. 2019, 218, 760–766. [Google Scholar] [CrossRef]
- Erridge, S.; Yeung, D.K.; Patel, H.R.; Purkayastha, S. Telementoring of surgeons: A systematic review. Surg. Innov. 2019, 26, 95–111. [Google Scholar] [CrossRef]
- Katić, D.; Wekerle, A.L.; Görtler, J.; Spengler, P.; Bodenstedt, S.; Röhl, S.; Suwelack, S.; Kenngott, H.G.; Wagner, M.; Müller-Stich, B.P.; et al. Context-aware augmented reality in laparoscopic surgery. Comput. Med. Imaging Graph. 2013, 37, 174–182. [Google Scholar] [CrossRef] [Green Version]
- Vedula, S.S.; Ishii, M.; Hager, G.D. Objective assessment of surgical technical skill and competency in the operating room. Annu. Rev. Biomed. Eng. 2017, 19, 301–325. [Google Scholar] [CrossRef]
- Vercauteren, T.; Unberath, M.; Padoy, N.; Navab, N. Cai4cai: The rise of contextual artificial intelligence in computer-assisted interventions. Proc. IEEE 2019, 108, 198–214. [Google Scholar] [CrossRef] [Green Version]
- Steinbach, E.; Hirche, S.; Kammerl, J.; Vittorias, I.; Chaudhari, R. Haptic data compression and communication. IEEE Signal Process. Mag. 2010, 28, 87–96. [Google Scholar] [CrossRef]
- Bodenstedt, S.; Rivoir, D.; Jenke, A.; Wagner, M.; Breucha, M.; Müller-Stich, B.; Mees, S.T.; Weitz, J.; Speidel, S. Active learning using deep Bayesian networks for surgical workflow analysis. Int. J. Comput. Assist. Radiol. Surg. 2019, 14, 1079–1087. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shademan, A.; Decker, R.S.; Opfermann, J.D.; Leonard, S.; Krieger, A.; Kim, P.C. Supervised autonomous robotic soft tissue surgery. Sci. Transl. Med. 2016, 8, 337ra64. [Google Scholar] [CrossRef] [PubMed]
- De Momi, E.; Kranendonk, L.; Valenti, M.; Enayati, N.; Ferrigno, G. A neural network-based approach for trajectory planning in robot–human handover tasks. Front. Robot. AI 2016, 3, 34. [Google Scholar] [CrossRef] [Green Version]
- Mayer, H.; Gomez, F.; Wierstra, D.; Nagy, I.; Knoll, A.; Schmidhuber, J. A system for robotic heart surgery that learns to tie knots using recurrent neural networks. Adv. Robot. 2008, 22, 1521–1537. [Google Scholar] [CrossRef] [Green Version]
- Antico, M.; Sasazawa, F.; Wu, L.; Jaiprakash, A.; Roberts, J.; Crawford, R.; Pandey, A.K.; Fontanarosa, D. Ultrasound guidance in minimally invasive robotic procedures. Med. Image Anal. 2019, 54, 149–167. [Google Scholar] [CrossRef]
- Rivoir, D.; Bodenstedt, S.; Funke, I.; von Bechtolsheim, F.; Distler, M.; Weitz, J.; Speidel, S. Rethinking Anticipation Tasks: Uncertainty-Aware Anticipation of Sparse Surgical Instrument Usage for Context-Aware Assistance. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Virtual. 4–8 October 2020; pp. 752–762. [Google Scholar] [CrossRef]
- Bodenstedt, S.; Wagner, M.; Mündermann, L.; Kenngott, H.; Müller-Stich, B.; Breucha, M.; Mees, S.T.; Weitz, J.; Speidel, S. Prediction of laparoscopic procedure duration using unlabeled, multimodal sensor data. Int. J. Comput. Assist. Radiol. Surg. 2019, 14, 1089–1095. [Google Scholar] [CrossRef] [Green Version]
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics-2020 Update: A Report From the American Heart Association. Circulation 2020, 141, e139–e596. [Google Scholar] [CrossRef]
- Werner, R.M.; Coe, N.B.; Qi, M.; Konetzka, R.T. Patient Outcomes After Hospital Discharge to Home with Home Health Care vs to a Skilled Nursing Facility. JAMA Intern. Med. 2019, 179, 617–623. [Google Scholar] [CrossRef]
- Lee, H.J.; Lee, S.H.; Seo, K.; Lee, M.; Chang, W.H.; Choi, B.O.; Ryu, G.H.; Kim, Y.H. Training for Walking Efficiency with a Wearable Hip-Assist Robot in Patients with Stroke. Stroke 2019, 50, 3545–3552. [Google Scholar] [CrossRef]
- Mehrholz, J.; Thomas, S.; Werner, C.; Kugler, J.; Pohl, M.; Elsner, B. Electromechanical-Assisted Training for Walking After Stroke. Stroke 2017, 48, e188–e189. [Google Scholar] [CrossRef] [PubMed]
- Wagner, T.H.; Lo, A.C.; Peduzzi, P.; Bravata, D.M.; Huang, G.D.; Krebs, H.I.; Ringer, R.J.; Federman, D.G.; Richards, L.G.; Haselkorn, J.K.; et al. An Economic Analysis of Robot-Assisted Therapy for Long-Term Upper-Limb Impairment After Stroke. Stroke 2011, 42, 2630–2632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aminov, A.; Rogers, J.M.; Middleton, S.; Caeyenberghs, K.; Wilson, P.H. What do randomized controlled trials say about virtual rehabilitation in stroke? A systematic literature review and meta-analysis of upper-limb and cognitive outcomes. J. Neuroeng. Rehabil. 2018, 15, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maier, M.; Rubio Ballester, B.; Duff, A.; Duarte Oller, E.; Verschure, P.F.M.J. Effect of Specific Over Nonspecific VR-Based Rehabilitation on Poststroke Motor Recovery: A Systematic Meta-analysis. Neurorehabilit. Neural Repair 2019, 33, 112–129. [Google Scholar] [CrossRef]
- Karamians, R.; Proffitt, R.; Kline, D.; Gauthier, L.V. Effectiveness of Virtual Reality- and Gaming-Based Interventions for Upper Extremity Rehabilitation Poststroke: A Meta-analysis. Arch. Phys. Med. Rehabil 2020, 101, 885–896. [Google Scholar] [CrossRef]
- Hu, X.; Yue, Z.; Zhang, X.; Wang, J. Hand Rehabilitation Robotics on Poststroke Motor Recovery. Behav. Neurol. 2017, 2017, 3908135. [Google Scholar] [CrossRef]
- Yap, H.K.; Lim, J.H.; Nasrallah, F.; Yeow, C.H. Design and Preliminary Feasibility Study of a Soft Robotic Glove for Hand Function Assistance in Stroke Survivors. Front. Neurosci. 2017, 11, 547. [Google Scholar] [CrossRef] [Green Version]
- Proulx, C.E.; Beaulac, M.; David, M.; Deguire, C.; Haché, C.; Klug, F.; Kupnik, M.; Higgins, J.; Gagnon, D.H. Review of the effects of soft robotic gloves for activity-based rehabilitation in individuals with reduced hand function and manual dexterity following a neurological event. J. Rehabil. Assist. Technol. Eng. 2020, 7, 2055668320918130. [Google Scholar] [CrossRef]
- Osuagwu, B.A.C.; Timms, S.; Peachment, R.; Dowie, S.; Thrussell, H.; Cross, S.; Shirley, R.; Segura-Fragoso, A.; Taylor, J. Home-based rehabilitation using a soft robotic hand glove device leads to improvement in hand function in people with chronic spinal cord injury:a pilot study. J. NeuroEng. Rehabil. 2020, 17, 40. [Google Scholar] [CrossRef]
- Saarakkala, S.; Dávila-Vilchis, J.M.; Ávila-Vilchis, J.C.; Vilchis-González, A.H.; Avilés, L. Design Criteria of Soft Exogloves for Hand Rehabilitation-Assistance Tasks. Appl. Bionics Biomech. 2020, 2020, 2724783. [Google Scholar] [CrossRef]
- Cappello, L.; Meyer, J.T.; Galloway, K.C.; Peisner, J.D.; Granberry, R.; Wagner, D.A.; Engelhardt, S.; Paganoni, S.; Walsh, C.J. Assisting hand function after spinal cord injury with a fabric-based soft robotic glove. J. NeuroEng. Rehabil. 2018, 15, 59. [Google Scholar] [CrossRef] [PubMed]
- Adams, R.J.; Ellington, A.L.; Armstead, K.; Sheffield, K.; Patrie, J.T.; Diamond, P.T. Upper Extremity Function Assessment Using a Glove Orthosis and Virtual Reality System. OTJR Occup. Particip. Health 2019, 39, 81–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mancuso, V.; Stramba-Badiale, C.; Cavedoni, S.; Pedroli, E.; Cipresso, P.; Riva, G. Virtual Reality Meets Non-invasive Brain Stimulation: Integrating Two Methods for Cognitive Rehabilitation of Mild Cognitive Impairment. Front. Neurol. 2020, 11, 566731. [Google Scholar] [CrossRef] [PubMed]
- Lu, L.; Zhang, J.; Xie, Y.; Gao, F.; Xu, S.; Wu, X.; Ye, Z. Wearable Health Devices in Health Care: Narrative Systematic Review. JMIR MHealth UHealth 2020, 8, e18907. [Google Scholar] [CrossRef]
- Cerf, V.G. Internet and Jurisdiction. IEEE Internet Comput. 2018, 22, 104-c3. [Google Scholar] [CrossRef] [Green Version]
- Qadri, Y.A.; Nauman, A.; Zikria, Y.B.; Vasilakos, A.V.; Kim, S.W. The Future of Healthcare Internet of Things: A Survey of Emerging Technologies. IEEE Commun. Surv. Tutor. 2020, 22, 1121–1167. [Google Scholar] [CrossRef]
- Emmerich, P.; Gallenmüller, S.; Raumer, D.; Wohlfart, F.; Carle, G. MoonGen: A Scriptable High-Speed Packet Generator. In Proceedings of the 2015 Internet Measurement Conference, Tokyo, Japan, 28–30 October 2015; pp. 275–287. [Google Scholar] [CrossRef] [Green Version]
- Kirsch, J.; Noll, A.; Strese, M.; Liu, Q.; Steinbach, E. A Low-Cost Acquisition, Display, and Evaluation Setup for Tactile Codec Development. In Proceedings of the 2018 IEEE International Symposium on Haptic, Audio and Visual Environments and Games (HAVE), Dalian, China, 20–21 September 2018; pp. 1–6. [Google Scholar] [CrossRef]
- Seeling, P.; Reisslein, M. Video Transport Evaluation with H.264 Video Traces. IEEE Commun. Surv. Tutor. 2012, 14, 1142–1165. [Google Scholar] [CrossRef] [Green Version]
- Jain, R. The Art of Computer Systems Performance Analysis; Wiley: Hoboken, NJ, USA, 1991. [Google Scholar] [CrossRef]
- Smith, A.S.; Trevelyan, E. The Older Population in Rural America: 2012–2016. In American Community Survey Reports ACS-41; U.S. Census Bureau: Washington, DC, USA, 2018. [Google Scholar]
- U.S. Department of Homeland Security. Hospitals Data Set. Homeland Infrastructure Foundation-Level Data (HIFLD) Database, 2020. Available online: https://hifld-geoplatform.opendata.arcgis.com/datasets/geoplatform::hospitals-1 (accessed on 29 November 2021).
- U.S. Department of Homeland Security. Cellular Towers Data Set. Homeland Infrastructure Foundation-Level Data (HIFLD) Database, 2020. Available online: https://hifld-geoplatform.opendata.arcgis.com/datasets/cellular-towers-5 (accessed on 29 November 2021).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Interaction/Applications | Round-Trip Latency Requirement | |
|---|---|---|
| pxHuman–Machine Interaction (Sensitivity to Neural Timing among Cortical Areas [20,21]) | Tactile | <1 ms |
| Auditory | <3 ms | |
| Visual | <15 ms | |
| Motion Control Applications [22] | Machine Tool | <0.5 ms |
| Packaging Machine | <1 ms | |
| Printing Machine | <2 ms |
| Tactile | Auditory | Visual | |
|---|---|---|---|
| Baseline | 1.450 | 0.772 | 3.172 |
| Baseline + BG | 5.049 | 44.576 | 273.675 |
| IEEE 802.1Q + BG | 1.451 | 5.042 | 4.128 |
| IEEE 802.1Qbv + BG | 13.756 | 98.081 | 771.183 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Senk, S.; Ulbricht, M.; Tsokalo, I.; Rischke, J.; Li, S.-C.; Speidel, S.; Nguyen, G.T.; Seeling, P.; Fitzek, F.H.P. Healing Hands: The Tactile Internet in Future Tele-Healthcare. Sensors 2022, 22, 1404. https://0-doi-org.brum.beds.ac.uk/10.3390/s22041404
Senk S, Ulbricht M, Tsokalo I, Rischke J, Li S-C, Speidel S, Nguyen GT, Seeling P, Fitzek FHP. Healing Hands: The Tactile Internet in Future Tele-Healthcare. Sensors. 2022; 22(4):1404. https://0-doi-org.brum.beds.ac.uk/10.3390/s22041404
Chicago/Turabian StyleSenk, Stefan, Marian Ulbricht, Ievgenii Tsokalo, Justus Rischke, Shu-Chen Li, Stefanie Speidel, Giang T. Nguyen, Patrick Seeling, and Frank H. P. Fitzek. 2022. "Healing Hands: The Tactile Internet in Future Tele-Healthcare" Sensors 22, no. 4: 1404. https://0-doi-org.brum.beds.ac.uk/10.3390/s22041404