
The Reliability and Validity of a Portable Three-Dimensional Scanning System to Measure Leg Volume

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
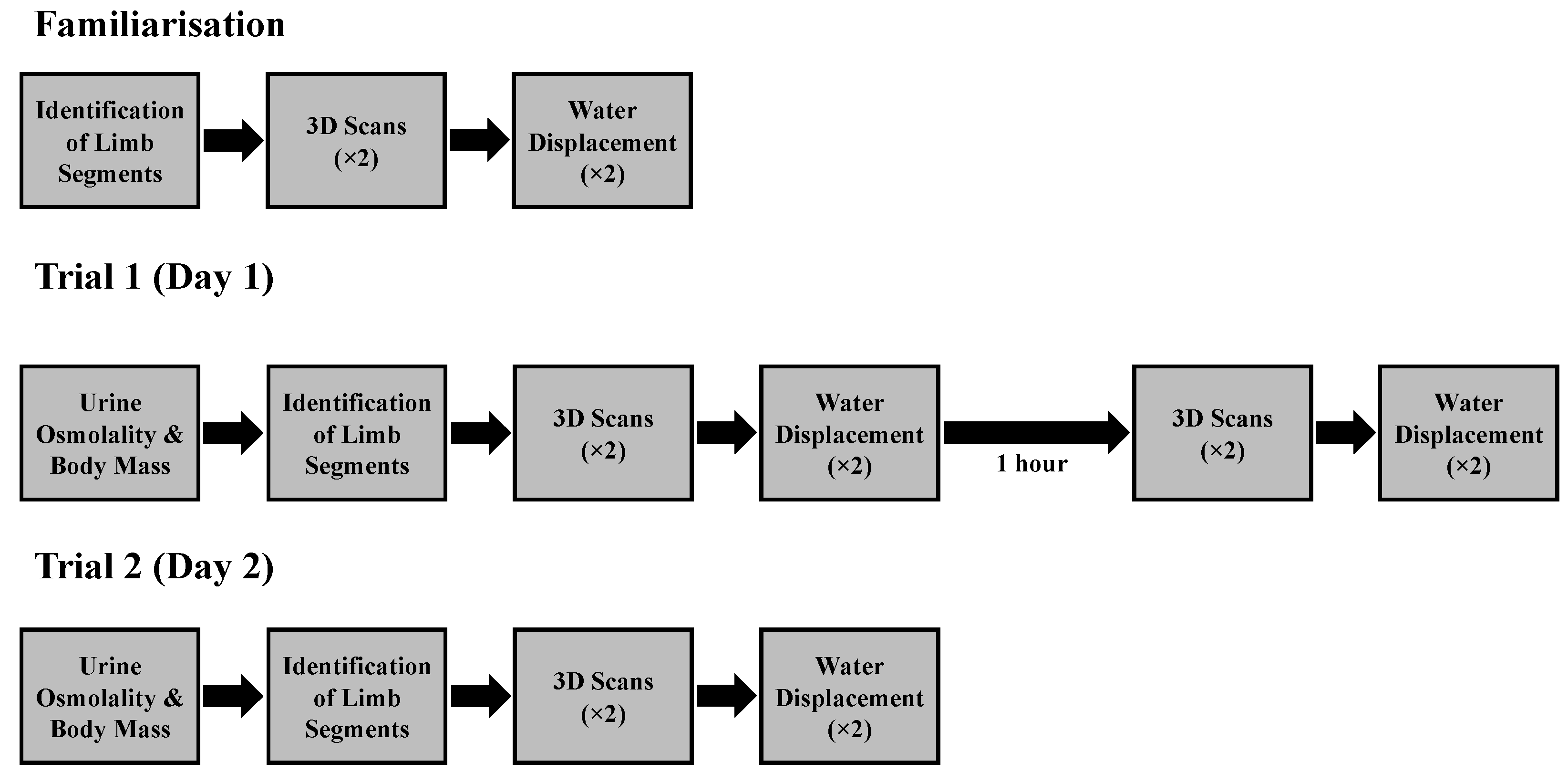
2.2. Experimental Design
2.3. Leg Volume Locations
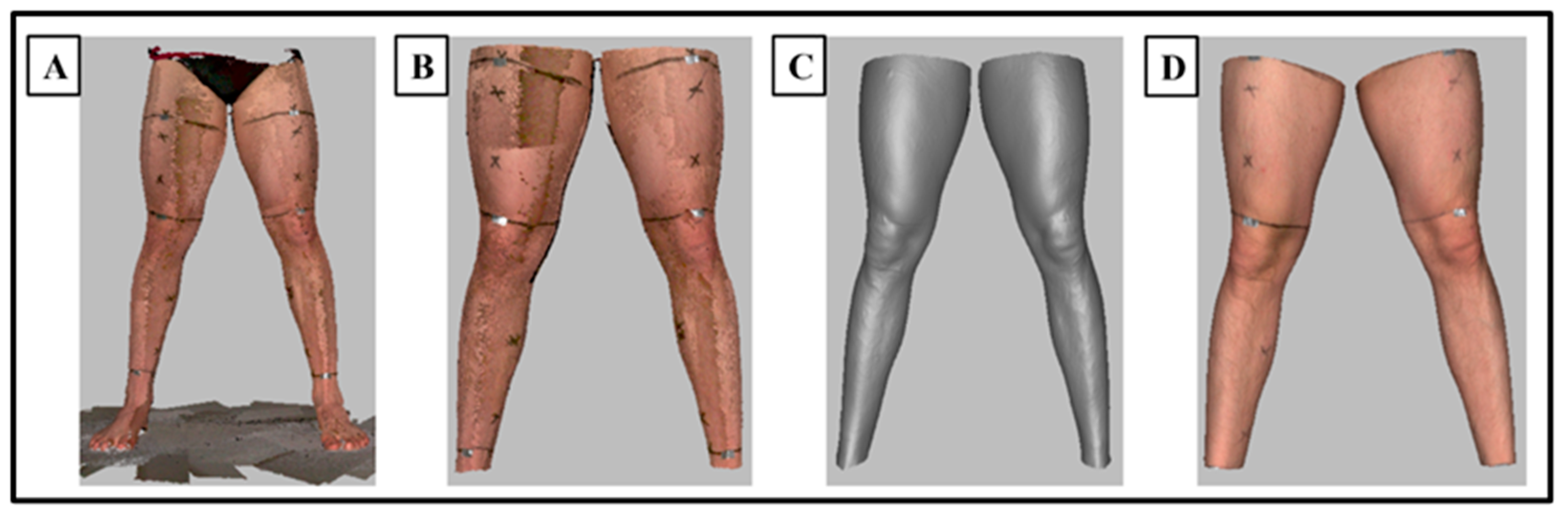
2.4. 3D Scanning Procedure
2.5. 3D Scan Processing
2.6. 3D Scan Volume Extraction
2.7. Water Displacement Procedure
2.8. Data Analysis
2.9. Statistical Analysis
3. Results
3.1. 3D Scanning: Test–Retest Reliability (Lower Leg)
3.2. Water Displacement: Test–Retest Reliability (Lower Leg)
3.3. 3D Scanning: Test–Retest Reliability (Upper Leg)
3.4. Water Displacement: Test–Retest Reliability (Upper Leg)
3.5. 3D Scanning: Intra- and Inter-Day Reliability (Lower Leg)
3.6. Water Displacement: Intra- and Inter-Day Reliability (Lower Leg)
3.7. 3D Scanning: Intra- and Inter-Day Reliability (Upper Leg)
3.8. Water Displacement: Intra- and Inter-Day Reliability (Upper Leg)
3.9. 3D Scanning versus Water Displacement: Validity (Lower Leg)
3.10. 3D Scanning versus Water Displacement: Validity (Upper Leg)
3.11. Hydration Status and Body Mass
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brijker, F.; Heijdra, Y.F.; Van Den Elshout, F.J.; Bosch, F.H.; Folgering, H.T. Volumetric Measurements of Peripheral Oedema in Clinical Conditions. Clin. Physiol. 2000, 20, 56–61. [Google Scholar] [CrossRef]
- Ribeiro, C.; Lima, S.; Carreira, A.; Masiero, D.; Chamlian, T. Inter-Tester Reliability Assessment of the Volumetric Measurement of the Hand in Subjects without Any Changes in Their Upper Extremities. Acta Fisiatr. 2010, 17, 3–7. [Google Scholar] [CrossRef]
- Ridner, S.H.; Montgomery, L.D.; Hepworth, J.T.; Stewart, B.R.; Armer, J.M. Comparison of Upper Limb Volume Measurement Techniques and Arm Symptoms between Healthy Volunteers and Individuals with Known Lymphedema. Lymphology 2007, 40, 35–46. [Google Scholar]
- Chromy, A.; Zalud, L.; Dobsak, P.; Suskevic, I.; Mrkvicova, V. Limb Volume Measurements: Comparison of Accuracy and Decisive Parameters of the Most Used Present Methods. Springerplus 2015, 4, 707. [Google Scholar] [CrossRef]
- Cerqueira, M.S.; Santos Borges, L.; dos Santos Rocha, J.A.; Brito Andrade, H.; Silva PirÔpo, U.; Lupato Conrado, L.A.; Pereira, R. Twelve Hours of a Compression Sleeve Is Not Enough to Improve the Muscle Recovery of an Exercise-Damaged Upper Arm. Apunt. Med. l’Esport 2015, 50, 23–28. [Google Scholar] [CrossRef]
- Tan, C.W.; Coutts, F.; Bulley, C. Measurement of Lower Limb Volume: Agreement between the Vertically Oriented Perometer and a Tape Measure Method. Physiotherapy 2013, 99, 247–251. [Google Scholar] [CrossRef]
- Man, I.O.W.; Markland, K.L.; Morrissey, M.C. The Validity and Reliability of the Perometer in Evaluating Human Knee Volume. Clin. Physiol. Funct. Imaging 2004, 24, 352–358. [Google Scholar] [CrossRef]
- Pasley, J.D.; O’Connor, P.J. High Day-to-Day Reliability in Lower Leg Volume Measured by Water Displacement. Eur. J. Appl. Physiol. 2008, 103, 393–398. [Google Scholar] [CrossRef]
- Heiss, R.; Hotfiel, T.; Kellermann, M.; May, M.S.; Wuest, W.; Janka, R.; Nagel, A.M.; Uder, M.; Hammon, M. Effect of Compression Garments on the Development of Edema and Soreness in Delayed-Onset Muscle Soreness (DOMS). J. Sports Sci. Med. 2018, 17, 392–401. [Google Scholar]
- Kremer, R.L.; Wolfe, M.E.; Brueckner, N.J.; Viola, M.C.; Fisher, M.I. Validity and Reliability of Three-Dimensional Imaging to Measure Limb Volume: A Systematic Review. Phys. Ther. Rev. 2020, 25, 21–28. [Google Scholar] [CrossRef]
- Sharkey, A.R.; King, S.W.; Kuo, R.Y.; Bickerton, S.B.; Ramsden, A.J.; Furniss, D. Measuring Limb Volume: Accuracy and Reliability of Tape Measurement Versus Perometer Measurement. Lymphat. Res. Biol. 2018, 16, 182–186. [Google Scholar] [CrossRef]
- Fernie, G.R.; Holliday, P.J. Volume Fluctuations in the Residual Limbs of Lower Limb Amputees. Arch. Phys. Med. Rehabil. 1982, 63, 162–165. [Google Scholar]
- Seminati, E.; Talamas, D.C.; Young, M.; Twiste, M.; Dhokia, V.; Bilzon, J.L.J. Validity and Reliability of a Novel 3D Scanner for Assessment of the Shape and Volume of Amputees’ Residual Limb Models. PLoS ONE 2017, 12, e0184498. [Google Scholar] [CrossRef]
- Rabe, E.; Stücker, M.; Ottillinger, B. Water Displacement Leg Volumetry in Clinical Studies—A Discussion of Error Sources. BMC Med. Res. Methodol. 2010, 10, 5. [Google Scholar] [CrossRef]
- Deltombe, T.; Jamart, J.; Recloux, S.; Legrand, C.; Vandenbroeck, N.; Theys, S.; Hanson, P. Reliability and Limits of Agreement of Circumferential, Water Displacement, and Optoelectronic Volumetry in the Measurement of Upper Limb Lymphedema. Lymphology 2007, 40, 26–34. [Google Scholar]
- Megens, A.M.; Harris, S.R.; Kim-Sing, C.; McKenzie, D.C. Measurement of Upper Extremity Volume in Women after Axillary Dissection for Breast Cancer. Arch. Phys. Med. Rehabil. 2001, 82, 1639–1644. [Google Scholar] [CrossRef]
- Sander, A.P.; Hajer, N.M.; Hemenway, K.; Miller, A.C. Upper-Extremity Volume Measurements in Women With Lymphedema: A Comparison of Measurements Obtained Via Water Displacement With Geometrically Determined Volume. Phys. Ther. 2002, 82, 1201–1212. [Google Scholar] [CrossRef]
- Buffa, R.; Mereu, E.; Lussu, P.; Succa, V.; Pisanu, T.; Buffa, F.; Marini, E. A New, Effective and Low-Cost Three-Dimensional Approach for the Estimation of Upper-Limb Volume. Sensors 2015, 15, 12342–12357. [Google Scholar] [CrossRef]
- Cau, N.; Galli, M.; Cimolin, V.; Aranci, M.; Caraceni, A.; Balzarini, A. Comparative Study between Circumferential Method and Laser Scanner 3D Method for the Evaluation of Arm Volume in Healthy Subjects. J. Vasc. Surg. Venous Lymphat. Disord. 2016, 4, 64–72. [Google Scholar] [CrossRef]
- Harrison, J.A.; Nixon, M.A.; Fright, W.R.; Snape, L. Use of Hand-Held Laser Scanning in the Assessment of Facial Swelling: A Preliminary Study. Br. J. Oral Maxillofac. Surg. 2004, 42, 8–17. [Google Scholar] [CrossRef]
- Modabber, A.; Peters, F.; Kniha, K.; Goloborodko, E.; Ghassemi, A.; Lethaus, B.; Hölzle, F.; Möhlhenrich, S.C. Evaluation of the Accuracy of a Mobile and a Stationary System for Three-Dimensional Facial Scanning. J. Craniomaxillofac. Surg. 2016, 44, 1719–1724. [Google Scholar] [CrossRef]
- Yamamoto, S.; Miyachi, H.; Fujii, H.; Ochiai, S.; Watanabe, S.; Shimozato, K. Intuitive Facial Imaging Method for Evaluation of Postoperative Swelling: A Combination of 3-Dimensional Computed Tomography and Laser Surface Scanning in Orthognathic Surgery. J. Oral Maxillofac. Surg. 2016, 74, 2506.e1–2506.e10. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, G.; Nevill, A.M. Selected Issues in the Design and Analysis of Sport Performance Research. J. Sports Sci. 2001, 19, 811–827. [Google Scholar] [CrossRef] [PubMed]
- Boland, R.; Adams, R. Development and Evaluation of a Precision Forearm and Hand Volumeter and Measuring Cylinder. J. Hand Ther. 1996, 9, 349–358. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Statistical Methods for Assessing Agreement between Two Methods of Clinical Measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef] [PubMed]
- Schober, P.; Schwarte, L.A. Correlation Coefficients: Appropriate Use and Interpretation. Anesth. Analg. 2018, 126, 1763–1768. [Google Scholar] [CrossRef] [PubMed]
- Nevill, A.M.; Atkinson, G. Assessing Agreement between Measurements Recorded on a Ratio Scale in Sports Medicine and Sports Science. Br. J. Sports Med. 1997, 31, 314–318. [Google Scholar] [CrossRef]
- McKinnon, J.G.; Wong, V.; Temple, W.J.; Galbraith, C.; Ferry, P.; Clynch, G.S.; Clynch, C. Measurement of Limb Volume: Laser Scanning versus Volume Displacement. J. Surg. Oncol. 2007, 96, 381–388. [Google Scholar] [CrossRef]
- Stout, N.; Partsch, H.; Szolnoky, G.; Forner-Cordero, I.; Mosti, G.; Mortimer, P.; Flour, M.; Damstra, R.; Piller, N.; Geyer, M.J.; et al. Chronic Edema of the Lower Extremities: International Consensus Recommendations for Compression Therapy Clinical Research Trials. Int. Angiol. 2012, 31, 316–329. [Google Scholar]
- Armer, J.M.; Stewart, B.R. A Comparison of Four Diagnostic Criteria for Lymphedema in a Post-Breast Cancer Population. Lymphat. Res. Biol. 2005, 3, 208–217. [Google Scholar] [CrossRef]
- Asim, M.; Cham, A.; Banerjee, S.; Nancekivell, R.; Dutu, G.; McBride, C.; Cavanagh, S.; Lawrenson, R.; Campbell, I. Difficulties with Defining Lymphoedema after Axillary Dissection for Breast Cancer. N. Z. Med. J. 2012, 125, 29–39. [Google Scholar]
- Johansson, K.; Ingvar, C.; Albertsson, M.; Ekdahl, C. Arm Lymphoedema, Shoulder Mobility and Muscle Strength after Breast Cancer Treatment ? A Prospective 2-Year Study. Adv. Physiother. 2001, 3, 55–66. [Google Scholar] [CrossRef]
- Whitehead, N.P.; Allen, T.J.; Morgan, D.L.; Proske, U. Damage to Human Muscle from Eccentric Exercise after Training with Concentric Exercise. J. Physiol. 1998, 512, 615–620. [Google Scholar] [CrossRef]
- Whitehead, N.P.; Weerakkody, N.S.; Gregory, J.E.; Morgan, D.L.; Proske, U. Changes in Passive Tension of Muscle in Humans and Animals after Eccentric Exercise. J. Physiol. 2001, 533, 593–604. [Google Scholar] [CrossRef]
- Engelberger, R.P.; Indermühle, A.; Baumann, F.; Fahrni, J.; Diehm, N.; Kucher, N.; Egermann, U.; Laederach, K.; Baumgartner, I.; Willenberg, T. Diurnal Changes of Lower Leg Volume in Obese and Non-Obese Subjects. Int. J. Obes. 2014, 38, 801–805. [Google Scholar] [CrossRef]
- Hebeda, C.L.; de Boer, E.M.; Verburgh, C.A.; Krijnen, R.M.A.; Nieboer, C.; Bezemer, P.D. Lower Limb Volume Measurements: Standardization and Reproducibility of an Adapted Optical Leg Volume Meter. Phlebology 1993, 8, 162–166. [Google Scholar] [CrossRef]
- Zhou, C.; Yahathugoda, C.; De Silva, L.; Rathnapala, U.; Owen, G.; Weerasooriya, M.; Rao, R.U.; Weil, G.J.; Budge, P.J. Portable Infrared Imaging for Longitudinal Limb Volume Monitoring in Patients with Lymphatic Filariasis. PLoS Negl. Trop. Dis. 2019, 13, e0007762. [Google Scholar] [CrossRef] [PubMed]
- Angelhed, J.-E.; Strid, L.; Bergelin, E.; Fagerberg, B. Measurement of Lower-Leg Volume Change by Quantitative Computed Tomography. Acta Radiol. 2008, 49, 1024–1030. [Google Scholar] [CrossRef] [PubMed]
- Kaulesar Sukul, D.M.; den Hoed, P.T.; Johannes, E.J.; van Dolder, R.; Benda, E. Direct and Indirect Methods for the Quantification of Leg Volume: Comparison between Water Displacement Volumetry, the Disk Model Method and the Frustum Sign Model Method, Using the Correlation Coefficient and the Limits of Agreement. J. Biomed. Eng. 1993, 15, 477–480. [Google Scholar] [CrossRef]
- Dickinson, A.S.; Donovan-Hall, M.K.; Kheng, S.; Bou, K.; Steer, J.W.; Metcalf, C.D.; Worsley, P.R. Selecting Appropriate 3D Scanning Technologies for Prosthetic Socket Design and Transtibial Residual Limb Shape Characterization. J. Prosthet. Orthot. 2022, 34, 33–43. [Google Scholar] [CrossRef]
- Doomen, M.C.H.A.; Rijpma, D.; Pijpe, A.; Meij-de Vries, A.; Niessen, F.B.; Karaoglu, S.; de Vet, H.C.W.; Gevers, T.; van Zuijlen, P.P.M. A Clinimetric Assessment of the Validity and Reliability of 3D Technology for Scar Surface Area Measurement. Burns 2023, 49, 583–594. [Google Scholar] [CrossRef] [PubMed]
- Kecelj-Leskovec, N.; Jezeršek, M.; Možina, J.; Pavlović, M.D.; Lunder, T. Measurement of Venous Leg Ulcers with a Laser-Based Three-Dimensional Method: Comparison to Computer Planimetry with Photography. Wound Repair Regen. 2007, 15, 767–771. [Google Scholar] [CrossRef] [PubMed]
- Hassan, N.M.; Buldt, A.K.; Shields, N.; Landorf, K.B.; Menz, H.B.; Munteanu, S.E. Differences in Foot Dimensions between Children and Adolescents with and without Down Syndrome. Disabil. Rehabil. 2022, 44, 3959–3966. [Google Scholar] [CrossRef]
- Rauter, S.; Simenko, J. Morphological Asymmetries Profile and the Difference between Low-and High-Performing Road Cyclists Using 3d Scanning. Biology 2021, 10, 1199. [Google Scholar] [CrossRef] [PubMed]
- Derouchey, J.D.; Tomkinson, G.R.; Rhoades, J.L.; Fitzgerald, J.S. Reliability of the Styku 3D Whole-Body Scanner for the Assessment of Body Size in Athletes. Meas Phys. Educ. Exerc. Sci. 2020, 24, 228–234. [Google Scholar] [CrossRef]
- Brown, F.C.W.; Hill, J.A.; van Someren, K.; Howatson, G.; Pedlar, C.R. The Effect of Custom-Fitted Compression Garments Worn Overnight for Recovery from Judo Training in Elite Athletes. Eur. J. Sport Sci. 2022, 22, 521–529. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline | 1 h Post Baseline | 24 h Post Baseline | |
|---|---|---|---|
| Sample Size | n = 30 | n = 30 | n = 30 |
| Measurement 1 (X ± SD) [mL] | 3405 ± 330 | 3466 ± 372 | 3413 ± 306 |
| Measurement 2 (X ± SD) [mL] | 3443 ± 355 | 3483 ± 369 | 3427 ± 316 |
| Systematic Bias (mL) | 38 | 17 | 14 |
| LOA (mL) | 134 | 126 | 134 |
| Lower; Upper LOA (raw) | −97; 172 | −109; 143 | −120; 148 |
| Systematic Bias (ln) | 1.01 | 1.01 | 1.00 |
| LOA (ln) | 1.04 | 1.04 | 1.04 |
| Lower; Upper LOA (ln) | 0.97; 1.05 | 0.97; 1.04 | 0.96; 1.05 |
| Pearsons r | 0.98 (p < 0.001) | 0.99 (p < 0.001) | 0.98 (p < 0.001) |
| Baseline | 1 h Post Baseline | 24 h Post Baseline | |
|---|---|---|---|
| Sample Size | n = 30 | n = 30 | n = 30 |
| Measurement 1 (X ± SD) [mL] | 3086 ± 502 | 3359 ± 519 | 3149 ± 478 |
| Measurement 2 (X ± SD) [mL] | 3052 ± 497 | 3346 ± 568 | 3092 ± 478 |
| Systematic Bias (mL) | −33 | −13 | −56 |
| LOA (mL) | 168 | 187 | 190 |
| Lower; Upper LOA (raw) | −202; 135 | −200; 174 | −246; 134 |
| Systematic Bias (ln) | 0.99 | 0.99 | 0.98 |
| LOA (ln) | 1.05 | 1.06 | 1.07 |
| Lower; Upper LOA (ln) | 0.94; 1.04 | 0.94; 1.05 | 0.92; 1.05 |
| Pearsons r | 0.99 (p < 0.001) | 0.99 (p < 0.001) | 0.98 (p < 0.001) |
| Baseline | 1 h Post Baseline | 24 h Post Baseline | |
|---|---|---|---|
| Sample Size | n = 30 | n = 30 | n = 30 |
| Measurement 1 (X ± SD) [mL] | 5288 ± 664 | 5283 ± 685 | 5280 ± 662 |
| Measurement 2 (X ± SD) [mL] | 5343 ± 655 | 5305 ± 679 | 5274 ± 671 |
| Systematic Bias (mL) | 55 | 22 | −6 |
| LOA (mL) | 219 | 173 | 176 |
| Lower; Upper LOA (raw) | −164; 274 | −151; 195 | −183; 170 |
| Systematic Bias (ln) | 1.01 | 1.00 | 1.00 |
| LOA (ln) | 1.05 | 1.03 | 1.04 |
| Lower; Upper LOA (ln) | 0.97; 1.06 | 0.97; 1.04 | 0.96; 1.04 |
| Pearsons r | 0.99 (p < 0.001) | 0.99 (p < 0.001) | 0.99 (p < 0.001) |
| Baseline | 1 h Post Baseline | 24 h Post Baseline | |
|---|---|---|---|
| Sample Size | n = 30 | n = 30 | n = 30 |
| Measurement 1 (X ± SD) [mL] | 5355 ± 658 | 5461 ± 662 | 5349 ± 665 |
| Measurement 2 (X ± SD) [mL] | 5325 ± 692 | 5413 ± 673 | 5308 ± 654 |
| Systematic Bias (mL) | −30 | −48 | −41 |
| LOA (mL) | 315 | 186 | 272 |
| Lower; Upper LOA (raw) | −344; 285 | −233; 138 | −313; 231 |
| Systematic Bias (ln) | 0.99 | 0.99 | 0.99 |
| LOA (ln) | 1.06 | 1.04 | 1.06 |
| Lower; Upper LOA (ln) | 0.94; 1.05 | 0.96; 1.03 | 0.94; 1.05 |
| Pearsons r | 0.97 (p < 0.001) | 0.99 (p < 0.001) | 0.98 (p < 0.001) |
| Baseline vs. 1 h Post Baseline | Baseline vs. 24 h Post Baseline | |
|---|---|---|
| Sample Size | n = 30 | n = 30 |
| 3D Scan (X ± SD) [mL] | 3404 ± 382 | 3404 ± 382 |
| 3D Scan (X ± SD) [mL] | 3456 ± 386 | 3388 ± 347 |
| Systematic Bias (mL) | 52 | −16 |
| LOA (mL) | 208 | 191 |
| Lower; Upper LOA (raw) | −155; 260 | −207; 174 |
| Systematic Bias (ln) | 1.02 | 1.00 |
| LOA (ln) | 1.07 | 1.06 |
| Lower; Upper LOA (ln) | 0.95; 1.08 | 0.99; 1.05 |
| Pearsons r | 0.96 (p < 0.001) | 0.97 (p < 0.001) |
| Baseline vs. 1 h Post Baseline | Baseline vs. 24 h Post Baseline | |
|---|---|---|
| Sample Size | n = 30 | n = 30 |
| WD (X ± SD) [mL] | 3102 ± 507 | 3102 ± 507 |
| WD (X ± SD) [mL] | 3366 ± 532 | 3143 ± 462 |
| Systematic Bias (mL) | 263 | 40 |
| LOA (mL) | 615 | 485 |
| Lower; Upper LOA (raw) | −351; 878 | −445; 525 |
| Systematic Bias (ln) | 1.09 | 1.02 |
| LOA (ln) | 1.20 | 1.16 |
| Lower; Upper LOA (ln) | 0.91; 1.30 | 0.87; 1.18 |
| Pearsons r | 0.82 (p < 0.001) | 0.87 (p < 0.001) |
| Baseline vs. 1 h Post Baseline | Baseline vs. 24 h Post Baseline | |
|---|---|---|
| Sample Size | n = 30 | n = 30 |
| 3D Scan (X ± SD) [mL] | 5311 ± 654 | 5311 ± 654 |
| 3D Scan (X ± SD) [mL] | 5334 ± 646 | 5315 ± 622 |
| Systematic Bias (mL) | 23 | 4 |
| LOA (mL) | 224 | 258 |
| Lower; Upper LOA (raw) | −201; 247 | −254; 262 |
| Systematic Bias (ln) | 1.01 | 1.00 |
| LOA (ln) | 1.04 | 1.05 |
| Lower; Upper LOA (ln) | 0.97; 1.05 | 0.95; 1.06 |
| Pearsons r | 0.98 (p < 0.001) | 0.98 (p < 0.001) |
| Baseline vs. 1 h Post Baseline | Baseline vs. 24 h Post Baseline | |
|---|---|---|
| Sample Size | n = 30 | n = 30 |
| WD (X ± SD) [mL] | 5351 ± 657 | 5351 ± 657 |
| WD (X ± SD) [mL] | 5431 ± 638 | 5340 ± 654 |
| Systematic Bias (mL) | 80 | −10 |
| LOA (mL) | 365 | 448 |
| Lower; Upper LOA (raw) | −285; 445 | −458; 438 |
| Systematic Bias (ln) | 1.02 | 1.00 |
| LOA (ln) | 1.08 | 1.09 |
| Lower; Upper LOA (ln) | 0.95; 1.09 | 0.91; 1.09 |
| Pearsons r | 0.96 (p < 0.001) | 0.94 (p < 0.001) |
| Baseline | 1 h Post Baseline | 24 h Post Baseline | |
|---|---|---|---|
| Sample Size | n = 30 | n = 30 | n = 30 |
| WD Volume (X ± SD) [mL] | 3102 ± 507 | 3366 ± 532 | 3143 ± 462 |
| 3D Scan Volume (X ± SD) [mL] | 3404 ± 382 | 3456 ± 386 | 3388 ± 347 |
| Systematic Bias (mL) | 302 | 91 | 245 |
| LOA (mL) | 696 | 464 | 544 |
| Lower; Upper LOA (raw) | −394; 998 | −373; 554 | −299; 789 |
| Systematic Bias (ln) | 1.10 | 1.03 | 1.08 |
| LOA (ln) | 1.27 | 1.15 | 1.20 |
| Lower; Upper LOA (ln) | 0.87; 1.40 | 0.90; 1.19 | 0.90; 1.30 |
| Pearsons r | 0.71 (p < 0.001) | 0.92 (p < 0.001) | 0.80 (p < 0.001) |
| Baseline | 1 h Post Baseline | 24 h Post Baseline | |
|---|---|---|---|
| Sample Size | n = 30 | n = 30 | n = 30 |
| WD Volume (X ± SD) [mL] | 5351 ± 657 | 5431 ± 638 | 5340 ± 654 |
| 3D Scan Volume (X ± SD) [mL] | 5311 ± 654 | 5334 ± 646 | 5315 ± 622 |
| Systematic Bias (mL) | −40 | −96 | −25 |
| LOA (mL) | 324 | 365 | 408 |
| Lower; Upper LOA (raw) | −364; 284 | −491; 299 | −433; 383 |
| Systematic Bias (ln) | 0.99 | 0.98 | 1.00 |
| LOA (ln) | 1.07 | 1.08 | 1.09 |
| Lower; Upper LOA (ln) | 0.93; 1.06 | 0.91; 1.06 | 0.91; 1.09 |
| Pearsons r | 0.97 (p < 0.001) | 0.95 (p < 0.001) | 0.95 (p < 0.001) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ashby, J.; Lewis, M.; Sunderland, C.; Barrett, L.A.; Morris, J.G. The Reliability and Validity of a Portable Three-Dimensional Scanning System to Measure Leg Volume. Sensors 2023, 23, 9177. https://0-doi-org.brum.beds.ac.uk/10.3390/s23229177
Ashby J, Lewis M, Sunderland C, Barrett LA, Morris JG. The Reliability and Validity of a Portable Three-Dimensional Scanning System to Measure Leg Volume. Sensors. 2023; 23(22):9177. https://0-doi-org.brum.beds.ac.uk/10.3390/s23229177
Chicago/Turabian StyleAshby, Jack, Martin Lewis, Caroline Sunderland, Laura A. Barrett, and John G. Morris. 2023. "The Reliability and Validity of a Portable Three-Dimensional Scanning System to Measure Leg Volume" Sensors 23, no. 22: 9177. https://0-doi-org.brum.beds.ac.uk/10.3390/s23229177