
New Hemodynamic Parameters in Peri-Operative and Critical Care—Challenges in Translation

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
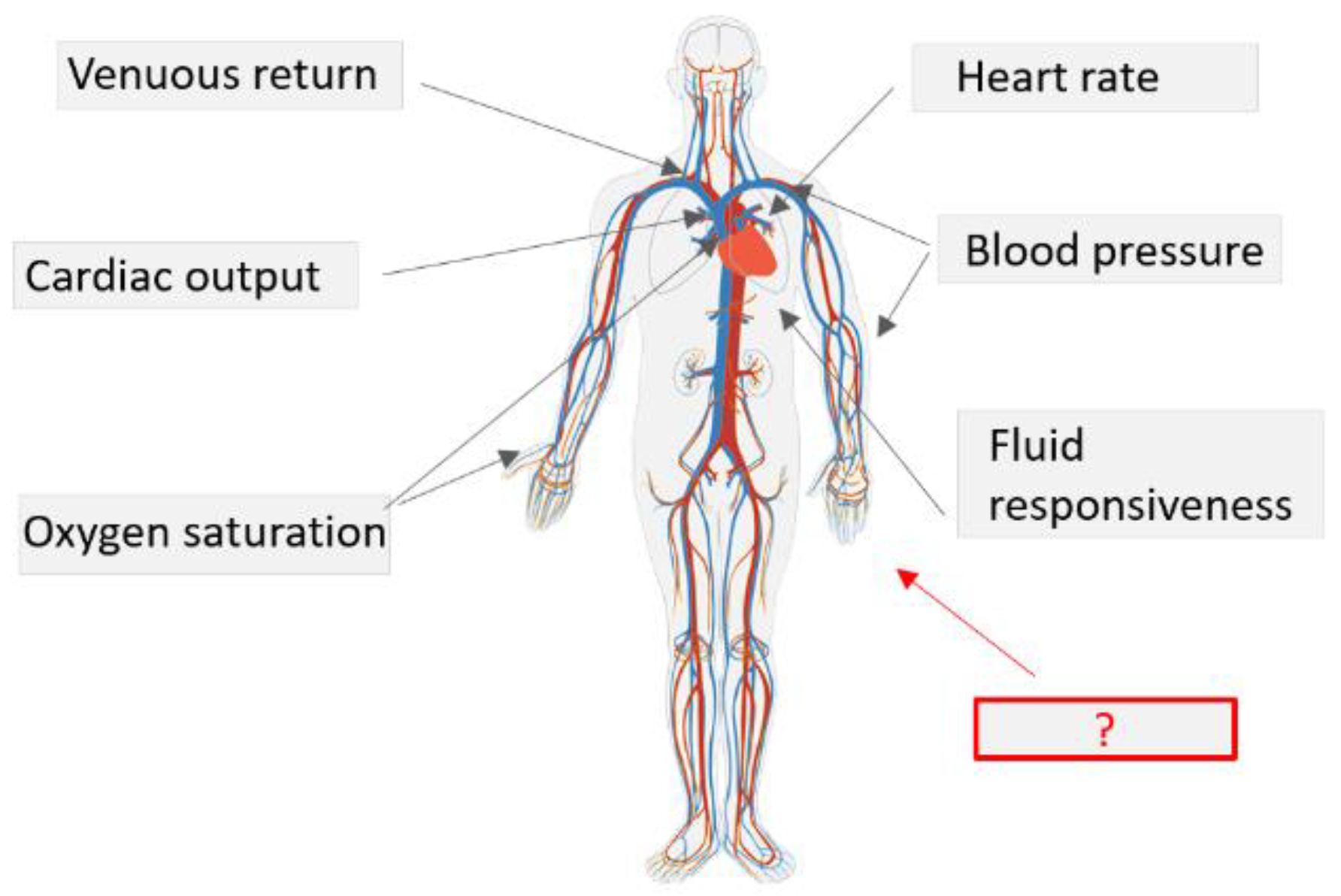
- Interpretation of the widely used parameters via functional hemodynamic monitoring. This is based on measuring the response of the circulatory system to a defined stimulus [1].
- Measurement of the microcirculation [13]—direct assessment of the pathways of oxygen delivery and of the primary site at which oxygen exchange takes place.
- Emerging technologies for characterization of dynamic vascular regulation—recent cardiovascular research is focused on the study of natural compensatory mechanisms. Changes in vascular properties (compliance, viscosity, and artery-vein interaction [18,19,20]) can precede changes in commonly measured hemodynamic indices such as BP, CO.
- Data-driven, machine-learning (ML) assessment of physiological signals. Statistical methods are used to identify complex interactions between physiological signal characteristics to predict adverse hemodynamic events or to estimate variables that are not directly measured.
2. Interpretation of the Widely Used Parameters via Functional Hemodynamic Monitoring
Current Challenges
3. Develop Technology Specifically Designed to Assess Microcirculation
Current Challenges
“Despite their high spatial and temporal resolutions, optical imaging modalities are still not widely used for clinical imaging of the microcirculation due to their limited tissue penetration. Diffuse optical imaging techniques such as NIRS ameliorate this to some extent, but at the expense of spatial resolution.”[48]
4. More Advanced Assessment of the Vascular Properties
4.1. Cardiovascular Research and Its Relevance for Critical Care
“When modeling blood circulation, the heart is usually considered the main element, the only one which has an actual relevance in the operation of the system, thus neglecting blood vessels, which are considered simple conduits that connect the cardiac pump with the organs. Such a basic approach underestimates the prominent role shown by blood vessels in general and by arteries in particular“, “The active stress developed by smooth muscle has been overlooked as a contributor to the mechanic behavior of vessels, although it has been demonstrated that the activation of smooth muscle changes the stress–strain relationship towards high levels of stress”, “This is very important when studying the cardiovascular system given the active participation of the nervous system in hemodynamic regulation.”[19]
4.2. Arterial Stiffness
“An important overarching concept underlying cuffless measurement of blood pressure is the fundamental relationship between transmural pressure and mechanical properties of the arterial wall which influence wave propagation phenomena. This is the pressure dependency of the material stiffness of all blood vessels. This property is present in all species with pressurized circulatory systems and is a fundamental evolutionary property of arterial design.”[18]
“PTT is a measure for arterial stiffness. When blood pressure increases, the vascular tone increases and the arterial wall becomes stiffer, causing the PTT to shorten.”[18]
“Is “Cuffless” the Future of Blood Pressure Monitoring? There have been many patent submissions, start-up companies, and scientific publications, but to date there is no device that is universally accepted by the wider community beyond research laboratories and company boardrooms.”[18]
4.2.1. Insights on Vascular Regulation Mechanisms
4.2.2. Insights on Technology Requirements
4.2.3. Value for Critical Care
Value for Recalibration of Standard Measurements
“The major weakness of all these devices is the drift in values whenever there is a major change in vascular compliance, as, for example, in vascular leak syndrome with increased vessel wall edema leading to decreased arterial compliance.”[6]
Value as Predictive Parameter and Improvement of Blood Pressure Estimation
4.2.4. Current Challenges
“The direct effect of smooth muscle relaxation on arterial elastic properties is controversial.”” In human subjects, the contribution of smooth muscle to arterial elastic mechanics has been limited by difficulty in separating the direct effects of a vasodilator drug on the arterial wall from the indirect effects due to reduced blood pressure.”[59]
4.3. Beyond Arterial Stiffness
“Finally, it is particularly important to note that changes in the compliance and resistance deduced with the aid of the model exhibit a dependency on pressure and flow, respectively, which is characteristic of the compliance and resistance of blood vessels. This suggests that a particularly appropriate application for the model is to use changes in the model parameters to monitor circulatory changes of the limb, such as those, for instance, that may occur during clinical anaesthesia.”[20]
Current Challenges
“It is well known that hemodynamics of large arteries is too complex to be apprehended using only non-invasive measurements and medical imaging techniques.”, “As 3D models can only be used in small portions of the cardiovascular system due to their high modelling and computational costs, reduced-order models have gained attention to reproduce complex wave propagation behaviors in large networks of arteries.”, “Although arterial pressure is easy to measure, the precise measurement of blood pressure requires highly invasive techniques.” [19] “In cases where it is not possible to develop physical models it becomes necessary to use shortcuts based on empirical, statistical, or even simple profile models.”[105]
5. Data-Driven Approaches
“How can one tell whether a pulse is ‘full’, ‘rapid’ or ‘rhythmical’? Is there a perceptible pause when the artery has reached the limit of its contraction and, again, of this expansion? Is there also a pause when the artery returns to its normal size? Such questions Galen resolved partly historically, by referring to earlier authorities, and partly from experience. His own enthusiasm for studying the pulse, which has been with him since youth, and his hours of practice had given him, he claimed, a most sensitive touch, an example worth imitation.”[106]
5.1. Current Challenges
- Cuff-based non-invasive BP measurement algorithms are optimized for normotensive patients, and significant errors in clinical BP readings are being reported in hypo- and hypertensive patients [119].
- An algorithm for predicting kidney injury (DeepMinds [120]) was trained on data collected mainly from patients in a veteran hospital—a demographic that is not representative of the general population.
5.2. Future Possibilities Involving Data Infrastructures and Explainable Artificial Intelligence
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pinsky, M.R.; Payen, D. Functional hemodynamic monitoring. Crit. Care 2005, 9, 566–572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aya, H.D.; Cecconi, M. Determinants of Venous Return. In Hemodynamic Monitoring. Lessons from the ICU (under the Auspices of the European Society of Intensive Care Medicine); Pinsky, M.R., Teboul, J.L., Vincent, J.L., Eds.; Springer: Cham, Switzerland, 2019. [Google Scholar] [CrossRef]
- Kellum, J.A. Rationale for Hemodynamic Monitoring. In Applied Cardiovascular Physiology; Pinsky, M.R., Ed.; Update in Intensive Care and Emergency Medicine; Springer: Berlin/Heidelberg, Germany, 1997; Volume 28. [Google Scholar] [CrossRef]
- Groeneveld, A.B.J. Non-Invasive Hemodynamic and Metabolic Monitoring. In Applied Cardiovascular Physiology; Pinsky, M.R., Ed.; Update in Intensive Care and Emergency Medicine; Springer: Berlin/Heidelberg, Germany, 1997; Volume 28. [Google Scholar] [CrossRef]
- Takala, J. Introduction to “Hemodynamic Monitoring”. In Hemodynamic Monitoring. Lessons from the ICU (under the Auspices of the European Society of Intensive Care Medicine); Pinsky, M.R., Teboul, J.L., Vincent, J.L., Eds.; Springer: Cham, Switzerland, 2019. [Google Scholar] [CrossRef]
- Vincent, J.-L.; Rhodes, A.; Perel, A.; Martin, G.S.; Della Rocca, G.; Vallet, B.; Pinsky, M.R.; Hofer, C.K.; Teboul, J.-L.; De Boode, W.-P.; et al. Clinical review: Update on hemodynamic monitoring—A consensus of 16. Crit. Care 2011, 15, 229. [Google Scholar] [CrossRef] [Green Version]
- Teboul, J.-L.; Saugel, B.; Cecconi, M.; De Backer, D.; Hofer, C.K.; Monnet, X.; Perel, A.; Pinsky, M.R.; Reuter, D.A.; Rhodes, A.; et al. Less invasive hemodynamic monitoring in critically ill patients. Intensiv. Care Med. 2016, 42, 1350–1359. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.-L.; Einav, S.; Pearse, R.; Jaber, S.; Kranke, P.; Overdyk, F.J.; Whitaker, D.K.; Gordo, F.; Dahan, A.; Hoeft, A. Improving detection of patient deterioration in the general hospital ward environment. Eur. J. Anaesthesiol. 2018, 35, 325–333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khanna, A.K. Defending a mean arterial pressure in the intensive care unit: Are we there yet? Ann. Intensiv. Care 2018, 8, 116. [Google Scholar] [CrossRef] [PubMed]
- Futier, E.; Lefrant, J.-Y.; Guinot, P.-G.; Godet, T.; Lorne, E.; Cuvillon, P.; Bertran, S.; Leone, M.; Pastene, B.; Piriou, V.; et al. Effect of Individualized vs Standard Blood Pressure Management Strategies on Postoperative Organ Dysfunction Among High-Risk Patients Undergoing Major Surgery. JAMA 2017, 318, 1346–1357. [Google Scholar] [CrossRef] [PubMed]
- Leone, M.; Asfar, P.; Radermacher, P.; Vincent, J.-L.; Martin, C. Optimizing mean arterial pressure in septic shock: A critical reappraisal of the literature. Crit. Care 2015, 19, 101. [Google Scholar] [CrossRef] [Green Version]
- Jozwiak, M.; Chambaz, M.; Sentenac, P.; Monnet, X.; Teboul, J.-L. Assessment of tissue oxygenation to personalize mean arterial pressure target in patients with septic shock. Microvasc. Res. 2020, 132, 104068. [Google Scholar] [CrossRef] [PubMed]
- Hernández, G.; Teboul, J.-L. Is the macrocirculation really dissociated from the microcirculation in septic shock? Intensiv. Care Med. 2016, 42, 1621–1624. [Google Scholar] [CrossRef]
- Pearse, R.M.; Moreno, R.P.; Bauer, P.; Pelosi, P.; Metnitz, P.; Spies, C.; Vallet, B.; Vincent, J.-L.; Hoeft, A.; Rhodes, A. Mortality after surgery in Europe: A 7 day cohort study. Lancet 2012, 380, 1059–1065. [Google Scholar] [CrossRef] [Green Version]
- Michard, F.; Bellomo, R.; Taenzer, A. The rise of ward monitoring: Opportunities and challenges for critical care specialists. Intensiv. Care Med. 2018, 45, 671–673. [Google Scholar] [CrossRef] [PubMed]
- Henderson, W.R.; Griesdale, D.E.; Walley, K.R.; Sheel, A.W.W. Clinical review: Guyton-the role of mean circulatory filling pressure and right atrial pressure in controlling cardiac output. Crit. Care 2010, 14, 243–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beard, D.A. Assessing the Validity and Utility of the Guyton Model of Arterial Blood Pressure Control. Hypertension 2018, 72, 1272–1273. [Google Scholar] [CrossRef]
- Solà, J.; Delgado-Gonzalo, R. Handbook of Cuffless Blood Pressure Monitoring; Springer: Cham, Switzerland, 2019. [Google Scholar]
- Armentano, R.L.; Cabrera Fischer, E.I.; Cymberknop, L.J. Biomechanical Modeling of the Cardiovascular System; Iop Publishing Ltd.: Philadelphia, PA, USA, 2019; ISBN 978-0750312820. [Google Scholar]
- Seagar, A.D.; Gibbs, J.M.; Davis, F.M. Interpretation of venous occlusion plethysmographic measurements using a simple model. Med. Biol. Eng. Comput. 1984, 22, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Michael, R. Pinsky, Functional Hemodynamic Monitoring. Crit. Care Clin. 2015, 31, 89–111. [Google Scholar] [CrossRef] [Green Version]
- Monnet, X.; Marik, P.; Teboul, J.-L. Passive leg raising for predicting fluid responsiveness: A systematic review and meta-analysis. Intensiv. Care Med. 2016, 42, 1935–1947. [Google Scholar] [CrossRef] [PubMed]
- Teboul, J.-L.; Monnet, X.; Chemla, D.; Michard, F. Arterial Pulse Pressure Variation with Mechanical Ventilation. Am. J. Respir. Crit. Care Med. 2019, 199, 22–31. [Google Scholar] [CrossRef]
- Michard, F.; Teboul, J.-L. Using heart-lung interactions to assess fluid responsiveness during mechanical ventilation. Crit. Care 2000, 4, 282–289. [Google Scholar] [CrossRef] [Green Version]
- Kuvin, J.T.; Karas, R.H. Clinical Utility of Endothelial Function Testing. Circulation 2003, 107, 3243–3247. [Google Scholar] [CrossRef]
- Rosenberry, R.; Nelson, M.D. Reactive hyperemia: A review of methods, mechanisms, and considerations. Am. J. Physiol. Integr. Comp. Physiol. 2020, 318, R605–R618. [Google Scholar] [CrossRef]
- Mayeur, C.; Campard, S.; Richard, C.; Teboul, J.-L. Comparison of four different vascular occlusion tests for assessing reactive hyperemia using near-infrared spectroscopy. Crit. Care Med. 2011, 39, 695–701. [Google Scholar] [CrossRef] [PubMed]
- Aya, H.D.; Rhodes, A.; Fletcher, N.; Grounds, R.M.; Cecconi, M. Transient stop-flow arm arterial–venous equilibrium pressure measurement: Determination of precision of the technique. J. Clin. Monit. Comput. 2015, 30, 55–61. [Google Scholar] [CrossRef] [PubMed]
- García, M.I.M.; Gil Cano, A.; Monrové, J.C.D. Arterial pressure changes during the Valsalva maneuver to predict fluid responsiveness in spontaneously breathing patients. Intensiv. Care Med. 2008, 35, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Orbegozo, D.; Mongkolpun, W.; Stringari, G.; Markou, N.; Creteur, J.; Vincent, J.-L.; De Backer, D. Skin microcirculatory reactivity assessed using a thermal challenge is decreased in patients with circulatory shock and associated with outcome. Ann. Intensiv. Care 2018, 8, 60. [Google Scholar] [CrossRef] [Green Version]
- Michard, F.; Chemla, D.; Teboul, J.-L. Applicability of pulse pressure variation: How many shades of grey? Crit. Care 2015, 19, 144. [Google Scholar] [CrossRef] [Green Version]
- Jun, J.-H.; Chung, R.K.; Baik, H.J.; Chung, M.H.; Hyeon, J.-S.; Lee, Y.-G.; Park, S.-H. The tidal volume challenge improves the reliability of dynamic preload indices during robot-assisted laparoscopic surgery in the Trendelenburg position with lung-protective ventilation. BMC Anesthesiol. 2019, 19, 142. [Google Scholar] [CrossRef] [Green Version]
- Monnet, X.; Saugel, B. Could resuscitation be based on microcirculation data? We are not sure. Intensiv. Care Med. 2018, 44, 950–953. [Google Scholar] [CrossRef] [Green Version]
- Cecconi, M.; De Backer, D.; Antonelli, M.; Beale, R.; Bakker, J.; Hofer, C.; Jaeschke, R.; Mebazaa, A.; Pinsky, M.R.; Teboul, J.L.; et al. Consensus on circulatory shock and hemodynamic monitoring. Task force of the European Society of Intensive Care Medicine. Intensiv. Care Med. 2014, 40, 1795–1815. [Google Scholar] [CrossRef] [Green Version]
- Dubin, A.; Henriquez, E.; Hernández, G. Monitoring peripheral perfusion and microcirculation. Curr. Opin. Crit. Care 2018, 24, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Ince, C. The microcirculation is the motor of sepsis. Crit. Care 2005, 9, S13–S19. [Google Scholar] [CrossRef] [Green Version]
- Mesquida, J.; Gruartmoner, G.; Espinal, C. Skeletal Muscle Oxygen Saturation (StO2) Measured by Near-Infrared Spectroscopy in the Critically Ill Patients. BioMed Res. Int. 2013, 2013, 502194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McNulty, J.; Born, M.; Pozos, R.S. Near-Infrared Spectroscopy (NIRS). In Springer Handbook of Medical Technology. Springer Handbooks; Kramme, R., Hoffmann, K.P., Pozos, R.S., Eds.; Springer: Berlin/Heidelberg, Germany, 2011. [Google Scholar] [CrossRef]
- Martin, D.S.; Levett, D.Z.; Bezemer, R.; Montgomery, H.E.; Grocott, M.P.; Caudwell Xtreme Everest Research Group. The Use of Skeletal Muscle Near Infrared Spectroscopy and a Vascular Occlusion Test at High Altitude. High Alt. Med. Biol. 2013, 14, 256–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vos, J.J.; Ellermann, S.F.; Scheeren, T.W.L. Journal of Clinical Monitoring and Computing 2017/2018 end of year summary: Monitoring—And provocation—Of the microcirculation and tissue oxygenation. J. Clin. Monit. Comput. 2019, 33, 201–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edul, V.S.K.; Ince, C.; Navarro, N.; Previgliano, L.; Risso-Vazquez, A.; Rubatto, P.N.; Dubin, A. Dissociation between sublingual and gut microcirculation in the response to a fluid challenge in postoperative patients with abdominal sepsis. Ann. Intensiv. Care 2014, 4, 39. [Google Scholar] [CrossRef] [Green Version]
- Knotzer, H.; Hasibeder, W.R. Microcirculatory function monitoring at the bedside—A view from the intensive care. Physiol. Meas. 2007, 28, R65–R86. [Google Scholar] [CrossRef]
- Bartels, S.A.; Bezemer, R.; Milstein, D.M.; Radder, M.; Lima, A.; Cherpanath, T.G.; Heger, M.; Karemaker, J.M.; Ince, C. The microcirculatory response to compensated hypovolemia in a lower body negative pressure model. Microvasc. Res. 2011, 82, 374–380. [Google Scholar] [CrossRef]
- Bezemer, R.; Karemaker, J.M.; Klijn, E.; Martin, D.; Mitchell, K.; Grocott, M.; Heger, M.; Ince, C. Simultaneous multi-depth assessment of tissue oxygen saturation in thenar and forearm using near-infrared spectroscopy during a simple cardiovascular challenge. Crit. Care 2009, 13, S5. [Google Scholar] [CrossRef] [Green Version]
- Lima, A.; Bakker, J. Noninvasive monitoring of peripheral perfusion. Intensiv. Care Med. 2005, 31, 1316–1326. [Google Scholar] [CrossRef]
- Sun, S.; Hayes-Gill, B.R.; He, D.; Zhu, Y.; Huynh, N.T.; Morgan, S.P. Comparison of laser Doppler and laser speckle contrast imaging using a concurrent processing system. Opt. Lasers Eng. 2016, 83, 1–9. [Google Scholar] [CrossRef]
- Alnawaiseh, M.; Ertmer, C.; Seidel, L.; Arnemann, P.H.; Lahme, L.; Kampmeier, T.-G.; Rehberg, S.W.; Heiduschka, P.; Eter, N.; Hessler, M. Feasibility of optical coherence tomography angiography to assess changes in retinal microcirculation in ovine haemorrhagic shock. Crit. Care 2018, 22, 138. [Google Scholar] [CrossRef] [Green Version]
- Guerraty, M.; Bhargava, A.; Senarathna, J.; Mendelson, A.A.; Pathak, A.P. Advances in translational imaging of the microcirculation. Microcirculation 2021, 28, e12683. [Google Scholar] [CrossRef] [PubMed]
- Harrois, A.; Duranteau, J. Contrast-enhanced ultrasound: A new vision of microcirculation in the intensive care unit. Crit. Care 2013, 17, 449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steinberg, I.; Huland, D.M.; Vermesh, O.; Frostig, H.E.; Tummers, W.S.; Gambhir, S.S. Photoacoustic clinical imaging. Photoacoustics 2019, 14, 77–98. [Google Scholar] [CrossRef]
- Wang, C.; Li, X.; Hu, H.; Zhang, L.; Huang, Z.; Lin, M.; Zhang, Z.; Yin, Z.; Huang, B.; Gong, H.; et al. Monitoring of the central blood pressure waveform via a conformal ultrasonic device. Nat. Biomed. Eng. 2018, 2, 687–695. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.; Epstein, F.H.; Kramer, C.M. Evaluation of the microcirculation: Advances in cardiac magnetic resonance perfusion imaging. J. Nucl. Cardiol. 2008, 15, 698–708. [Google Scholar] [CrossRef] [Green Version]
- Wilkins, E.; Wilson, L.; Wickramasinghe, K.; Bhatnagar, P.; Leal, J.; Luengo-Fernandez, R.; Burns, R.; Rayner, M.; Townsend, N. European Cardiovascular Disease Statistics 2017. European Heart Network. 2017. Available online: http://www.ehnheart.org/images/CVD-statistics-report-August-2017.pdf (accessed on 3 May 2019).
- Armentano, R.L.; Legnani, W.; Cymberknop, L.J.; Brambila, F. Fractal Analysis of Cardiovascular Signals Empowering the Bioengineering Knowledge; IntechOpen: London, UK, 2017; ISBN 978-953-51-3214-1. [Google Scholar]
- Hermeling, E.; Hoeks, A.P.; Winkens, M.H.; Waltenberger, J.L.; Reneman, R.S.; Kroon, A.A.; Reesink, K.D. Noninvasive Assessment of Arterial Stiffness Should Discriminate Between Systolic and Diastolic Pressure Ranges. Hypertension 2010, 55, 124–130. [Google Scholar] [CrossRef] [Green Version]
- Nottin, S.; Walther, G.; Vinet, A.; Dauzat, M.; Beck, L.; Messner-Pellenc, P.; Obert, P. Reproducibility of automated pulse wave velocity measurement during exercise. Running head: Pulse wave velocity during exercise. Arch. Mal. Coeur Vaiss. 2006, 99, 564–568. [Google Scholar]
- Argyris, A.A.; Nasothimiou, E.; Aissopou, E.; Papaioannou, T.G.; Zhang, Y.; Blacher, J.; Safar, M.E.; Sfikakis, P.P.; Protogerou, A.D. Mechanisms of pulse pressure amplification dipping pattern during sleep time: The SAFAR study. J. Am. Soc. Hypertens. 2018, 12, 117–127. [Google Scholar] [CrossRef]
- Zong, W.; Moody, G.B.; Mark, R.G. Effects of vasoactive drugs on the relationship between ECG-pulse wave delay time and arterial blood pressure in ICU patients. In Proceedings of the Computers in Cardiology 1998. Vol. 25 (Cat. No.98CH36292), Cleveland, OH, USA, 13–16 September 1998; IEEE: Piscataway, NJ, USA, 1998; pp. 673–676. [Google Scholar] [CrossRef]
- Bank, A.J.; Wilson, R.F.; Kubo, S.H.; Holte, J.E.; Dresing, T.J.; Wang, H. Direct Effects of Smooth Muscle Relaxation and Contraction on In Vivo Human Brachial Artery Elastic Properties. Circ. Res. 1995, 77, 1008–1016. [Google Scholar] [CrossRef]
- Lin, A.C.; Lowe, A.; Sidhu, K.; Harrison, W.; Ruygrok, P.; Stewart, R. Evaluation of a novel sphygmomanometer, which estimates central aortic blood pressure from analysis of brachial artery suprasystolic pressure waves. J. Hypertens. 2012, 30, 1743–1750. [Google Scholar] [CrossRef] [Green Version]
- Reymond, P.; Merenda, F.; Perren, F.; Rüfenacht, D.; Stergiopulos, N. Validation of a one-dimensional model of the systemic arterial tree. Am. J. Physiol. Circ. Physiol. 2009, 297, H208–H222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Block, R.C.; Yavarimanesh, M.; Natarajan, K.; Carek, A.; Mousavi, A.; Chandrasekhar, A.; Kim, C.-S.; Zhu, J.; Schifitto, G.; Mestha, L.K.; et al. Conventional pulse transit times as markers of blood pressure changes in humans. Sci. Rep. 2020, 10, 16373. [Google Scholar] [CrossRef] [PubMed]
- Jadooei, A.; Zaderykhin, O.; Shulgin, V.I. Adaptive algorithm for continuous monitoring of blood pressure using a pulse transit time. In Proceedings of the 2013 IEEE XXXIII International Scientific Conference Electronics and Nanotechnology (ELNANO), Kiev, Ukraine, 16–19 April 2013; pp. 297–301. [Google Scholar]
- Cattivelli, F.S.; Garudadri, H. Noninvasive cuffless estimation of blood pressure from pulse arrival time and heart rate with adaptive calibration. In Proceedings of the 2009 Sixth International Workshop on Wearable and Implantable Body Sensor Networks, Berkeley, CA, USA, 3–5 June 2009; pp. 114–119. [Google Scholar] [CrossRef]
- Chandrasekhar, A.; Yavarimanesh, M.; Natarajan, K.; Hahn, J.-O.; Mukkamala, R. PPG Sensor Contact Pressure Should Be Taken Into Account for Cuff-Less Blood Pressure Measurement. IEEE Trans. Biomed. Eng. 2020, 67, 3134–3140. [Google Scholar] [CrossRef] [PubMed]
- Sola, J.; Vybornova, A.; Fallet, S.; Olivero, E.; De Marco, B.; Grossenbacher, O.; Ignjatovic, N.; Favre-Bulle, M.; Levinson, N.; Siutryk, N.; et al. Are cuffless devices challenged enough? Design of a validation protocol for ambulatory blood pressure monitors at the wrist: The case of the Aktiia Bracelet. In Proceedings of the 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2020; pp. 4437–4440. [Google Scholar] [CrossRef]
- Jilek, J.; Stork, M. Cuff width alters the amplitude envelope of wrist cuff pressure pulse waveforms. Physiol. Meas. 2010, 31, N43–N49. [Google Scholar] [CrossRef]
- Spitz, R.W.; Bell, Z.W.; Wong, V.; Viana, R.B.; Chatakondi, R.N.; Abe, T.; Loenneke, J.P. The position of the cuff bladder has a large impact on the pressure needed for blood flow restriction. Physiol. Meas. 2019, 41, 01NT01. [Google Scholar] [CrossRef]
- Otsuka, T.; Munakata, R.; Kato, K.; Kodani, E.; Ibuki, C.; Kusama, Y.; Seino, Y.; Kawada, T. Oscillometric measurement of brachial artery cross-sectional area and its relationship with cardiovascular risk factors and arterial stiffness in a middle-aged male population. Hypertens. Res. 2013, 36, 910–915. [Google Scholar] [CrossRef]
- Wassertheurer, S.; Kropf, J.; Weber, T.; Van Der Giet, M.; Baulmann, J.; Ammer, M.; Hametner, B.; Mayer, C.C.; Eber, B.; Magometschnigg, D. A new oscillometric method for pulse wave analysis: Comparison with a common tonometric method. J. Hum. Hypertens. 2010, 24, 498–504. [Google Scholar] [CrossRef]
- Beutel, F.; Van Hoof, C.; Rottenberg, X.; Reesink, K.; Hermeling, E. Pulse Arrival Time Segmentation Into Cardiac and Vascular Intervals–Implications for Pulse Wave Velocity and Blood Pressure Estimation. IEEE Trans. Biomed. Eng. 2021, 68, 2810–2820. [Google Scholar] [CrossRef]
- Wang, G.; Atef, M.; Lian, Y. Towards a Continuous Non-Invasive Cuffless Blood Pressure Monitoring System Using PPG: Systems and Circuits Review. IEEE Circuits Syst. Mag. 2018, 18, 6–26. [Google Scholar] [CrossRef]
- Pulse Wave Analysis & Arterial Stiffness. Aortic Pulse Wave Velocity (PWVao). Available online: https://www.tensiomed.com/parameters/aortic-pulse-wave-velocity-pwvao/ (accessed on 10 March 2022).
- Salvi, P.; Scalise, F.; Rovina, M.; Moretti, F.; Salvi, L.; Grillo, A.; Gao, L.; Baldi, C.; Faini, A.; Furlanis, G.; et al. Noninvasive Estimation of Aortic Stiffness Through Different Approaches. Hypertension 2019, 74, 117–129. [Google Scholar] [CrossRef] [Green Version]
- Bogatu, L.I.; Turco, S.; Mischi, M.; Woerlee, P.; Bouwman, A.; Korsten, E.H.; Muehlsteff, J. A modelling framework for assessment of arterial compliance by fusion of oscillometry and pulse wave velocity information. Comput. Methods Programs Biomed. 2020, 196, 105492. [Google Scholar] [CrossRef]
- Bresch, E.; Muehlsteff, J.; Schmitt, L. Cuff-induced changes of pulse arrival time: Models and experimental results. In EMBEC & NBC 2017 IFMBE Proceedings; Springer: Singapore, 2018; Volume 65. [Google Scholar]
- Yan, Y.S.; Zhang, Y.T. A model-based calibration method for noninvasive and cuffless measurement of arterial blood pressure. In Proceedings of the 2006 IEEE Biomedical Circuits and Systems Conference, London, UK, 29 November–1 December 2006; pp. 234–236. [Google Scholar] [CrossRef]
- Bank, A.J.; Kaiser, D.R.; Rajala, S.; Cheng, A. In Vivo Human Brachial Artery Elastic Mechanics. Circulation 1999, 100, 41–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butlin, M.; Qasem, A. Large Artery Stiffness Assessment Using SphygmoCor Technology. Pulse 2016, 4, 180–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holz, C.; Wang, E. Glabella: Continuously Sensing Blood Pressure Behavior using an Unobtrusive Wearable Device. In Proceedings of the ACM on Interactive, Mobile, Wearable and Ubiquitous Technologies; Article 58; Association for Computing Machinery: New York, NY, USA, 2017; Volume 1, pp. 1–23. [Google Scholar]
- Reiter, H.; Muehlsteff, J.; Sipilä, A. Medical application and clinical validation for reliable and trustworthy physiological monitoring using functional textiles: Experience from the HeartCycle and MyHeart project. In Proceedings of the 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011; pp. 3270–3273. [Google Scholar] [CrossRef]
- Carek, A.M.; Jung, H.; Inan, O.T. A Reflective Photoplethysmogram Array and Channel Selection Algorithm for Weighing Scale Based Blood Pressure Measurement. IEEE Sensors J. 2019, 20, 3849–3858. [Google Scholar] [CrossRef]
- Chan, C.; Zhang, Y. Continuous and long-term arterial blood pressure monitoring by using h-Shirt. In Proceedings of the 2008 International Conference on Information Technology and Applications in Biomedicine, Shenzhen, China, 30–31 May 2008; pp. 267–269. [Google Scholar] [CrossRef]
- Visvanathan, A.; Sinha, A.; Pal, A. Estimation of blood pressure levels from reflective Photoplethysmograph using smart phones. In Proceedings of the 13th IEEE International Conference on BioInformatics and BioEngineering, Chania, Greece, 10–13 November 2013; pp. 1–5. [Google Scholar] [CrossRef]
- Solà, J.; Adler, A.; Santos, A.; Tusman, G.; Suarez-Sipmann, F.; Bohm, S.H. Non-invasive monitoring of central blood pressure by electrical impedance tomography: First experimental evidence. Med. Biol. Eng. Comput. 2011, 49, 409–415. [Google Scholar] [CrossRef] [Green Version]
- Wei, J.; Luo, H.; Wu, S.J.; Zheng, P.P.; Fu, G.; Lee, K. Transdermal Optical Imaging Reveal Basal Stress via Heart Rate Variability Analysis: A Novel Methodology Comparable to Electrocardiography. Front. Psychol. 2018, 9, 98. [Google Scholar] [CrossRef] [Green Version]
- Bogatu, L.I.; Turco, S.; Mischi, M.; Muehlsteff, J.; Woerlee, P. An Experimental Study on the Blood Pressure Cuff as a Transducer for Oscillometric Blood Pressure Measurements. IEEE Trans. Instrum. Meas. 2021, 70, 9501611. [Google Scholar] [CrossRef]
- Zhang, G.; Gao, M.; Xu, D.; Olivier, N.B.; Mukkamala, R. Pulse arrival time is not an adequate surrogate for pulse transit time as a marker of blood pressure. J. Appl. Physiol. 2011, 111, 1681–1686, Erratum in J. Appl. Physiol. 2014, 117, 1212. [Google Scholar] [CrossRef] [Green Version]
- Mukkamala, R.; Hahn, J.O.; Inan, O.T.; Mestha, L.K.; Kim, C.S.; Töreyin, H.; Kyal, S. Toward Ubiquitous Blood Pressure Monitoring via Pulse Transit Time: Theory and Practice. IEEE Trans Biomed Eng. 2015, 62, 1879–1901. [Google Scholar] [CrossRef] [Green Version]
- Balmer, J.C.; Pretty, C.G.; Davidson, S.; Desaive, T.; Kamoi, S.; Pironet, A.; Morimont, P.; Janssen, N.; Lambermont, B.; Shaw, G.M.; et al. Pre-ejection period, the reason why the electrocardiogram Q-wave is an unreliable indicator of pulse wave initialization. Physiol. Meas. 2018, 39, 095005. [Google Scholar] [CrossRef]
- Teng, X.-F.; Zhang, Y.-T. Theoretical Study on the Effect of Sensor Contact Force on Pulse Transit Time. IEEE Trans. Biomed. Eng. 2007, 54, 1490–1498. [Google Scholar] [CrossRef] [PubMed]
- Zulliger, M.A.; Kwak, N.T.M.R.; Tsapikouni, T.; Nikos Stergiopulos, N. Effects of longitudinal stretch on VSM tone and distensibility of muscular conduit arteries. Am. J. Physiol. -Heart Circ. Physiol. 2002, 283, H2599–H2605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bogatu, L.; Bresch, E.; Muehlsteff, J.; Smink, J.; Woerlee, P. Insights into oscillometry: An Experimental Study for Improvement of Cuff-Based Blood Pressure Measurement Technology. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019. [Google Scholar] [CrossRef]
- Bogatu, L.I.; Turco, S.; Mischi, M.; Schmitt, L.; Woerlee, P.; Bresch, E.; Noordergraaf, G.J.; Paulussen, I.; Bouwman, A.; Korsten, H.H.; et al. Modulation of pulse propagation and blood flow via cuff inflation—New distal insights. Sensor 2021, 21, 5593. [Google Scholar] [CrossRef] [PubMed]
- Selvaraj, N.; Jaryal, A.K.; Santhosh, J.; Anand, S.; Deepak, K.K. Monitoring of reactive hyperemia using photoplethysmographic pulse amplitude and transit time. J. Clin. Monit. Comput. 2009, 23, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Babbs, C.F. Oscillometric measurement of systolic and diastolic blood pressures validated in a physiologic mathematical model. Biomed. Eng. Online 2012, 11, 56. [Google Scholar] [CrossRef] [Green Version]
- Drzewiecki, G.; Pilla, J.J. Noninvasive measurement of the human brachial artery pressure-area relation in collapse and hypertension. Ann. Biomed. Eng. 1998, 26, 965–974. [Google Scholar] [CrossRef]
- Drzewiecki, G.; Hood, R.; Apple, H. Theory of the oscillometric maximum and the systolic and diastolic detection ratios. Ann. Biomed. Eng. 1994, 22, 88–96. [Google Scholar] [CrossRef]
- Cymberknop, L.J.; Castillo, F.G.; Armentano, R.L. Beat to Beat Modulation of Arterial Pulse Wave Velocity Induced by Vascular Smooth Muscle Tone. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 5030–5033. [Google Scholar] [CrossRef]
- Salvucci, F.P.; Schiavone, J.; Craiem, D.; Barra, J.G. Arterial wall mechanics as a function of heart rate: Role of vascular smooth muscle. J. Phys. Conf. Ser. 2007, 90, 012010. [Google Scholar] [CrossRef]
- Roca, F.; Iacob, M.; Remy-Jouet, I.; Bellien, J.; Joannides, R. Evidence for a Role of Vascular Endothelium in the Control of Arterial Wall Viscosity in Humans. Hypertension 2018, 71, 143–150. [Google Scholar] [CrossRef]
- Wurzel, M.; Cowper, G.R.; McCook, J.M. Smooth muscle contraction and viscoelasticity of arterial wall. Can. J. Physiol. Pharmacol. 1970, 48, 510–523. [Google Scholar] [CrossRef]
- van Knippenberg, L.; van Sloun, R.J.G.; Shulepov, S.; Bouwman, R.A.; Mischi, M. An Angle-Independent Cross-Sectional Doppler Method for Flow Estimation in the Common Carotid Artery. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2020, 67, 1513–1524. [Google Scholar] [CrossRef]
- Brattain, L.J.; Telfer, B.A.; Dhyani, M.; Grajo, J.R.; Samir, A.E. Machine learning for medical ultrasound: Status, methods, and future opportunities. Abdom. Imaging 2018, 43, 786–799. [Google Scholar] [CrossRef]
- Ottesen, J.T.; Olufsen, M.S.; Larsen, J.K. Applied Mathematical Models in Human Physiology; Society for Industrial & Applied Mathematics: Philadephia, PA, USA,, 2004. [Google Scholar] [CrossRef] [Green Version]
- Conrad, L.I.; Neve, M.; Nutton, V.; Porter, R.; Wear, A. The Western Medical Tradition: 800 BC to AD 1800; Cambridge University Press: Cambridge, UK, 1995; p. 68. ISBN 0521475643/9780521475648. [Google Scholar]
- Hatib, F.; Jian, Z.; Buddi, S.; Lee, C.; Settels, J.; Sibert, K.; Rinehart, J.; Cannesson, M. Machine-learning Algorithm to Predict Hypotension Based on High-fidelity Arterial Pressure Waveform Analysis. Anesthesiology 2018, 129, 663–674. [Google Scholar] [CrossRef] [PubMed]
- Landry, C.; Hedge, E.T.; Hughson, R.L.; Peterson, S.D.; Arami, A. Cuffless Blood Pressure Estimation for Activities of Daily Living. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2020, 2020, 4441–4445. [Google Scholar] [CrossRef]
- El-Hajj, C.; Kyriacou, P. A review of machine learning techniques in photoplethysmography for the non-invasive cuff-less measurement of blood pressure. Biomed. Signal Process. Control 2020, 58, 101870. [Google Scholar] [CrossRef]
- Shillan, D.; Sterne, J.A.C.; Champneys, A.; Gibbison, B. Use of machine learning to analyse routinely collected intensive care unit data: A systematic review. Crit. Care 2019, 23, 284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moss, T.; Lake, D.E.; Calland, J.F.; Enfield, K.B.; Delos, J.B.; Fairchild, K.D.; Moorman, J.R. Signatures of Subacute Potentially Catastrophic Illness in the ICU. Crit. Care Med. 2016, 44, 1639–1648. [Google Scholar] [CrossRef] [Green Version]
- Sun, S.; Bezemer, R.; Long, X.; Muehlsteff, J.; Aarts, R.M. Systolic blood pressure estimation using PPG and ECG during physical exercise. Physiol. Meas. 2016, 37, 2154–2169. [Google Scholar] [CrossRef]
- Kendale, S.; Kulkarni, P.; Rosenberg, A.D.; Wang, J. Supervised Machine-learning Predictive Analytics for Prediction of Postinduction Hypotension. Anesthesiology 2018, 129, 675–688. [Google Scholar] [CrossRef]
- Scheeren, T.L.; Vos, J. Intraoperative hypotension and its prediction. Indian J. Anaesth. 2019, 63, 877–885. [Google Scholar] [CrossRef]
- Michard, F.; Teboul, J.L. Predictive analytics: Beyond the buzz. Ann. Intensiv. Care 2019, 9, 46. [Google Scholar] [CrossRef] [PubMed]
- Greenspan, H.; van Ginneken, B.; Summers, R.M. Guest Editorial Deep Learning in Medical Imaging: Overview and Future Promise of an Exciting New Technique. IEEE Trans. Med. Imaging 2016, 35, 1153–1159. [Google Scholar] [CrossRef]
- Zhu, B.; Liu, J.Z.; Cauley, S.F.; Rosen, B.R.; Rosen, M.S. Image reconstruction by domain-transform manifold learning. Nature 2018, 555, 487–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rudin, C. Stop explaining black box machine learning models for high stakes decisions and use interpretable models instead. Nat. Mach. Intell. 2019, 1, 206–215. [Google Scholar] [CrossRef] [Green Version]
- Wax, D.B.; Lin, H.-M.; Leibowitz, A.B. Invasive and Concomitant Noninvasive Intraoperative Blood Pressure Monitoring. Anesthesiology 2011, 115, 973–978. [Google Scholar] [CrossRef]
- Tomašev, N.; Glorot, X.; Rae, J.W.; Zielinski, M.; Askham, H.; Saraiva, A.; Mottram, A.; Meyer, C.; Ravuri, S.; Protsyuk, I.; et al. A clinically applicable approach to continuous prediction of future acute kidney injury. Nature 2019, 572, 116–119. [Google Scholar] [CrossRef]
- Asfar, P.; Meziani, F.; Hamel, J.-F.; Grelon, F.; Megarbane, B.; Anguel, N.; Mira, J.-P.; Dequin, P.-F.; Gergaud, S.; Weiss, N.; et al. High versus low blood-pressure target in patients with septic shock. N. Engl. J. Med. 2014, 370, 1583–1593. [Google Scholar] [CrossRef] [Green Version]
- Hall, P.; Gill, N. An Introduction to Machine Learning Interpretability, 2nd ed.; O’Reilly Media, Inc.: Sebastopol, CA, USA, 2019. [Google Scholar]
- Fong, R.C.; Vedaldi, A. Interpretable explanations of black boxes by meaningful perturbation. Proc. IEEE Int. Conf. Comput. Vis. 2017, 1, 3449–3457. [Google Scholar]
- Pals, R.A.S.; Hansen, U.M.; Johansen, C.B.; Hansen, C.S.; Jørgensen, M.E.; Fleischer, J.; Willaing, I. Making sense of a new technology in clinical practice: A qualitative study of patient and physician perspectives. BMC Health Serv. Res. 2015, 15, 402. [Google Scholar] [CrossRef] [Green Version]
- Ramsingh, D.; Alexander, B.; Cannesson, M. Clinical review: Does it matter which hemodynamic monitoring system is used? Crit. Care 2012, 17, 208–213. [Google Scholar] [CrossRef] [Green Version]
- Michard, F. Hemodynamic monitoring in the era of digital health. Ann. Intensiv. Care 2016, 6, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Device | Measurement Procedure |
|---|---|
| Arteriograph (TensioMed, Budapest, Hungary) [73] | A cuff placed at brachial site is pressurized suprasytolically, therefore removing effects stemming from vasculature under the cuff and distal from the cuff. Arterial pulsations occur at the upper edge of the cuff. The resulting cuff signal is processed to obtain information such as central pulse wave velocity, aortic pressure values, wave reflection characteristics. |
| Mobil-O-Graph (IEM Gmbm, Stolberg, Germany) [70] | A cuff placed at brachial site is used; the cuff pressure is recorded with the use of a high-fidelity pressure sensor. The inflation process includes several seconds where the cuff pressure is held at diastolic vale. The waveform is analyzed to estimate aortic pressure values, wave reflection characteristics. |
| Complior (ALAM, Vincennes, France) [74] | The method uses two non-invasive tonometric sensors to simultaneously record pulse waves in the carotid and femoral arteries to measure carotid-femoral pulse wave velocity for assessment of arterial stiffness. |
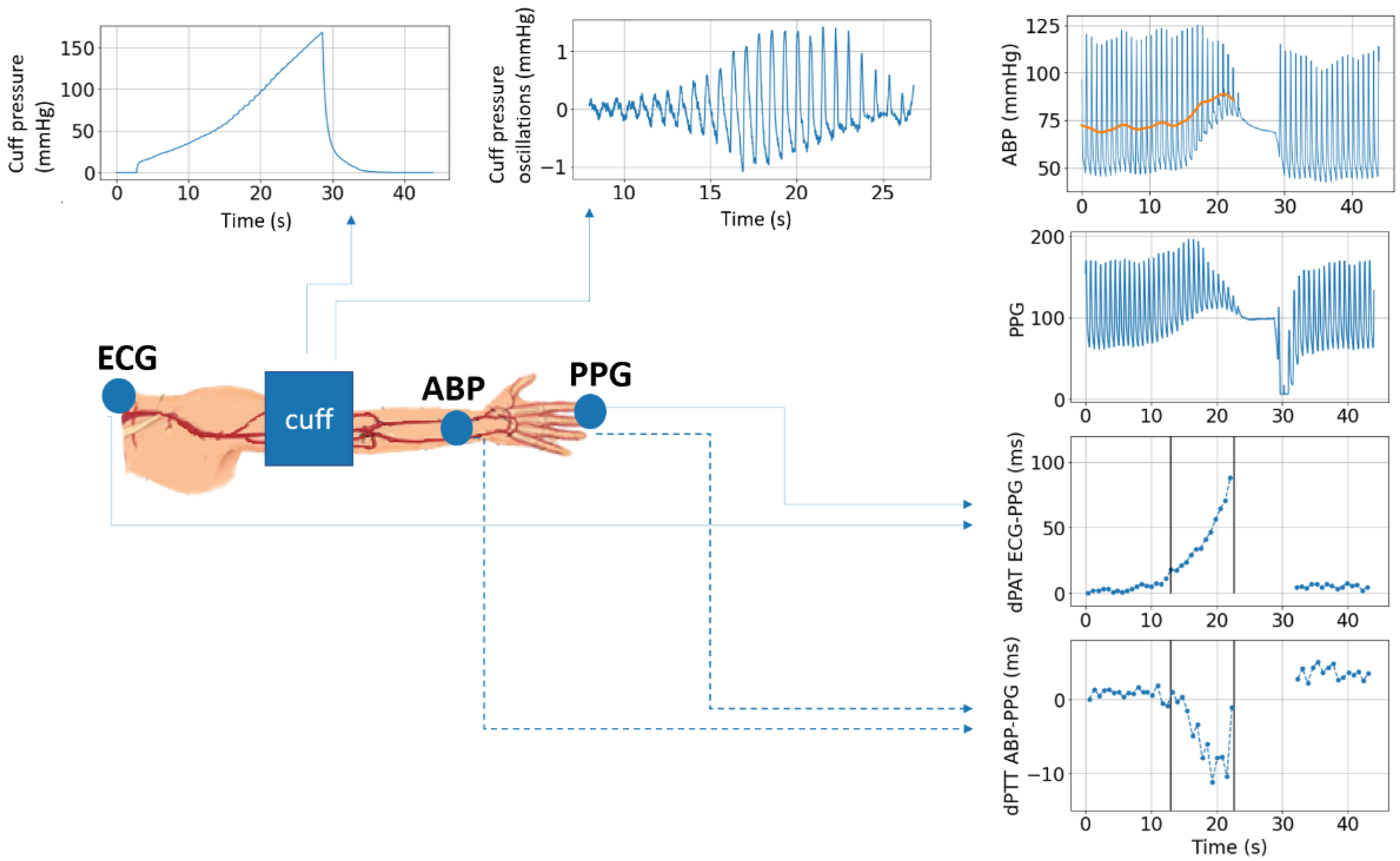
| PTT-BP calibration based on cuff modulation [75,76,77] | A cuff is used to alter transmural pressure across the brachial artery for the purpose of modulating PTT. The change in PTT with respect to the controlled transmural pressure is measured via ECG and PPG and analyzed in order to calibrate the BP-PAT relationship for the purpose of beat-to-beat PAT-based BP estimation and arterial stiffness estimation. |
| Chronos TM-2771 (A&D Company, Tokyo, Japan) [69] | Arterial diameter at brachial site is measured via a device consisting of four adjacent cuffs. The cuffs are designed of soft and hard materials such that the resulting cuff pressure oscillation reflects brachial artery volume oscillation as accurately as possible. |
| Water-filled cuff [78] | A water-filled blood pressure cuff is used to allow the brachial artery to be simultaneously imaged via ultrasound. The aim is to obtain an accurate measurement of brachial arterial volume during cuff-based occlusion. |
| SphygmoCor (AtCor Medical, Sydney, NSW, Australia) [79] | Brachial and femoral cuffs or, alternatively, applanation tonometry of the carotid and femoral sites are used together with specially developed algorithms to acquire central aortic pressure waveform and carotid-femoral arterial PWV for the purpose of estimating cardiovascular risk. |
| Aktiia SA (Aktiia SA, Neuchâtel, Switzerland) [66] | Optical sensors perform green reflective photoplethysmography (PPG) measurements on the skin vasculature of the wrist to measure BP. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bogatu, L.; Turco, S.; Mischi, M.; Schmitt, L.; Woerlee, P.; Bezemer, R.; Bouwman, A.R.; Korsten, E.H.H.M.; Muehlsteff, J. New Hemodynamic Parameters in Peri-Operative and Critical Care—Challenges in Translation. Sensors 2023, 23, 2226. https://0-doi-org.brum.beds.ac.uk/10.3390/s23042226
Bogatu L, Turco S, Mischi M, Schmitt L, Woerlee P, Bezemer R, Bouwman AR, Korsten EHHM, Muehlsteff J. New Hemodynamic Parameters in Peri-Operative and Critical Care—Challenges in Translation. Sensors. 2023; 23(4):2226. https://0-doi-org.brum.beds.ac.uk/10.3390/s23042226
Chicago/Turabian StyleBogatu, Laura, Simona Turco, Massimo Mischi, Lars Schmitt, Pierre Woerlee, Rick Bezemer, Arthur R. Bouwman, Erik H. H. M. Korsten, and Jens Muehlsteff. 2023. "New Hemodynamic Parameters in Peri-Operative and Critical Care—Challenges in Translation" Sensors 23, no. 4: 2226. https://0-doi-org.brum.beds.ac.uk/10.3390/s23042226