

A Study on the Effectiveness of Deep Learning-Based Anomaly Detection Methods for Breast Ultrasonography
 , ,
, ,
Abstract
:1. Introduction
2. Related Work
2.1. Deep Learning-Based Anomaly Detection
Unsupervised Deep Anomaly Detection
2.2. Deep Learning-Based Anomaly Detection for Medical Images
3. Materials & Methods
3.1. Materials
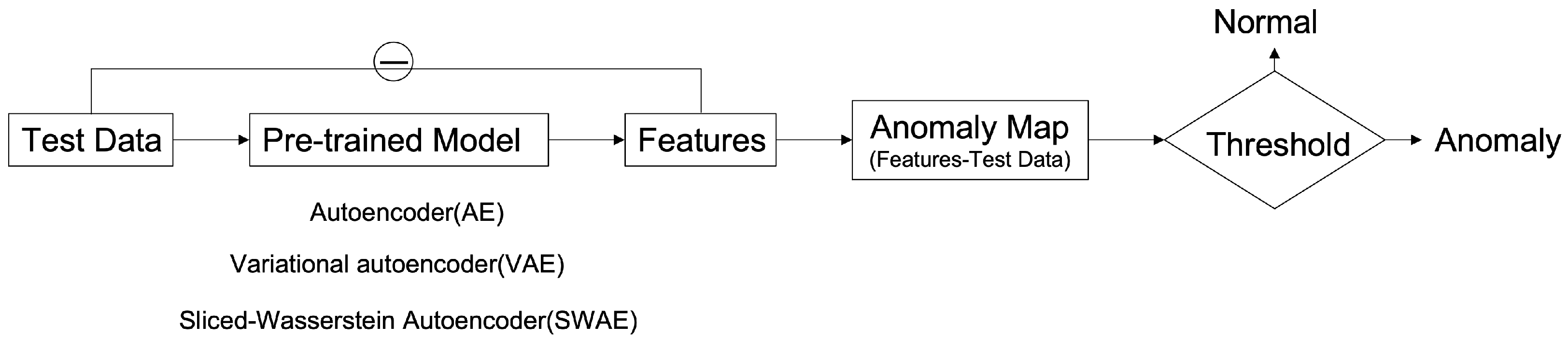
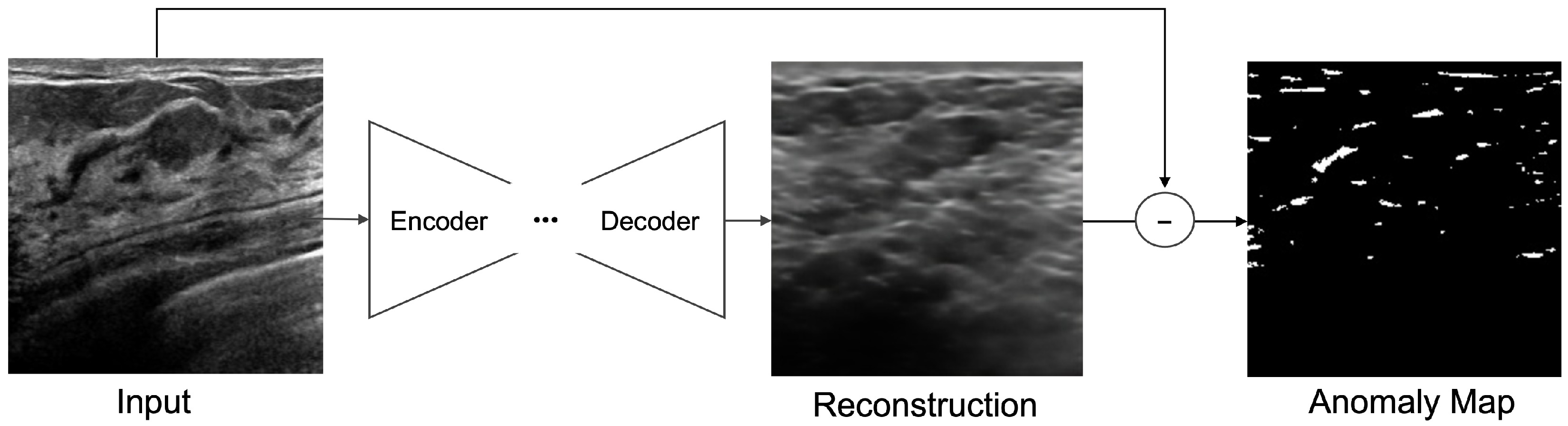
3.2. Reconstruction-Based Anomaly Detection
3.2.1. Hyperparameter Tuning
3.2.2. Model Architecture of Anomaly Detection Model for Breast Ultrasound
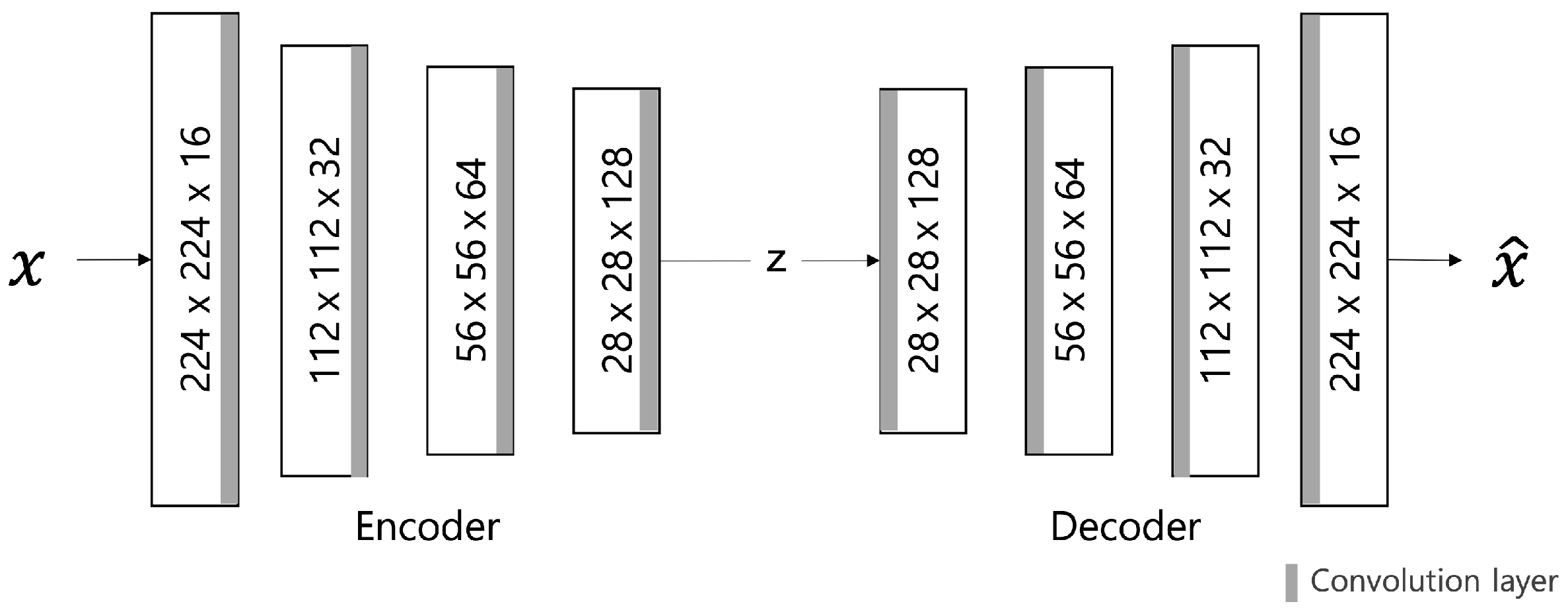
Autoencoder (AE) Model
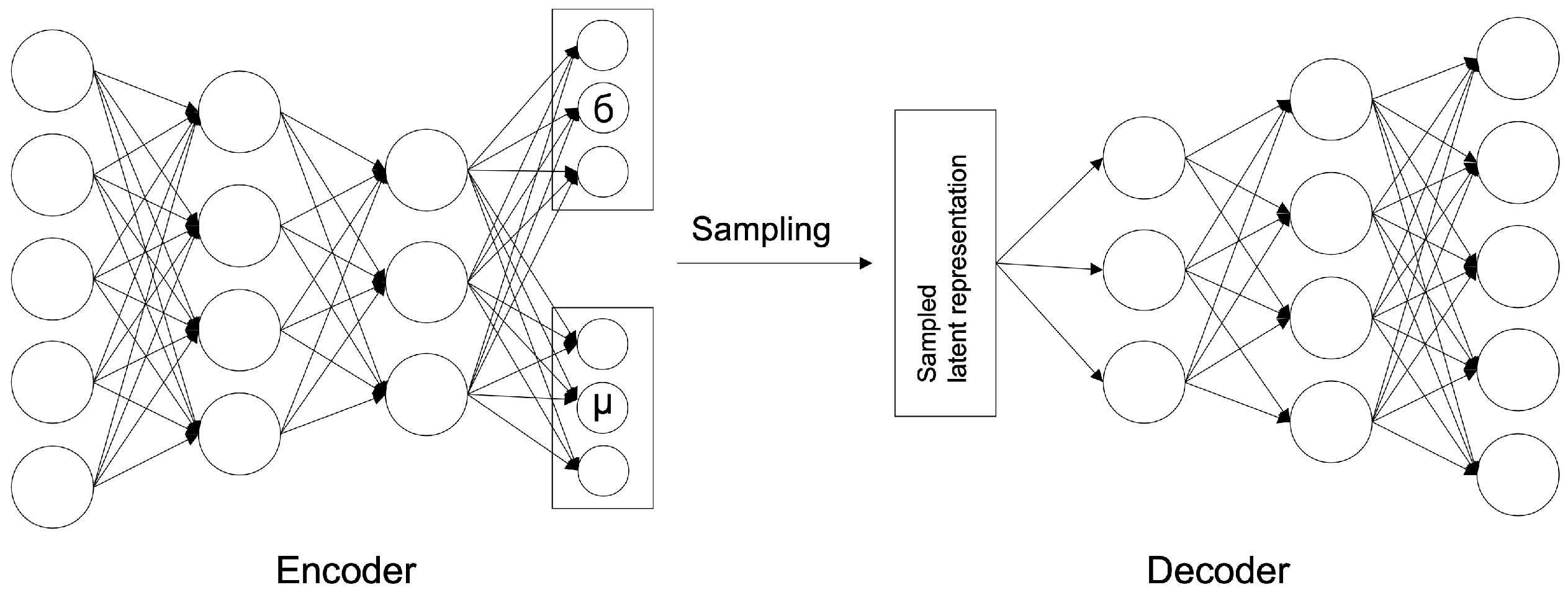
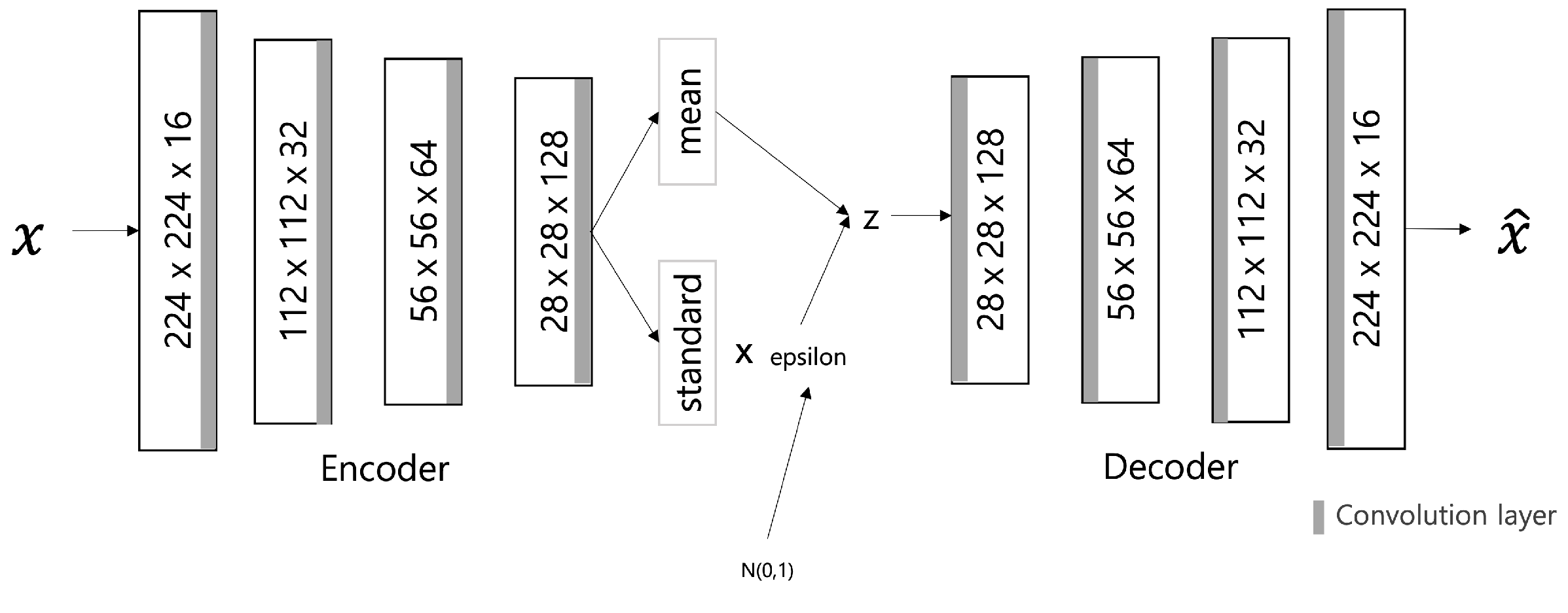
Variational Autoencoder (VAE) Model
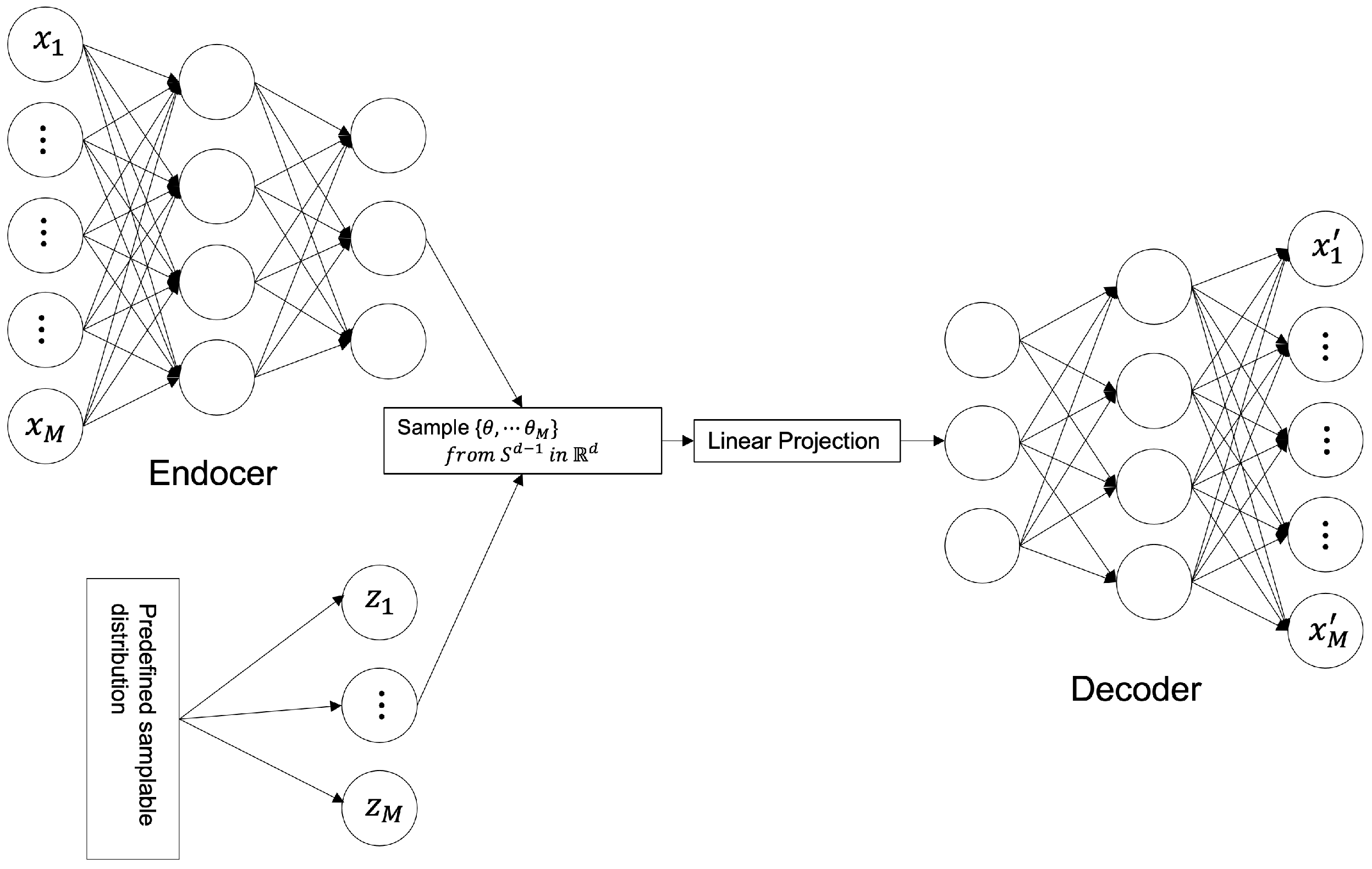
SWAE Model
3.2.3. Validation of Anomaly Detection Method for Breast Ultrasonography
Performance Evaluation of Anomaly Detection
Analysis of Factor Influencing Anomalous Region Detection
| Algorithm 1: Find threshold for anomaly detection |
Input: anomaly map of validation dataset Output: threshold
|
4. Experimental Results and Analysis
4.1. Experimental Overview and Environment
4.2. Evaluation of Anomalous Region Detection in Ultrasonography
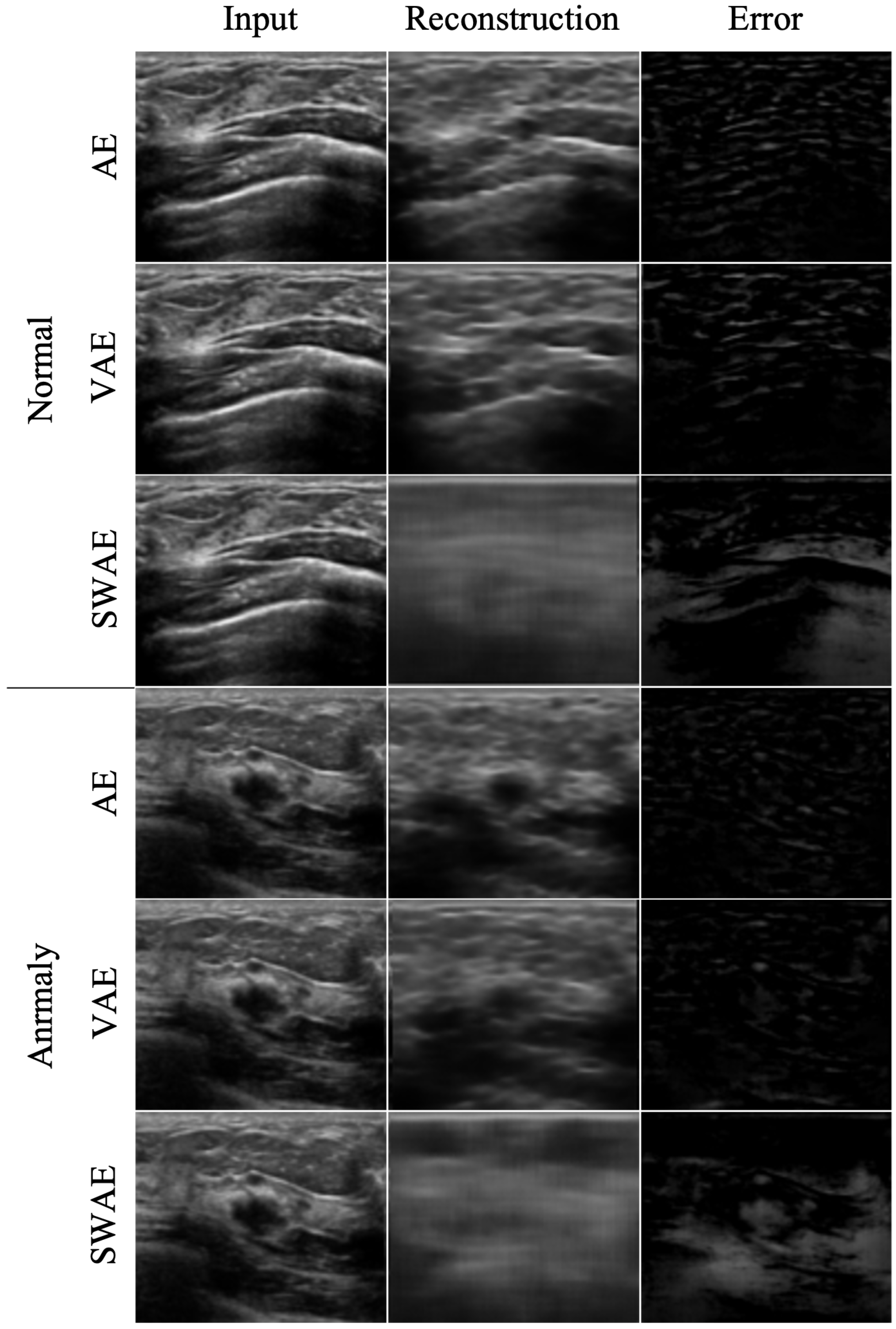
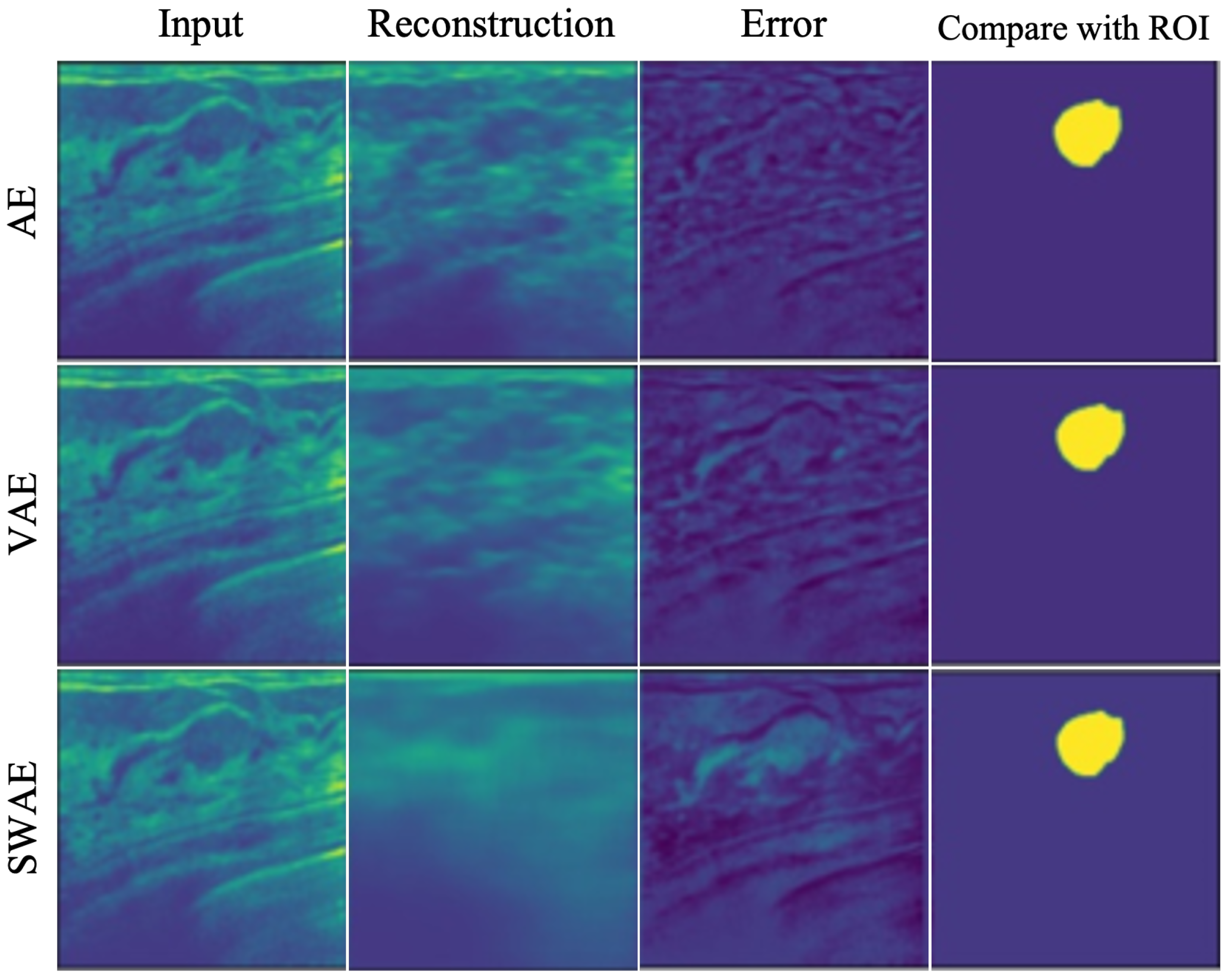
4.2.1. Reconstruction Performance by Model
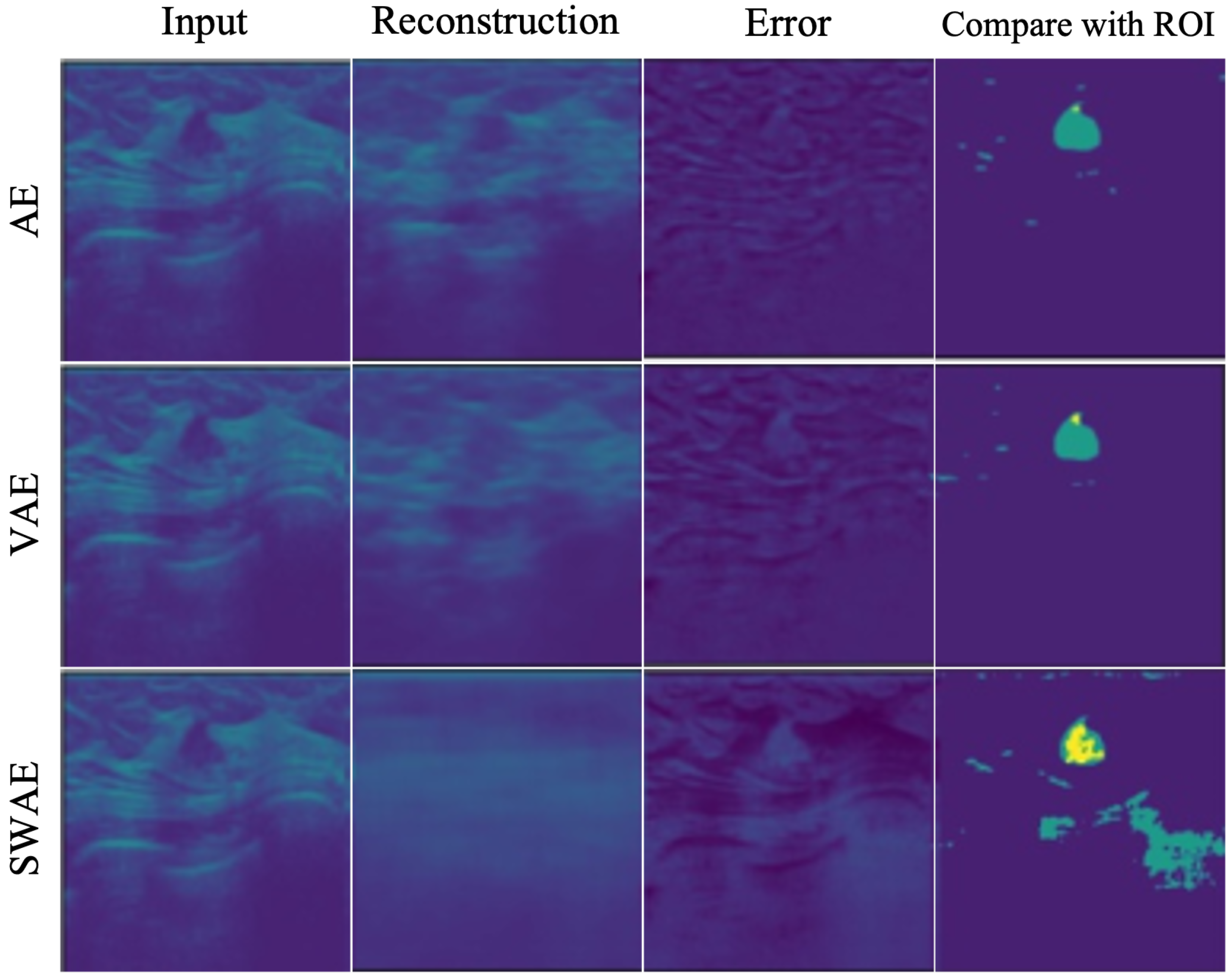
4.2.2. Anomalous Region Detection
4.3. Analysis of Factor Influencing Anomalous Region Detection in Ultrasonography
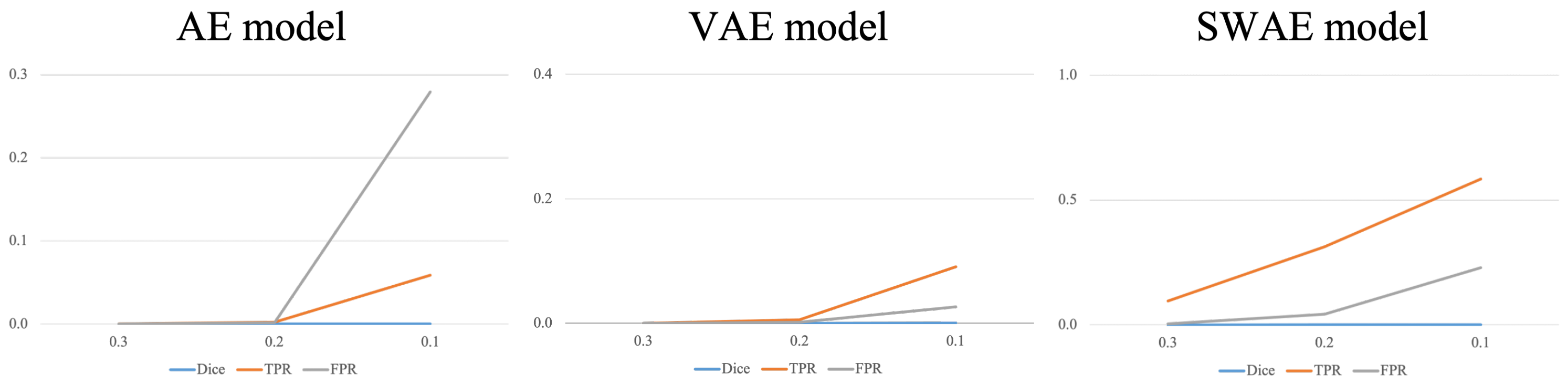
4.3.1. Threshold
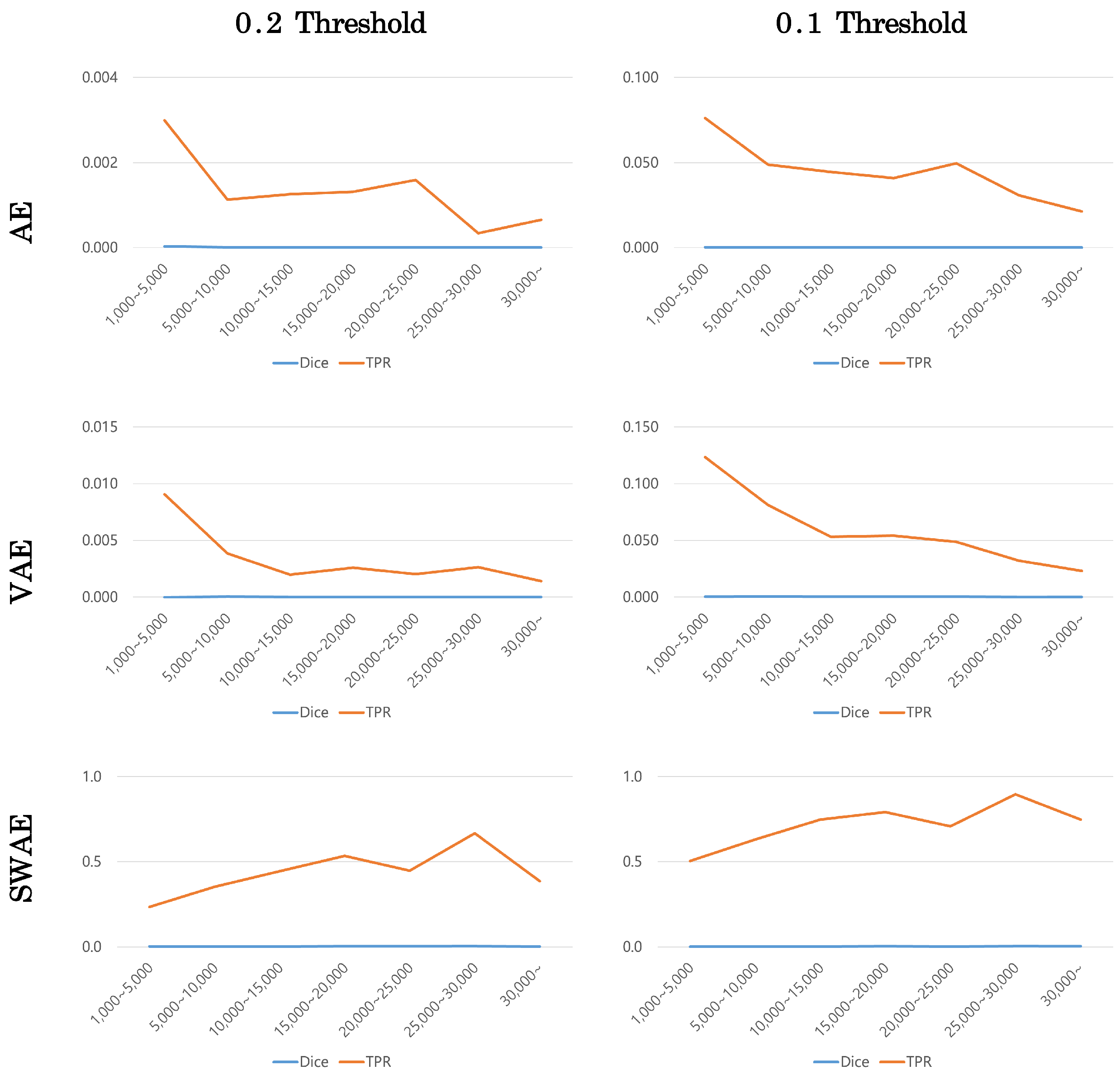
4.3.2. Size of Tumor
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Edwards, B.I.; Khougali, N.H.O.; Cheok, A.D. Trends in Computer-Aided Diagnosis Using Deep Learning Techniques: A Review of Recent Studies on Algorithm Development. Preprints 2017, 2017100117. [Google Scholar] [CrossRef]
- Alom, M.Z.; Taha, T.M.; Yakopcic, C.; Westberg, S.; Sidike, P.; Nasrin, M.S.; Hasan, M.; Van Essen, B.C.; Awwal, A.A.; Asari, V.K. A state-of-the-art survey on deep learning theory and architectures. Electronics 2019, 8, 292. [Google Scholar] [CrossRef] [Green Version]
- Shin, S.J.; Jeong, B.J. Principle and comprehension of ultrasound imaging. J. Korean Orthop. Assoc. 2013, 48, 325–333. [Google Scholar] [CrossRef] [Green Version]
- Berg, W.A.; Blume, J.D.; Cormack, J.B.; Mendelson, E.B. Operator dependence of physician-performed whole-breast US: Lesion detection and characterization. Radiology 2006, 241, 355–365. [Google Scholar] [CrossRef] [PubMed]
- Boyd, N.F.; Martin, L.J.; Yaffe, M.J.; Minkin, S. Mammographic density and breast cancer risk: Current understanding and future prospects. Breast Cancer Res. 2011, 13, 223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chandola, V.; Banerjee, A.; Kumar, V. Anomaly detection: A survey. ACM Comput. Surv. CSUR 2009, 41, 1–58. [Google Scholar] [CrossRef]
- Pang, G.; Shen, C.; Cao, L.; Hengel, A.V.D. Deep learning for anomaly detection: A review. ACM Comput. Surv. CSUR 2021, 54, 1–38. [Google Scholar] [CrossRef]
- Lee, J.G.; Jun, S.; Cho, Y.W.; Lee, H.; Kim, G.B.; Seo, J.B.; Kim, N. Deep learning in medical imaging: General overview. Korean J. Radiol. 2017, 18, 570–584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruff, L.; Vandermeulen, R.; Goernitz, N.; Deecke, L.; Siddiqui, S.A.; Binder, A.; Müller, E.; Kloft, M. Deep one-class classification. In Proceedings of the International Conference on Machine Learning. PMLR, Stockholm, Sweden, 10–15 July 2018; pp. 4393–4402. [Google Scholar]
- Zong, B.; Song, Q.; Min, M.R.; Cheng, W.; Lumezanu, C.; Cho, D.; Chen, H. Deep autoencoding Gaussian mixture model for unsupervised anomaly detection. In Proceedings of the International Conference on Learning Representations, Vancouver, BC, Canada, 30 April–3 May 2018. [Google Scholar]
- Chalapathy, R.; Chawla, S. Deep learning for anomaly detection: A survey. arXiv 2019, arXiv:1901.03407. [Google Scholar]
- Kingma, D.P.; Welling, M. Auto-encoding variational bayes. arXiv 2013, arXiv:1312.6114. [Google Scholar]
- Kolouri, S.; Pope, P.E.; Martin, C.E.; Rohde, G.K. Sliced Wasserstein auto-encoders. In Proceedings of the International Conference on Learning Representations, Vancouver, BC, Canada, 30 April–3 May 2018. [Google Scholar]
- Liao, S.; Gao, Y.; Oto, A.; Shen, D. Representation learning: A unified deep learning framework for automatic prostate MR segmentation. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Nagoya, Japan, 22–26 September 2013; Springer: Berlin/Heidelberg, Germany, 2013; pp. 254–261. [Google Scholar]
- Vasilev, A.; Golkov, V.; Meissner, M.; Lipp, I.; Sgarlata, E.; Tomassini, V.; Jones, D.K.; Cremers, D. q-Space novelty detection with variational autoencoders. In Computational Diffusion MRI; Springer: Berlin/Heidelberg, Germany, 2020; pp. 113–124. [Google Scholar]
- Chen, X.; Konukoglu, E. Unsupervised detection of lesions in brain MRI using constrained adversarial auto-encoders. arXiv 2018, arXiv:1806.04972. [Google Scholar]
- Baur, C.; Wiestler, B.; Albarqouni, S.; Navab, N. Deep autoencoding models for unsupervised anomaly segmentation in brain MR images. In Proceedings of the International MICCAI Brainlesion Workshop, Granada, Spain, 16 September 2018; Springer: Berlin/Heidelberg, Germany, 2018; pp. 161–169. [Google Scholar]
- Vu, H.S.; Ueta, D.; Hashimoto, K.; Maeno, K.; Pranata, S.; Shen, S.M. Anomaly detection with adversarial dual autoencoders. arXiv 2019, arXiv:1902.06924. [Google Scholar]
- Schlegl, T.; Seeböck, P.; Waldstein, S.M.; Schmidt-Erfurth, U.; Langs, G. Unsupervised anomaly detection with generative adversarial networks to guide marker discovery. In Proceedings of the International Conference on Information Processing in Medical Imaging, Boone, NC, USA, 25–30 June 2017; Springer: Berlin/Heidelberg, Germany, 2017; pp. 146–157. [Google Scholar]
- Seeböck, P.; Waldstein, S.M.; Klimscha, S.; Bogunovic, H.; Schlegl, T.; Gerendas, B.S.; Donner, R.; Schmidt-Erfurth, U.; Langs, G. Unsupervised identification of disease marker candidates in retinal OCT imaging data. IEEE Trans. Med Imaging 2018, 38, 1037–1047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seeböck, P.; Orlando, J.I.; Schlegl, T.; Waldstein, S.M.; Bogunović, H.; Klimscha, S.; Langs, G.; Schmidt-Erfurth, U. Exploiting epistemic uncertainty of anatomy segmentation for anomaly detection in retinal OCT. IEEE Trans. Med. Imaging 2019, 39, 87–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, K.; Gao, S.; Cheng, J.; Gu, Z.; Fu, H.; Tu, Z.; Yang, J.; Zhao, Y.; Liu, J. Sparse-gan: Sparsity-constrained generative adversarial network for anomaly detection in retinal oct image. In Proceedings of the 2020 IEEE 17th International Symposium on Biomedical Imaging (ISBI), Iowa City, IA, USA, 3–7 April 2020; pp. 1227–1231. [Google Scholar]
- Davletshina, D.; Melnychuk, V.; Tran, V.; Singla, H.; Berrendorf, M.; Faerman, E.; Fromm, M.; Schubert, M. Unsupervised anomaly detection for X-ray images. arXiv 2020, arXiv:2001.10883. [Google Scholar]
- Tataru, C.; Yi, D.; Shenoyas, A.; Ma, A. Deep Learning for abnormality detection in Chest X-Ray images. In Proceedings of the IEEE Conference on Deep Learning, Cancun, Mexico, 18–21 December 2017. [Google Scholar]
- Lu, Y.; Xu, P. Anomaly detection for skin disease images using variational autoencoder. arXiv 2018, arXiv:1807.01349. [Google Scholar]
- Burlina, P.; Joshi, N.; Billings, S.; Wang, I.J.; Albayda, J. Unsupervised deep novelty detection: Application to muscle ultrasound and myositis screening. In Proceedings of the 2019 IEEE 16th International Symposium on Biomedical Imaging (ISBI 2019), Venice, Italy, 8–11 April 2019; pp. 1910–1914. [Google Scholar]
- Naval Marimont, S.; Tarroni, G. Implicit field learning for unsupervised anomaly detection in medical images. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Strasbourg, France, 27 September–1 October 2021; Springer: Berlin/Heidelberg, Germany, 2021; pp. 189–198. [Google Scholar]
- van Hespen, K.M.; Zwanenburg, J.J.; Dankbaar, J.W.; Geerlings, M.I.; Hendrikse, J.; Kuijf, H.J. An anomaly detection approach to identify chronic brain infarcts on MRI. Sci. Rep. 2021, 11, 7714. [Google Scholar] [CrossRef] [PubMed]
- Nakao, T.; Hanaoka, S.; Nomura, Y.; Murata, M.; Takenaga, T.; Miki, S.; Watadani, T.; Yoshikawa, T.; Hayashi, N.; Abe, O. Unsupervised deep anomaly detection in chest radiographs. J. Digit. Imaging 2021, 34, 418–427. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Kim, J. Review of evaluation metrics for 3D medical image segmentation. J. Korean Soc. Imaging Infor. Med. 2017, 23, 14–20. [Google Scholar]
- Jang, J. Deep Learning Algorithms for Visual Inspection. Ph.D. Thesis, Seoul National University Graduate School, Seoul, Republic of Korea, 2020. [Google Scholar]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hyper Parameter | Value |
|---|---|
| Activation Function | LeakyReLU |
| Output Function | Sigmoid |
| Loss Function | L1 distance |
| Optimizer | Adam |
| Batch Size | 16 |
| Epochs | 150 |
| Learning Rate | 0.0002 |
| Hyper Parameter | Value |
|---|---|
| Activation Function | LeakyReLU |
| Output Function | Sigmoid |
| Loss Function | Reconstruction Error + KLD |
| Optimizer | Adam |
| Batch Size | 16 |
| Epochs | 150 |
| Learning Rate | 0.0002 |
| Hyper Parameter | Value |
|---|---|
| Activation Function | LeakyReLU |
| Output Function | Sigmoid |
| Loss Function | Reconstruction Error + SWD |
| Optimizer | Adam |
| Batch Size | 16 |
| Epochs | 150 |
| Learning Rate | 0.0002 |
| Model | Normal Ultrasound RMSE | Abnormal Ultrasound RMSE |
|---|---|---|
| AE | 0.077 | 0.072 |
| VAE | 0.089 | 0.084 |
| SWAE | 0.139 | 0.139 |
| Model | Similarity (Dice) | True Positive Rate (TPR) | False Positive Rate (FPR) |
|---|---|---|---|
| AE | 0.000017 | 0.001995 | 0.001494 |
| VAE | 0.00005 | 0.005804 | 0.001616 |
| SWAE | 0.001252 | 0.312863 | 0.043162 |
| Threshold | AE Model | VAE Model | SWAE Model |
|---|---|---|---|
| Applying Relu | 0.52675 | 0.559735 | 0.497874 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yun, C.; Eom, B.; Park, S.; Kim, C.; Kim, D.; Jabeen, F.; Kim, W.H.; Kim, H.J.; Kim, J. A Study on the Effectiveness of Deep Learning-Based Anomaly Detection Methods for Breast Ultrasonography. Sensors 2023, 23, 2864. https://0-doi-org.brum.beds.ac.uk/10.3390/s23052864
Yun C, Eom B, Park S, Kim C, Kim D, Jabeen F, Kim WH, Kim HJ, Kim J. A Study on the Effectiveness of Deep Learning-Based Anomaly Detection Methods for Breast Ultrasonography. Sensors. 2023; 23(5):2864. https://0-doi-org.brum.beds.ac.uk/10.3390/s23052864
Chicago/Turabian StyleYun, Changhee, Bomi Eom, Sungjun Park, Chanho Kim, Dohwan Kim, Farah Jabeen, Won Hwa Kim, Hye Jung Kim, and Jaeil Kim. 2023. "A Study on the Effectiveness of Deep Learning-Based Anomaly Detection Methods for Breast Ultrasonography" Sensors 23, no. 5: 2864. https://0-doi-org.brum.beds.ac.uk/10.3390/s23052864