
Pilot Study: Magnetic Motion Analysis for Swallowing Detection Using MEMS Cantilever Actuators
 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
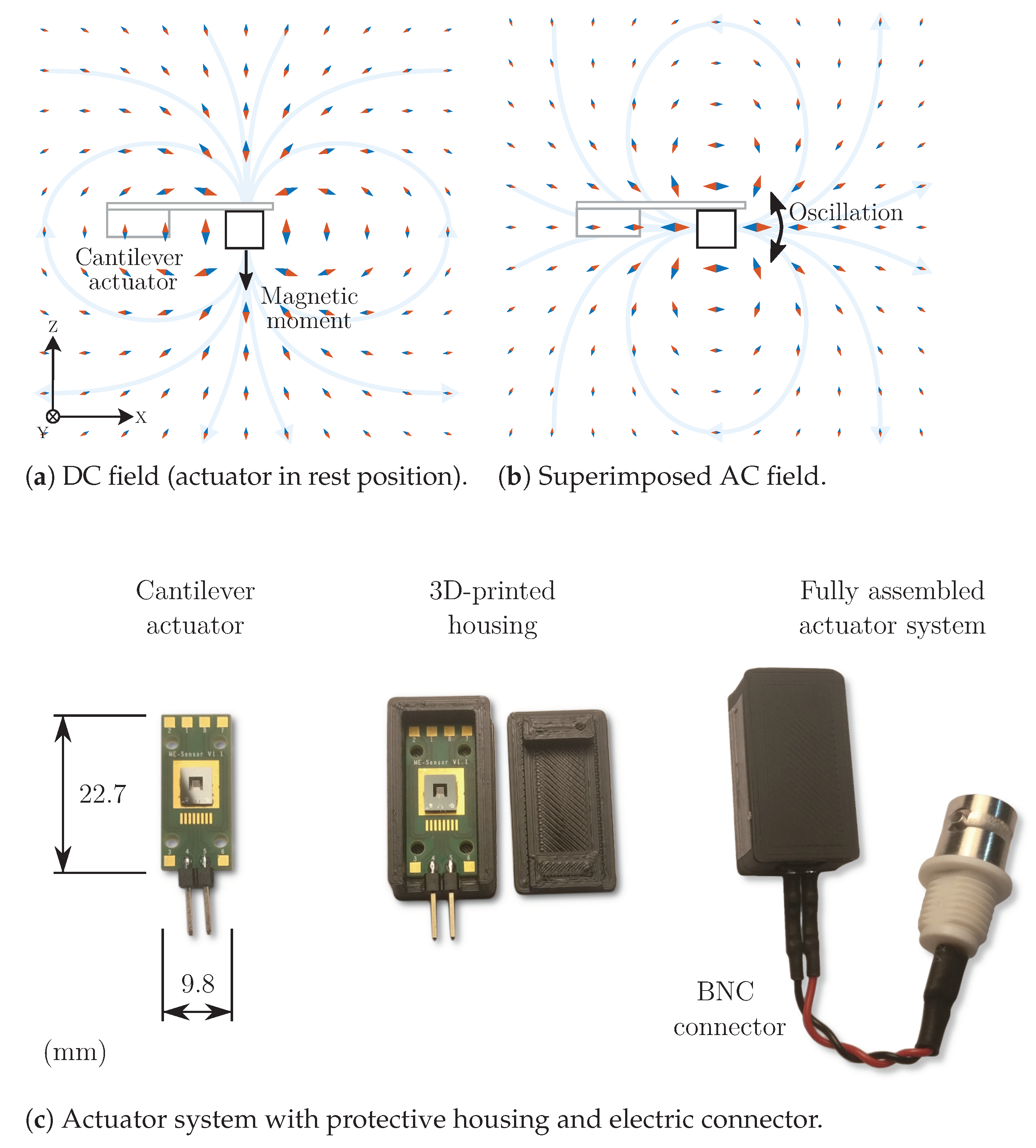
2.1. Cantilever Actuators
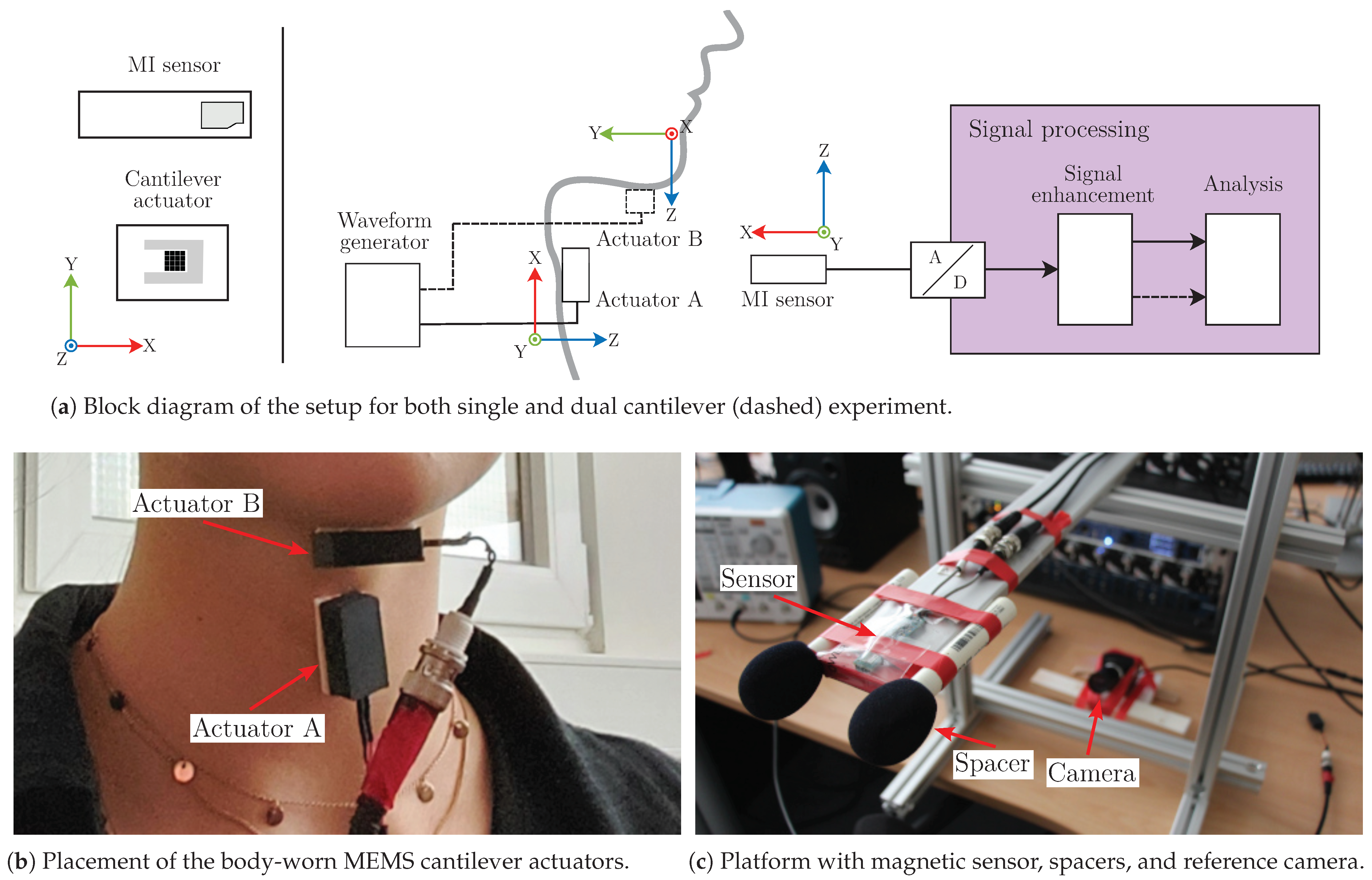
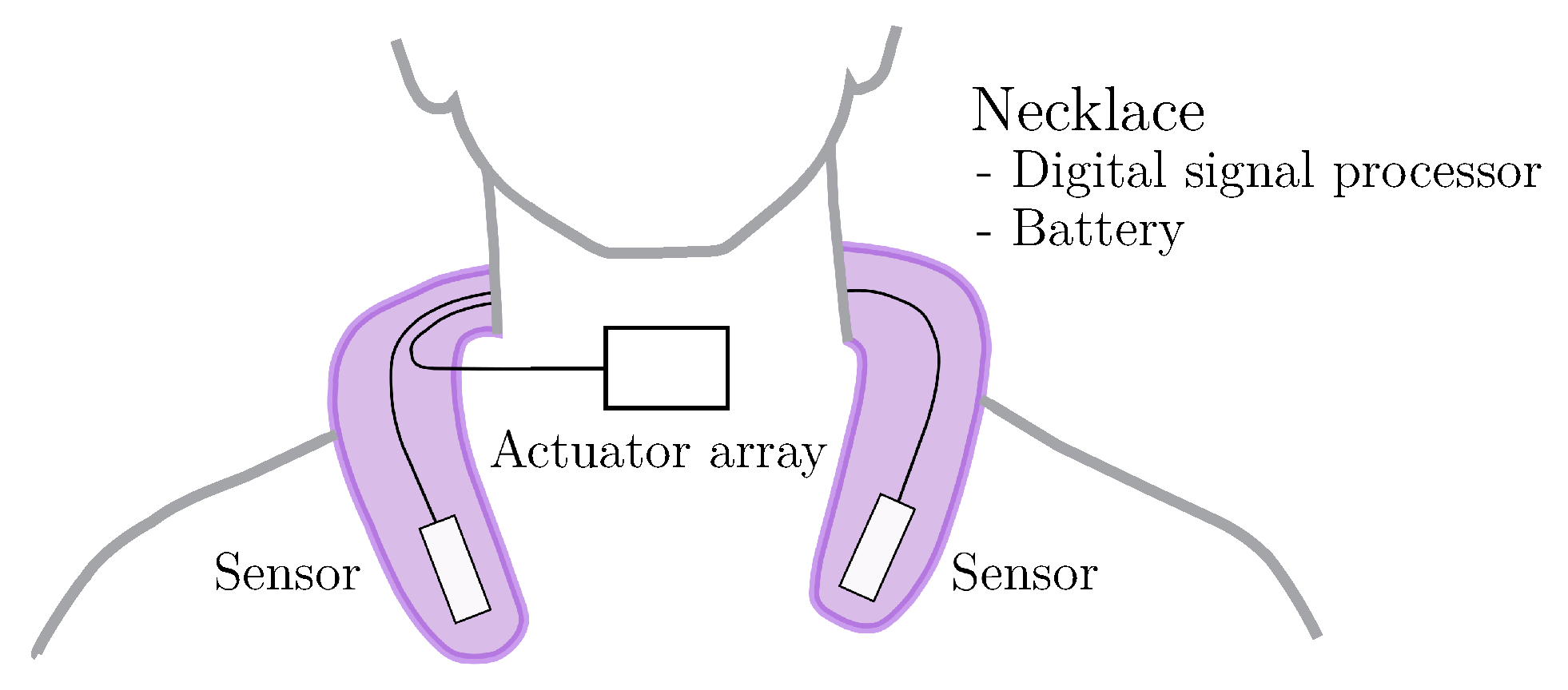
2.2. Measurement Setup
2.3. Data Acquisition
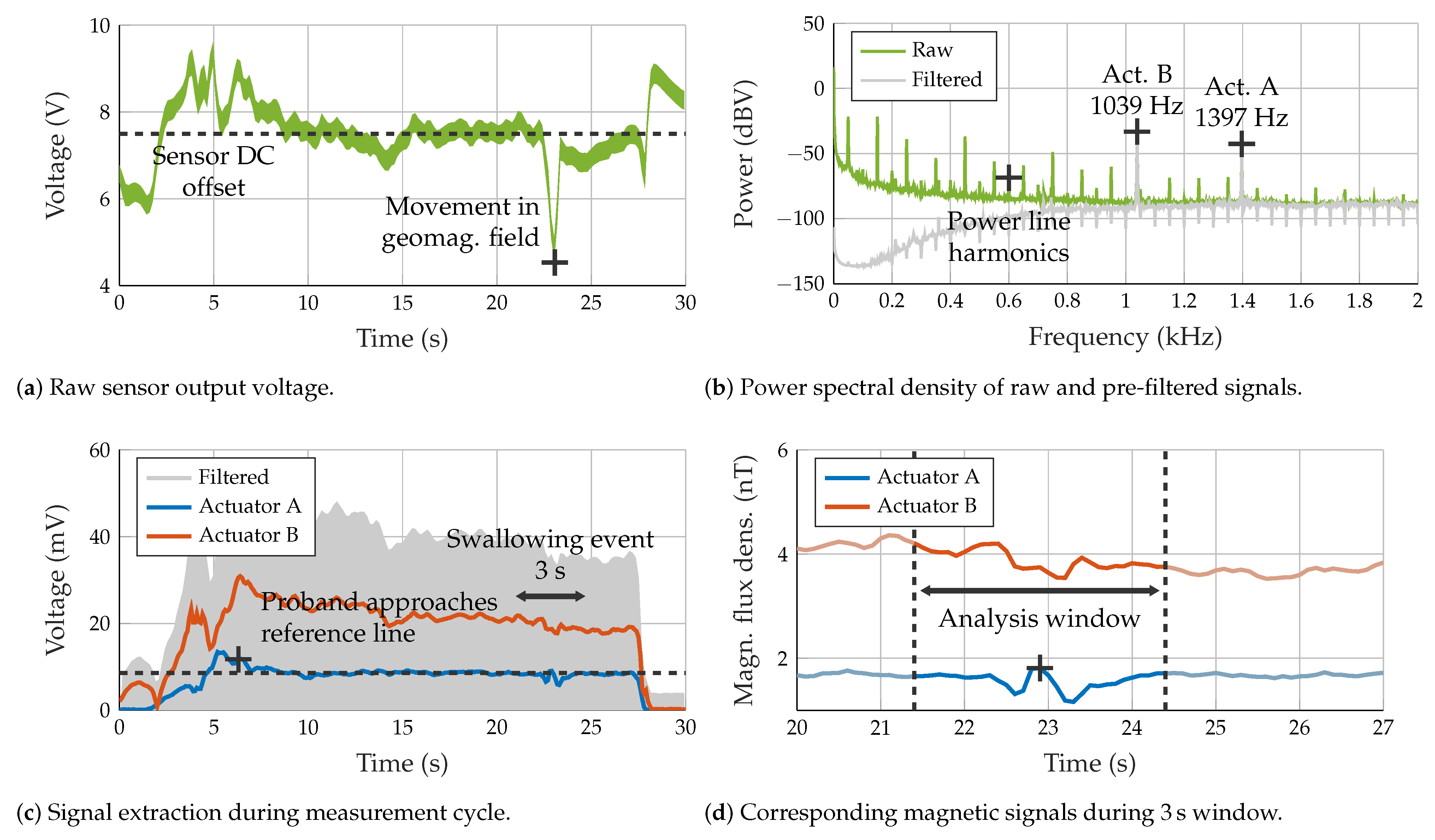
2.4. Pre-Processing
2.5. Segmentation and Detrending
2.6. Signal Characterization
3. Experiments and Results
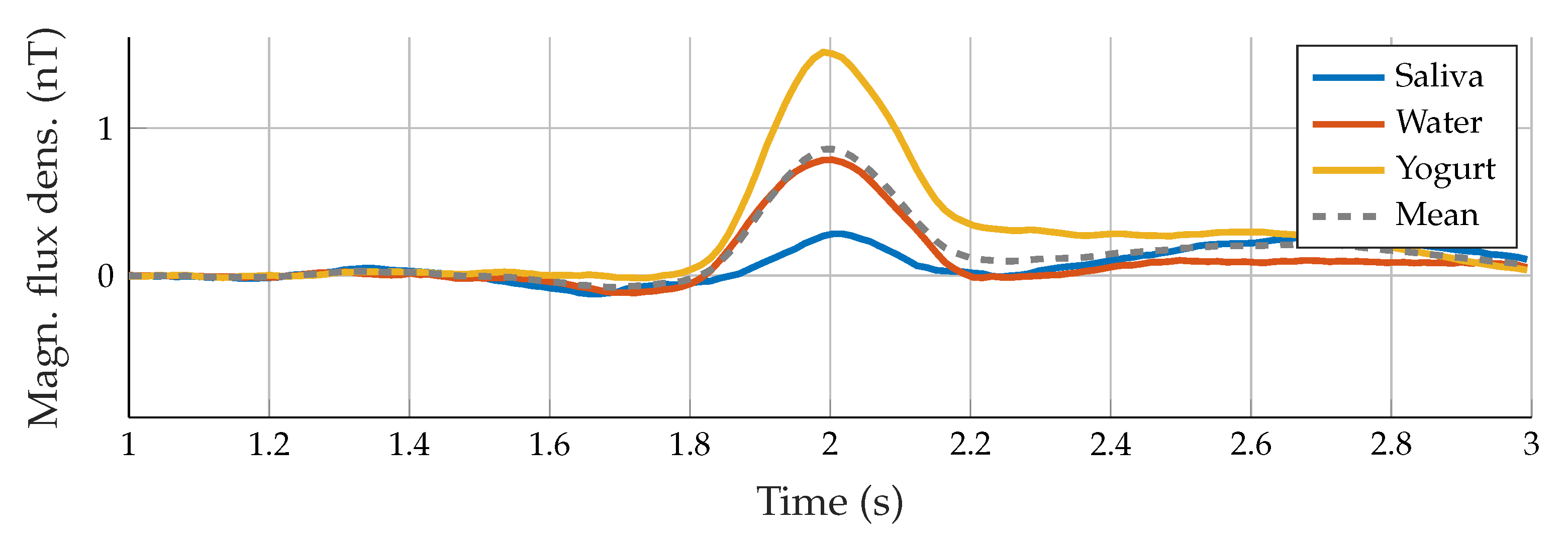
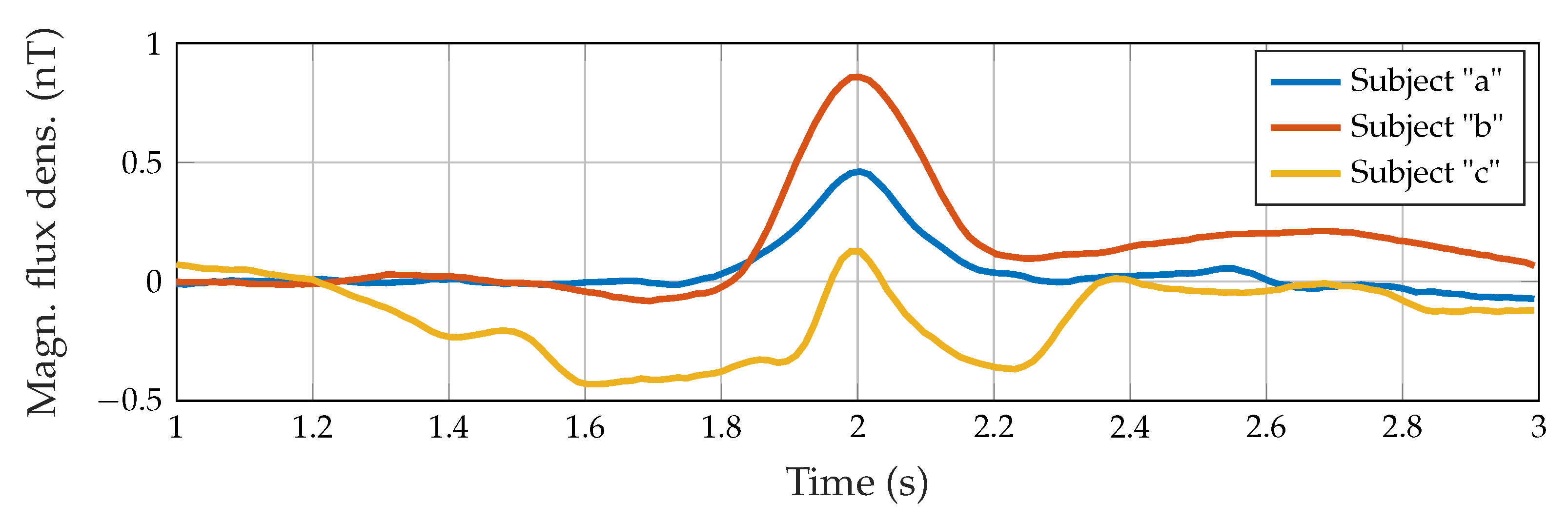
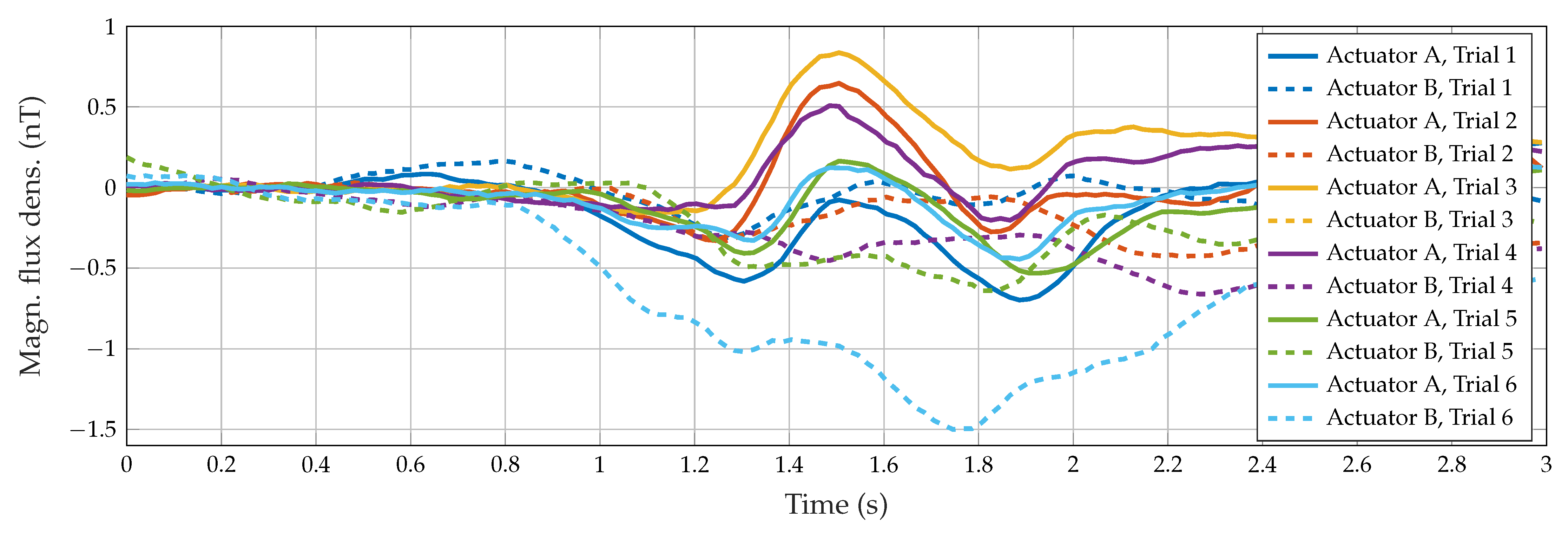
3.1. Visual Inspection
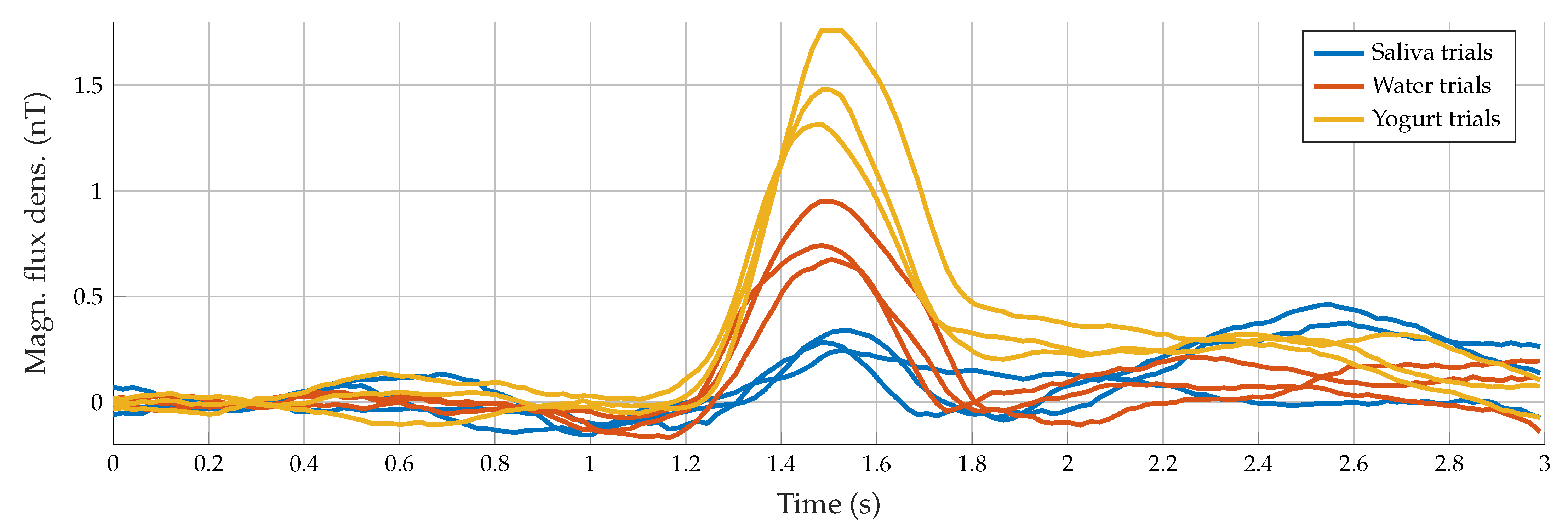
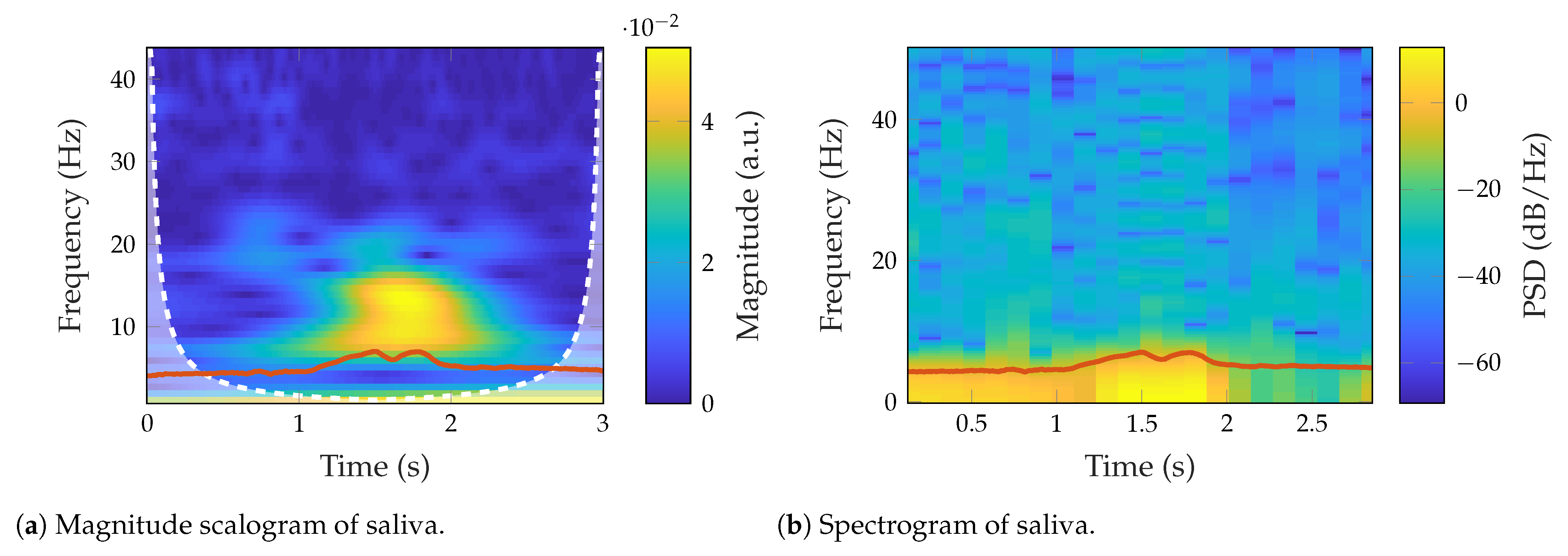
3.2. Signal Characterization
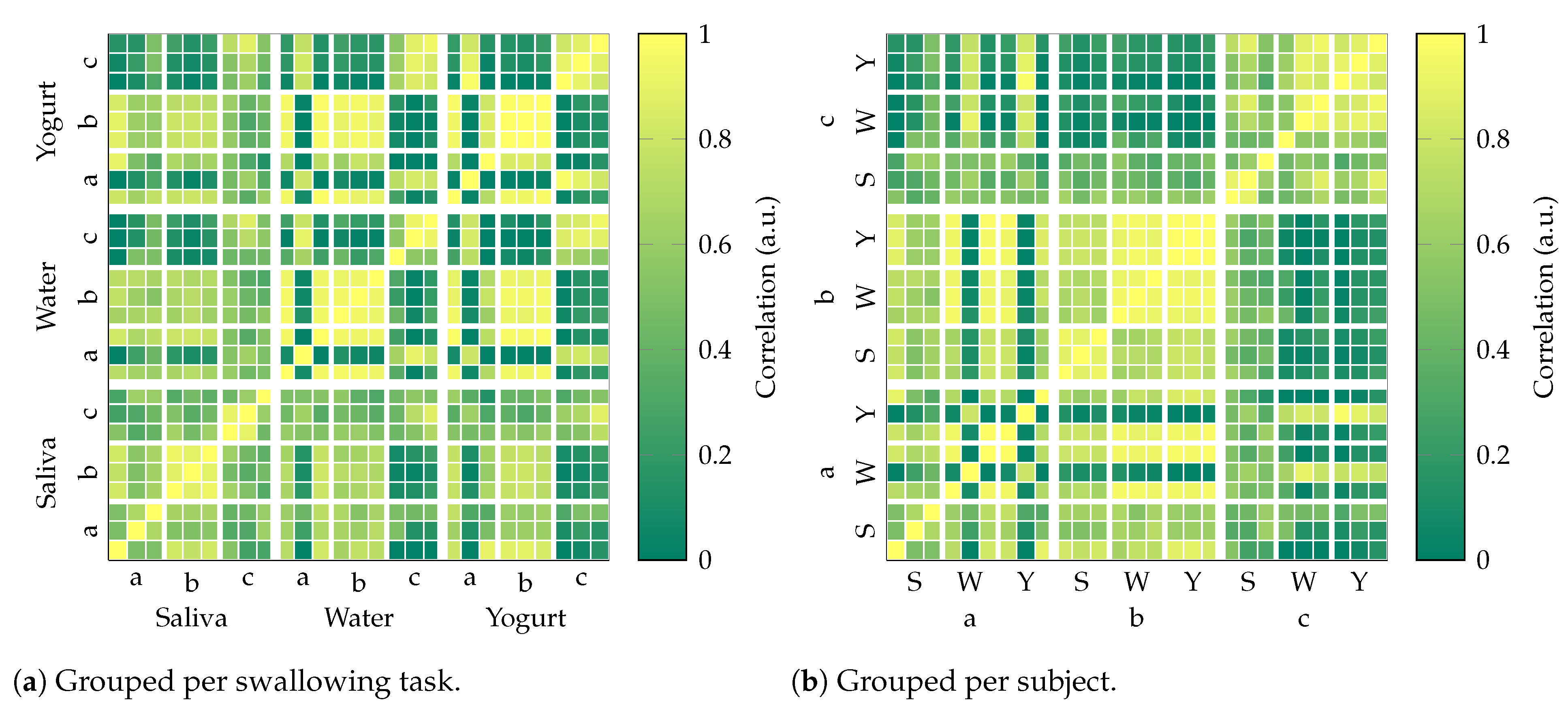
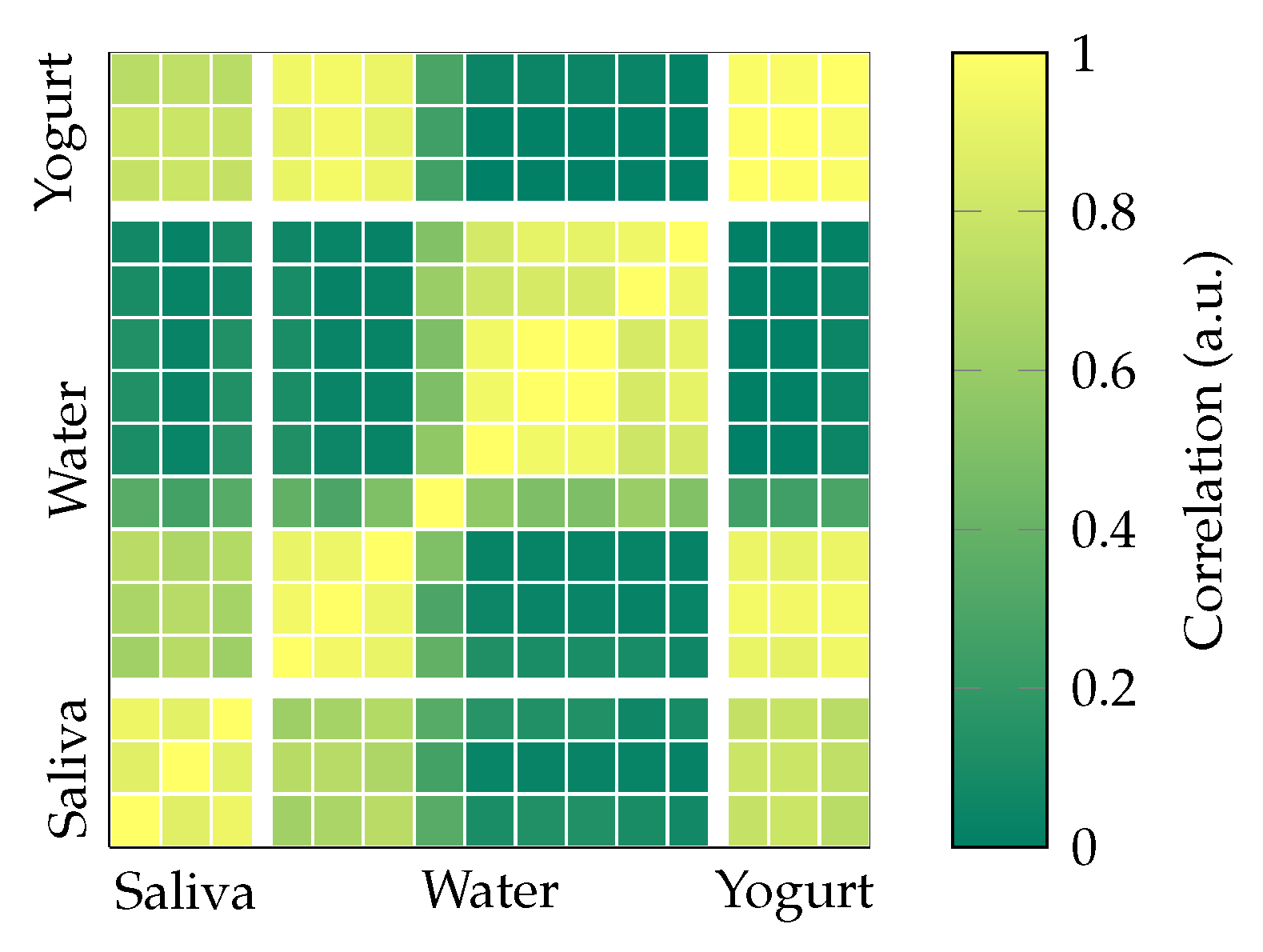
3.3. Correlation Matrix
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| MEMS | MicroElectroMechanical Systems |
| ISIT | Institute for Silicon Technology |
| CA | Cervical Auscultation |
| IMU | Inertial Measurement Unit |
| MR | MagnetoResistive |
| MI | MagnetoImpedance |
| ME | MagnetoElectric |
| PCB | Printed Circuit Board |
| ABS | Acrylonitrile Butadiene Styrene |
| DC | Direct Current |
| BNC | Bayonet Neill–Concelman |
| IIR | Infinite Impulse Response |
| RMS | Root Mean Square |
| VAR | Variance |
| MNF | Mean Frequency |
| MDF | MeDian Frequency |
| MNP | MeaN Power |
| PKF | Peak Frequency |
| BW | BandWidth |
| PSD | Power Spectral Density |
| CRC | Collaborative Research Center |
References
- Wirth, R.; Dziewas, R.; Beck, A.M.; Clavé, P.; Hamdy, S.; Heppner, H.J.; Langmore, S.; Leischker, A.H.; Martino, R.; Pluschinski, P.; et al. Oropharyngeal dysphagia in older persons–From pathophysiology to adequate intervention: A review and summary of an international expert meeting. Clin. Interv. Aging 2016, 11, 189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pfeiffer, R.F. Neurogenic dysphagia. In Bradley’s Neurology in Clinical Practice, 7th ed.; Daroff, R.B., Jankovic, J., Mazziotta, J.C., Pomeroy, S.L., Eds.; Elsevier Health Sciences: Amsterdam, The Netherlands, 2016; pp. 148–157.e2. [Google Scholar]
- Warnecke, T.; Labeit, B.; Schroeder, J.; Reckels, A.; Ahring, S.; Lapa, S.; Claus, I.; Muhle, P.; Suntrup-Krueger, S.; Dziewas, R. Neurogenic dysphagia: Systematic review and proposal of a classification system. Neurology 2021, 96, e876–e889. [Google Scholar] [CrossRef] [PubMed]
- Giraldo-Cadavid, L.F.; Gutiérrez-Achury, A.M.; Ruales-Suárez, K.; Rengifo-Varona, M.L.; Barros, C.; Posada, A.; Romero, C.; Galvis, A.M. Validation of the Spanish Version of the Eating Assessment Tool-10 (EAT-10 spa) in Colombia. A Blinded Prospective Cohort Study. Dysphagia 2016, 31, 398–406. [Google Scholar] [CrossRef]
- Earl, V.J.; Badawy, M.K. Radiation exposure to staff and patient during videofluoroscopic swallowing studies and recommended protection strategies. Dysphagia 2019, 34, 290–297. [Google Scholar] [CrossRef] [PubMed]
- Nacci, A.; Ursino, F.; La Vela, R.; Matteucci, F.; Mallardi, V.; Fattori, B. Fiberoptic endoscopic evaluation of swallowing (FEES): Proposal for informed consent. Acta Otorhinolaryngol. Ital. 2008, 28, 206. [Google Scholar] [PubMed]
- Langmore, S.E. Evaluation of oropharyngeal dysphagia: Which diagnostic tool is superior? Curr. Opin. Otolaryngol. Head Neck Surg. 2003, 11, 485–489. [Google Scholar] [CrossRef]
- Zoratto, D.; Chau, T.; Steele, C. Hyolaryngeal excursion as the physiological source of swallowing accelerometry signals. Physiol. Meas. 2010, 31, 843. [Google Scholar] [CrossRef]
- Lee, J.; Steele, C.; Chau, T. Time and time–frequency characterization of dual-axis swallowing accelerometry signals. Physiol. Meas. 2008, 29, 1105. [Google Scholar] [CrossRef]
- Dudik, J.M.; Kurosu, A.; Coyle, J.L.; Sejdić, E. A statistical analysis of cervical auscultation signals from adults with unsafe airway protection. J. Neuroeng. Rehabil. 2016, 13, 7. [Google Scholar] [CrossRef] [Green Version]
- Nikjoo, M.S.; Steele, C.M.; Sejdić, E.; Chau, T. Automatic discrimination between safe and unsafe swallowing using a reputation-based classifier. Biomed. Eng. Online 2011, 10, 100. [Google Scholar] [CrossRef] [Green Version]
- Mao, S.; Sabry, A.; Khalifa, Y.; Coyle, J.L.; Sejdic, E. Estimation of laryngeal closure duration during swallowing without invasive X-rays. Future Gener. Comput. Syst. 2021, 115, 610–618. [Google Scholar] [CrossRef]
- Donohue, C.; Khalifa, Y.; Mao, S.; Perera, S.; Sejdić, E.; Coyle, J.L. Characterizing Swallows From People With Neurodegenerative Diseases Using High-Resolution Cervical Auscultation Signals and Temporal and Spatial Swallow Kinematic Measurements. J. Speech Lang. Hear. Res. 2021, 64, 3416–3431. [Google Scholar] [CrossRef] [PubMed]
- Movahedi, F.; Kurosu, A.; Coyle, J.L.; Perera, S.; Sejdić, E. A comparison between swallowing sounds and vibrations in patients with dysphagia. Comput. Methods Programs Biomed. 2017, 144, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Hamlet, S.; Penney, D.G.; Formolo, J. Stethoscope acoustics and cervical auscultation of swallowing. Dysphagia 1994, 9, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Waito, A.; Bailey, G.L.; Molfenter, S.M.; Zoratto, D.C.; Steele, C.M. Voice-quality abnormalities as a sign of dysphagia: Validation against acoustic and videofluoroscopic data. Dysphagia 2011, 26, 125–134. [Google Scholar] [CrossRef]
- Hassan, H.E.; Aboloyoun, A.I. The value of bedside tests in dysphagia evaluation. Egypt. J. Ear Nose Throat Allied Sci. 2014, 15, 197–203. [Google Scholar] [CrossRef] [Green Version]
- Santos, K.W.d.; Scheeren, B.; Maciel, A.C.; Cassol, M. Vocal variability post swallowing in individuals with and without oropharyngeal dysphagia. Int. Arch. Otorhinolaryngol. 2015, 19, 61–66. [Google Scholar]
- Farneti, D. Voice and dysphagia. In Dysphagia; Springer: Cham, Switzerland, 2017; pp. 257–274. [Google Scholar]
- Miles, J.; Johnston, D.L.; Friary, A. Effect of Lee Silverman Voice Treatment (LSVT LOUD) on swallowing and cough in Parkinson’s disease: A pilot study. Neurol Sci. 2017, 383, 180–187. [Google Scholar] [CrossRef]
- Roldan-Vasco, S.; Orozco-Duque, A.; Suarez-Escudero, J.C.; Orozco-Arroyave, J.R. Machine learning based analysis of speech dimensions in functional oropharyngeal dysphagia. Comput. Methods Programs Biomed. 2021, 208, 106248. [Google Scholar] [CrossRef]
- Vaiman, M. Standardization of surface electromyography utilized to evaluate patients with dysphagia. Head Face Med. 2007, 3, 7. [Google Scholar] [CrossRef] [Green Version]
- Vaiman, M.; Eviatar, E. Surface electromyography as a screening method for evaluation of dysphagia and odynophagia. Head Face Med. 2009, 5, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aydogdu, I.; Kiylioglu, N.; Tarlaci, S.; Tanriverdi, Z.; Alpaydin, S.; Acarer, A.; Baysal, L.; Arpaci, E.; Yuceyar, N.; Secil, Y.; et al. Diagnostic value of “dysphagia limit” for neurogenic dysphagia: 17 years of experience in 1278 adults. Clin. Neurophysiol. 2015, 126, 634–643. [Google Scholar] [CrossRef] [PubMed]
- Schultheiss, C.; Schauer, T.; Nahrstaedt, H.; Seidl, R.O. Automated detection and evaluation of swallowing using a combined EMG/bioimpedance measurement system. Sci. World J. 2014, 2014, 405471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, M.; Yu, B.; Yang, W.; Jiang, Y.; Lu, L.; Huang, Z.; Chen, S.; Li, G. Evaluation of normal swallowing functions by using dynamic high-density surface electromyography maps. Biomed. Eng. Online 2017, 16, 18. [Google Scholar] [CrossRef] [Green Version]
- Constantinescu, G.; Hodgetts, W.; Scott, D.; Kuffel, K.; King, B.; Brodt, C.; Rieger, J. Electromyography and mechanomyography signals during swallowing in healthy adults and head and neck cancer survivors. Dysphagia 2017, 32, 90–103. [Google Scholar] [CrossRef]
- Riebold, B.; Nahrstaedt, H.; Schauer, T.; Seidl, R.O. Self-adapting Classification System for Swallow Intention Detection in Dysphagia Therapy. Curr. Dir. Biomed. Eng. 2019, 5, 49–52. [Google Scholar] [CrossRef]
- Roldan-Vasco, S.; Restrepo-Agudelo, S.; Valencia-Martinez, Y.; Orozco-Duque, A. Automatic detection of oral and pharyngeal phases in swallowing using classification algorithms and multichannel EMG. J. Electromyogr. Kinesiol. 2018, 43, 193–200. [Google Scholar] [CrossRef]
- Suzuki, M.; Sasaki, M.; Kamata, K.; Nakayama, A.; Shibamoto, I.; Tamada, Y. Swallowing pattern classification method using multichannel surface EMG signals of suprahyoid and infrahyoid muscles. Adv. Biomed. Eng. 2020, 9, 10–20. [Google Scholar] [CrossRef] [Green Version]
- Inoue, K.; Yoshioka, M.; Yagi, N.; Nagami, S.; Oku, Y. Using machine learning and a combination of respiratory flow, laryngeal motion, and swallowing sounds to classify safe and unsafe swallowing. IEEE Trans. Biomed. Eng. 2018, 65, 2529–2541. [Google Scholar] [CrossRef]
- Lee, J.; Steele, C.M.; Chau, T. Swallow segmentation with artificial neural networks and multi-sensor fusion. Med. Eng. Phys. 2009, 31, 1049–1055. [Google Scholar] [CrossRef]
- Ertekin, C.; Aydoğdu, I.; Yüceyar, N. Piecemeal deglutition and dysphagia limit in normal subjects and in patients with swallowing disorders. J. Neurol. Neurosurg. Psychiatry 1996, 61, 491–496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalantarian, H.; Alshurafa, N.; Le, T.; Sarrafzadeh, M. Monitoring eating habits using a piezoelectric sensor-based necklace. Comput. Biol. Med. 2015, 58, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Sabatini, A.M. Quaternion-based extended Kalman filter for determining orientation by inertial and magnetic sensing. IEEE Trans. Biomed. Eng. 2006, 53, 1346–1356. [Google Scholar] [CrossRef] [PubMed]
- Yun, X.; Calusdian, E.; Bachmann, R.; McGhee, R.B. Estimation of Human Foot Motion During Normal Walking Using Inertial and Magnetic Sensor Measurements. IEEE Trans. Instrum. Meas. 2012, 61, 2059–2072. [Google Scholar] [CrossRef]
- Cheng, C.; Huo, X.; Ghovanloo, M. Towards a magnetic localization system for 3-D tracking of tongue movements in speech-language therapy. In Proceedings of the 2009 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Minneapolis, MN, USA, 3–6 September 2009; pp. 563–566. [Google Scholar] [CrossRef] [Green Version]
- Hu, C.; Song, S.; Wang, X.; Meng, M.; Li, B. A Novel Positioning and Orientation System Based on Three-Axis Magnetic Coils. IEEE Trans. Magn. 2012, 48, 2211–2219. [Google Scholar] [CrossRef]
- Bald, C.; Schmidt, G. Processing Chain for Localization of Magnetoelectric Sensors in Real Time. Sensors 2021, 21, 5675. [Google Scholar] [CrossRef]
- Hoffmann, H.; Hansen, C.; Maetzler, W.; Schmidt, G. A Concept for 6D Motion Sensing with Magnetoelectric Sensors. Curr. Dir. Biomed. Eng. 2022, 8, 451–454. [Google Scholar] [CrossRef]
- Hoffmann, J.; Elzenheimer, E.; Bald, C.; Hansen, C.; Maetzler, W.; Schmidt, G. Active Magnetoelectric Motion Sensing: Examining Performance Metrics with an Experimental Setup. Sensors 2021, 21, 8000. [Google Scholar] [CrossRef]
- Kaluza, F.; Grüger, A.; Grüger, H. New and future applications of fluxgate sensors. Sens. Actuators A Phys. 2003, 106, 48–51. [Google Scholar] [CrossRef]
- Jogschies, L.; Klaas, D.; Kruppe, R.; Rittinger, J.; Taptimthong, P.; Wienecke, A.; Rissing, L.; Wurz, M. Recent Developments of Magnetoresistive Sensors for Industrial Applications. Sensors 2015, 15, 28665–28689. [Google Scholar] [CrossRef] [Green Version]
- Wang, T.; Zhou, Y.; Lei, C.; Luo, J.; Xie, S.; Pu, H. Magnetic impedance biosensor: A review. Biosens. Bioelectron. 2017, 90, 418–435. [Google Scholar] [CrossRef] [PubMed]
- Elzenheimer, E.; Bald, C.; Engelhardt, E.; Hoffmann, J.; Hayes, P.; Arbustini, J.; Bahr, A.; Quandt, E.; Höft, M.; Schmidt, G. Quantitative Evaluation for Magnetoelectric Sensor Systems in Biomagnetic Diagnostics. Sensors 2022, 22, 1018. [Google Scholar] [CrossRef] [PubMed]
- Niekiel, F.; Su, J.; Bodduluri, M.T.; Lisec, T.; Blohm, L.; Pieper, I.; Wagner, B.; Lofink, F. Highly sensitive MEMS magnetic field sensors with integrated powder-based permanent magnets. Sens. Actuators A Phys. 2019, 297, 111560. [Google Scholar] [CrossRef]
- Dong, C.; He, Y.; Li, M.; Tu, C.; Chu, Z.; Liang, X.; Chen, H.; Wei, Y.; Zaeimbashi, M.; Wang, X.; et al. A Portable Very Low Frequency (VLF) Communication System Based on Acoustically Actuated Magnetoelectric Antennas. IEEE Antennas Wirel. Propag. Lett. 2020, 19, 398–402. [Google Scholar] [CrossRef]
- Arbustini, J.; Muñoz, J.; Wang, H.; Elzenheimer, E.; Hoffmann, H.; Thormählen, L.; Hayes, P.; Niekiel, F.; Heidari, H.; Höft, M.; et al. MEMS Magnetic Field Source for Frequency Conversion Approaches for ME Sensors. Curr. Dir. Biomed. Eng. 2022, 8, 309–312. [Google Scholar] [CrossRef]
- Moriniére, S.; Boiron, M.; Alison, D.; Makris, P.; Beutter, P. Origin of the sound components during pharyngeal swallowing in normal subjects. Dysphagia 2008, 23, 267–273. [Google Scholar] [CrossRef]
- Dudik, J.M.; Coyle, J.L.; Sejdić, E. Dysphagia screening: Contributions of cervical auscultation signals and modern signal-processing techniques. IEEE Trans.-Hum.-Mach. Syst. 2015, 45, 465–477. [Google Scholar] [CrossRef] [Green Version]
- Shaw, S.M.; Martino, R. The normal swallow: Muscular and neurophysiological control. Otolaryngol. Clin. N. Am. 2013, 46, 937–956. [Google Scholar] [CrossRef]
- Sampaio, M.; Argolo, N.; Melo, A.; Nóbrega, A.C. Wet voice as a sign of penetration/aspiration in Parkinson’s disease: Does testing material matter? Dysphagia 2014, 29, 610–615. [Google Scholar] [CrossRef]
- van den Engel-Hoek, L.; de Groot, I.J.; Esser, E.; Gorissen, B.; Hendriks, J.C.; de Swart, B.J.; Geurts, A.C. Biomechanical events of swallowing are determined more by bolus consistency than by age or gender. Physiol. Behav. 2012, 106, 285–290. [Google Scholar] [CrossRef]
- Walton, J.; Silva, P. Physiology of swallowing. Surgery 2018, 36, 529–534. [Google Scholar]
- Schmidt, G.; Bald, C.; Kreisel, J. Removal of Signal Trends. Available online: https://dss-kiel.de/index.php/teaching/red-main/red-trend-removal (accessed on 27 December 2022).
- Phinyomark, A.; Phukpattaranont, P.; Limsakul, C. Feature reduction and selection for EMG signal classification. Expert Syst. Appl. 2012, 39, 7420–7431. [Google Scholar] [CrossRef]
- Dudik, J.M.; Jestrović, I.; Luan, B.; Coyle, J.L.; Sejdić, E. A comparative analysis of swallowing accelerometry and sounds during saliva swallows. Biomed. Eng. Online 2015, 14, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roldan-Vasco, S.; Perez-Giraldo, E.; Orozco-Duque, A. Continuous wavelet transform for muscle activity detection in surface EMG signals during swallowing. In Proceedings of the Workshop on Engineering Applications, Medellín, Colombia, 17–19 October 2018; Springer: Cham, Switzerland, 2018; pp. 245–255. [Google Scholar]
- Roldán-Vasco, S.; Pérez-Giraldo, E.; Orozco-Duque, A. Scalogram-energy based segmentation of surface electromyography signals from swallowing related muscles. Comput. Methods Programs Biomed. 2020, 194, 105480. [Google Scholar] [CrossRef]
- Watts, C.R.; Kelly, B. The effect of bolus consistency and sex on electrophysiological measures of hyolaryngeal muscle activity during swallowing. Dysphagia 2015, 30, 551–557. [Google Scholar] [CrossRef]
- Nakao, Y.; Onishi, H.; Haji, T.; Shiromoto, O.; Saito, S.; Nanto, T.; Uchiyama, Y.; Domen, K. Impact of Thickened Liquids on Laryngeal Movement Velocity in Patients with Dysphagia. Dysphagia 2022, 37, 207–215. [Google Scholar] [CrossRef]
- Youmans, S.R.; Stierwalt, J.A. Normal swallowing acoustics across age, gender, bolus viscosity, and bolus volume. Dysphagia 2011, 26, 374–384. [Google Scholar] [CrossRef]
- Taniwaki, M.; Kohyama, K. Fast Fourier transform analysis of sounds made while swallowing various foods. J. Acoust. Soc. Am. 2012, 132, 2478–2482. [Google Scholar] [CrossRef]
- Dudik, J.M.; Jestrović, I.; Luan, B.; Coyle, J.L.; Sejdić, E. Characteristics of dry chin-tuck swallowing vibrations and sounds. IEEE Trans. Biomed. Eng. 2015, 62, 2456–2464. [Google Scholar] [CrossRef] [Green Version]
- Restrepo-Agudelo, S.; Roldan-Vasco, S.; Ramirez-Arbelaez, L.; Cadavid-Arboleda, S.; Perez-Giraldo, E.; Orozco-Duque, A. Improving surface EMG burst detection in infrahyoid muscles during swallowing using digital filters and discrete wavelet analysis. J. Electromyogr. Kinesiol. 2017, 35, 8. [Google Scholar] [CrossRef]
- Sunada, Y.; Magara, J.; Tsujimura, T.; Ono, K.; Inoue, M. Endurance measurement of hyoid muscle activity and hyoid-laryngeal position during tongue lift movement. J. Oral Rehabil. 2020, 47, 967–976. [Google Scholar] [CrossRef]
- Koshi, N.; Magara, J.; Sakai, S.; Tsujimura, T.; Ono, K.; Inoue, M. Properties of hyoid muscle contraction during tongue lift measurement. J. Oral Rehabil. 2020, 47, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Monaco, A.; Cattaneo, R.; Spadaro, A.; Giannoni, M. Surface electromyography pattern of human swallowing. BMC Oral Health 2008, 8, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khalifa, Y.; Coyle, J.L.; Sejdić, E. Non-invasive identification of swallows via deep learning in high resolution cervical auscultation recordings. Sci. Rep. 2020, 10, 13. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject | Sex | Age |
|---|---|---|
| a | Male | 36 |
| b | Female | 24 |
| c | Male | 50 |
| Feature | Equation | Feature | Equation |
|---|---|---|---|
| VAR | RMS | ||
| MNP | MNF | ||
| MDF | PKF | ||
| Feature | Saliva | Water | Yogurt |
|---|---|---|---|
| Amplitude (nT) | 0.67 ± 0.08 | 0.66 ± 0.13 | 0.85 ± 0.13 |
| Pulse width (s) | 0.28 ± 0.01 | 0.26 ± 0.03 | 0.29 ± 0.04 |
| RMS (nT) | 0.28 ± 0.18 | 0.19 ± 0.07 | 0.30 ± 0.08 |
| VAR (nT2) | 0.10 ± 0.12 | 0.04 ± 0.03 | 0.09 ± 0.05 |
| MNF (Hz) | 0.83 ± 0.20 | 1.03 ± 0.18 | 0.73 ± 0.13 |
| MDF (Hz) | 0.56 ± 0.21 | 0.85 ± 0.25 | 0.47 ± 0.16 |
| PKF (Hz) | 0.43 ± 0.29 | 0.67 ± 0.38 | 0.33 ± 0.10 |
| (Hz) | 0.24 ± 0.05 | 0.34 ± 0.16 | 0.24 ± 0.05 |
| (Hz) | 0.73 ± 0.34 | 1.08 ± 0.51 | 0.51 ± 0.08 |
| BW (Hz) | 0.50 ± 0.31 | 0.73 ± 0.47 | 0.27 ± 0.08 |
| MNP (nT2Hz−1) | 0.06 ± 0.07 | 0.02 ± 0.02 | 0.06 ± 0.03 |
| (dB) | 12.68 ± 5.49 | 9.93 ± 3.61 | 14.57 ± 2.23 |
| (dB) | −7.78 ± 5.04 | −7.69 ± 4.44 | −5.97 ± 3.58 |
| Feature | Actuator A | Actuator B |
|---|---|---|
| RMS (nT) | 0.21 ± 0.05 | 0.23 ± 0.13 |
| VAR (nT2) | 0.05 ± 0.02 | 0.06 ± 0.07 |
| MNF (Hz) | 1.00 ± 0.24 | 0.64 ± 0.23 |
| MDF (Hz) | 0.74 ± 0.30 | 0.38 ± 0.21 |
| PKF (Hz) | 0.42 ± 0.29 | 0.33 ± 0.24 |
| (Hz) | 0.31 ± 0.18 | 0.21 ± 0.13 |
| (Hz) | 0.60 ± 0.32 | 0.56 ± 0.19 |
| BW (Hz) | 0.30 ± 0.17 | 0.35 ± 0.13 |
| MNP (nT2Hz−1) | 0.03 ± 0.01 | 0.04 ± 0.05 |
| (dB) | 11.35 ± 2.15 | 11.78 ± 4.76 |
| (dB) | −7.78 ± 1.45 | −11.20 ± 3.42 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hoffmann, J.; Roldan-Vasco, S.; Krüger, K.; Niekiel, F.; Hansen, C.; Maetzler, W.; Orozco-Arroyave, J.R.; Schmidt, G. Pilot Study: Magnetic Motion Analysis for Swallowing Detection Using MEMS Cantilever Actuators. Sensors 2023, 23, 3594. https://0-doi-org.brum.beds.ac.uk/10.3390/s23073594
Hoffmann J, Roldan-Vasco S, Krüger K, Niekiel F, Hansen C, Maetzler W, Orozco-Arroyave JR, Schmidt G. Pilot Study: Magnetic Motion Analysis for Swallowing Detection Using MEMS Cantilever Actuators. Sensors. 2023; 23(7):3594. https://0-doi-org.brum.beds.ac.uk/10.3390/s23073594
Chicago/Turabian StyleHoffmann, Johannes, Sebastian Roldan-Vasco, Karolin Krüger, Florian Niekiel, Clint Hansen, Walter Maetzler, Juan Rafael Orozco-Arroyave, and Gerhard Schmidt. 2023. "Pilot Study: Magnetic Motion Analysis for Swallowing Detection Using MEMS Cantilever Actuators" Sensors 23, no. 7: 3594. https://0-doi-org.brum.beds.ac.uk/10.3390/s23073594