

Indirect Calorimetry in Spontaneously Breathing, Mechanically Ventilated and Extracorporeally Oxygenated Patients: An Engineering Review

Abstract
:1. Introduction
2. Theoretical Aspects of Indirect Calorimetry
2.1. The Weir Formula
2.2. The Haldane Transformation
3. Technical Aspects of Indirect Calorimetry
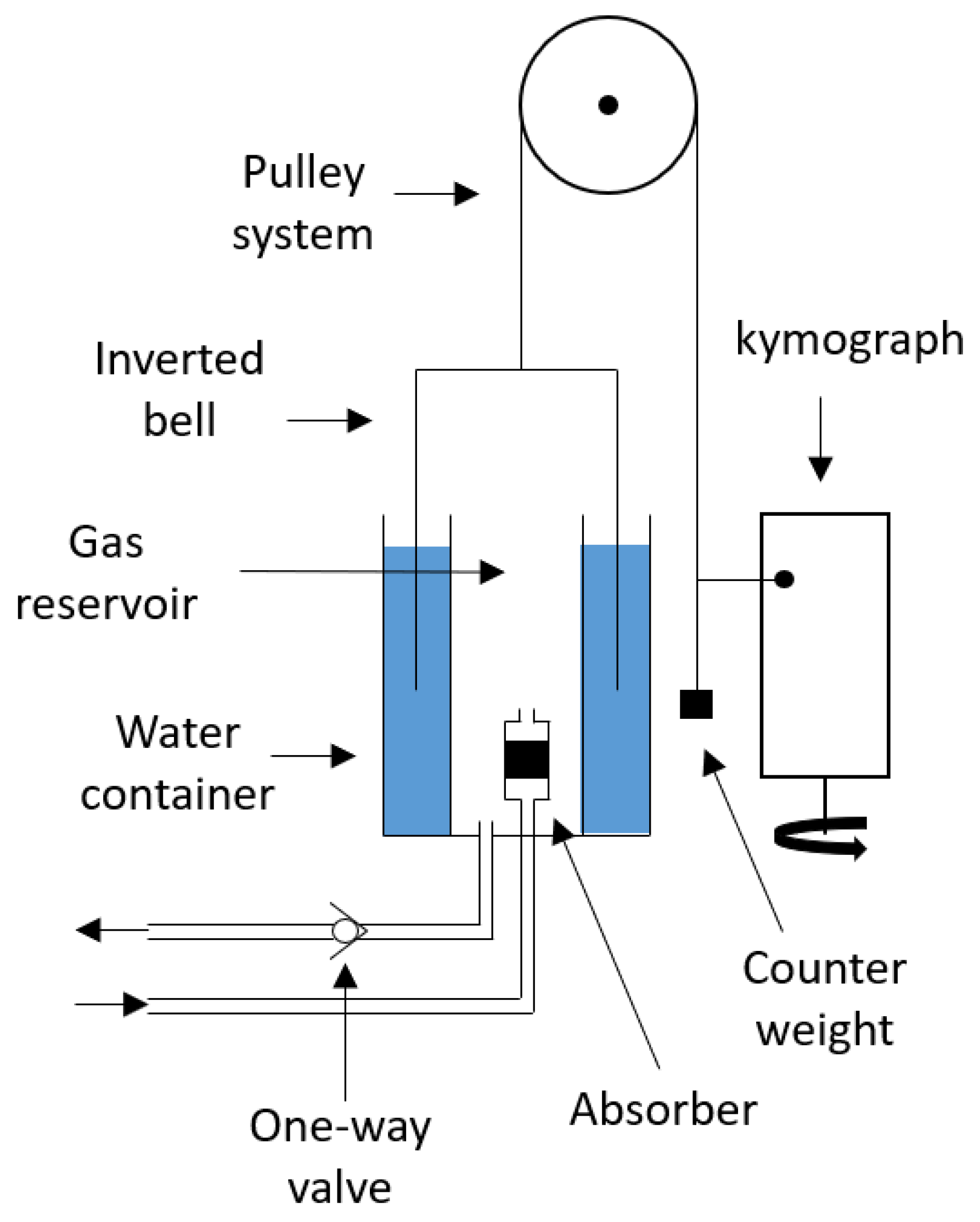
3.1. Closed-Circuit Indirect Calorimetry
3.2. Open-Circuit Technique
4. Indirect Calorimetry in Patients Undergoing ECMO
4.1. Traditional Indirect Calorimetry in Patients Undergoing ECMO
4.2. A Combination of Traditional Indirect Calorimetry and Blood Gas Analysis in Patients Undergoing ECMO
5. Sensors Used in Indirect Calorimeters
5.1. Oxygen Analyzer
5.2. Carbon Dioxide Analyzer
5.3. Flow Meter
6. Discussion
6.1. Comparison between the Open- and Closed-Circuit Indirect Calorimetry Techniques
6.2. Comparison between Mixing Chamber and Breath-by-Breath
6.3. Comparison of Current Indirect Calorimetry Techniques for Patients Undergoing ECMO
6.4. Limitations and Advantages of the Sensors Used in Indirect Calorimetry
7. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ASPEN | American Society for Parental and Enteral Nutrition and Metabolism |
| BGA | Blood gas analysis |
| Carbon dioxide | |
| ECMO | Extracorporeal Membrane Oxygenation |
| ESPEN | European Society for Clinical Nutrition and Metabolism |
| GFC | Galvanic fuel cell |
| IC | Indirect calorimetry |
| MEEP | Measuring Energy Expenditure in extracorporeal lung support Patients |
| Nitrogen | |
| NDIR | Non-dispersive infrared |
| Oxygen | |
| REE | Resting energy expenditure |
| RQ | Respiratory quotient |
| SCCM | Society of Critical Care Medicine |
| UN | Urinary nitrogen |
Symbols
| c | Concentration (mol m) |
| D | Diameter (m) |
| F | Volume fraction (%v/v) |
| I | Light intensity (W m) |
| L | Length (m) |
| m | Mass (kg) |
| Mass flow rate (kg s) | |
| p | Fraction of caloric production due to protein metabolism (%) |
| P | Pressure (Pa) |
| t | Time (s) |
| T | Period (s) |
| T | Temperature (°C) |
| T | Transmittance (-) |
| Volumetric flow rate (m s) | |
| Relative error (%) | |
| Molar absorption coefficient (m mol) | |
| µ | Dynamic viscosity (Pa s) |
Appendix A. Derivation of the Weir Formula

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Carbohydrate | Protein | Fat | |
|---|---|---|---|
| RQ | 1 | 0.802 | 0.718 |
| Energy per volume metabolized (kcal/L) | 5.047 | 4.463 | 4.735 |
Appendix B. Derivation of the Haldane Transformation
References
- Singer, P.; Blaser, A.R.; Berger, M.M.; Alhazzani, W.; Calder, P.C.; Casaer, M.P.; Hiesmayr, M.; Mayer, K.; Montejo, J.C.; Pichard, C.; et al. ESPEN guideline on clinical nutrition in the intensive care unit. Clin. Nutr. 2019, 38, 48–79. [Google Scholar] [CrossRef] [PubMed]
- Duan, J.Y.; Zheng, W.H.; Zhou, H.; Xu, Y.; Huang, H.B. Energy delivery guided by indirect calorimetry in critically ill patients: A systematic review and meta-analysis. Crit. Care 2021, 25, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Pertzov, B.; Bar-Yoseph, H.; Menndel, Y.; Bendavid, I.; Kagan, I.; Glass, Y.D.; Singer, P. The effect of indirect calorimetry guided isocaloric nutrition on mortality in critically ill patients—A systematic review and meta-analysis. Eur. J. Clin. Nutr. 2022, 76, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Harvey, S.E.; Segaran, E.; Leonard, R. Trial of the route of early nutritional support in critically ill adults. N. Eng. J. Med. 2015, 372, 488–489. [Google Scholar] [CrossRef] [PubMed]
- Heidegger, C.P.; Berger, M.M.; Graf, S.; Zingg, W.; Darmon, P.; Costanza, M.C.; Thibault, R.; Pichard, C. Optimisation of energy provision with supplemental parenteral nutrition in critically ill patients: A randomised controlled clinical trial. Lancet 2013, 381, 385–393. [Google Scholar] [CrossRef]
- McClave, S.A.; Taylor, B.E.; Martindale, R.G.; Warren, M.M.; Johnson, D.R.; Braunschweig, C.; McCarthy, M.S.; Davanos, E.; Rice, T.W.; Cresci, G.A.; et al. Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Adult Critically Ill Patient. J. Parenter. Enter. Nutr. 2016, 40, 159–211. [Google Scholar] [CrossRef]
- Zusman, O.; Kagan, I.; Bendavid, I.; Theilla, M.; Cohen, J.; Singer, P. Predictive equations versus measured energy expenditure by indirect calorimetry: A retrospective validation. Clin. Nutr. 2019, 38, 1206–1210. [Google Scholar] [CrossRef]
- Oshima, T.; Berger, M.M.; De Waele, E.; Guttormsen, A.B.; Heidegger, C.P.; Hiesmayr, M.; Singer, P.; Wernerman, J.; Pichard, C. Indirect calorimetry in nutritional therapy. A position paper by the ICALIC study group. Clin. Nutr. 2017, 36, 651–662. [Google Scholar] [CrossRef]
- Tonna, J.E.; Abrams, D.; Brodie, D.; Greenwood, J.C.; Mateo-Sidron, J.A.R.; Usman, A.; Fan, E. Management of adult patients supported with venovenous extracorporeal membrane oxygenation (VV ECMO): Guideline from the extracorporeal life support organization (ELSO). ASAIO J. 2021, 67, 601–610. [Google Scholar] [CrossRef]
- Ling, R.R.; Ramanathan, K.; Sim, J.J.L.; Wong, S.N.; Chen, Y.; Amin, F.; Fernando, S.M.; Rochwerg, B.; Fan, E.; Barbaro, R.P.; et al. Evolving outcomes of extracorporeal membrane oxygenation during the first 2 years of the COVID-19 pandemic: A systematic review and meta-analysis. Crit. Care 2022, 26, 1–13. [Google Scholar] [CrossRef]
- Lusk, G. The Elements of the Science of Nutrition; W.B. Saunders Company: Philadelphia, PA, USA, 1928. [Google Scholar]
- Weir, J.B.D.B. New methods for calculating metabolic rate with special reference to protein metabolism. J. Physiol. 1949, 109, 1–9. [Google Scholar] [CrossRef] [PubMed]
- da Rocha, E.E.M.; Alves, V.G.F.; da Fonseca, R.B.V. Indirect calorimetry: Methodology, instruments and clinical application. Curr. Opin. Clin. Nutr. Metab. Care 2006, 9, 247–256. [Google Scholar] [CrossRef] [PubMed]
- Matarese, L.E. Indirect Calorimetry: Technical Aspects. J. Am. Diet. Assoc. 1997, 97, S154–S160. [Google Scholar] [CrossRef]
- Wilmore, J.H.; Costill, D.L. Adequacy of the Haldane transformation in the computation of exercise VO2 in man. J. Appl. Physiol. 1973, 35, 85–89. [Google Scholar] [CrossRef] [PubMed]
- McLean, J.; Tobin, G. Animal and Human Calorimetry; Cambridge University Press: Cambridge, UK, 2007. [Google Scholar]
- Wilmore, D.W. The Metabolic Management of the Critically Ill; Springer: Berlin/Heidelberg, Germany, 2012. [Google Scholar]
- Archiza, B.; Welch, J.F.; Sheel, A.W. Classical experiments in whole-body metabolism: Closed-circuit respirometry. Eur. J. Appl. Physiol. 2017, 117, 1929–1937. [Google Scholar] [CrossRef]
- Petty, J.T. Charles’ Law of Gases: A Simple Experimental Demonstration. J. Chem. Educ. 1995, 72, 257. [Google Scholar] [CrossRef]
- Branson, R.D.; Johannigman, J.A. The measurement of energy expenditure. Nutr. Clin. Pract. 2004, 19, 622–636. [Google Scholar] [CrossRef] [PubMed]
- Cadena, M.; Sacristan, E.; Infante, O.; Escalante, B.; Rodriguez, F. Steady state condition in the measurement of VO2 and VCO2 by indirect calorimetry. In Proceedings of the 2005 IEEE Engineering in Medicine and Biology 27th Annual Conference, Shanghai, China, 17–18 January 2006; IEEE: Piscataway, NJ, USA, 2006; pp. 7773–7776. [Google Scholar] [CrossRef]
- Achamrah, N.; Oshima, T.; Genton, L. Innovations in energy expenditure assessment. Curr. Opin. Clin. Nutr. Metab. Care 2018, 21, 321–328. [Google Scholar] [CrossRef]
- Weissman, C.; Sardar, A.; Kemper, M. In vitro evaluation of a compact metabolic measurement instrument. J. Parenter. Enter. Nutr. 1990, 14, 216–221. [Google Scholar] [CrossRef]
- Delsoglio, M.; Dupertuis, Y.M.; Oshima, T.; van der Plas, M.; Pichard, C. Evaluation of the accuracy and precision of a new generation indirect calorimeter in canopy dilution mode. Clin. Nutr. 2020, 39, 1927–1934. [Google Scholar] [CrossRef]
- De Waele, E.; Van Zwam, K.; Mattens, S.; Staessens, K.; Diltoer, M.; Honoré, P.; Czapla, J.; Nijs, J.; La Meir, M.; Huyghens, L.; et al. Measuring resting energy expenditure during extracorporeal membrane oxygenation: Preliminary clinical experience with a proposed theoretical model. Acta Anaesthesiol. Scand. 2015, 59, 1296–1302. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.; Stewart, C.; Bailey, M.; Nieszkowska, A.; Kelly, J.; Murphy, L.; Pilcher, D.; Cooper, D.J.; Scheinkestel, C.; Pellegrino, V.; et al. Mechanical ventilation management during extracorporeal membrane oxygenation for acute respiratory distress syndrome: A retrospective international multicenter study. Crit. Care Med. 2015, 43, 654–664. [Google Scholar] [CrossRef] [PubMed]
- Wollersheim, T.; Frank, S.; Müller, M.C.; Skrypnikov, V.; Carbon, N.M.; Pickerodt, P.A.; Spies, C.; Mai, K.; Spranger, J.; Weber-Carstens, S. Measuring Energy Expenditure in extracorporeal lung support Patients (MEEP)—Protocol, feasibility and pilot trial. Clin. Nutr. 2018, 37, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Dash, R.K.; Bassingthwaighte, J.B. Erratum to: Blood HbO2 and HbCO2 Dissociation Curves at Varied O2, CO2, pH, 2,3-DPG and Temperature Levels. Ann. Biomed. Eng. 2010, 38, 1683–1701. [Google Scholar] [CrossRef] [PubMed]
- Frankenfield, D.C.; Ashcraft, C.M.; Wood, C.; Chinchilli, V.M. Validation of an indirect calorimeter using n-of-1 methodology. Clin. Nutr. 2016, 35, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Shuk, P.; Jantz, R. Oxygen gas sensing technologies: A comprehensive review. In Proceedings of the 2015 9th International Conference on Sensing Technology (ICST), Auckland, New Zealand, 8–10 December 2015; IEEE: Piscataway, NJ, USA, 2015; pp. 12–17. [Google Scholar] [CrossRef]
- Jasek, K.; Pasternak, M.; Grabka, M. Paramagnetic Sensors for the Determination of Oxygen Concentration in Gas Mixtures. ACS Sens. 2022, 7, 3228–3242. [Google Scholar] [CrossRef]
- Manning, A.C.; Keeling, R.F.; Severinghaus, J.P. Precise atmospheric oxygen measurements with a paramagnetic oxygen analyzer. Glob. Biogeochem. Cycles 1999, 13, 1107–1115. [Google Scholar] [CrossRef]
- Kovacich, R.; Martin, N.; Clift, M.; Stocks, C.; Gaskin, I.; Hobby, J. Highly accurate measurement of oxygen using a paramagnetic gas sensor. Meas. Sci. Technol. 2006, 17, 1579. [Google Scholar] [CrossRef]
- Ali, S.; Walker, J. Measurement of gas concentrations (O2, CO2, N2O and volatile agents). Anaesth. Intensive Care Med. 2014, 15, 526–529. [Google Scholar] [CrossRef]
- MerilÄinen, P.T. A differential paramagnetic sensor for breath-by-breath oximetry. J. Clin. Monit. 1990, 6, 65–73. [Google Scholar] [CrossRef]
- Meriläinen, P.T. Metabolic monitor. Int. J. Clin. Monit. Comput. 1987, 4, 167–177. [Google Scholar] [CrossRef] [PubMed]
- Conway, C.; Leigh, J.; Lindop, M.; Webb, D. An evaluation of the “rapox” rapid response paramagnetic oxygen analyser. Br. J. Anaesth. 1973, 45, 1191–1197. [Google Scholar] [CrossRef] [PubMed]
- Tsai, C.L.; Fann, C.S.; Wang, S.H.; Fung, R.F. Paramagnetic oxygen measurement using an optical-fiber microphone. Sens. Actuators B Chem. 2001, 73, 211–215. [Google Scholar] [CrossRef]
- McGrath, S.; Wendelken, S. Oxygen Analyzers. In Encyclopedia of Medical Devices and Instrumentation; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2006. [Google Scholar] [CrossRef]
- Garg, R.; Gupta, R.C. Analysis of oxygen, anaesthesia agent and flows in anaesthesia machine. Indian J. Anaesth. 2013, 57, 481. [Google Scholar] [CrossRef] [PubMed]
- Mancy, K.; Okun, D.; Reilley, C. A galvanic cell oxygen analyzer. J. Electroanal. Chem. (1959) 1962, 4, 65–92. [Google Scholar] [CrossRef]
- Roe, P.; Tyler, C.; Tennant, R.; Barnes, P. Oxygen analysers: An evaluation of five fuel cell models. Anaesthesia 1987, 42, 175–181. [Google Scholar] [CrossRef]
- Chen, R.; Formenti, F.; Obeid, A.; Hahn, C.E.; Farmery, A.D. A fibre-optic oxygen sensor for monitoring human breathing. Physiol. Meas. 2013, 34, N71. [Google Scholar] [CrossRef]
- Torda, T.; Grant, G. Test of a fuel cell oxygen analyzer. BJA Br. J. Anaesth. 1972, 44, 1108–1112. [Google Scholar] [CrossRef]
- Gurr, K. Oxygen Sensors and Their Use within Rebreathers. 2013. Available online: https://static1.squarespace.com/static/5d1f8b6514f05200011df35c/t/62ca824138a6e824689f7635/1657438789174/Oxygen+Sensors+for+use+in+rebreathers+-+release+V1.pdf (accessed on 5 April 2023).
- Sable Systems International. FC-10 Oxygen Analyzer. 2023. Available online: https://www.sablesys.com/products/classic-line/fc-10-oxygen-analyzer., (accessed on 5 April 2023).
- Cosmed. Quark RMR Indirect Calorimetry. 2022. Available online: https://www.cosmed.com/hires/QuarkRMR_Technical_Specs_A4_C03098-02-80_EN_print.pdf (accessed on 5 April 2023).
- Parvomedics. Parvo Medics TrueOne 2400. 2013. Available online: https://www.parvo.com/trueone-2400/ (accessed on 5 April 2023).
- AEI Technologies. MAX-II and MAX-IIa Metabolic Cart. 2022. Available online: https://aeitechnologies.com/max-ii-max-iia-metabolic-systems/ (accessed on 5 April 2023).
- Cosmed. Q-NRG Metabolic Monitor Technical Specifications. 2022. Available online: https://www.cosmed.com/hires/Q-NRG_Technical_Specs_A4_C04672-02-80_EN_print.pdf (accessed on 5 April 2023).
- Cosmed. Q-NRG+ Metabolic Monitor Technical Specifications. 2022. Available online: https://www.cosmed.com/hires/Q-NRG+_Technical_Specs_A4_C04672-22-80_EN_print.pdf (accessed on 5 April 2023).
- MGC Diagnostics. Ultima CPX Metabolic Stress Testing System. 2020. Available online: https://mgcdiagnostics.com/images/uploads/documents/Ultima_CPX_sellsheet_060155-001.pdf (accessed on 5 April 2023).
- Graf, S.; Karsegard, V.L.; Viatte, V.; Heidegger, C.P.; Fleury, Y.; Pichard, C.; Genton, L. Evaluation of three indirect calorimetry devices in mechanically ventilated patients: Which device compares best with the Deltatrac II: A prospective observational study. Clin. Nutr. 2015, 34, 60–65. [Google Scholar] [CrossRef]
- Dupertuis, Y.M.; Delsoglio, M.; Hamilton-James, K.; Berger, M.M.; Pichard, C.; Collet, T.H.; Genton, L. Clinical Evaluation of the New Indirect Calorimeter in Canopy and Face Mask Mode for Energy Expenditure Measurement in Spontaneously Breathing Patients. Clin. Nutr. 2022, 41, 1591–1599. [Google Scholar] [CrossRef]
- Dinh, T.V.; Choi, I.Y.; Son, Y.S.; Kim, J.C. A review on non-dispersive infrared gas sensors: Improvement of sensor detection limit and interference correction. Sens. Actuators B Chem. 2016, 231, 529–538. [Google Scholar] [CrossRef]
- Swinehart, D.F. The beer-lambert law. J. Chem. Educ. 1962, 39, 333. [Google Scholar] [CrossRef]
- Fei, J.; Zhu, Z.; Pavlidis, I. Imaging breathing rate in the co 2 absorption band. In Proceedings of the 2005 IEEE Engineering in Medicine and Biology 27th Annual Conference, Shanghai, China, 17–18 January 2006; IEEE: Piscataway, NJ, USA, 2006; pp. 700–705. [Google Scholar] [CrossRef]
- Jia, X.; Roels, J.; Baets, R.; Roelkens, G. On-chip non-dispersive infrared CO2 sensor based on an integrating cylinder. Sensors 2019, 19, 4260. [Google Scholar] [CrossRef] [PubMed]
- GSS Gas Sensing Solutions, SprintIR-6S Datasheet. High-Speed CO2 Sensor. 2020. Available online: https://www.gassensing.co.uk/file-dnld-link/SprintIR-6S%20Data%20Sheet%20Rev%204.12_1.pdf (accessed on 5 April 2023).
- Vasilchenko, D.; Popov, Y.B.; Bodnar, V.; Khubiev, R.K. Analysis of methods and equipment for inhaled/exhaled airflow rate measurement. IOP Conf. Ser. Mater. Sci. Eng. 2020, 1001, 012079. [Google Scholar] [CrossRef]
- Baker, R.C. Flow Measurement Handbook; Cambridge University Press: Cambridge, UK, 2000; Volume 99. [Google Scholar]
- Sharma, J.; Singh, J. Design and development of miniature turbine based flow sensing device for respiratory flow diagnosis. Int. J. Sci. Res. 2014, 3, 754–758. [Google Scholar]
- Du, Y.; Guo, Y. Theoretical and experimental study on wide range optical fiber turbine flow sensor. Sensors 2016, 16, 1095. [Google Scholar] [CrossRef]
- Cascetta, F.; Rotondo, G. Effects of intermittent flows on turbine gas meters accuracy. Measurement 2015, 69, 280–286. [Google Scholar] [CrossRef]
- Sutera, S.P.; Skalak, R. The history of Poiseuille’s law. Annu. Rev. Fluid Mech. 1993, 25, 1–20. [Google Scholar] [CrossRef]
- Jewitt, H.; Thomas, G. Measurement of flow and volume of gases. Anaesth. Intensive Care Med. 2012, 13, 106–110. [Google Scholar] [CrossRef]
- Lilly, J.C. Flow meter for recording respiratory flow of human subjects. Methods Med. Res. 1950, 2, 113–121. [Google Scholar]
- Sivieri, E.M.; Dysart, K.; Abbasi, S. Evaluation of pulmonary function in the neonate. In Fetal and Neonatal Physiology; Elsevier: Amsterdam, The Netherlands, 2017; pp. 754–765. [Google Scholar]
- Huang, Y.; Young, M.S.; Tai, C. Noninvasive respiratory monitoring system based on the piezoceramic transducer’s pyroelectric effect. Rev. Sci. Instrum. 2008, 79, 035103. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.D.; Plyley, M.; Thomas, S.; Goodman, L.; Duffin, J. Effects of concurrent inspiratory and expiratory muscle training on respiratory and exercise performance in competitive swimmers. Eur. J. Appl. Physiol. 2005, 94, 527–540. [Google Scholar] [CrossRef] [PubMed]
- Schena, E.; Lupi, G.; Cecchini, S.; Silvestri, S. Linearity dependence on oxygen fraction and gas temperature of a novel Fleisch pneumotachograph for neonatal ventilation at low flow rates. Measurement 2012, 45, 2064–2071. [Google Scholar] [CrossRef]
- Lang, S.; Herold, R.; Kraft, A.; Harth, V.; Preisser, A.M. Spiroergometric measurements under increased inspiratory oxygen concentration (FIO2)—Putting the Haldane transformation to the test. PLoS ONE 2018, 13, e0207648. [Google Scholar] [CrossRef] [PubMed]
- Svensson, K.; Sonander, H.; Stenqvist, O. Validation of a system for measurement of metabolic gas exchange during anaesthesia with controlled ventilation in an oxygen consuming lung model. Br. J. Anaesth. 1990, 64, 311–319. [Google Scholar] [CrossRef]
- Oshima, T.; Dupertuis, Y.M.; Delsoglio, M.; Graf, S.; Heidegger, C.P.; Pichard, C. In vitro validation of indirect calorimetry device developed for the ICALIC project against mass spectrometry. Clin. Nutr. ESPEN 2019, 32, 50–55. [Google Scholar] [CrossRef]
- Kim, D.y.; Robergs, R.A. Validation of a new mixing chamber system for breath-by-breath indirect calorimetry. Appl. Physiol. Nutr. Metab. 2012, 37, 157–166. [Google Scholar] [CrossRef]
- Campbell, R.S.; Branson, R.D.; Burke, W.C.; Covington, J. Metabolic Measurement Using Indirect Calorimetry During Mechanical Ventilation. Int. Anesthesiol. Clin. 1996, 34, 111–120. [Google Scholar] [CrossRef]
- Mehta, N.M.; Bechard, L.J.; Leavitt, K.; Duggan, C. Severe weight loss and hypermetabolic paroxysmal dysautonomia following hypoxic ischemic brain injury: The role of indirect calorimetry in the intensive care unit. J. Parenter. Enter. Nutr. 2008, 32, 281–284. [Google Scholar] [CrossRef]
- Vasileiou, G.; Mulder, M.B.; Qian, S.; Iyengar, R.; Gass, L.M.; Parks, J.; Lineen, E.; Byers, P.; Yeh, D.D. Continuous indirect calorimetry in critically injured patients reveals significant daily variability and delayed, sustained hypermetabolism. J. Parenter. Enter. Nutr. 2020, 44, 889–894. [Google Scholar] [CrossRef]
- Mtaweh, H.; Tuira, L.; Floh, A.A.; Parshuram, C.S. Indirect calorimetry: History, technology, and application. Front. Pediatr. 2018, 6, 257. [Google Scholar] [CrossRef]
- Irwin, R.S.; Rippe, J.M. Manual of Intensive Care Medicine; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2010. [Google Scholar]
- Beaver, W.L.; Wasserman, K.; Whipp, B.J. On-line computer analysis and breath-by-breath graphical display of exercise function tests. J. Appl. Physiol. 1973, 34, 128–132. [Google Scholar] [CrossRef] [PubMed]
- Stapel, S.N.; Weijs, P.J.; Girbes, A.R.; Oudemans-van Straaten, H.M. Indirect calorimetry in critically ill mechanically ventilated patients: Comparison of E-sCOVX with the deltatrac. Clin. Nutr. 2019, 38, 2155–2160. [Google Scholar] [CrossRef] [PubMed]
- Hughson, R.; Northey, D.; Xing, H.; Dietrich, B.; Cochrane, J. Alignment of ventilation and gas fraction for breath-by-breath respiratory gas exchange calculations in exercise. Comput. Biomed. Res. 1991, 24, 118–128. [Google Scholar] [CrossRef] [PubMed]
- Noguchi, H.; Ogushi, Y.; Yoshiya, I.; Itakura, N.; Yamabayashi, H. Breath-by-breath VCO2 and VO2 required compensation for transport delay and dynamic response. J. Appl. Physiol. 1982, 52, 79–84. [Google Scholar] [CrossRef]
- Bernard, T.E. Aspects of on-line digital integration of pulmonary gas transfer. J. Appl. Physiol. 1977, 43, 375–378. [Google Scholar] [CrossRef]
- Roecker, K.; Prettin, S.; Sorichter, S. Gas exchange measurements with high temporal resolution: The breath-by-breath approach. Int. J. Sport Med. 2005, 26, S11–S18. [Google Scholar] [CrossRef]
- Beijst, C.; Schep, G.; Breda, E.V.; Wijn, P.F.; Pul, C.V. Accuracy and precision of CPET equipment: A comparison of breath-by-breath and mixing chamber systems. J. Med. Eng. Technol. 2013, 37, 35–42. [Google Scholar] [CrossRef]
- Broman, L.M.; Malfertheiner, M.V.; Montisci, A.; Pappalardo, F. Weaning from veno-venous extracorporeal membrane oxygenation: How I do it. J. Thorac. Dis. 2018, 10, S692. [Google Scholar] [CrossRef]
- Singer, P.; Pichard, C.; De Waele, E. Practical guidance for the use of indirect calorimetry during COVID 19 pandemic. Clin. Nutr. Exp. 2020, 33, 18–23. [Google Scholar] [CrossRef]
- Meyer, J.U.; Kullik, G.; Wruck, N.; Kück, K.; Manigel, J. Advanced technologies and devices for inhalational anesthetic drug dosing. Mod. Anesth. 2008, 182, 451–470. [Google Scholar] [CrossRef]
- Goswami, A.; Cooper, R. Measurement of gases (O2, CO2, N2, N2O and volatile agents). Anaesth. Intensive Care Med. 2011, 12, 568–573. [Google Scholar] [CrossRef]
- Sundström, M.; Tjäder, I.; Rooyackers, O.; Wernerman, J. Indirect calorimetry in mechanically ventilated patients. A systematic comparison of three instruments. Clin. Nutr. 2013, 32, 118–121. [Google Scholar] [CrossRef] [PubMed]
- Ye, X.; LeVan, M.D. Water transport properties of Nafion membranes: Part I. Single-tube membrane module for air drying. J. Membr. Sci. 2003, 221, 147–161. [Google Scholar] [CrossRef]
- Cobianu, C.; Serban, B.; Avramescu, V.; Hobbs, B.; Pratt, K.; Willett, M. Lead-free galvanic oxygen sensors—A conceptual approach. In Proceedings of the CAS 2012 (International Semiconductor Conference), Sinaia, Romania, 15–17 October 2012; IEEE: Piscataway, NJ, USA, 2012; Volume 1, pp. 161–164. [Google Scholar] [CrossRef]
- Warburton, P.R.; Sawtelle, R.S.; Watson, A.; Wang, A.Q. Failure prediction for a galvanic oxygen sensor. Sens. Actuators B Chem. 2001, 72, 197–203. [Google Scholar] [CrossRef]
- Singh, S.P.; Hote, M.P. Ventilatory management of patients on ECMO. Indian J. Thorac. Cardiovasc. Surg. 2021, 37, 248–253. [Google Scholar] [CrossRef]
- Sable Systems International. PA-10 Paramagnetic Oxygen Analyzer. 2019. Available online: https://www.sablesys.com/products/classic-line/pa-10-paramagnetic-oxygen-analyzer/ (accessed on 5 April 2023).
- Tipparaju, V.V.; Mora, S.J.; Yu, J.; Tsow, F.; Xian, X. Wearable transcutaneous CO2 monitor based on miniaturized nondispersive infrared sensor. IEEE Sens. J. 2021, 21, 17327–17334. [Google Scholar] [CrossRef]
- GSS Gas Sensing Solutions, SprintIR-R datasheet. Very High-Speed CO2 Sensor. 2021. Available online: https://www.gassensing.co.uk/file-dnld-link/SprintIR-R%20Data%20Sheet%20Rev%204.12_3.pdf (accessed on 5 April 2023).
- Vincent, T.A.; Gardner, J. A low cost MEMS based NDIR system for the monitoring of carbon dioxide in breath analysis at ppm levels. Sens. Actuators B Chem. 2016, 236, 954–964. [Google Scholar] [CrossRef]
- SST Sensing, ExplorIR-M Datasheet. Small Footprint Low Power CO2 Sensor. 2020. Available online: https://sstsensing.com/wp-content/uploads/2020/08/DS0179rev1_ExplorIR-M.pdf) (accessed on 5 April 2023).
- Fleming, L.; Gibson, D.; Song, S.; Li, C.; Reid, S. Reducing N2O induced cross-talk in a NDIR CO2 gas sensor for breath analysis using multilayer thin film optical interference coatings. Surf. Coat. Technol. 2018, 336, 9–16. [Google Scholar] [CrossRef]
- Turney, S.; Blumenfeld, W. Heated Fleisch pneumotachometer: A calibration procedure. J. Appl. Physiol. 1973, 34, 117–121. [Google Scholar] [CrossRef]
- Yeh, M.; Adams, T.; Gardner, R.; Yanowitz, F. Effect of O2, N2, and CO2 composition on nonlinearity of Fleisch pneumotachograph characteristics. J. Appl. Physiol. 1984, 56, 1423–1425. [Google Scholar] [CrossRef] [PubMed]
- Turner, M.; MacLeod, I.; Rothberg, A. Calibration of Fleisch and screen pneumotachographs for use with various oxygen concentrations. Med. Biol. Eng. Comput. 1990, 28, 200–204. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.; Turner, M.J.; Yem, J.S.; Baker, A.B. Calibration of pneumotachographs using a calibrated syringe. J. Appl. Physiol. 2003, 95, 571–576. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; Van Der Grinten, C.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef]
- Yeh, M.P.; Gardner, R.M.; Adams, T.D.; Yanowitz, F.G. Computerized determination of pneumotachometer characteristics using a calibrated syringe. J. Appl. Physiol. 1982, 53, 280–285. [Google Scholar] [CrossRef]
- Biselli, P.J.C.; Nóbrega, R.S.; Soriano, F.G. Nonlinear flow sensor calibration with an accurate syringe. Sensors 2018, 18, 2163. [Google Scholar] [CrossRef]
- Achamrah, N.; Delsoglio, M.; De Waele, E.; Berger, M.M.; Pichard, C. Indirect calorimetry: The 6 main issues. Clin. Nutr. 2021, 40, 4–14. [Google Scholar] [CrossRef]
- Yeh, M.P.; Adams, T.D.; Gardner, R.M.; Yanowitz, F.G. Turbine flowmeter vs. Fleisch pneumotachometer: A comparative study for exercise testing. J. Appl. Physiol. 1987, 63, 1289–1295. [Google Scholar] [CrossRef]
- Bridgeman, D.; Tsow, F.; Xian, X.; Forzani, E. A new differential pressure flow meter for measurement of human breath flow: Simulation and experimental investigation. AIChE J. 2016, 62, 956–964. [Google Scholar] [CrossRef]
- García-Río, F.; Calle, M.; Burgos, F.; Casan, P.; Del Campo, F.; Galdiz, J.B.; Giner, J.; González-Mangado, N.; Ortega, F.; Maestu, L.P. Spirometry. Arch. Bronconeumol. 2013, 49, 388–401. [Google Scholar] [CrossRef]
- Singer, P.; Anbar, R.; Cohen, J.; Shapiro, H.; Shalita-Chesner, M.; Lev, S.; Grozovski, E.; Theilla, M.; Frishman, S.; Madar, Z. The tight calorie control study (TICACOS): A prospective, randomized, controlled pilot study of nutritional support in critically ill patients. Intensive Care Med. 2011, 37, 601–609. [Google Scholar] [CrossRef] [PubMed]











| Name | Manufacturer | Type | Range | Response Time (T90) | Accuracy | Resolution | Reference | |
|---|---|---|---|---|---|---|---|---|
| % | ms | %vol | % | %vol | ||||
| Quark RMR | Cosmed | Paramagnetic | 0–100 | 120 | ±0.05 | ±0.3 | N.R. * | [47] |
| TrueOne2400 | Parvo Medics | Paramagnetic | 0–100 | 200 | N.R. | ±0.1 | N.R. | [48] |
| Max-II and Max-IIa | AEI Technologies | Paramagnetic | 0–100 | N.R. | ±0.03 | N.R. | ±0.01 | [49] |
| Q-NRG and Q-NRG+ | Cosmed | Galvanic Fuel Cell | 0–75 | N.R. | <±0.05 | ±0.3 | ±0.01 | [50,51] |
| Ultima CPX | MGC Diagnostics | Galvanic Fuel Cell | 0–100 | <180 | N.R. | ±1 | N.R. | [52] |
| Name | Manufacturer | Range | Response Time (T90) | Accuracy | Resolution | Reference | |
|---|---|---|---|---|---|---|---|
| % | ms | %vol | % | %vol | |||
| Quark RMR | Cosmed | 0–10 | 100 | ±0.05 | ±1 | N.R. * | [47] |
| TrueOne2400 | Parvo Medics | 0–15 | 100 | N.R. | ±0.1 (for 0–10% ) | N.R. | [48] |
| Max-II and Max-IIa | AEI Technologies | 0–10 | N.R. | ±0.03 | N.R. | ±0.01 | [49] |
| Q-NRG and Q-NRG+ | Cosmed | 0–10 | N.R. | ±0.05 | ±1 | ±0.01 | [50,51] |
| Ultima CPX | MGC Diagnostics | 0–15 | <180 | N.R. | ±1 (for 0–10% ) | N.R. | [52] |
| Name | Manufacturer | Type | Range | Accuracy | Reference | |
|---|---|---|---|---|---|---|
| L/min | % | mL/s | ||||
| Quark RMR | Cosmed | Pneumotachometer | 0–960 | ±2 | ±20 | [47] |
| Turbine | 0–360 | ±2 | ±20 | |||
| TrueOne2400 | Parvo Medics | Pneumotachometer | 0–800 | ±2 | N.R. * | [48] |
| Max-II and Max-IIa | AEI Technologies | Pneumotachometer | 0–800 | <±1 | N.R. | [49] |
| Q-NRG | Cosmed | Turbine | 0–360 | ±2 | ±20 | [50] |
| Q-NRG+ | Cosmed | Pneumotachometer | 0–960 | ±2 | ±20 | [51] |
| Turbine | 0–360 | ±2 | ±20 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Priem, S.; Jonckheer, J.; De Waele, E.; Stiens, J. Indirect Calorimetry in Spontaneously Breathing, Mechanically Ventilated and Extracorporeally Oxygenated Patients: An Engineering Review. Sensors 2023, 23, 4143. https://0-doi-org.brum.beds.ac.uk/10.3390/s23084143
Priem S, Jonckheer J, De Waele E, Stiens J. Indirect Calorimetry in Spontaneously Breathing, Mechanically Ventilated and Extracorporeally Oxygenated Patients: An Engineering Review. Sensors. 2023; 23(8):4143. https://0-doi-org.brum.beds.ac.uk/10.3390/s23084143
Chicago/Turabian StylePriem, Sebastiaan, Joop Jonckheer, Elisabeth De Waele, and Johan Stiens. 2023. "Indirect Calorimetry in Spontaneously Breathing, Mechanically Ventilated and Extracorporeally Oxygenated Patients: An Engineering Review" Sensors 23, no. 8: 4143. https://0-doi-org.brum.beds.ac.uk/10.3390/s23084143