Oral Eplerenone Versus Observation in the Management of Acute Central Serous Chorioretinopathy: A Prospective, Randomized Comparative Study

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Visual Acuity Changes during the Follow-Up Visits
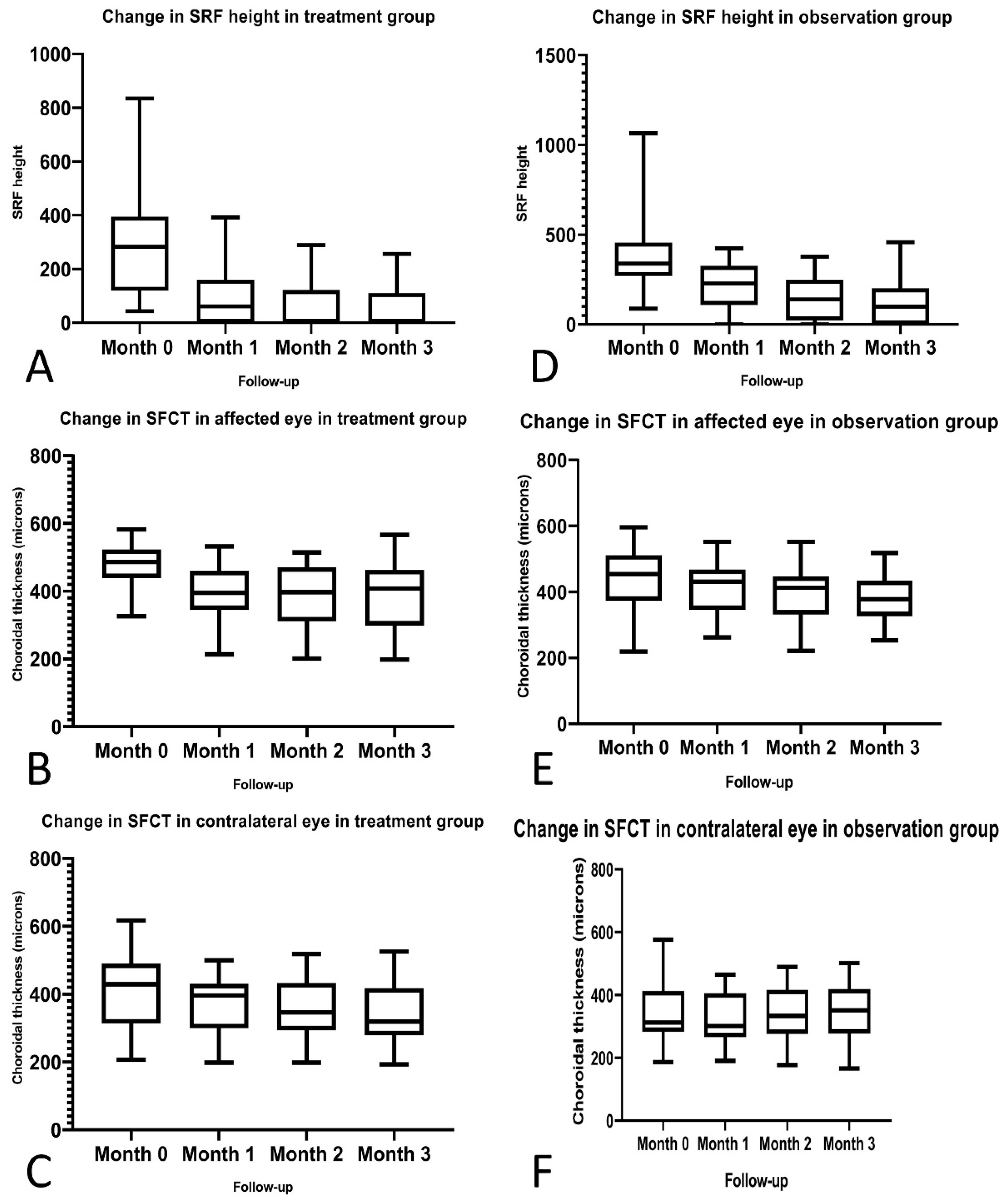
2.2. Efficacy of Eplerenone on the SRF Height in the Study Eye
2.3. Efficacy of Eplerenone on SRF Height and SFCT on Study Eye
2.4. Effect of Eplerenone on SFCT of the Fellow Eye
2.5. Safety
3. Discussion
4. Materials and Methods
4.1. Inclusion and Exclusion Criteria
4.2. Examination and Measurements
4.3. Follow-Up Visits
4.4. Outcome Measures
- Comparisons between the treatment group and observational group for the SRF height and SFCT in the study eye at every visit for the consecutive 3 months.
- SFCT measurement comparison between the treatment and the observation groups in the fellow eye at each visit.
- Side effects and drug tolerance at each visit.
4.5. Statistical TESTS
4.6. Declarations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| CSCR | central serous chorioretinopathy |
| SRF | subretinal fluid |
| OCT | optical coherence tomography |
| RPE | retinal pigment epithelium |
| SFCT | subfoveal choroidal thickness |
References
- Wang, M.; Munch, I.C.; Hasler, P.W.; Prünte, C.; Larsen, M. Central serous chorioretinopathy. Acta Ophthalmol. 2008, 86, 126–145. [Google Scholar] [CrossRef] [PubMed]
- Imamura, Y.; Fujiwara, T.; Spaide, R.F. Fundus autofluorescence and visual acuity in central serous chorioretinopathy. Ophthalmology 2011, 118, 700–705. [Google Scholar] [CrossRef] [PubMed]
- Liew, G.; Quin, G.; Gillies, M.; Fraser-Bell, S. Central serous chorioretinopathy: A review of epidemiology and pathophysiology: Central serous chorioretinopathy. Clin Exp. Ophthalmol. 2013, 41, 201–214. [Google Scholar] [CrossRef] [PubMed]
- Loo, R.H.; Scott, I.U.; Flynn, H.W.; Gass, J.D.M.; Murray, T.G.; Lewis, M.L.; Rosenfeld, P.J.; Smiddy, W.E. Factors associated with reduced visual acuity during long-term follow-up of patients with idiopathic central serous chorioretinopathy. Retina (Philadelphia, Pa.) 2002, 22, 19–24. [Google Scholar] [CrossRef]
- Baran, N.V.; Gürlü, V.P.; Esgin, H. Long-term macular function in eyes with central serous chorioretinopathy. Clin. Exp. Ophthalmol. 2005, 33, 369–372. [Google Scholar] [CrossRef] [PubMed]
- Spaide, R.F.; Hall, L.; Haas, A.; Campeas, L.; Yannuzzi, L.A.; Fisher, Y.L.; Guyer, D.R.; Slakter, J.S.; Sorenson, J.A.; Orlock, D.A. Indocyanine green videoangiography of older patients with central serous chorioretinopathy. Retina (Philadelphia, Pa.) 1996, 16, 203–213. [Google Scholar] [CrossRef]
- Iida, T.; Kishi, S.; Hagimura, N.; Shimizu, K. Persistent and bilateral choroidal vascular abnormalities in central serous chorioretinopathy. Retina (Philadelphia, Pa.) 1999, 19, 508–512. [Google Scholar] [CrossRef]
- Hanumunthadu, D.; van Dijk, E.H.C.; Dumpala, S.; Rajesh, B.; Jabeen, A.; Jabeen, A.; Ansari, M.; Mehta, P.; Shah, S.; Sarvaiya, C.; et al. Evaluation of Choroidal Layer Thickness in Central Serous Chorioretinopathy. J. Ophthalmic Vis. Res. 2019, 14, 164–170. [Google Scholar] [CrossRef]
- Maruko, I.; Iida, T.; Sugano, Y.; Ojima, A.; Sekiryu, T. Subfoveal choroidal thickness in fellow eyes of patients with central serous chorioretinopathy. Retina (Philadelphia, Pa.) 2011, 31, 1603–1608. [Google Scholar] [CrossRef]
- Araki, T.; Ishikawa, H.; Iwahashi, C.; Niki, M.; Mitamura, Y.; Sugimoto, M.; Kondo, M.; Kinoshita, T.; Nishi, T.; Ueda, T.; et al. Central serous chorioretinopathy with and without steroids: A multicenter survey. PLoS ONE 2019, 14, e0213110. [Google Scholar] [CrossRef] [Green Version]
- Karadimas, P.; Bouzas, E.A. Glucocorticoid use represents a risk factor for central serous chorioretinopathy: A prospective, case-control study. Graefes Arch. Clin. Exp. Ophthalmol. 2004, 242, 800–802. [Google Scholar] [CrossRef]
- Yang, D.; Eliott, D. Systemic Mineralocorticoid Antagonists in the Treatment of Central Serous Chorioretinopathy. Semin. Ophthalmol. 2017, 32, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, B.P.; Atchison, E.; Idris, A.A.; Bakri, S.J. Central serous chorioretinopathy and glucocorticoids: An update on evidence for association. Surv. Ophthalmol. 2018, 63, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.; Célérier, I.; Bousquet, E.; Jeanny, J.-C.; Jonet, L.; Savoldelli, M.; Offret, O.; Curan, A.; Farman, N.; Jaisser, F.; et al. Mineralocorticoid receptor is involved in rat and human ocular chorioretinopathy. J. Clin. Investig. 2012, 122, 2672–2679. [Google Scholar] [CrossRef] [PubMed]
- Craft, J. Eplerenone (Inspra), a new aldosterone antagonist for the treatment of systemic hypertension and heart failure. Proc. (Bayl. Univ. Med. Cent.) 2004, 17, 217–220. [Google Scholar] [CrossRef] [Green Version]
- Struthers, A.; Krum, H.; Williams, G.H. A comparison of the aldosterone-blocking agents eplerenone and spironolactone. Clin. Cardiol. 2008, 31, 153–158. [Google Scholar] [CrossRef]
- Karagiannis, A.; Athyros, V.G.; Mikhailidis, D.P. A comparison of the aldosterone-blocking agents eplerenone and spironolactone. Clin. Cardiol. 2009, 32, 230. [Google Scholar] [CrossRef]
- Falavarjani, K.G.; Amirsardari, A.; Habibi, A.; Eshaghi, A.; Bakhti, S.; Aghdam, K.A. Visual and Anatomical Outcomes of Spironolactone Therapy in Patients with Chronic Central Serous Chorioretinopathy. J. Ophthalmic Vis. Res. 2017, 12, 281–289. [Google Scholar] [CrossRef]
- Rahimy, E.; Pitcher, J.D.; Hsu, J.; Adam, M.K.; Shahlaee, A.; Samara, W.A.; Vander, J.F.; Kaiser, R.S.; Chiang, A.; Spirn, M.J.; et al. A Randomized Double-Blind Placebo-Control Pilot Study of Eplerenone for The Treatment of Central Serous Chorioretinopathy (Ecselsior). Retina (Philadelphia, Pa.) 2018, 38, 962–969. [Google Scholar] [CrossRef]
- Lotery, A.; Sivaprasad, S.; O’Connell, A.; Harris, R.A.; Culliford, L.; Ellis, L.; Cree, A.; Madhusudhan, S.; Behar-Cohen, F.; Chakravarthy, U.; et al. Eplerenone for chronic central serous chorioretinopathy in patients with active, previously untreated disease for more than 4 months (VICI): A randomised, double-blind, placebo-controlled trial. Lancet 2020, 395, 294–303. [Google Scholar] [CrossRef]
- Sun, X.; Shuai, Y.; Fang, W.; Li, J.; Ge, W.; Yuan, S.; Liu, Q. Spironolactone versus observation in the treatment of acute central serous chorioretinopathy. Br. J. Ophthalmol. 2018, 102, 1060–1065. [Google Scholar] [CrossRef] [PubMed]
- Zucchiatti, I.; Sacconi, R.; Parravano, M.C.; Costanzo, E.; Querques, L.; Montorio, D.; Bandello, F.; Querques, G. Eplerenone Versus Observation in the Treatment of Acute Central Serous Chorioretinopathy: A Retrospective Controlled Study. Ophthalmol. Ther. 2018, 7, 109–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brandl, C.; Helbig, H.; Gamulescu, M.A. Choroidal thickness measurements during central serous chorioretinopathy treatment. Int. Ophthalmol. 2014, 34, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Matsunaga, H.; Nangoh, K.; Uyama, M.; Nanbu, H.; Fujiseki, Y.; Takahashi, K. Occurrence of choroidal neovascularization following photocoagulation treatment for central serous retinopathy. Nippon Ganka Gakkai Zasshi 1995, 99, 460–468. [Google Scholar]
- Chan, W.-M.; Lai, T.Y.Y.; Lai, R.Y.K.; Liu, D.T.L.; Lam, D.S.C. Half-dose verteporfin photodynamic therapy for acute central serous chorioretinopathy: One-year results of a randomized controlled trial. Ophthalmology 2008, 115, 1756–1765. [Google Scholar] [CrossRef]
- Reibaldi, M.; Cardascia, N.; Longo, A.; Furino, C.; Avitabile, T.; Faro, S.; Sanfilippo, M.; Russo, A.; Uva, M.G.; Munno, F.; et al. Standard-fluence versus low-fluence photodynamic therapy in chronic central serous chorioretinopathy: A nonrandomized clinical trial. Am. J. Ophthalmol. 2010, 149, 307–315.e2. [Google Scholar] [CrossRef]
- Lu, H.Q.; Wang, E.Q.; Zhang, T.; Chen, Y.X. Photodynamic therapy and anti-vascular endothelial growth factor for acute central serous chorioretinopathy: A systematic review and meta-analysis. Eye 2016, 30, 15–22. [Google Scholar] [CrossRef] [Green Version]
- Ji, S.; Wei, Y.; Chen, J.; Tang, S. Clinical efficacy of anti-VEGF medications for central serous chorioretinopathy: A meta-analysis. Int. J. Clin. Pharm. 2017, 39, 514–521. [Google Scholar] [CrossRef]
- Maleki, A.; Nezamdust, Z.; Salari, A.; Ahmadi, S.S.; Sabbaghi, H.; Bagherzadeh, O.; Ataollahi, A.; Yaseri, M. The Effect of Intravitreal Bevacizumab on Central Serous Chorioretinopathy. Med. Hypothesis Discov. Innov. Ophthalmol. 2018, 7, 176–182. [Google Scholar]
- Ünlü, C.; Erdogan, G.; Aydogan, T.; Sezgin Akcay, B.I.; Kardes, E.; Kiray, G.A.; Bozkurt, T.K. Intravitreal Bevacizumab for Treatment of Central Serous Chorioretinopathy. J. Ophthalmic Vis. Res. 2016, 11, 61–65. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Treatment Group (N = 29) | Observation Group (N = 29) | p Value |
|---|---|---|---|
| Age (years) | 40.4 ± 7.1 | 43.3 ± 8.34 | 0.24 |
| Sex (M:F) | 23:6 | 25:4 | 0.73 |
| Laterality (RE:LE) | 18:11 | 17:12 | >0.999 |
| Mean duration of symptoms (weeks) | 6.46 ± 1.45 | 5.87 ± 2.09 | 0.897 |
| Visual acuity at presentation (N, %) | 6/6–6/12—17,57 6/18–6/36—11,38 ≤6/60—1,3 | 6/6–6/12—20,69 6/18–6/36—9,31 ≤6/60—0,0 | |
| SRF height (µm) at baseline | 307 ± 234 | 381 ± 227 | 0.146 |
| SFCT study eye (µm) at baseline | 479 ± 58.6 | 443 ± 97.8 | 0.144 |
| SFCT contralateral eye (µm) at baseline | 406 ± 106 | 340 ± 92.3 | 0.060 |
| Eyes with complete SRF resolution at month 1 | 13/29 (45%) | 3/29 (10%) | 0.007 |
| Eyes with complete SRF resolution at month 2 | 16/29 (55%) | 6/29 (21%) | 0.014 |
| Eyes with complete SRF resolution at month 3 | 18/29 (62%) | 9/29 (31%) | 0.034 |
| Improvement in visual acuity to 6/6 at month 1 | 27/29 (92%) | 21/29 (74%) | 0.079 |
| Improvement in visual acuity to 6/6 at month 2 | 29/29 (100%) | 25/29 (86%) | 0.112 |
| Improvement in visual acuity to 6/6 at month 3 | 29/29 (100%) | 29/29 (100%) | >0.999 |
| Variable | Group | Baseline | Month 1 | p Value (Wilcoxon) | Month 2 | p Value (Wilcoxon) | Month 3 | p Value (Wilcoxon) | p Value ANOVA |
|---|---|---|---|---|---|---|---|---|---|
| SRF (µm) | Treatment | 307 ± 234 | 87.9 ± 101 | <0.000 | 64.4 ± 87.6 | <0.000 | 61.7 ± 84.8 | <0.000 | <0.000 |
| Observation | 381 ± 227 | 217 ± 128 | <0.000 | 147 ± 121 | <0.000 | 116 ± 115 | <0.000 | <0.000 | |
| SFCT study eye (µm) | Treatment | 479 ± 58.6 | 395 ± 75.6 | <0.000 | 387 ± 82.6 | <0.000 | 385 ± 97.7 | <0.000 | <0.000 |
| Observation | 443 ± 97.8 | 407 ± 78.3 | 0.032 | 390 ± 78.5 | 0.003 | 378 ± 74 | 0.000 | 0.001 | |
| SFCT contralateral eye (µm) | Treatment | 406 ± 106 | 372 ± 80.7 | 0.025 | 354 ± 83.4 | 0.004 | 340 ± 90.9 | 0.004 | 0.005 |
| Observation | 340 ± 92.3 | 321 ± 80.4 | 0.007 | 336 ± 85.3 | 0.402 | 343 ± 87.8 | 0.987 | 0.276 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Venkatesh, R.; Pereira, A.; Jayadev, C.; Prabhu, V.; Aseem, A.; Jain, K.; Bavaharan, B.; Yadav, N.K.; Chhablani, J. Oral Eplerenone Versus Observation in the Management of Acute Central Serous Chorioretinopathy: A Prospective, Randomized Comparative Study. Pharmaceuticals 2020, 13, 170. https://0-doi-org.brum.beds.ac.uk/10.3390/ph13080170
Venkatesh R, Pereira A, Jayadev C, Prabhu V, Aseem A, Jain K, Bavaharan B, Yadav NK, Chhablani J. Oral Eplerenone Versus Observation in the Management of Acute Central Serous Chorioretinopathy: A Prospective, Randomized Comparative Study. Pharmaceuticals. 2020; 13(8):170. https://0-doi-org.brum.beds.ac.uk/10.3390/ph13080170
Chicago/Turabian StyleVenkatesh, Ramesh, Arpitha Pereira, Chaitra Jayadev, Vishma Prabhu, Aditya Aseem, Kushagra Jain, Bharathi Bavaharan, Naresh Kumar Yadav, and Jay Chhablani. 2020. "Oral Eplerenone Versus Observation in the Management of Acute Central Serous Chorioretinopathy: A Prospective, Randomized Comparative Study" Pharmaceuticals 13, no. 8: 170. https://0-doi-org.brum.beds.ac.uk/10.3390/ph13080170