
Cannabis-Based Oral Formulations for Medical Purposes: Preparation, Quality and Stability

 , , , and
, , , and
Abstract
:1. Introduction
2. Results
2.1. Capsules Preparation
2.2. Capsules’ Quality
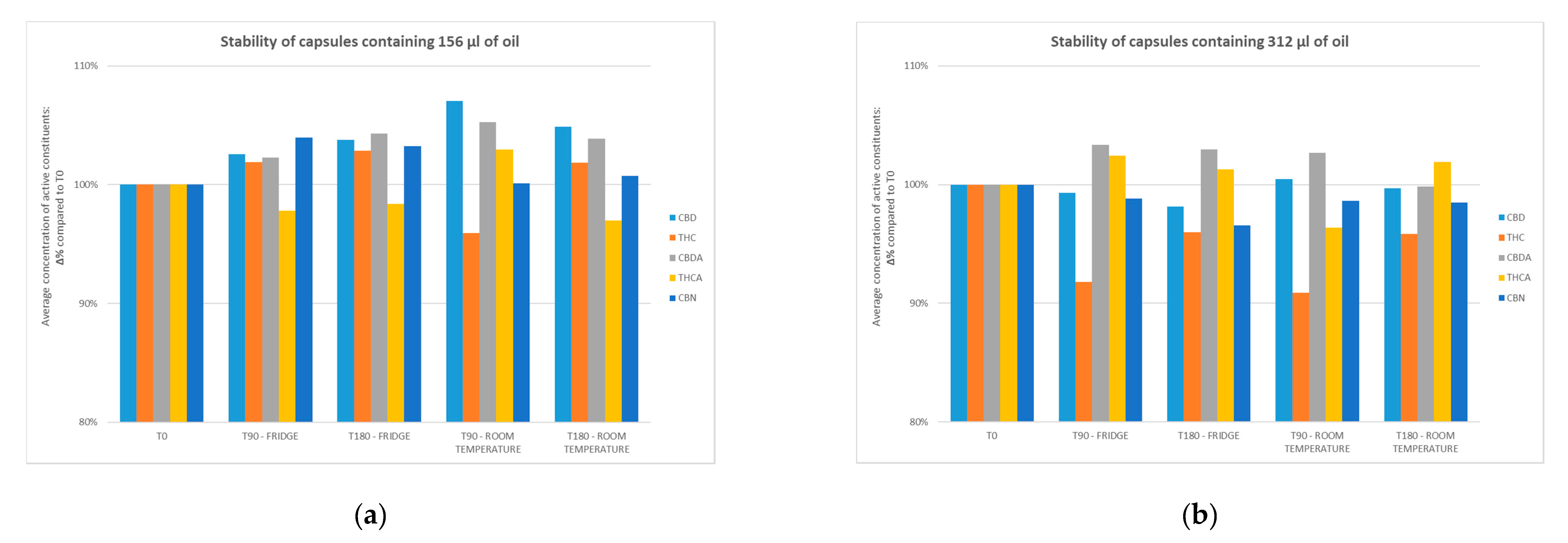
2.3. Stability Tests
3. Discussion
4. Materials and Methods
4.1. Active Compounds
4.2. Materials for the Galenic Preparation and Reagents for Quantitative Analysis
4.3. Oils and Capsules Preparation
4.4. Analytical Method
4.5. Stability Test
4.6. Statistical Evaluation
5. Conclusions
6. Patent
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| THCA | delta-9-tetrahydrocannabinolic acid |
| CBDA | cannabidiolic acid |
| THC | delta-9-tetrahydrocannabinol |
| CBD | cannabidiol |
| CBN | cannabinol |
| CE | collision energies |
References
- Lafaye, G.; Karila, L.; Blecha, L.; Benyamina, A. Cannabis, cannabinoids, and health. Dialogues Clin. Neurosc. 2017, 19, 309–316. [Google Scholar]
- Pisanti, S.; Bifulco, M. Medical Cannabis: A plurimillennial history of an evergreen. J. Cell. Physiol. 2019, 234, 8342–8351. [Google Scholar] [CrossRef]
- Hill, K.P. Medical Marijuana for Treatment of Chronic Pain and Other Medical and Psychiatric Problems: A Clinical Review. JAMA 2015, 313, 2474–2483. [Google Scholar] [CrossRef]
- Whiting, P.F.; Wolff, R.F.; Deshpande, S.; Di Nisio, M.; Duffy, S.; Hernandez, A.V.; Keurentjes, J.C.; Lang, S.; Misso, K.; Ryder, S.; et al. Cannabinoids for medical use. JAMA 2015, 313, 2456–2473. [Google Scholar] [CrossRef] [PubMed]
- Bar-Lev Schleider, L.; Abuhasira, R.; Novack, V. Medical Cannabis: Aligning use to evidence-based medicine approach. Br. J. Clin. Pharmacol. 2018, 84, 2458–2462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gould, J. The cannabis crop. Nature 2015, 525, S2–S3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grotenhermen, F. Pharmacokinetics and pharmacodynamics of cannabinoids. Clin. Pharm. 2003, 42, 327–360. [Google Scholar] [CrossRef]
- President of the Italian Republic. Decree of the President of the Italian Republic, DPR 309/1990. Testo unico delle leggi in materia di disciplina degli stupefacenti e sostanze psicotrope, prevenzione, cura e riabilitazione dei relativi stati di tossicodipendenza. GU n.255 del 31-10-1990—Suppl. Ordinario n. 67. Available online: https://www.gazzettaufficiale.it/eli/id/2015/11/30/15A08888/sg;jses= (accessed on 31 January 2021).
- Ministry of Health. Ministerial Decree November, 2015. Funzioni di Organismo statale per la cannabis previsto dagli articoli 23 e 28 della convenzione unica sugli stupefacenti del 1961, come modificata nel 1972. Allegato rettificato dal Comunicato 07 gennaio 2016. G.U. Serie Generale, n. 279 del 30 Novembre 2015. Available online: https://www.gazzettaufficiale.it/eli/id/1990/10/31/090G0363/sg (accessed on 31 January 2021).
- Pharmaceutical Chemical Military Facility in Florence. Medical Cannabis Production. Available online: http://www.farmaceuticomilitare.it/cannabis.aspx?lnrid=25 (accessed on 31 September 2020).
- Ministry of Health. Raccomandazioni Per il Medico Prescrittore di Sostanza Vegetale Cannabis fm2 Infiorescenze. 2017. Available online: http://www.salute.gov.it/imgs/C_17_pagineAree_4589_listaFile_itemName_2_file.pdf (accessed on 31 September 2020).
- Baratta, F.; Simiele, M.; Pignata, I.; Ravetto Enri, L.; Torta, R.; De Luca, A.; Collino, M.; D’Avolio, A.; Brusa, P. Development of Standard Operating Protocols for the Optimization of Cannabis-Based Formulations for Medical Purposes. Front. Pharmacol. 2019, 10, 701. [Google Scholar] [CrossRef]
- Romano, L.L.; Hazekamp, A. Cannabis oil: Chemical evaluation of an upcoming cannabis- based medicine. Cannabinoids 2013, 1, 1–11. [Google Scholar]
- Citti, C.; Ciccarella, G.; Braghiroli, D.; Parenti, C.; Vandelli, M.A.; Cannazza, G. Medicinal Cannabis: Principal cannabinoids concentration and their stability evaluated by a high performance liquid chromatography coupled to diode array and quadrupole time of flight mass spectrometry method. J. Pharm. Biomed. Anal. 2016, 128, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Roda, G.; Casagni, E.; Gambaro, V. Titolazione, controllo qualità e analisi farmaceutiche. In Proceedings of the First Italian Conference on Cannabis as a Possible Drug, Milan, Italy, 15 May 2018; Available online: https://www.youtube.com/watch?v=ewc3cq9ssRo (accessed on 31 January 2021).
- Società Italiana Farmacisti Preparatori (SIFAP). 2016. Available online: https://www.sifap.org/procedure/estrazione-oleosa-di-infiorescenze-femminili-di-cannabi (accessed on 31 September 2020).
- European Directorate for the Quality of Medicines and HealthCare. European Pharmacopoeia, 10th ed.; Council of Europe: Geneva, Switzerland, 2020. [Google Scholar]
- Ramella, A.; Roda, G.; Pavlovic, R.; Dei Cas, M.; Casagni, E.; Mosconi, G.; Cecati, F.; Minghetti, P.; Grizzetti, C. Impact of Lipid Sources on Quality Traits of Medical Cannabis-Based Oil Preparations. Molecules 2020, 25, 2986. [Google Scholar] [CrossRef]
- Pacifici, R.; Marchei, E.; Salvatore, F.; Guandalini, L.; Busardò, F.P.; Pichini, S. Evaluation of cannabinoids concentration and stability in standardized preparations of cannabis tea and cannabis oil by ultra-high performance liquid chromatography tandem mass spectrometry. Clin. Chem. Lab. Med. 2017, 55, 1555–1563. [Google Scholar] [CrossRef]
- Pacifici, R.; Marchei, E.; Salvatore, F.; Guandalini, L.; Busardò, F.P.; Pichini, S. Evaluation of long-term stability of cannabinoids in standardized preparations of cannabis flowering tops and cannabis oil by ultra-high-performance liquid chromatography tandem mass spectrometry. Clin. Chem. Lab. Med. 2018, 28, 94–96. [Google Scholar] [CrossRef]
- Calvi, L.; Pentimalli, D.; Panseri, S.; Giupponi, L.; Gelmini, F.; Beretta, G.; Vitali, D.; Bruno, M.; Zilio, E.; Pavlovic, R.; et al. Comprehensive quality evaluation of medical Cannabis sativa L. inflorescence and macerated oils based on HS-SPME coupled to GC–MS and LC-HRMS (q-exactive orbitrap®) approach. J. Pharm. Biomed. Anal. 2018, 150, 208–219. [Google Scholar] [CrossRef]
- Wang, M.; Wang, Y.H.; Avula, B.; Radwan, M.M.; Wanas, A.S.; Van Antwerp, J.; Parcher, J.F.; ElSohly, M.A.; Khan, I.A. Decarboxylation Study of Acidic Cannabinoids: A Novel Approach Using Ultra-High-Performance Supercritical Fluid Chromatography/Photodiode Array-Mass Spectrometry. Cannabis Cannabinoid Res. 2016, 1, 262–271. [Google Scholar] [CrossRef] [Green Version]
- Carcieri, C.; Tomasello, C.; Simiele, M.; De Nicolò, A.; Avataneo, V.; Canzoneri, L.; Cusato, J.; Di Perri, G.; D’Avolio, A. Cannabinoids concentration variability in cannabis olive oil galenic preparations. J. Pharm. Pharmacol. 2018, 70, 143–149. [Google Scholar] [CrossRef]
- Pichini, S.; Mannocchi, G.; Gottardi, M.; Pérez-Acevedo, A.P.; Poyatos, L.; Papaseit, E.; Pérez-Mañá, C.; Farré, M.; Pacifici, R.; Busardò, F.P. Fast and sensitive UHPLC-MS/MS analysis of cannabinoids and their acid precursors in pharmaceutical preparations of medical cannabis and their metabolites in conventional and non-conventional biological matrices of treated individual. Talanta 2020, 209, 120537. [Google Scholar] [CrossRef]
- Pichini, S.; Malaca, S.; Gottardi, M.; Pérez-Acevedo, A.P.; Papaseit, E.; Perez-Maña, C.; Farré, M.; Pacifici, R.; Tagliabracci, A.; Mannocchi, G.; et al. UHPLC-MS/MS analysis of cannabidiol metabolites in serum and urine samples. Application to an individual treated with medical cannabis. Talanta 2021, 223, 121772. [Google Scholar] [CrossRef]
- Brunetti, P.; Pichini, S.; Pacifici, R.; Busardò, F.P.; Del Rio, A. Herbal Preparations of Medical Cannabis: A Vademecum for Prescribing Doctors. Medicina 2020, 56, 237. [Google Scholar] [CrossRef]
- Wong, K.U.; Baum, C.R. Acute Cannabis Toxicity. Pediatr. Emerg. Care 2019, 35, 799–806. [Google Scholar] [CrossRef]
- Maida, V.; Daeninck, P.J. A user’s guide to cannabinoid therapies in oncology. Curr. Oncol. 2016, 23, 398–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lucas, C.; Galettis, P.; Schneider, J. The pharmacokinetics and the pharmacodynamics of cannabinoids. Br. J. Clin. Pharmacol. 2018, 84, 2477–2482. [Google Scholar] [CrossRef] [Green Version]
- Merrick, J.; Lane, B.; Sebree, T.; Yaksh, T.; O’Neill, C.; Banks, S.L. Identification of Psychoactive Degradants of Cannabidiol in Simulated Gastric and Physiological Fluid. Cannabis Cannabinoid Res. 2016, 1, 102–112. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Oil | Capsules Containing 156 µL of Oil, T0 | Capsules Containing 312 µL of Oil, T0 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Active Constituent | Average Concentration of Active Constituent (mg/mL) in Oil | Average Concentration of Active Constituent (mg/mL) in Capsules | Standard Deviation | Δ% Compared to Oil | Concentration of Active Molecule: Minimum Value (mg/mL) in Capsules | Concentration of Active Molecule: Maximum Value (mg/mL) in Capsules | Average Concentration of Active Constituent (mg/mL) in Capsules | Standard Deviation | Δ% Compared to Oil | Concentration of Active Molecule: Minimum Value (mg/mL) in Capsules | Concentration of Active Molecule: Maximum Value (mg/mL) in Capsules |
| CBD | 12.092 | 12.057 | 0.42 | −0.29 | 11.483 | 12.524 | 12.557 | 0.57 | 3.85 | 11.400 | 13.139 |
| THC | 6.971 | 7.216 | 0.21 | 3.51 | 6.873 | 7.455 | 7.286 | 0.46 | 4.51 | 6.348 | 7.661 |
| CBDA | 0.631 | 0.611 | 0.03 | −3.25 | 0.580 | 0.657 | 0.630 | 0.02 | 0.11 | 0.608 | 0.676 |
| THCA | 0.036 | 0.037 | 0.00 | 1.667 | 0.034 | 0.039 | 0.036 | 0.00 | −0.32 | 0.033 | 0.039 |
| CBN | 0.450 | 0.441 | 0.03 | −2.078 | 0.412 | 0.489 | 0.455 | 0.02 | 1.16 | 0.429 | 0.494 |
| Oils-Fridge | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OILS, T0 | T15 | T30 | T60 | |||||||||||||||||
| Active Constituent | Average Concentration of Active Constituent (mg/mL) | Standard Deviation | Concentration of Active Molecule: Minimum Value (mg/mL) | Concentration of Active Molecule: Maximum Value (mg/mL) | Average Concentration of Active Constituent (mg/mL) | Δ% Compared to T0 | Standard Deviation | Concentration of Active Molecule: Minimum Value (mg/mL) | Concentration of Active Molecule: Maximum Value (mg/mL) | Average Concentration of Active Constituent (mg/mL) | Δ% Compared to T0 | Standard Deviation | Concentration of Active Molecule: Minimum Value (mg/mL) | Concentration of Active Molecule: Maximum Value (mg/mL) | Average Concentration of Active Constituent (mg/mL) | Δ% Compared to T0 | Standard Deviation | Concentration of Active Molecule: Minimum Value (mg/mL) | Concentration of Active Molecule: Maximum Value (mg/mL) | |
| CBD | 12.092 | 1.31 | 10.442 | 14.814 | 12.338 | 2.04 | 1.26 | 10.524 | 14.007 | 12.591 | 4.12 | 1.01 | 10.941 | 14.496 | 12.917 | 6.82 | 0.90 | 11.551 | 14.092 | |
| THC | 6.971 | 0.61 | 5.935 | 8.188 | 6.790 | −2.60 | 0.43 | 6.309 | 7.452 | 6.781 | −2.73 | 0.28 | 6.111 | 7.035 | 6.754 | −3.11 | 0.15 | 6.510 | 7.039 | |
| CBDA | 0.631 | 0.07 | 0.504 | 0.783 | 0.573 | −9.29 | 0.12 | 0.406 | 0.757 | 0.576 | −8.81 | 0.10 | 0.423 | 0.706 | 0.608 | −3.64 | 0.07 | 0.492 | 0.688 | |
| THCA | 0.036 | 0.09 | 0.010 | 0.070 | 0.034 | −7.25 | 0.01 | 0.010 | 0.043 | 0.039 | 8.17 | 0.01 | 0.030 | 0.052 | 0.035 | −4.59 | 0.02 | 0.017 | 0.064 | |
| CBN | 0.450 | 0.02 | 0.329 | 0.602 | 0.414 | −7.92 | 0.04 | 0.357 | 0.494 | 0.412 | −8.28 | 0.04 | 0.349 | 0.479 | 0.471 | 4.78 | 0.05 | 0.407 | 0.552 | |
| Oils-Fridge | ||||||||||||||||||||
| T90 | T120 | T150 | T180 | |||||||||||||||||
| Active Constituent | Average Concentration of Active Constituent (mg/mL) | Δ% Compared to T0 | Standard Deviation | Concentration of Active Molecule: Minimum Value (mg/mL) | Concentration of Active Molecule: Maximum Value (mg/mL) | Average Concentration of Active Constituent (mg/mL) | Δ% Compared to T0 | Standard Deviation | Concentration of Active Molecule: Minimum Value (mg/mL) | Concentration of Active Molecule: Maximum Value (mg/mL) | Average Concentration of Active Constituent (mg/mL) | Δ% Compared to T0 | Standard Deviation | Concentration of Active Molecule: Minimum Value (mg/mL) | Concentration of Active Molecule: Maximum Value (mg/mL) | Average Concentration of Active Constituent (mg/mL) | Δ% Compared to T0 | Standard Deviation | Concentration of Active Molecule: Minimum Value (mg/mL) | Concentration of Active Molecule: Maximum Value (mg/mL) |
| CBD | 10.994 | −9.09 | 0.75 | 9.909 | 12.170 | 11.658 | −3.59 | 1.25 | 10.136 | 13.632 | 11.566 | −4.36 | 0.95 | 10.245 | 12.664 | 11.533 | −4.63 | 0.68 | 10.700 | 12.826 |
| THC | 6.468 | −7.22 | 0.36 | 5.897 | 6.943 | 7.134 | 2.34 | 0.51 | 6.204 | 7.715 | 7.108 | 1.96 | 0.26 | 6.773 | 7.566 | 6.790 | −2.61 | 0.29 | 6.209 | 7.156 |
| CBDA | 0.658 | 4.28 | 0.10 | 0.535 | 0.846 | 0.682 | 8.08 | 0.12 | 0.514 | 0.886 | 0.657 | 4.14 | 0.11 | 0.501 | 0.817 | 0.688 | 8.94 | 0.08 | 0.588 | 0.844 |
| THCA | 0.038 | 3.90 | 0.02 | 0.012 | 0.056 | 0.033 | −8.26 | 0.02 | 0.013 | 0.064 | 0.034 | −6.73 | 0.02 | 0.010 | 0.050 | 0.039 | 7.34 | 0.02 | 0.010 | 0.061 |
| CBN | 0.417 | −7.23 | 0.04 | 0.361 | 0.485 | 0.475 | 5.60 | 0.08 | 0.354 | 0.579 | 0.490 | 9.01 | 0.07 | 0.347 | 0.568 | 0.465 | 3.37 | 0.04 | 0.425 | 0.529 |
| Oils-Room Temperature | ||||||||||||||||||||
| Oils, T0 | T15 | T30 | T60 | |||||||||||||||||
| Active Constituent | Average Concentration of Active Constituent (mg/mL) | Standard Deviation | Concentration of Active Molecule: Minimum Value (mg/mL) | Concentration of Active Molecule: Maximum Value (mg/mL) | Average Concentration of Active Constituent (mg/mL) | Δ% Compared to T0 | Standard Deviation | Concentration of Active Molecule: Minimum Value (mg/mL) | Concentration of Active Molecule: Maximum Value (mg/mL) | Average Concentration of Active Constituent (mg/mL) | Δ% Compared to T0 | Standard Deviation | Concentration of Active Molecule: Minimum Value (mg/mL) | Concentration of Active Molecule: Maximum Value (mg/mL) | Average Concentration of Active Constituent (mg/mL) | Δ% Compared to T0 | Standard Deviation | Concentration of Active Molecule: Minimum Value (mg/mL) | Concentration of Active Molecule: Maximum Value (mg/mL) | |
| CBD | 12.092 | 1.31 | 10.442 | 14.814 | 11.725 | −3.04 | 1.26 | 9.891 | 13.897 | 12.516 | 3.51 | 0.73 | 11.542 | 13.883 | 12.904 | 6.72 | 1.26 | 10.848 | 14.961 | |
| THC | 6.971 | 0.61 | 5.935 | 8.188 | 6.482 | −7.02 | 0.45 | 5.646 | 7.240 | 6.633 | −4.85 | 0.33 | 6.116 | 7.128 | 6.587 | −5.52 | 0.19 | 6.905 | 6.402 | |
| CBDA | 0.631 | 0.07 | 0.504 | 0.783 | 0.570 | −9.64 | 0.05 | 0.468 | 0.631 | 0.573 | −9.22 | 0.04 | 0.503 | 0.629 | 0.598 | −5.30 | 0.06 | 0.504 | 0.699 | |
| THCA | 0.036 | 0.09 | 0.010 | 0.070 | 0.036 | −0.92 | 0.01 | 0.013 | 0.050 | 0.039 | 7.95 | 0.01 | 0.015 | 0.054 | 0.035 | −2.75 | 0.01 | 0.017 | 0.056 | |
| CBN | 0.450 | 0.02 | 0.329 | 0.602 | 0.406 | −9.60 | 0.03 | 0.362 | 0.451 | 0.435 | −3.23 | 0.03 | 0.390 | 0.484 | 0.489 | 8.69 | 0.04 | 0.412 | 0.543 | |
| Oils-Room Temperature | ||||||||||||||||||||
| T90 | T120 | T150 | T180 | |||||||||||||||||
| Active Constituent | Average Concentration of Active Constituent (mg/mL) | Δ% Compared to T0 | Standard Deviation | Concentration of Active Molecule: Minimum Value (mg/mL) | Concentration of Active Molecule: Maximum Value (mg/mL) | Average Concentration of Active Constituent (mg/mL) | Δ% Compared to T0 | Standard Deviation | Concentration of Active Molecule: Minimum Value (mg/mL) | Concentration of Active Molecule: Maximum Value (mg/mL) | Average Concentration of Active Constituent (mg/mL) | Δ% Compared to T0 | Standard Deviation | Concentration of Active Molecule: Minimum Value (mg/mL) | Concentration of Active Molecule: Maximum Value (mg/mL) | Average Concentration of Active Constituent (mg/mL) | Δ% Compared to T0 | Standard Deviation | Concentration of Active Molecule: Minimum Value (mg/mL) | Concentration of Active Molecule: Maximum Value (mg/mL) |
| CBD | 11.101 | −8.20 | 1.23 | 10.005 | 13.253 | 12.005 | −0.72 | 1.07 | 10.302 | 13.340 | 12.123 | 0.26 | 0.77 | 10.687 | 13.018 | 11.921 | −1.41 | 1.04 | 10.388 | 13.269 |
| THC | 6.426 | −7.82 | 0.63 | 5.474 | 7.005 | 6.788 | −2.63 | 0.37 | 6.319 | 7.341 | 6.942 | −0.42 | 0.39 | 6.286 | 7.346 | 6.826 | −2.09 | 0.16 | 6.584 | 7.084 |
| CBDA | 0.603 | −4.44 | 0.08 | 0.397 | 0.709 | 0.667 | 5.65 | 0.07 | 0.578 | 0.804 | 0.627 | −0.72 | 0.08 | 0.544 | 0.750 | 0.665 | 5.28 | 0.08 | 0.529 | 0.791 |
| THCA | 0.039 | 7.68 | 0.02 | 0.011 | 0.066 | 0.035 | −3.67 | 0.02 | 0.014 | 0.062 | 0.039 | 7.92 | 0.02 | 0.010 | 0.061 | 0.034 | −5.51 | 0.02 | 0.010 | 0.067 |
| CBN | 0.471 | 4.73 | 0.09 | 0.604 | 0.297 | 0.465 | 3.40 | 0.11 | 0.304 | 0.589 | 0.476 | 5.87 | 0.04 | 0.407 | 0.535 | 0.481 | 6.96 | 0.07 | 0.375 | 0.596 |
| Capsules Containing 156 µL of Oil | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T90 Fridge | T180 Fridge | |||||||||||
| Active Constituent | Average Concentration of Active Constituent (mg/mL) in Capsules | Standard Deviation | Δ% Compared to Oil | Δ% Compared to Cps at T0 | Concentration of Active Molecule: Minimum Value (mg/mL) in Capsules | Concentration of Active Molecule: Maximum Value (mg/mL) in Capsules | Average Concentration of Active Constituent (mg/mL) in Capsules | Standard Deviation | Δ% Compared to Oil | Δ% Compared to Cps at T0 | Concentration of Active Molecule: Minimum Value (mg/mL) in Capsules | Concentration of Active Molecule: Maximum Value (mg/mL) in Capsules |
| CBD | 12.369 | 0.34 | 2.29 | 2.59 | 12.030 | 12.843 | 12.511 | 0.55 | 3.47 | 3.77 | 11.485 | 13.545 |
| THC | 7.351 | 0.24 | 5.45 | 1.87 | 7.029 | 7.603 | 7.420 | 0.21 | 6.44 | 2.83 | 7.135 | 7.640 |
| CBDA | 0.624 | 0.04 | −1.11 | 2.27 | 0.570 | 0.680 | 0.637 | 0.03 | 0.95 | 4.32 | 0.592 | 0.676 |
| THCA | 0.036 | 0.00 | 0.00 | -2.19 | 0.034 | 0.039 | 0.036 | 0.00 | 0.00 | −1.64 | 0.033 | 0.039 |
| CBN | 0.458 | 0.01 | 1.78 | 3.98 | 0.442 | 0.471 | 0.455 | 0.03 | 1.11 | 3.25 | 0.414 | 0.491 |
| T90 Room Temperature | T180 Room Temperature | |||||||||||
| Active Constituent | Average Concentration of Active Constituent (mg/mL) in Capsules | Standard Deviation | Δ% Compared to Oil | Δ% Compared to Cps at T0 | Concentration of Active Molecule: Minimum Value (mg/mL) in Capsules | Concentration of Active Molecule: Maximum Value (mg/mL) in Capsules | Average Concentration of Active Constituent (Mg/Ml) in Capsules | Standard Deviation | Δ% Compared to Oil | Δ% Compared to Cps at T0 | Concentration of Active Molecule: Minimum Value (mg/mL) in Capsules | Concentration of Active Molecule: Maximum Value (mg/mL) in Capsules |
| CBD | 12.904 | 0.31 | 6.72 | 7.02 | 12.571 | 13.301 | 12.648 | 0.50 | 4.60 | 4.90 | 11.857 | 13.278 |
| THC | 6.923 | 0.37 | −0.69 | −4.06 | 6.286 | 7.255 | 7.349 | 0.17 | 5.42 | 1.84 | 7.111 | 7.592 |
| CBDA | 0.643 | 0.02 | 1.90 | 5.24 | 0.611 | 0.658 | 0.634 | 0.02 | 0.48 | 3.89 | 0.590 | 0.656 |
| THCA | 0.038 | 0.00 | 5.56 | 2.94 | 0.036 | 0.039 | 0.036 | 0.00 | 0.00 | −3.01 | 0.033 | 0.039 |
| CBN | 0.441 | 0.04 | −2.00 | 0.12 | 0.486 | 0.488 | 0.444 | 0.03 | −1.33 | 0.73 | 0.406 | 0.481 |
| Capsules Containing 312 µL of Oil | ||||||||||||
| T90 Fridge | T180 Fridge | |||||||||||
| Active Constituent | Average Concentration of Active Constituent (mg/mL) in Capsules | Standard Deviation | Δ% Compared to Oil | Δ% Compared to Cps at T0 | Concentration of Active Molecule: Minimum Value (mg/mL) in Capsules | Concentration of Active Molecule: Maximum Value (mg/mL) in Capsules | Average Concentration of Active Constituent (mg/mL) in Capsules | Standard Deviation | Δ% Compared to Oil | Δ% Compared to Cps at T0 | Concentration of Active Molecule: Minimum Value (mg/mL) in Capsules | Concentration of Active Molecule: Maximum Value (mg/mL) in Capsules |
| CBD | 12.471 | 0.82 | 3.13 | −0.69 | 10.977 | 13.283 | 12.325 | 0.61 | 1.93 | −1.85 | 10.946 | 12.874 |
| THC | 6.767 | 0.35 | −2.93 | −8.21 | 6.441 | 7.345 | 7.076 | 0.37 | 1.51 | −4.02 | 6.475 | 7.595 |
| CBDA | 0.652 | 0.03 | 3.33 | 3.36 | 0.62 | 0.691 | 0.649 | 0.03 | 2.85 | 2.96 | 0.601 | 0.692 |
| THCA | 0.037 | 0.00 | 2.78 | 2.44 | 0.035 | 0.039 | 0.037 | 0.00 | 2.78 | 1.30 | 0.033 | 0.039 |
| CBN | 0.455 | 0.03 | 1.11 | −1.16 | 0.406 | 0.494 | 0.444 | 0.02 | −1.33 | −3.42 | 0.411 | 0.485 |
| T90 Room Temperature | T180 Room Temperature | |||||||||||
| Active Constituent | Average Concentration of Active Constituent (mg/mL) in Capsules | Standard Deviation | Δ% Compared to Oil | Δ% Compared to Cps at T0 | Concentration of Active Molecule: Minimum Value (mg/mL) in Capsules | Concentration of Active Molecule: Maximum Value (mg/mL) in Capsules | Average Concentration of Active Constituent (mg/mL) in Capsules | Standard Deviation | Δ% Compared to oil | Δ% Compared to Cps at T0 | Concentration of Active Molecule: Minimum Value (mg/mL) in Capsules | Concentration of Active Molecule: Maximum Value (mg/mL) in Capsules |
| CBD | 12.618 | 0.51 | 4.35 | 0.48 | 11.886 | 13.279 | 12.52 | 0.50 | 3.54 | −0.30 | 11.833 | 12.988 |
| THC | 6.701 | 0.47 | −3.87 | −9.10 | 6.317 | 7.595 | 7.066 | 0.17 | 1.36 | −4.15 | 6.624 | 7.618 |
| CBDA | 0.647 | 0.03 | 2.54 | 2.67 | 0.604 | 0.686 | 0.629 | 0.02 | −0.32 | −0.14 | 0.598 | 0.684 |
| THCA | 0.035 | 0.00 | −2.78 | −3.62 | 0.033 | 0.037 | 0.037 | 0.00 | 2.78 | 1.90 | 0.034 | 0.039 |
| CBN | 0.449 | 0.03 | −0.22 | −1.379 | 0.41 | 0.495 | 0.453 | 0.03 | 0.67 | −1.51 | 0.422 | 0.487 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baratta, F.; Simiele, M.; Pignata, I.; Ravetto Enri, L.; D’Avolio, A.; Torta, R.; De Luca, A.; Collino, M.; Brusa, P. Cannabis-Based Oral Formulations for Medical Purposes: Preparation, Quality and Stability. Pharmaceuticals 2021, 14, 171. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14020171
Baratta F, Simiele M, Pignata I, Ravetto Enri L, D’Avolio A, Torta R, De Luca A, Collino M, Brusa P. Cannabis-Based Oral Formulations for Medical Purposes: Preparation, Quality and Stability. Pharmaceuticals. 2021; 14(2):171. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14020171
Chicago/Turabian StyleBaratta, Francesca, Marco Simiele, Irene Pignata, Lorenzo Ravetto Enri, Antonio D’Avolio, Riccardo Torta, Anna De Luca, Massimo Collino, and Paola Brusa. 2021. "Cannabis-Based Oral Formulations for Medical Purposes: Preparation, Quality and Stability" Pharmaceuticals 14, no. 2: 171. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14020171