
Therapeutic Drug Monitoring of Busulfan in Patients Undergoing Hematopoietic Cell Transplantation: A Pilot Single-Center Study in Taiwan

 ,
, 
Abstract
:1. Introduction
2. Results
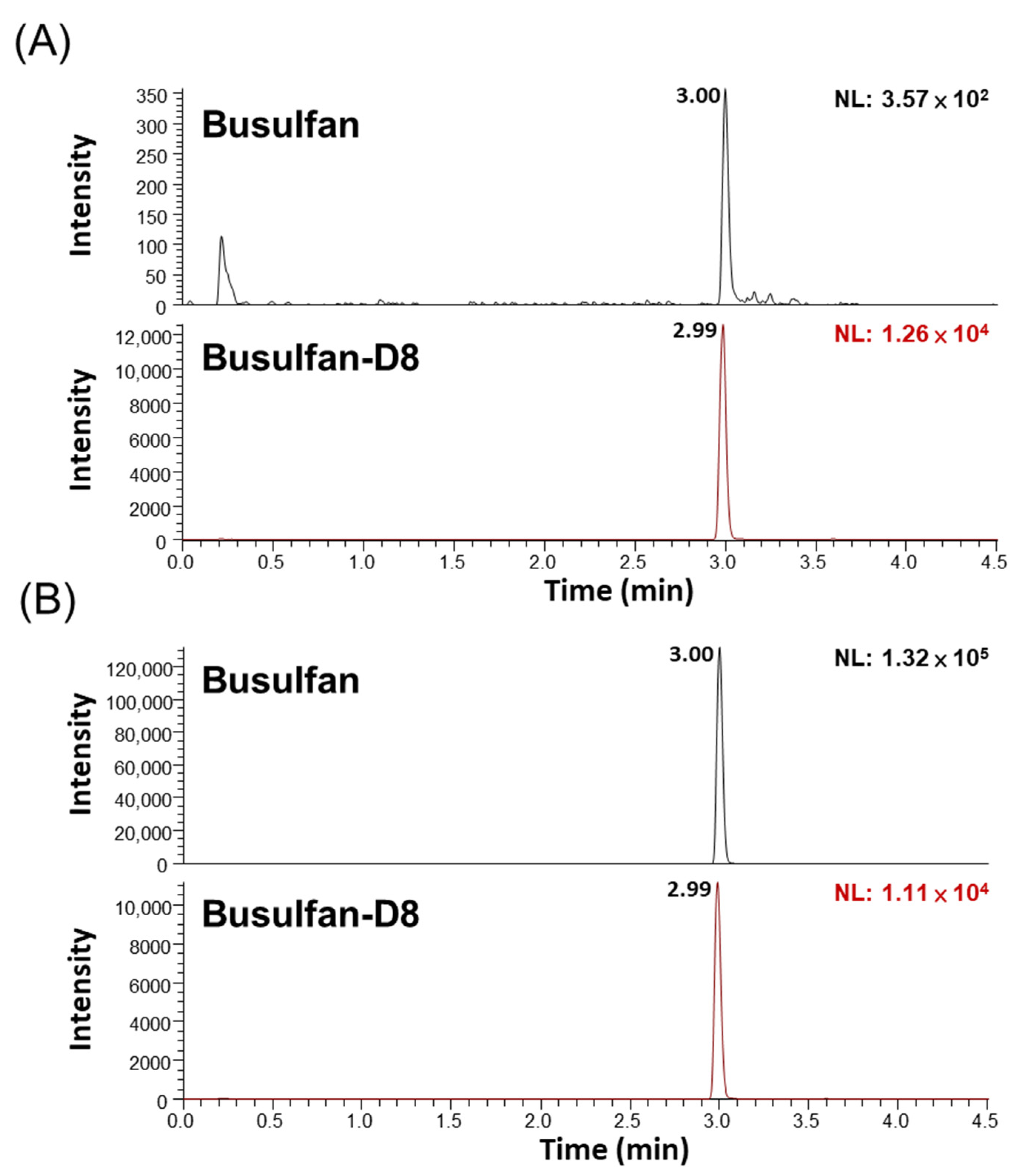
2.1. Recovery and Matrix Effect
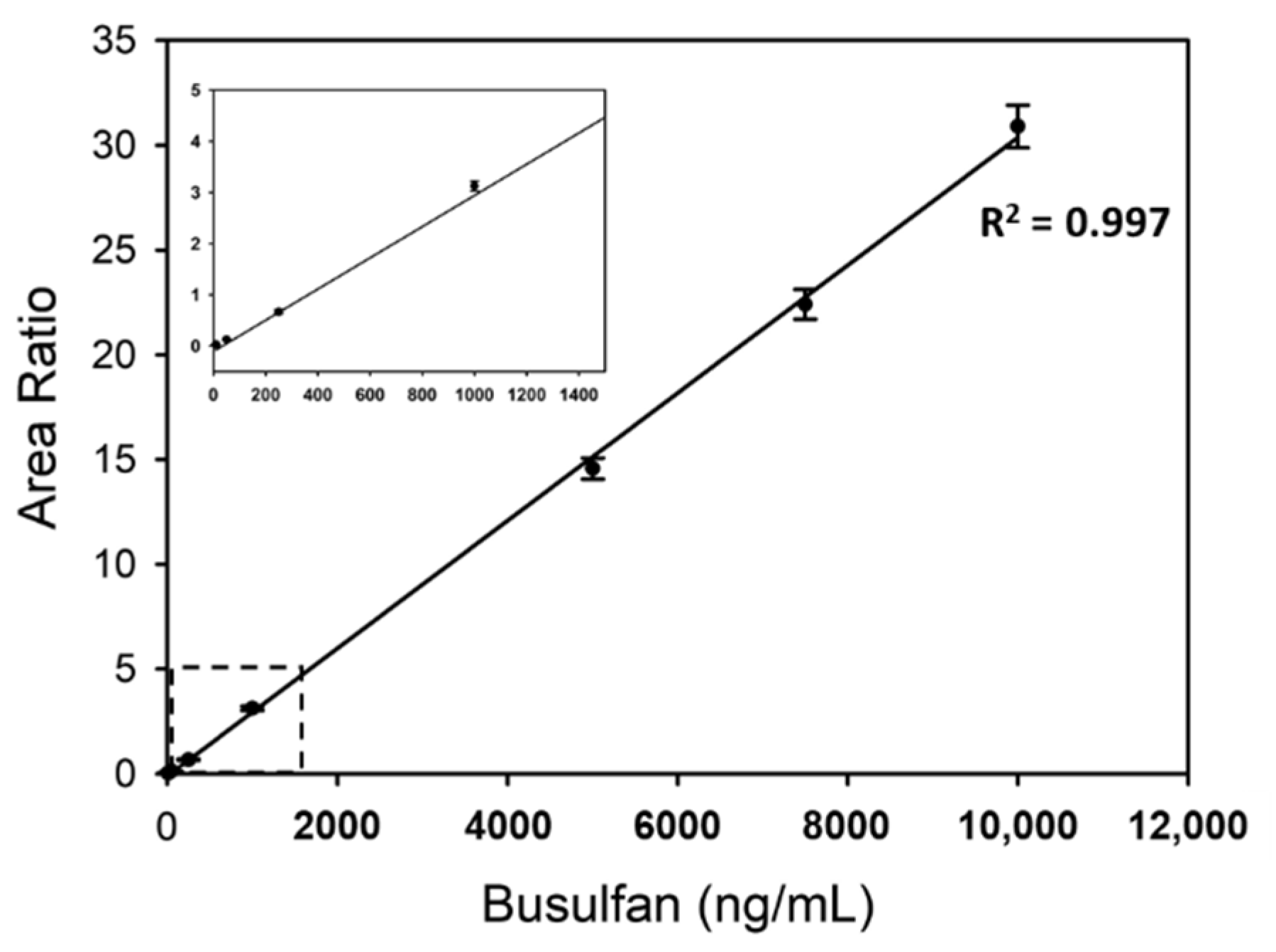
2.2. Linearity
2.3. Precision and Accuracy
2.4. Proficiency Test
2.5. Clinical Samples
3. Discussion
4. Materials and Methods
4.1. Chemicals and Reagents
4.2. Patients and Samples
4.3. Preparation of Standards Internal Standard and Quality Control (QC) Samples
4.4. Sample Preparation
4.5. LC–MS/MS
4.6. Method Validation
4.7. Busulfan Exposure Calculation and Dose Adjustment
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gyurkocza, B.; Sandmaier, B.M. Conditioning regimens for hematopoietic cell transplantation: One size does not fit all. Blood 2014, 124, 344–353. [Google Scholar] [CrossRef] [Green Version]
- Santos, G.W.; Tutschka, P.J.; Mellits, D.; Sensenbrenner, L.L.; Stuart, R.K.; Yeager, A.M.; Brookmeyer, R.; Saral, R.; Beschorner, W.E.; Bias, W.B.; et al. Marrow Transplantation for Acute Nonlymphocytic Leukemia after Treatment with Busulfan and Cyclophosphamide. N. Engl. J. Med. 1983, 309, 1347–1353. [Google Scholar] [CrossRef]
- Elborai, Y.; Hafez, H.; Moussa, E.A.; Hammad, M.; Hussein, H.; Lehmann, L.; Elhaddad, A. Comparison of toxicity following different conditioning regimens (busulfan/melphalan and carboplatin/etoposide/melphalan) for advanced stage neuroblastoma: Experience of two transplant centers. Pediatr. Transplant. 2015, 20, 284–289. [Google Scholar] [CrossRef]
- Pasqualini, C.; Dufour, C.; Goma, G.; Raquin, M.-A.; Lapierre, V.; Valteau-Couanet, D. Tandem high-dose chemotherapy with thiotepa and busulfan-melphalan and autologous stem cell transplantation in very high-risk neuroblastoma patients. Bone Marrow Transplant. 2016, 51, 227–231. [Google Scholar] [CrossRef] [Green Version]
- Engelen, M.; Kemp, S.; De Visser, M.; Van Geel, B.M.; Wanders, R.J.A.; Aubourg, P.; Poll-The, B.T. X-linked adrenoleukodystrophy (X-ALD): Clinical presentation and guidelines for diagnosis, follow-up and management. Orphanet J. Rare Dis. 2012, 7, 51. [Google Scholar] [CrossRef]
- Nyhan, W.L.; Parkman, R.; Page, T.; E Gruber, H.; Pyati, J.; Jolly, D.; Friedmann, T. Bone marrow transplantation in lesch-nyhan disease: 147. Pediatr. Res. 1985, 19, 768. [Google Scholar] [CrossRef] [Green Version]
- Kállay, K.; Liptaï, Z.; Benyó, G.; Kassa, C.; Goda, V.; Sinkó, J.; Tóth, Á.; Kriván, G. Successful unrelated umbilical cord blood transplantation in Lesch-Nyhan syndrome. Metab. Brain Dis. 2012, 27, 193–196. [Google Scholar] [CrossRef]
- Andersson, B.S.; Kashyap, A.; Gian, V.; Wingard, J.R.; Fernandez, H.; Cagnoni, P.J.; Jones, R.B.; Tarantolo, S.; Hu, W.W.; Blume, K.G.; et al. Conditioning therapy with intravenous busulfan and cyclophosphamide (IV BuCy2) for hematologic malignancies prior to allogeneic stem cell transplantation: A phase II study. Biol. Blood Marrow Transplant. 2002, 8, 145–154. [Google Scholar] [CrossRef] [Green Version]
- Iravani, M.; Evazi, M.; Ghavamzadeh, A.; Mousavi, S.A.; Shamshiri, A.R.; Tavakoli, M.; Ashouri, A.; Samiee, S.; Chahardovali, B.; Alimoghaddam, K.; et al. Fludarabine and busulfan as a myeloablative conditioning regimen for allogeneic stem cell transplantation in high- and standard-risk leukemic patients. Bone Marrow Transplant. 2007, 40, 105–110. [Google Scholar] [CrossRef] [Green Version]
- Bornhäuser, M.; Storer, B.; Slattery, J.T.; Appelbaum, F.R.; Deeg, H.J.; Hansen, J.; Martin, P.J.; McDonald, G.B.; Nichols, W.G.; Radich, J.; et al. Conditioning with fludarabine and targeted busulfan for transplantation of allogeneic hematopoietic stem cells. Blood 2003, 102, 820–826. [Google Scholar] [CrossRef] [Green Version]
- Haddow, A.; Timmis, G. Myleran in chronic myeloid leukæmia chemical constitution and biological action. Lancet 1953, 261, 207–208. [Google Scholar] [CrossRef]
- Grochow, L.B. Busulfan disposition: The role of therapeutic monitoring in bone marrow transplantation induction regimens. Semin. Oncol. 1993, 20, 18–25. [Google Scholar] [PubMed]
- Bhagwatwar, H.P.; Phadungpojna, S.; Chow, D.S.-L.; Andersson, B.S. Formulation and stability of busulfan for intravenous administration in high-dose chemotherapy. Cancer Chemother. Pharmacol. 1996, 37, 401–408. [Google Scholar] [CrossRef] [PubMed]
- Wall, D.A.; Chan, K.W.; Nieder, M.L.; Hayashi, R.J.; Yeager, A.M.; Kadota, R.; Przepiorka, D.; Mezzi, K.; Kletzel, M. Safety, efficacy, and pharmacokinetics of intravenous busulfan in children undergoing allogeneic hematopoietic stem cell transplantation. Pediatr. Blood Cancer 2009, 54, 291–298. [Google Scholar] [CrossRef]
- Hao, C.; Ma, X.; Wang, L.; Zhang, W.; Hu, J.; Huang, J.; Yang, W. Predicting the presence and mechanism of busulfan drug-drug interactions in hematopoietic stem cell transplantation using pharmacokinetic interaction network–based molecular structure similarity and network pharmacology. Eur. J. Clin. Pharmacol. 2021, 77, 595–605. [Google Scholar] [CrossRef] [PubMed]
- Myers, A.L.; Kawedia, J.D.; Champlin, R.E.; Kramer, M.A.; Nieto, Y.; Ghose, R.; Andersson, B.S. Clarifying busulfan metabolism and drug interactions to support new therapeutic drug monitoring strategies: A comprehensive review. Expert Opin. Drug Metab. Toxicol. 2017, 13, 901–923. [Google Scholar] [CrossRef]
- Krivoy, N.; Hoffer, E.; Lurie, Y.; Bentur, Y.; Rowe, J.M. Busulfan use in hematopoietic stem cell transplantation: Pharmacology, dose adjustment, safety and efficacy in adults and children. Curr. Drug Saf. 2008, 3, 60–66. [Google Scholar] [CrossRef]
- Dhere, V.; Edelman, S.; Waller, E.K.; Langston, A.; Graiser, M.; Connolly, E.C.; Switchenko, J.M.; Esiashvili, N.; Khan, M.K. Myeloablative busulfan/cytoxan conditioning versus reduced-intensity fludarabine/melphalan conditioning for allogeneic hematopoietic stem cell transplant in patients with acute myelogenous leukemia. Leuk. Lymphoma 2018, 59, 837–843. [Google Scholar] [CrossRef] [Green Version]
- Andersson, B.S.; de Lima, M.; Thall, P.F.; Wang, X.; Couriel, D.; Korbling, M.; Roberson, S.; Giralt, S.; Pierre, B.; Russell, J.A.; et al. Once Daily i.v. Busulfan and Fludarabine (i.v. Bu-Flu) Compares Favorably with i.v. Busulfan and Cyclophosphamide (i.v. BuCy2) as Pretransplant Conditioning Therapy in AML/MDS. Biol. Blood Marrow Transplant. 2008, 14, 672–684. [Google Scholar] [CrossRef] [Green Version]
- Bouligand, J.; Richard, C.; Valteau-Couanet, D.; Orear, C.; Mercier, L.; Kessari, R.; Simonnard, N.; Munier, F.; Daudigeos-Dubus, E.; Tou, B.; et al. Iron Overload Exacerbates Busulfan-Melphalan Toxicity Through a Pharmacodynamic Interaction in Mice. Pharm. Res. 2016, 33, 1913–1922. [Google Scholar] [CrossRef]
- Russell, J.; Kangarloo, S.B. Therapeutic Drug Monitoring of Busulfan in Transplantation. Curr. Pharm. Des. 2008, 14, 1936–1949. [Google Scholar] [CrossRef]
- Ciurea, S.O.; Andersson, B.S. Busulfan in Hematopoietic Stem Cell Transplantation. Biol. Blood Marrow Transplant. 2009, 15, 523–536. [Google Scholar] [CrossRef] [Green Version]
- Bartelink, I.H.; Bredius, R.G.; Ververs, T.T.; Raphael, M.F.; Van Kesteren, C.; Bierings, M.; Rademaker, C.M.; den Hartigh, J.; Uiterwaal, C.S.; Zwaveling, J.; et al. Once-Daily Intravenous Busulfan with Therapeutic Drug Monitoring Compared to Conventional Oral Busulfan Improves Survival and Engraftment in Children Undergoing Allogeneic Stem Cell Transplantation. Biol. Blood Marrow Transplant. 2008, 14, 88–98. [Google Scholar] [CrossRef] [Green Version]
- Bartelink, I.H.; Bredius, R.G.; Belitser, S.V.; Suttorp, M.M.; Bierings, M.; Knibbe, C.A.; Egeler, M.; Lankester, A.C.; Egberts, A.C.; Zwaveling, J.; et al. Association between Busulfan Exposure and Outcome in Children Receiving Intravenous Busulfan before Hematologic Stem Cell Transplantation. Biol. Blood Marrow Transplant. 2009, 15, 231–241. [Google Scholar] [CrossRef] [Green Version]
- Bartelink, I.H.; Lalmohamed, A.; van Reij, E.M.L.; Dvorak, C.C.; Savic, R.M.; Zwaveling, J.; Bredius, R.G.M.; Egberts, A.C.G.; Bierings, M.; Kletzel, M.; et al. Association of busulfan exposure with survival and toxicity after haemopoietic cell transplantation in children and young adults: A multicentre, retrospective cohort analysis. Lancet Haematol. 2016, 3, e526–e536. [Google Scholar] [CrossRef] [Green Version]
- Bartelink, I.H.; Van Kesteren, C.; Boelens, J.J.; Egberts, T.C.; Bierings, M.B.; Cuvelier, G.D.; Wynn, R.; Slatter, M.A.; Chiesa, R.; Danhof, M.; et al. Predictive Performance of a Busulfan Pharmacokinetic Model in Children and Young Adults. Ther. Drug Monit. 2012, 34, 574–583. [Google Scholar] [CrossRef]
- Matar, K.M.; Alshemmari, S.H.; Refaat, S.; Anwar, A. UPLC-Tandem Mass Spectrometry for Quantification of Busulfan in Human Plasma: Application to Therapeutic Drug Monitoring. Sci. Rep. 2020, 10, 8913. [Google Scholar] [CrossRef] [PubMed]
- Punt, A.M.; Langenhorst, J.B.; Egas, A.C.; Boelens, J.J.; van Kesteren, C.; van Maarseveen, E.M. Simultaneous quantification of busulfan, clofarabine and F-ARA-A using isotope labelled standards and standard addition in plasma by LC–MS/MS for exposure monitoring in hematopoietic cell transplantation conditioning. J. Chromatogr. B 2017, 1055–1056, 81–85. [Google Scholar] [CrossRef]
- French, D.; Sujishi, K.K.; Long-Boyle, J.R.; Ritchie, J.C. Development and Validation of a Liquid Chromatography–Tandem Mass Spectrometry Assay to Quantify Plasma Busulfan. Ther. Drug Monit. 2014, 36, 169–174. [Google Scholar] [CrossRef]
- Snyder, M.L.; Ritchie, J.C. Quantification of Busulfan in Plasma Using Liquid Chromatography Electrospray Tandem Mass Spectrometry (HPLC-ESI-MS/MS). Methods Mol. Biol. 2010, 603, 129–136. [Google Scholar] [CrossRef]
- Bunch, D.R.; Heideloff, C.; Ritchie, J.C.; Wang, S. A fast and simple assay for busulfan in serum or plasma by liquid chromatography–tandem mass spectrometry using turbulent flow online extraction technology. J. Chromatogr. B 2010, 878, 3255–3258. [Google Scholar] [CrossRef]
- Chen, L.; Zhou, Z.; Shen, M.; Ma, A. Quantitative Analysis of Busulfan in Human Plasma by LC-MS-MS. Chromatographia 2009, 70, 1727–1732. [Google Scholar] [CrossRef]
- Langenhorst, J.B.; Dorlo, T.; Van Maarseveen, E.M.; Nierkens, S.; Kuball, J.; Boelens, J.J.; Van Kesteren, C.; Huitema, A.D.R. Population Pharmacokinetics of Fludarabine in Children and Adults during Conditioning Prior to Allogeneic Hematopoietic Cell Transplantation. Clin. Pharmacokinet. 2019, 58, 627–637. [Google Scholar] [CrossRef] [Green Version]
- Xie, J.; Span, M.; Haber, M.; Trahair, T.; Lau, L.; Marshall, G.M.; Lock, R.B.; Van Maarseveen, E.; Langenhorst, J.; Boddy, A.; et al. Optimization of a clofarabine-based drug combination regimen for the preclinical evaluation of pediatric acute lymphoblastic leukemia. Pediatr. Blood Cancer 2020, 67, e28133. [Google Scholar] [CrossRef] [PubMed]
- Langenhorst, J.B.; Dorlo, T.P.; van Kesteren, C.; van Maarseveen, E.M.; Nierkens, S.; de Witte, M.A.; Boelens, J.J.; Huitema, A.D. Clinical Trial Simulation to Optimize Trial Design for Fludarabine Dosing Strategies in Allogeneic Hematopoietic Cell Transplantation. CPT Pharmacometrics Syst. Pharmacol. 2020, 9, 272–281. [Google Scholar] [CrossRef] [Green Version]
- Admiraal, R.; Boelens, J.J. Individualized conditioning regimes in cord blood transplantation: Towards improved and predictable safety and efficacy. Expert Opin. Biol. Ther. 2016, 16, 801–813. [Google Scholar] [CrossRef] [Green Version]
- Moon, S.Y.; Lim, M.K.; Hong, S.; Jeon, Y.; Han, M.; Song, S.H.; Lim, K.S.; Yu, K.-S.; Jang, I.-J.; Lee, J.W.; et al. Quantification of Human Plasma-Busulfan Concentration by Liquid Chromatography-Tandem Mass Spectrometry. Ann. Lab. Med. 2014, 34, 7–14. [Google Scholar] [CrossRef]
- Bellm, L.A.; Epstein, J.B.; Rose-Ped, A.; Martin, P.; Fuchs, H.J. Patient reports of complications of bone marrow transplantation. Support. Care Cancer 2000, 8, 33–39. [Google Scholar] [CrossRef]
- Grochow, L.B.; Jones, R.J.; Brundrett, R.B.; Braine, H.G.; Chen, T.-L.; Saral, R.; Santos, G.W.; Colvin, O.M. Pharmacokinetics of busulfan: Correlation with veno-occlusive disease in patients undergoing bone marrow transplantation. Cancer Chemother. Pharmacol. 1989, 25, 55–61. [Google Scholar] [CrossRef]
- Geddes, M.; Kangarloo, S.B.; Naveed, F.; Quinlan, D.; Chaudhry, M.A.; Stewart, D.; Savoie, M.L.; Bahlis, N.J.; Brown, C.; Storek, J.; et al. High Busulfan Exposure Is Associated with Worse Outcomes in a Daily i.v. Busulfan and Fludarabine Allogeneic Transplant Regimen. Biol. Blood Marrow Transplant. 2008, 14, 220–228. [Google Scholar] [CrossRef] [Green Version]
- McCune, J.; Gooley, T.; McCune, J.; Gibbs, J.P.; Sanders, J.E.; Petersdorf, E.W.; Appelbaum, F.R.; Anasetti, C.; Risler, L.; Sultan, D.; et al. Busulfan concentration and graft rejection in pediatric patients undergoing hematopoietic stem cell transplantation. Bone Marrow Transplant. 2002, 30, 167–173. [Google Scholar] [CrossRef] [Green Version]
- Boelens, J.J.; Bierings, M.B.; Wynn, R. HSCT in inborn errors of metabolism and osteopetrosis. In EBMT-ESH Handbook on Haematopoietic Stem Cell Transplantation; Apperley, J., Carreras, E., Gluckman, E., Masszi, T., Eds.; Forum Service Editore: Genoa, Italy, 2012; pp. 558–571. [Google Scholar]
- Mohty, M.; Malard, F.; Abecassis, M.; Aerts, E.; Alaskar, A.; Aljurf, M.; Arat, M.; Bader, P.; Baron, F.; Bazarbachi, A.; et al. Revised diagnosis and severity criteria for sinusoidal obstruction syndrome/veno-occlusive disease in adult patients: A new classification from the European Society for Blood and Marrow Transplantation. Bone Marrow Transplant. 2016, 51, 906–912. [Google Scholar] [CrossRef]
- Bowen, J.M.; Wardill, H.R. Advances in the understanding and management of mucositis during stem cell transplantation. Curr. Opin. Support. Palliat. Care 2017, 11, 341–346. [Google Scholar] [CrossRef]
- Gajewski, J.L.; McClellan, M.B.; Majhail, N.S.; Hari, P.N.; Bredeson, C.N.; Maziarz, R.T.; LeMaistre, C.F.; Lill, M.C.; Farnia, S.H.; Komanduri, K.V.; et al. Payment and Care for Hematopoietic Cell Transplantation Patients: Toward a Specialized Medical Home for Complex Care Patients. Biol. Blood Marrow Transplant. 2018, 24, 4–12. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Busulfan Level | Concentration (ng/mL) | Recovery (%) n = 2 | Matrix Factor (%) n = 2 |
|---|---|---|---|
| LQC | 25 | 92.34 | 88.53 |
| HQC | 8000 | 99.54 | 99.32 |
| Busulfan Level | Concentration (ng/mL) | Within-Run CV (%) | Between-Run CV (%) | Overall CV (%) | Overall Bias (%) |
|---|---|---|---|---|---|
| LQC | 25 | 9.70 | 1.08 | 9.76 | 1.04 |
| MQC | 4000 | 2.54 | 1.19 | 2.78 | 2.18 |
| HQC | 8000 | 2.87 | 0.88 | 2.97 | 7.58 |
| Patient | Laboratory | Measured Busulfan Concentration (ng/mL) | cAUC 4 (mg × h/L) | |||
|---|---|---|---|---|---|---|
| 5 min | 1 h | 2 h | 3 h | |||
| A | UMC 1 | 5216 | 3886 | 3186 | 2479 | 29.2 |
| FJCU 2 | 4836 | 3995 | 3226 | 2658 | 29.3 | |
| %Difference 3 | −7.86 | 2.73 | 1.24 | 6.73 | 0.34 | |
| B | UMC | 3946 | 2982 | 2318 | 1804 | 22.4 |
| FJCU | 3871 | 3182 | 2398 | 1925 | 23.9 | |
| %Difference | −1.94 | 6.29 | 3.34 | 6.29 | 6.28 | |
| C | UMC | 5127 | 3247 | 2458 | 1935 | 23.8 |
| FJCU | 4729 | 3124 | 2293 | 1735 | 22.4 | |
| %Difference | −8.42 | −3.94 | −7.20 | −11.53 | −6.25 | |
| No. | Underlying Diseases 1 | Age (yrs)/Gender | Conditioning Regimen 1 | BW 1-Guided Dose (mg) [26] | TDM 1-Guided Dose (mg) [25] | Difference 2 (%) | Mucositis | VOD 1 |
|---|---|---|---|---|---|---|---|---|
| 1 | AML, relapsed | 21/F | Flu + Bu | 804 | 617 | −5.2 | Grade 2 | None |
| 2 | LNS | 1.5/M | Flu + Bu | 178 | 142 | −20.3 | Grade 2 | None |
| 3 | AML, relapsed | 55/M | Flu + Bu + Clo | 876 | 1047 | 19.5 | Grade 1 | None |
| 4 | AML | 50/F | Flu + Bu | 696 | 762 | 9.5 | Grade 1 | None |
| 5 | ALD | 5/M | Flu + Bu | 400 | 300 | −25.0 | Grade 2 | None |
| 6 | AML | 16/M | Flu + Bu | 240 | 240 | 0.0 | Grade 3 | None |
| 7 | NB | 7/M | Bu + Mel | 360 | 420 | 16.7 | Grade 2 | Yes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, R.-L.; Fang, L.-H.; Yang, X.-Y.; El Amrani, M.; Uijtendaal, E.V.; Chen, Y.-F.; Ku, W.-C. Therapeutic Drug Monitoring of Busulfan in Patients Undergoing Hematopoietic Cell Transplantation: A Pilot Single-Center Study in Taiwan. Pharmaceuticals 2021, 14, 613. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14070613
Chen R-L, Fang L-H, Yang X-Y, El Amrani M, Uijtendaal EV, Chen Y-F, Ku W-C. Therapeutic Drug Monitoring of Busulfan in Patients Undergoing Hematopoietic Cell Transplantation: A Pilot Single-Center Study in Taiwan. Pharmaceuticals. 2021; 14(7):613. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14070613
Chicago/Turabian StyleChen, Rong-Long, Li-Hua Fang, Xin-Yi Yang, Mohsin El Amrani, Esther Veronique Uijtendaal, Yen-Fu Chen, and Wei-Chi Ku. 2021. "Therapeutic Drug Monitoring of Busulfan in Patients Undergoing Hematopoietic Cell Transplantation: A Pilot Single-Center Study in Taiwan" Pharmaceuticals 14, no. 7: 613. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14070613