
Higher Ventricular-Arterial Coupling Derived from Three-Dimensional Echocardiography Is Associated with a Worse Clinical Outcome in Systemic Sclerosis

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Echocardiography and Pressure-Volume Curve Parameters in SSc Patients and Controls
2.2. Echocardiography and Pressure-Volume Curve Parameters According to VAC Value
2.3. Echocardiography and Pressure-Volume Curve Parameters in dcSSc and lcSSc Patients
2.4. Correlations of Pressure-Volume Curve Parameters
2.5. Association between VAC and Other Clinical Variables
2.6. Factors Associated with VAC > 0.63
2.7. Major Adverse Cardiac Events
2.8. Risk Factors for MACEs in the Study Cohort
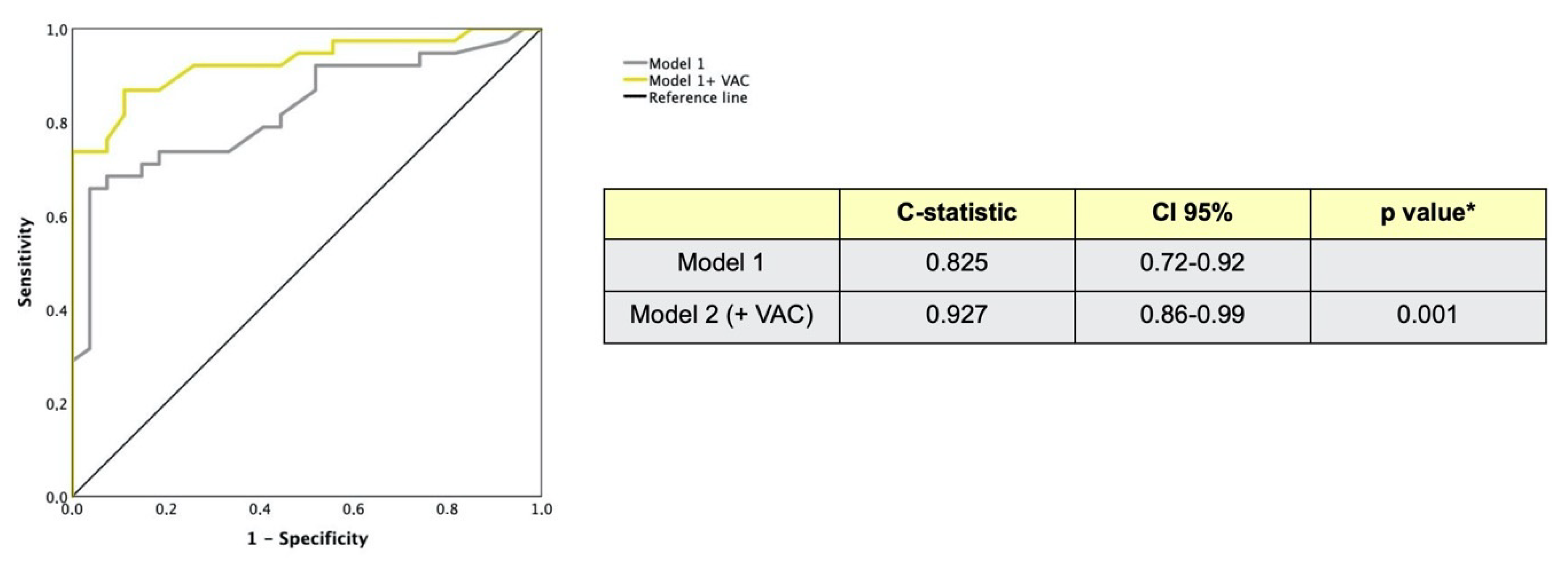
2.9. Incremental Value of VAC for Predicting Adverse Cardiac Events
2.10. Intra and Interobserver Reproducibility of VAC by 3D
2.11. Ventricular-Arterial Coupling by 2D and 3D Echo Modalities
3. Discussion
4. Materials and Methods
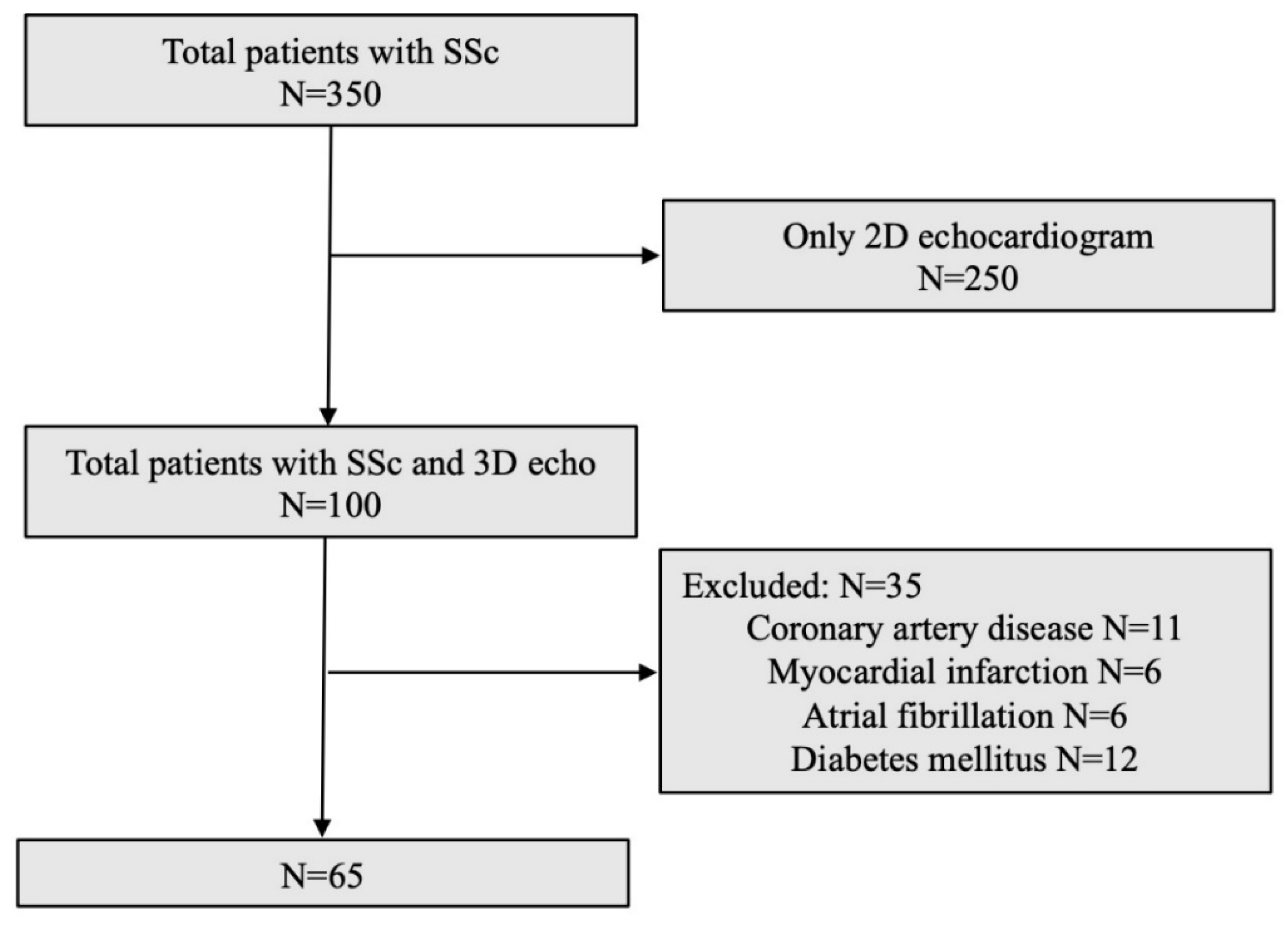
4.1. Study Population
- Inclusion and Exclusion Criteria
4.2. Echocardiography
4.2.1. Transthoracic Real-Time 3D Imaging
4.2.2. Left Ventricular Volume Measurements
- (1)
- Automatic slicing of LV full-volume data set. The end-diastolic frames needed for contour detection were automatically displayed in quad-view: apical four-, two-chamber, long-axis views and LV short-axis plane. Each longitudinal view was color-coded and indicated on the short-axis image at 60° between each plane. Both reference frames in the end-systole and end-diastole could be also manually selected, if necessary.
- (2)
- Alignment. Rapid manual alignment by pivoting and translating the four-chamber plane was first performed in order that the corresponding intersection line of all planes was placed in the middle of the LV cavity, crossing the LV apex and the center of mitral valve opening in each view. Aligning one plane automatically changed the others. Once LV central longitudinal axis was identified, accurate orientation of LV views was ensured by manual refinement of the angles between the LV planes on the LV short-axis view, in order to correspond to the defining anatomical landmarks of each view.
- (3)
- Left ventricular reference point identification. To subsequently identify a fitting geometric model, the software required manual input of only two single points in any of the three LV apical planes (on points on mitral annulus, and one at the apex) first in end-diastolic frames, and then for corresponding end-systolic frames.
- (4)
- Automated identification of endocardial border. The software automatically detected LV cavity endocardial border in 3D and provided the measured end-diastolic volume (LVEDV). Three additional short-axis views at different levels were displayed in order to facilitate verification of the accuracy of endocardial surface detection both in cross-section and in long-axis by rotating and translating active view plane. At this stage, LV borders could be manually adjusted, if unsatisfactory, by (dis)placing as many additional points as needed (manually corrected AutoLVQ), with secondary immediate automated refinement of boundary detection accordingly. This could be done on each of the six simultaneously displayed LV views, but also possible in between reference planes for LV with distorted shape. After completing steps 1–4 for end-diastolic views, only 3–4 sequence was required for end-systolic frames, since adjustments done in steps 1–2 were automatically carried out subsequently in end-systolic views.
- (5)
- Final quantitative analysis and data display. Using the initial contours in both end-systole and end-diastole, a corresponding dynamic surface-rendered LV cast was derived. Final data panel automatically displayed LVEDV, LVESV, LVEF, SV, cardiac output, and heart rate values. A volume–time plot was also provided.
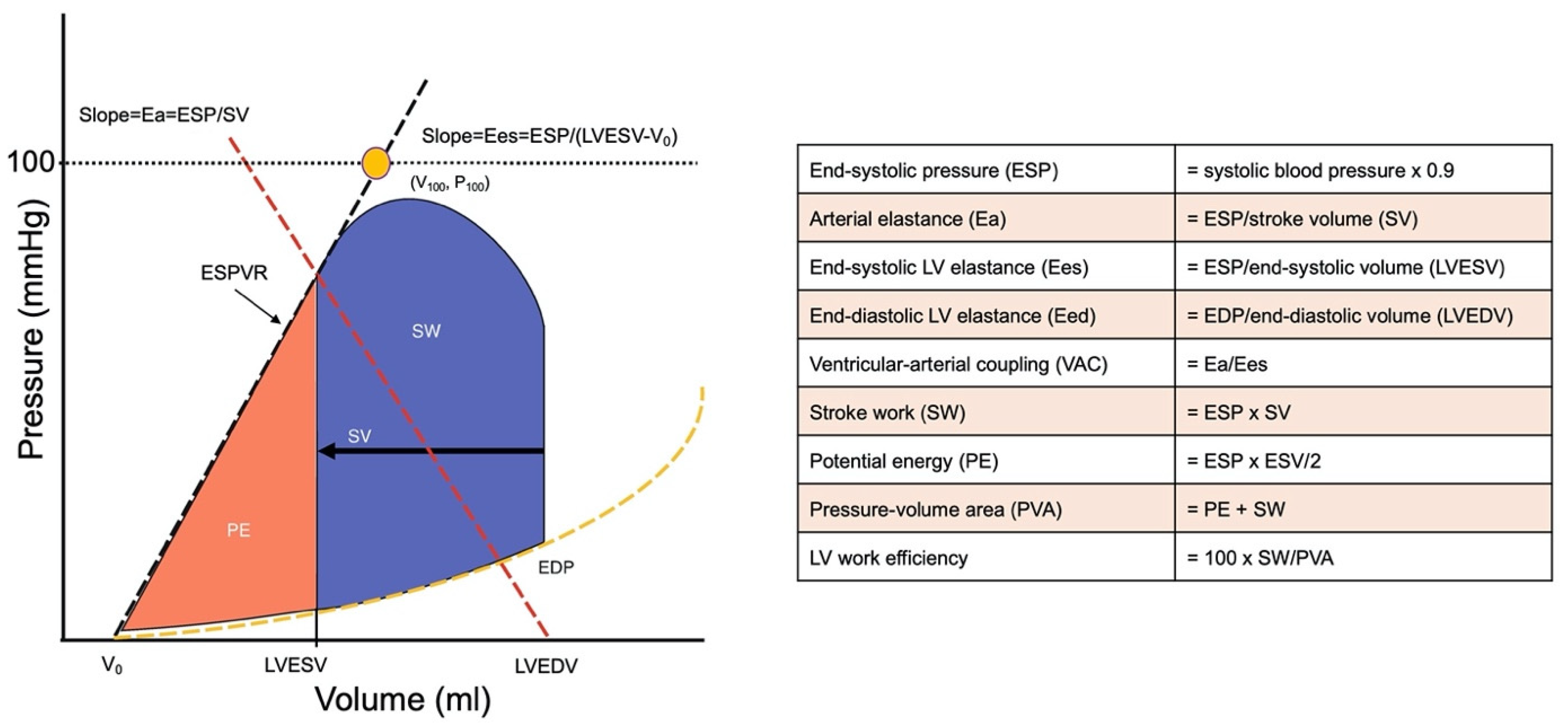
4.2.3. Variables Derived from Left Ventricular Pressure-Volume Relations
4.3. Primary Study Endpoint: Major Adverse Cardiovascular Events (MACEs) during Follow-up
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Denton, C.P.; Khanna, D. Systemic sclerosis. Lancet 2017, 390, 1685–1699. [Google Scholar] [CrossRef]
- Zanatta, E.; Famoso, G.; Boscain, F.; Montisci, R.; Pigatto, E.; Polito, P.; Schiavon, F.; Iliceto, S.; Cozzi, F.; Doria, A.; et al. Nailfold avascular score and coronary microvascular dysfunction in systemic sclerosis: A newsworthy association. Autoimmun. Rev. 2019, 18, 177–183. [Google Scholar] [CrossRef]
- Bissell, L.-A.; Yusof, Y.M.; Buch, M. Primary myocardial disease in scleroderma—A comprehensive review of the literature to inform the UK Systemic Sclerosis Study Group cardiac working group. Rheumatology 2016, 56, 882–895. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zanatta, E.; Colombo, C.; D’Amico, G.; D’Humières, T.; Lin, C.D.; Tona, F. Inflammation and Coronary Microvascular Dysfunction in Autoimmune Rheumatic Diseases. Int. J. Mol. Sci. 2019, 20, 5563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rangarajan, V.; Matiasz, R.; Freed, B.H. Cardiac complications of systemic sclerosis and management: Recent progress. Curr. Opin. Rheumatol. 2017, 29, 574–584. [Google Scholar] [CrossRef] [PubMed]
- Zanatta, E.; Polito, P.; Famoso, G.; LaRosa, M.; De Zorzi, E.; Scarpieri, E.; Cozzi, F.; Doria, A. Pulmonary arterial hypertension in connective tissue disorders: Pathophysiology and treatment. Exp. Biol. Med. 2019, 244, 120–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.J.; Park, J.-B.; Park, J.-H.; Cho, G.-Y. Global Longitudinal Strain to Predict Mortality in Patients with Acute Heart Failure. J. Am. Coll. Cardiol. 2018, 71, 1947–1957. [Google Scholar] [CrossRef]
- Asanoi, H.; Sasayama, S.; Kameyama, T. Ventriculoarterial coupling in normal and failing heart in humans. Circ. Res. 1989, 65, 483–493. [Google Scholar] [CrossRef] [Green Version]
- Ky, B.; French, B.; Khan, A.M.; Plappert, T.; Wang, A.; Chirinos, J.A.; Fang, J.C.; Sweitzer, N.K.; Borlaug, B.A.; Kass, D.A.; et al. Ventricular-Arterial Coupling, Remodeling, and Prognosis in Chronic Heart Failure. J. Am. Coll. Cardiol. 2013, 62, 1165–1172. [Google Scholar] [CrossRef] [Green Version]
- Milewska, A.; Minczykowski, A.; Krauze, T.; Piskorski, J.; Heathers, J.; Szczepanik, A.; Banaszak, A.; Guzik, P.; Wykretowicz, A. Prognosis after acute coronary syndrome in relation with ventricular–arterial coupling and left ventricular strain. Int. J. Cardiol. 2016, 220, 343–348. [Google Scholar] [CrossRef]
- Ikonomidis, I.; Aboyans, V.; Blacher, J.; Brodmann, M.; Brutsaert, D.L.; Chirinos, J.A.; De Carlo, M.; Delgado, V.; Lancellotti, P.; Lekakis, J.; et al. The role of ventricular–arterial coupling in cardiac disease and heart failure: Assessment, clinical implications and therapeutic interventions. A consensus document of the European Society of Cardiology Working Group on Aorta & Peripheral Vascular Diseases, European Association of Cardiovascular Imaging, and Heart Failure Association. Eur. J. Heart Fail. 2019, 21, 402–424. [Google Scholar] [CrossRef] [Green Version]
- Dorosz, J.L.; Lezotte, D.C.; Weitzenkamp, D.A.; Allen, L.A.; Salcedo, E.E. Performance of 3-Dimensional Echocardiography in Measuring Left Ventricular Volumes and Ejection Fraction: A systematic review and meta-analysis. J. Am. Coll. Cardiol. 2012, 59, 1799–1808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gayat, E.; Mor-Avi, V.; Weinert, L.; Yodwut, C.; Lang, R.M. Noninvasive quantification of left ventricular elastance and ventricu-lar-arterial coupling using three-dimensional echocardiography and arterial tonometry. Am. J. Physiol. Heart Circ. Physiol. 2011, 301, H1916–H1923. [Google Scholar] [CrossRef] [PubMed]
- Chirinos, J.A. Ventricular–arterial coupling: Invasive and non-invasive assessment. Artery Res. 2013, 7, 2–14. [Google Scholar] [CrossRef] [Green Version]
- Sunagawa, K.; Maughan, W.L.; Burkhoff, D. Left ventricular interaction with arterial load studied in isolated canine ventricle. Am. J. Physiol. 1983, 245 Pt 1, H773–H780. [Google Scholar] [CrossRef]
- Tennøe, A.H.; Murbræch, K.; Andreassen, J.C.; Fretheim, H.; Garen, T.; Gude, E.; Andreassen, A.; Aakhus, S.; Molberg, Ø; Hoffmann-Vold, A.-M. Left Ventricular Diastolic Dysfunction Predicts Mortality in Patients With Systemic Sclerosis. J. Am. Coll. Cardiol. 2018, 72, 1804–1813. [Google Scholar] [CrossRef]
- Hinchcliff, M.; Desai, C.S.; Varga, J.; Shah, S.J. Prevalence, prognosis, and factors associated with left ventricular diastolic dys-function in systemic sclerosis. Clin. Exp. Rheumatol. 2012, 30 (Suppl. 71), S30–S37. [Google Scholar] [PubMed]
- Butt, S.A.; Jeppesen, J.L.; Torp-Pedersen, C.; Sam, F.; Gislason, G.; Jacobsen, S.; Andersson, C. Cardiovascular Manifestations of Systemic Sclerosis: A Danish Nationwide Cohort Study. J. Am. Heart Assoc. 2019, 8, e013405. [Google Scholar] [CrossRef] [PubMed]
- Constans, J.; Germain, C.; Gosse, P.; Taillard, J.; Tiev, K.; Delevaux, I.; Mouthon, L.; Schmidt, C.; Granel, F.; Soria, P.; et al. Arterial stiffness predicts severe progression in systemic sclerosis: The ERAMS study. J. Hypertens. 2007, 25, 1900–1906. [Google Scholar] [CrossRef] [PubMed]
- Faccini, A.; Kaski, J.C.; Camici, P.G. Coronary microvascular dysfunction in chronic inflammatory rheumatoid diseases. Eur. Heart J. 2016, 37, 1799–1806. [Google Scholar] [CrossRef] [Green Version]
- Di Franco, M.; Paradiso, M.; Riccieri, V.; Basili, S.; Mammarella, A.; Valesini, G. Autonomic dysfunction and microvascular damage in systemic sclerosis. Clin. Rheumatol. 2007, 26, 1278–1283. [Google Scholar] [CrossRef] [PubMed]
- Valentini, G.; Huscher, D.; Riccardi, A.; Fasano, S.; Irace, R.; Messiniti, V.; Matucci-Cerinic, M.; Guiducci, S.; Distler, O.; Maurer, B.; et al. Vasodilators and low-dose acetylsalicylic acid are associated with a lower incidence of distinct primary myocardial disease manifestations in systemic sclerosis: Results of the DeSScipher inception cohort study. Ann. Rheum. Dis. 2019, 78, 1576–1582. [Google Scholar] [CrossRef] [PubMed]
- Zanatta, E.; Codullo, V.; Avouac, J.; Allanore, Y. Systemic sclerosis: Recent insight in clinical management. Jt. Bone Spine 2020, 87, 293–299. [Google Scholar] [CrossRef]
- Van Den Hoogen, F.; Khanna, D.; Fransen, J.; Johnson, S.R.; Baron, M.; Tyndall, A.; Matucci-Cerinic, M.; Naden, R.P.; Medsger, T.A., Jr.; Carreira, P.E.; et al. 2013 Classification Criteria for Systemic Sclerosis: An American College of Rheumatology/European League Against Rheumatism Collaborative Initiative. Arthritis Rheum. 2013, 65, 2737–2747. [Google Scholar] [CrossRef] [Green Version]
- Williams, B.; Mancia, G.; Spiering, W.; Rosei, E.A.; Azizi, M.; Burnier, M.; Clement, D.; Coca, A.; De Simone, G.; Dominiczak, A.; et al. 2018 Practice Guidelines for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension ESC/ESH Task Force for the Management of Arterial Hypertension. J. Hypertens. 2018, 36, 2284–2309. [Google Scholar] [CrossRef] [Green Version]
- Devereux, R.B.; Alonso, D.R.; Lutas, E.M.; Gottlieb, G.J.; Campo, E.; Sachs, I.; Reichek, N. Echocardiographic assessment of left ventricular hypertrophy: Comparison to necropsy findings. Am. J. Cardiol. 1986, 57, 450–458. [Google Scholar] [CrossRef]
- Galderisi, M.; Cosyns, B.; Edvardsen, T.; Cardim, N.; Delgado, V.; Di Salvo, G.; Donal, E.; Sade, L.E.; Ernande, L.; Garbi, M.; et al. Reviewers: This document was reviewed by members of the 2016–2018 EACVI Scientific Documents Committee. Standardization of adult transthoracic echocardiography reporting in agreement with recent chamber quantification, diastolic function, and heart valve disease recommendations: An expert consensus document of the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 1301–1310. [Google Scholar] [CrossRef] [Green Version]
- Nagueh, S.F.; Appleton, C.P.; Gillebert, T.; Marino, P.; Oh, J.K.; Smiseth, O.A.; Waggoner, A.D.; Flachskampf, F.A.; Pellikka, P.A.; Evangelisa, A. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography. Eur. Heart J. Cardiovasc. Imaging 2008, 10, 165–193. [Google Scholar] [CrossRef] [Green Version]
- Muraru, D.; Badano, L.; Piccoli, G.; Gianfagna, P.; Del Mestre, L.; Ermacora, D.; Proclemer, A. Validation of a novel automated border-detection algorithm for rapid and accurate quantitation of left ventricular volumes based on three-dimensional echocardiography. Eur. Hear. J. Cardiovasc. Imaging 2010, 11, 359–368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muraru, D.; Badano, L.; Peluso, D.; Bianco, L.D.; Casablanca, S.; Kocabay, G.; Zoppellaro, G.; Iliceto, S. Comprehensive Analysis of Left Ventricular Geometry and Function by Three-Dimensional Echocardiography in Healthy Adults. J. Am. Soc. Echocardiogr. 2013, 26, 618–628. [Google Scholar] [CrossRef]
- Ommen, S.R.; Nishimura, R.A.; Appleton, C.P.; Miller, F.A.; Oh, J.K.; Redfield, M.M.; Tajik, A.J. Clinical utility of Doppler echocardi-ography and tissue Doppler imaging in the estimation of left ventricular filling pressures. A comparative simultaneous Doppler-catheterization study. Circulation 2000, 102, 1788–1794. [Google Scholar] [CrossRef]
- Chantler, P.D.; Lakatta, E.; Najjar, S.S. Arterial-ventricular coupling: Mechanistic insights into cardiovascular performance at rest and during exercise. J. Appl. Physiol. 2008, 105, 1342–1351. [Google Scholar] [CrossRef] [Green Version]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D.; ESC Scientific Document Group. Fourth universal definition of myocardial infarction. Eur. Heart J. 2019, 40, 237–269. [Google Scholar] [CrossRef] [Green Version]
- Roffi, M.; Patrono, C.; Collet, J.-P.; Mueller, C.; Valgimigli, M.; Andreotti, F.; Bax, J.J.; Borger, M.; Brotons, C.; Chew, D.P.; et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2015, 37, 267–315. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 65) | VAC ≤ 0.63 (n = 34) | VAC > 0.63 (n = 31) | p Value | |
| Age, years | 56 ± 14 | 58 ± 13 | 53 ± 16 | 0.12 |
| Female, n (%) | 54 (83) | 29 (85) | 25 (81) | 0.61 |
| Body weight, Kg | 60 ± 11 | 62 ± 9 | 59 ± 10 | 0.81 |
| BMI, Kg/m2 | 25 ± 2 | 26 ± 3 | 25 ± 1 | 0.80 |
| Systolic blood pressure, mmHg | 126 ± 21 | 127 ± 20 | 125 ± 22 | 0.55 |
| Diastolic blood pressure, mmHg | 74 ± 10 | 70 ± 9 | 79 ± 6 | 0.69 |
| Hemoglobin, g/dL | 14 ± 0.8 | 15 ± 0.6 | 13 ± 0.2 | 0.71 |
| Creatinine, mg/dL | 0.98 ± 0.02 | 0.95 ± 0.01 | 1.02 ± 0.02 | 0.81 |
| Clinical Features | ||||
| Disease duration, years | 19 ± 11 | 16 ± 9 | 22 ± 12 | 0.03 |
| Diffuse cutaneous form, n (%) | 27 (41) | 10 (29) | 17 (55) | 0.03 |
| PAH, n (%) | 22 (34) | 6 (17) | 16 (47) | 0.57 |
| ILD on HRCT, n (%) | 37 (57) | 20 (59) | 17 (55) | 0.86 |
| Digital ulcers, n (%) | 39 (60) | 20 (58) | 19 (61) | 0.66 |
| Treatment, n (%) | ||||
| Prostanoid ev | 12 (18) | 4 (12) | 8 (26) | 0.40 |
| ET-1 inhibitors | 22 (34) | 14 (41) | 8 (26) | 0.33 |
| Immunosuppressants | 30 (46) | 18 (53) | 12 (39) | 0.28 |
| Echocardiographic Measurements | ||||
| LVEDD, mm | 44.9 ± 0.5 | 45.1 ± 0.6 | 44.7 ± 0.5 | 0.94 |
| IVS thickness, mm | 11.4 ± 1.2 | 9.9 ± 1.9 | 13.6 ± 1.6 | 0.28 |
| PW thickness, mm | 11.5 ± 1.3 | 9.6 ± 1.9 | 13.2 ± 1.6 | 0.21 |
| LV mass, g | 155 ± 59 | 151 ± 63 | 161 ± 53 | 0.33 |
| LVEDV, mL | 88 ± 26 | 85 ± 29 | 91 ± 24 | 0.24 |
| LVESV, mL | 33 ± 11 | 28 ± 10 | 38 ± 11 | <0.0001 |
| SV, mL | 55 ± 17 | 57 ± 19 | 52 ± 14 | 0.41 |
| LVEF (%) | 62 ± 5 | 67 ± 3 | 57 ± 2 | <0.0001 |
| Aorta, mm | 30 ± 0.3 | 30 ± 0.3 | 30 ± 0.4 | 0.69 |
| Left atrium, mm | 49.8 ± 9 | 47.7 ± 8 | 51.9 ± 9 | 0.12 |
| RVEDD, cm2 | 19 ± 5 | 18.2 ± 5 | 20 ± 5 | 0.08 |
| TAPSE, cm | 2.25 ± 0.5 | 2.31 ± 0.5 | 2.19 ± 0.5 | 0.24 |
| Peak E velocity, m/s | 0.86 ± 0.2 | 0.85 ± 0.1 | 0.88 ± 0.2 | 0.58 |
| Peak A velocity, m/s | 0.79 ± 0.2 | 0.84 ± 0.2 | 0.75 ± 0.2 | 0.13 |
| DT, ms | 199 ± 60 | 219 ± 62 | 179 ± 52 | 0.08 |
| E/A ratio | 1.14 ± 0.3 | 1.07 ± 0.3 | 1.21 ± 0.3 | 0.16 |
| E/e’ ratio | 10.2 ± 4.3 | 10.9 ± 4.7 | 9.3 ± 3.6 | 0.23 |
| PAP, mmHg | 34 ± 19 | 32 ± 16 | 37 ± 21 | 0.42 |
| Pressure-Volume Curve Relationships | ||||
| End-diastolic elastance, mmHg/mL | 0.21 (0.17–0.28) | 0.23 (0.17–0.29) | 0.21 (0.16–0.24) | 0.42 |
| Arterial elastance, mmHg/mL | 2.10 (1.82–2.80) | 2.10 (1.78–3.01) | 2.10 (1.87–2.80) | 0.69 |
| End-systolic elastance, mmHg/mL | 3.79 (2.87–5.30) | 4.43 (3.3–6.3) | 2.94 (2.53–4.12) | <0.0001 |
| Ventricular-arterial coupling | 0.57 (0.49–0.72) | 0.51 (0.45–0.53) | 0.73 (0.68–0.75) | <0.0001 |
| Stroke work, mmHg·mL | 6021 (4275–8424) | 6351 (4325–8991) | 5346 (4252–7695) | 0.38 |
| Potential energy, mmHg·mL | 1566 (1258–2413) | 1532 (1194–2103) | 1935 (1521–3087) | 0.001 |
| Pressure-volume area, mmHg·mL | 7659 (5798–11,102) | 8008 (5550–11,274) | 7281 (5798–10,410) | 0.86 |
| LV efficiency, % | 78 (73–80) | 79 (78–81) | 73 (72–74) | <0.0001 |
| dcSSc (n = 27) | lcSSc (n = 38) | p Value | |
| Age, years | 51 ± 14 | 59 ± 14 | 0.02 |
| Female, n (%) | 19 (70) | 35 (92) | 0.01 |
| Body weight, Kg | 60 ± 5 | 57 ± 2 | 0.52 |
| BMI, Kg/m2 | 26 ± 2 | 25 ± 2 | 0.61 |
| Systolic blood pressure, mmHg | 124 ± 22 | 128 ± 21 | 0.44 |
| Diastolic blood pressure, mmHg | 77 ± 8 | 72 ± 7 | 0.62 |
| Hemoglobin, g/dL | 13 ± 0.3 | 15 ± 0.1 | 0.58 |
| Creatinine, mg/dL | 0.98 ± 0.01 | 0.93 ± 0.03 | 0.34 |
| Clinical features | |||
| Disease duration, years | 14 ± 7 | 22 ± 12 | 0.005 |
| PAH, n (%) | 10 (37) | 12 (31) | 0.25 |
| ILD on HRCT, n (%) | 12(44) | 25 (66) | 0.01 |
| Digital ulcers, n (%) | 17 (62) | 22 (58) | 0.83 |
| Treatment, n (%) | |||
| Prostanoid ev | 7 (26) | 5 (13) | 0.21 |
| ET-1 inibithors | 9 (33) | 13 (34) | 0.44 |
| Immunosuppressants | 8 (29) | 22 (58) | 0.008 |
| Echocardiographic measurements | |||
| LVEDD, mm | 46 ± 0.6 | 44 ± 0.5 | 0.07 |
| IVS thickness, mm | 10 ± 0.2 | 12 ± 0.2 | 0.46 |
| PW thickness, mm | 10 ± 0.2 | 12 ± 0.3 | 0.83 |
| LV mass, g | 148 ± 51 | 166 ± 71 | 0.54 |
| LVEDV, mL | 101 ± 29 | 82 ± 21 | 0.004 |
| LVESV, mL | 39 ± 12 | 29 ± 9 | 0.001 |
| SV, mL | 62 ± 20 | 52 ± 13 | 0.03 |
| LVEF (%) | 60 ± 6 | 64 ± 5 | 0.01 |
| Aorta, mm | 29 ± 0.4 | 30 ± 0.3 | 0.12 |
| Left atrium, mm | 48 ± 0.8 | 50 ± 0.9 | 0.50 |
| RVEDD, cm2 | 19.9 ± 5 | 18.3 ± 5 | 0.32 |
| TAPSE, cm | 2.24 ± 0.5 | 2.30 ± 0.5 | 0.65 |
| Peak E velocity, cm/s | 0.90 ± 0.2 | 0.84 ± 0.2 | 0.53 |
| Peak A velocity, cm/s | 0.81 ± 0.2 | 0.78 ± 0.2 | 0.53 |
| DT, ms | 180 ± 54 | 211 ± 61 | 0.38 |
| E/A ratio | 1.19 ± 0.3 | 1.11 ± 0.2 | 0.44 |
| E/e’ ratio | 8.6 ± 2 | 10.7 ± 4 | 0.07 |
| PAP, mmHg | 32 ± 3 | 34 ± 3 | 0.75 |
| Pressure-volume curve relationships | |||
| End-diastolic elastance, mmHg/mL | 0.17 (0.13–0.22) | 0.23 (0.19–0.28) | 0.03 |
| Arterial elastance, mmHg/mL | 1.83 (1.53–2.20) | 2.21 (1.88–2.73) | 0.01 |
| End-systolic elastance, mmHg/mL | 2.90 (2.22–3.56) | 4.06 (3.12–5.49) | 0.001 |
| Ventricular-arterial coupling | 0.69 (0.52–0.74) | 0.52 (0.45–0.65) | 0.02 |
| Stroke work, mmHg·mL | 6284 (4045–8748) | 5805 (4680–8748 | 0.25 |
| Potential energy, mmHg·mL | 1863 (1493–2973) | 1552 (1215–2268 | 0.01 |
| Pressure-volume area, mmHg·mL | 8008 (5487–11,522) | 7357 (6138–11,016 | 0.12 |
| LV efficiency, % | 74 (72–78) | 79 (76–81) | 0.02 |
| b | 95% CI | p Value | |
|---|---|---|---|
| dcSSc | 0.342 | 0.020–0.184 | 0.01 |
| Prostanoid ev | 0.247 | (−0.008)–0.154 | 0.07 |
| Disease duration | 0.133 | (−0.002)–0.005 | 0.39 |
| Age at SSc diagnosis | −0.077 | (−0.004)–0.002 | 0.63 |
| Corrected R2 | 0.008 | ||
| No MACEs (n = 27) | MACEs (n = 38) | p Value | |
| Age, years | 55 ± 11 | 56 ± 16 | 0.66 |
| Female, n (%) | 22 (81) | 32 (84) | 0.77 |
| Body weight, Kg | 58 ± 3 | 59 ± 2 | 0.81 |
| BMI, Kg/m2 | 25 ± 1 | 26 ± 2 | 0.89 |
| Systolic blood pressure, mmHg | 133 ± 19 | 122 ± 22 | 0.04 |
| Diastolic blood pressure, mmHg | 75 ± 6 | 73 ± 7 | 0.49 |
| Hemoglobin, g/dL | 14 ± 0.3 | 15 ± 0.4 | 0.68 |
| Creatinine, mg/dL | 0.95 ± 0.04 | 0.96 ± 0.01 | 0.89 |
| Clinical features | |||
| Disease duration, years | 10 ± 1 | 16 ± 1 | 0.03 |
| dcSSc, n (%) | 9 (33) | 16 (42) | 0.43 |
| PAH, n (%) | 8 (30) | 14 (36) | 0.69 |
| ILD on HRCT, n (%) | 10 (37) | 27 (71) | 0.03 |
| Digital ulcers, n (%) | 16 (59) | 23 (60) | 0.75 |
| Treatment, n (%) | |||
| Prostanoid ev | 6 (22) | 6 (15) | 0.64 |
| ET-1 inibithors | 9 (33) | 13 (34) | 0.44 |
| Immunosuppressants | 6 (22) | 24 (63) | 0.007 |
| Echocardiographic measurements | |||
| LVEDD, mm | 43 ± 0.5 | 45 ± 0.5 | 0.13 |
| IVS thickness, mm | 10 ± 0.2 | 13 ± 0.2 | 0.18 |
| PW thickness, mm | 9 ± 0.2 | 12 ± 0.3 | 0.22 |
| LV mass, g | 143 ± 50 | 168 ± 66 | 0.17 |
| LVEDV, mL | 85 ± 24 | 91 ± 28 | 0.36 |
| LVESV, mL | 30 ± 10 | 35 ± 12 | 0.06 |
| SV, mL | 54 ± 15 | 55 ± 18 | 0.84 |
| LVEF (%) | 64 ± 5 | 60 ± 5 | 0.01 |
| Aorta, mm | 30 ± 0.3 | 29 ± 0.3 | 0.46 |
| Left atrium, mm | 52 ± 0.9 | 48 ± 0.8 | 0.13 |
| RVEDD, cm2 | 17.7 ± 3 | 20 ± 6 | 0.12 |
| TAPSE, cm | 2.35 ± 0.5 | 2.15 ± 0.5 | 0.23 |
| Peak E velocity, cm/s | 0.92 ± 0.2 | 0.82 ± 0.3 | 0.50 |
| Peak A velocity, cm/s | 0.80 ± 0.2 | 0.73 ± 0.2 | 0.41 |
| DT, ms | 189 ± 50 | 200 ± 55 | 0.36 |
| E/A ratio | 1.17 ± 0.3 | 1.13 ± 0.2 | 0.71 |
| E/e’ ratio | 11 ± 4 | 9.2 ± 4 | 0.24 |
| PAPs, mmHg | 29 ± 9 | 37 ± 23 | 0.14 |
| Pressure-volume curve relationships | |||
| End-diastolic elastance, mmHg/mL | 0.23 (0.18–0.27) | 0.19 (0.16–0.24) | 0.68 |
| Arterial elastance, mmHg/mL | 1.25 (1.96–2.84) | 1.95 (1.69–2.45) | 0.52 |
| End-systolic elastance, mmHg/mL | 4.50 (3.08–6.08) | 3.30 (2.70–3.89) | 0.01 |
| Ventricular-arterial coupling | 0.51 (0.45–0.64) | 0.63 (0.53–0.72) | 0.008 |
| Stroke work, mmHg·mL | 6588 (4781–8910) | 5400 (4230–6705) | 0.44 |
| Potential energy, mmHg·mL | 1521 (1257–2322) | 1748 (1527–2252) | 0.52 |
| Pressure-volume area, mmHg·mL | 8100 (6169–11,381) | 7380 (5620–9459) | 0.67 |
| LV efficiency, % | 79 (75–81) | 75 (73–78) | 0.01 |
| Univariate | Multivariable Model | |||
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Age > 60 years | 1.5 (1.2–2.9) | 0.20 | ||
| Female | 2.0 (1.2–5.2) | 0.15 | ||
| Disease duration, years | 1.03 (1.006–1.06) | 0.01 | ||
| Diffuse cutaneous form | 1.7 (1.1–3.3) | 0.13 | ||
| PAH | 1.0 (0.3–3.4) | 0.94 | ||
| ILD on HRCT | 1.2 (0.5–2.6) | 0.54 | ||
| Immunosuppressants | 1.7 (0.8–3.8) | 0.13 | ||
| Echocardiographic measurements | ||||
| LVEDV > 85 mL | 1.0 (0.5–1.9) | 0.97 | ||
| LVESV > 34 mL | 1.1 (0.6–2.2) | 0.61 | ||
| SV < 53 mL | 1.3 (0.7–2.6) | 0.31 | ||
| LVEF < 62% | 2.1 (1.0–4.1) | 0.02 | ||
| TAPSE < 2.1 cm | 1.6 (0.6–4.3) | 0.29 | ||
| E/e’ ratio > 9 | 2.1 (0.6–6.8) | 0.21 | ||
| PAP > 30 mmHg | 0.8 (0.4–1.6) | 0.56 | ||
| Pressure-volume curve relationships | ||||
| End-diastolic elastance > 0.21 mmHg/mL | 1.0 (0.3–3.2) | 0.86 | ||
| Arterial elastance > 2 mmHg/mL | 0.8 (0.4–1.5) | 0.56 | ||
| End-systolic elastance < 3.4 mmHg/mL | 1.4 (0.7–2.8) | 0.24 | ||
| Ventricular-arterial coupling > 0.63 | 2.4 (1.2–4.8) | 0.008 | 2.5 (1.13–5.7) | 0.01 |
| Stroke work < 5671 mmHg·mL | 1.5 (0.8–2.9) | 0.19 | ||
| Potential energy > 1621 mmHg·mL | 1.1 (0.6–2.2) | 0.62 | ||
| Pressure-volume area < 7498 mmHg·mL | 0.9 (0.4–1.7) | 0.75 | ||
| LV efficiency < 76% | 2.1 (1.09–4.1) | 0.02 | ||
| 2D Echo | 3D Echo | p Value | |
|---|---|---|---|
| Arterial elastance, mmHg/mL | 2.29 (1.93–2.70) | 2.04 (1.77–2.66) | 0.23 |
| End-systolic elastance, mmHg/mL | 4.17 (3.38–4.97) | 3.41 (2.57–4.50) | 0.02 |
| Ventricular-arterial coupling | 0.57 (0.44–0.66) | 0.62 (0.48–0.71) | 0.15 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tona, F.; Zanatta, E.; Montisci, R.; Muraru, D.; Beccegato, E.; De Zorzi, E.; Benvenuti, F.; Civieri, G.; Cozzi, F.; Iliceto, S.; et al. Higher Ventricular-Arterial Coupling Derived from Three-Dimensional Echocardiography Is Associated with a Worse Clinical Outcome in Systemic Sclerosis. Pharmaceuticals 2021, 14, 646. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14070646
Tona F, Zanatta E, Montisci R, Muraru D, Beccegato E, De Zorzi E, Benvenuti F, Civieri G, Cozzi F, Iliceto S, et al. Higher Ventricular-Arterial Coupling Derived from Three-Dimensional Echocardiography Is Associated with a Worse Clinical Outcome in Systemic Sclerosis. Pharmaceuticals. 2021; 14(7):646. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14070646
Chicago/Turabian StyleTona, Francesco, Elisabetta Zanatta, Roberta Montisci, Denisa Muraru, Elena Beccegato, Elena De Zorzi, Francesco Benvenuti, Giovanni Civieri, Franco Cozzi, Sabino Iliceto, and et al. 2021. "Higher Ventricular-Arterial Coupling Derived from Three-Dimensional Echocardiography Is Associated with a Worse Clinical Outcome in Systemic Sclerosis" Pharmaceuticals 14, no. 7: 646. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14070646