
Pharmacokinetics and Bioequivalence of Two Empagliflozin, with Evaluation in Healthy Jordanian Subjects under Fasting and Fed Conditions

 , , and
, , and 
Abstract
:1. Introduction
2. Results
2.1. Empagliflozin Analysis
2.2. Tolerability and Safety
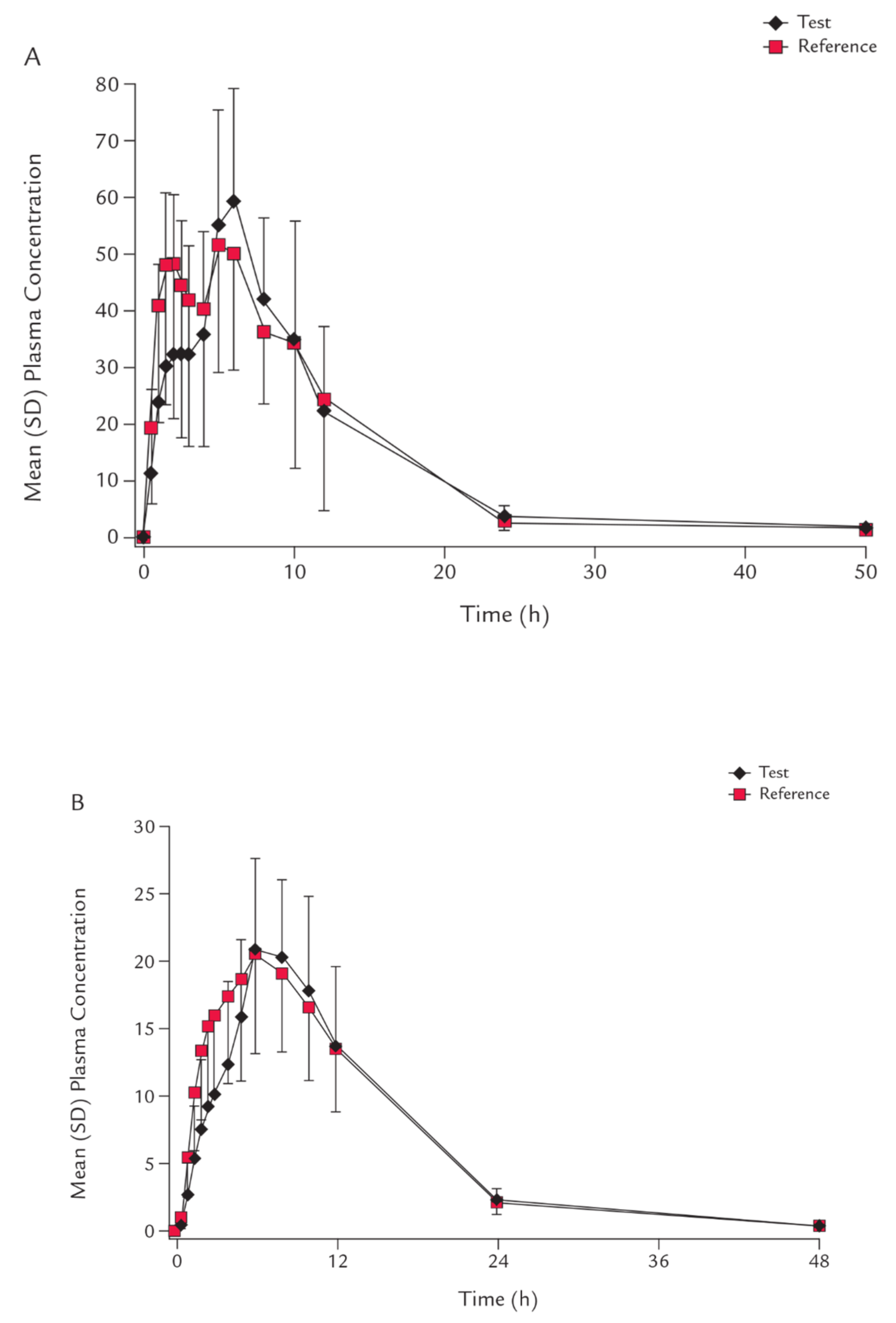
2.3. Pharmacokinetic Analysis
3. Discussion
4. Materials and Methods
4.1. Participants
4.2. Study Design
4.3. Subjects
4.4. Empagliflozin Dosing
4.5. Blood Sampling Plan
4.6. Assay Method
4.7. Pharmacokinetics and Statistical Analysis
4.8. Tolerability and Safety
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Scheen, A.J. Pharmacokinetic and Pharmacodynamic Profile of Empagliflozin, a Sodium Glucose Co-Transporter 2 Inhibitor. Clin. Pharmacokinet. 2014, 53, 213–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wright, E.M.; Loo, D.D.F.; Hirayama, B.A. Biology of Human Sodium Glucose Transporters. Physiol. Rev. 2011, 91, 733–794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeFronzo, R.A.; Norton, L.; Abdul-Ghani, M. Renal, metabolic and cardiovascular considerations of SGLT2 inhibition. Nat. Rev. Nephrol. 2016, 13, 11–26. [Google Scholar] [CrossRef] [PubMed]
- Chao, E.C. SGLT-2 Inhibitors: A New Mechanism for Glycemic Control. Clin. Diabetes 2014, 32, 4–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al Bawab, A.Q.; Al-Qerem, W.; Abusara, O.; Alkhatib, N.; Mansour, M.; Horne, R. What Are the Factors Associated with Non-adherence to Medications in Patients with Chronic Diseases? Healthcare 2021, 9, 1237. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.E.; Wright, E.E.; Shaefer, C.F. Empagliflozin: Role in Treatment Options for Patients with Type 2 Diabetes Mellitus. Diabetes Ther. 2016, 8, 33–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inzucchi, S.E.; Zinman, B.; Fitchett, D.; Wanner, C.; Ferrannini, E.; Schumacher, M.; Schmoor, C.; Ohneberg, K.; Johansen, O.E.; George, J.T.; et al. How does empagliflozin reduce car-diovascular mortality? Insights from a mediation analysis of the EMPA-REG OUTCOME trial. Diabetes Care 2018, 41, 356–363. [Google Scholar] [CrossRef] [Green Version]
- Stefani, M.; Singer, R.F.; Roberts, D.M. How to adjust drug doses in chronic kidney disease. Aust. Prescr. 2019, 42, 163–167. [Google Scholar] [CrossRef]
- Wanner, C.; Heerspink, H.J.; Zinman, B.; Inzucchi, S.E.; Koitka-Weber, A.; Mattheus, M.; Hantel, S.; Woerle, H.-J.; Broedl, U.C.; von Eynatten, M.; et al. Empagliflozin and Kidney Function Decline in Patients with Type 2 Diabetes: A Slope Analysis from the EMPA-REG OUTCOME Trial. J. Am. Soc. Nephrol. 2018, 29, 2755–2769. [Google Scholar] [CrossRef] [Green Version]
- Sizar, O.; Podder, V.; Talati, R. Empagliflozin. SA Pharm. J. 2021, 86, 45–47. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK532925/ (accessed on 8 December 2021).
- Neeland, I.J.; Salahuddin, U.; McGuire, D.K. A Safety Evaluation of Empagliflozin for the Treatment of Type 2 Diabetes. Expert Opin. Drug Saf. 2016, 15, 393–402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schorling, O.K.; Clark, D.; Zwiener, I.; Kaspers, S.; Lee, J.; Iliev, H. Pooled Safety and Tolerability Analysis of Empagliflozin in Patients with Type 2 Diabetes Mellitus. Adv. Ther. 2020, 37, 3463–3484. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Zhang, D.; Du, A.; Zhang, Y.; Zhang, Y.; Zhang, L.; Zang, S.; Liu, X.; Wang, Z.; Zhen, H.; et al. Pharmacokinetics, Safety, and Bioequivalence of Two Em-pagliflozin Formulations after Single Oral Administration under Fasting and Fed Conditions in Healthy Chinese Subjects: An Open-label Randomized Single-dose Two-sequence, Two-treatment, Two-period Crossover Study. Pharmacotherapy 2020, 40, 623–631. [Google Scholar] [CrossRef] [PubMed]
- Chawla, G.; Chaudhary, K.K. A complete review of empagliflozin: Most specific and potent SGLT2 inhibitor used for the treatment of type 2 diabetes mellitus. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 2001–2008. [Google Scholar] [CrossRef]
- FDA. Jardiance (Empagliflozin) Tablets, for Oral Use. Available online: www.fda.gov/medwatch (accessed on 8 December 2021).
- Ring, A.; Lang, B.; Kazaroho, C.; Labes, D.; Schall, R.; Schütz, H. Sample size determination in bioequivalence studies using statistical assurance. Br. J. Clin. Pharmacol. 2019, 85, 2369–2377. [Google Scholar] [CrossRef]
- Ndefo, U.A.; Anidiobi, N.O.; Basheer, E.; Eaton, A.T. Empagliflozin (Jardiance): A Novel SGLT2 Inhibitor for the Treatment of Type-2 Diabetes. Pharm. Ther. 2015, 40, 364–368. [Google Scholar]
- Levine, M.J. Empagliflozin for Type 2 Diabetes Mellitus: An Overview of Phase 3 Clinical Trials. Curr. Diabetes Rev. 2017, 13, 405–423. [Google Scholar] [CrossRef] [Green Version]
- DeFronzo, R.A. From the Triumvirate to the Ominous Octet: A New Paradigm for the Treatment of Type 2 Diabetes Mellitus. Diabetes 2009, 58, 773–795. [Google Scholar] [CrossRef] [Green Version]
- CHMP. Committee for Medicinal Products for Human Use (CHMP) Assessment Report. 2014. Available online: www.ema.europa.eu (accessed on 20 January 2022).
- Polidori, D.; Sha, S.; Mudaliar, S.; Ciaraldi, T.P.; Ghosh, A.; Vaccaro, N.; Farrel, K.; Rothenberg, P.; Henry, R.R. Canagliflozin lowers postprandial glucose and insulin by delaying intestinal glucose absorption in addition to increasing urinary glucose excretion: Results of a randomized, placebo-controlled study. Diabetes Care 2013, 36, 2154–2161. [Google Scholar] [CrossRef] [Green Version]
- Abdul-Ghani, M.A.; Norton, L.; DeFronzo, R.A. Role of Sodium-Glucose Cotransporter 2 (SGLT 2) Inhibitors in the Treatment of Type 2 Diabetes. Endocr. Rev. 2011, 32, 515–531. [Google Scholar] [CrossRef] [Green Version]
- Friedrich, C.; Metzmann, K.; Rose, P.; Mattheus, M.; Pinnetti, S.; Woerle, H.J. A Randomized, Open-Label, Crossover Study to Evaluate the Pharmacokinetics of Empagliflozin and Linagliptin After Coadministration in Healthy Male Volunteers. Clin. Ther. 2013, 35, A33–A42. [Google Scholar] [CrossRef] [PubMed]
- Abdul-Ghani, M.; Al Jobori, H.; Daniele, G.; Adams, J.; Cersosimo, E.; Triplitt, C.; DeFronzo, R.A. Inhibition of Renal Sodium–Glucose Cotransport With Empagliflozin Lowers Fasting Plasma Glucose and Improves β-Cell Function in Subjects With Impaired Fasting Glucose. Diabetes 2017, 66, 2495–2502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daems, C.; Welsch, S.; Boughaleb, H.; Vanderroost, J.; Robert, A.; Sokal, E.; Lysy, P.A. Early Treatment with Empagliflozin and GABA Improves β-Cell Mass and Glucose Tolerance in Streptozotocin-Treated Mice. J. Diabetes Res. 2019, 2019, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Häring, H.U.; Merker, L.; Seewaldt-Becker, E.; Weimer, M.; Meinicke, T.; Woerle, H.J.; Broedl, B.C. Empagliflozin as add-on to metformin plus sulfonylurea in patients with type 2 diabetes: A 24-week, randomized, double-blind, placebo-controlled trial. Diabetes Care 2013, 36, 3396–3404. [Google Scholar] [CrossRef] [Green Version]
- ICH Official Web Site. Available online: https://www.ich.org/page/efficacy-guidelines (accessed on 8 December 2021).
- Abu Dayyih, W.; Hamad, M.; Rahhal, A.; Mallah, E.; Abu Dayyih, A.; Zakaria, Z.; Arafat, T. Development and validation of liquid chromatography method for determination of glimepiride in presence of (Vimto®) soft drinks in rats: Application to pharmacokinetics studies. J. Pharm. Bioallied Sci. 2019, 11, 49–59. [Google Scholar] [CrossRef]
- Ahmad, R.; Hailat, M.; Jaber, M.; Alkhawaja, B.; Rasras, A.; Al-Shdefat, R.; Mallah, E.; Abu Dayyih, W. RP-HPLC method development for simultaneous estimation of empagliflozin, pioglitazone, and metformin in bulk and tablet dosage forms. Acta Pol. Pharm. Drug Res. 2021, 78, 305–315. [Google Scholar] [CrossRef]
- Abudayyih, W.; Mallah, E.; Al-Ani, I.H.; Arafat, T. Liquorice Beverage Effect On The Pharmacokinetic PaRameters Of Atorvastatin, Simvastatin, And Lovastatin By Liquid Chromatography-Mass Spectroscopy/Mass SpectroscopY. Asian J. Pharm. Clin. Res. 2016, 9, 174–179. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Parameters | Parent Reference Empagliflozin | |
|---|---|---|
| Test | Parent Reference | |
| Cmax μg/L | 75.06 (26.31) | 77.81 (21.23) |
| Tmax (h) | 4.77 (1.61) | 4.75 (1.619) |
| AUC0–ƚ (μg/L/h) | 516.80 (149.78) | 596.55 (154.29) |
| AUC0–∞ μg/L/h | 539.19 (141.16) | 527.05 (139.52) |
| t1/2 (h) | 4.49 (1.36) | 4.00 (1.12) |
| Vd (L) | 22.87 (8.99) | 19.07 (5.17) |
| Compound/Parameter | Test/Parent Reference (%) | 90% CI | p | |
|---|---|---|---|---|
| <80% | >125% | |||
| Parent Reference Empagliflozin | ||||
| In Cmax | 108.12 | 95.69–116.99 | 0.001 | 0.0029 |
| In AUC0–ƚ | 98.40 | 92.77–110.01 | <0.001 | <0.001 |
| In AUC0–∞ | 96.9 | 93.19–106.09 | <0.001 | <0.001 |
| Characteristic | Mean ± SD | Range |
|---|---|---|
| Age (Year) | 34.9 ± 1.7 | 22.7–57.3 |
| Weight (Kg) | 79.5 ± 9.8 | 66.7–92.4 |
| Height (cm) | 174.8 ± 8.8 | 161.7–189.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hailat, M.; Zakaraya, Z.; Al-Ani, I.; Meanazel, O.A.; Al-Shdefat, R.; Anwer, M.K.; Saadh, M.J.; Abu Dayyih, W. Pharmacokinetics and Bioequivalence of Two Empagliflozin, with Evaluation in Healthy Jordanian Subjects under Fasting and Fed Conditions. Pharmaceuticals 2022, 15, 193. https://0-doi-org.brum.beds.ac.uk/10.3390/ph15020193
Hailat M, Zakaraya Z, Al-Ani I, Meanazel OA, Al-Shdefat R, Anwer MK, Saadh MJ, Abu Dayyih W. Pharmacokinetics and Bioequivalence of Two Empagliflozin, with Evaluation in Healthy Jordanian Subjects under Fasting and Fed Conditions. Pharmaceuticals. 2022; 15(2):193. https://0-doi-org.brum.beds.ac.uk/10.3390/ph15020193
Chicago/Turabian StyleHailat, Mohammad, Zainab Zakaraya, Israa Al-Ani, Osaid Al Meanazel, Ramadan Al-Shdefat, Md. Khalid Anwer, Mohamed J. Saadh, and Wael Abu Dayyih. 2022. "Pharmacokinetics and Bioequivalence of Two Empagliflozin, with Evaluation in Healthy Jordanian Subjects under Fasting and Fed Conditions" Pharmaceuticals 15, no. 2: 193. https://0-doi-org.brum.beds.ac.uk/10.3390/ph15020193