
Pharmacogenetics of Metformin Transporters Suggests No Association with Therapeutic Inefficacy among Diabetes Type 2 Mexican Patients


 , ,
, ,
Abstract
:1. Introduction
2. Results
General Traits of Patient Groups According to Treatment
3. Discussion
4. Materials and Methods
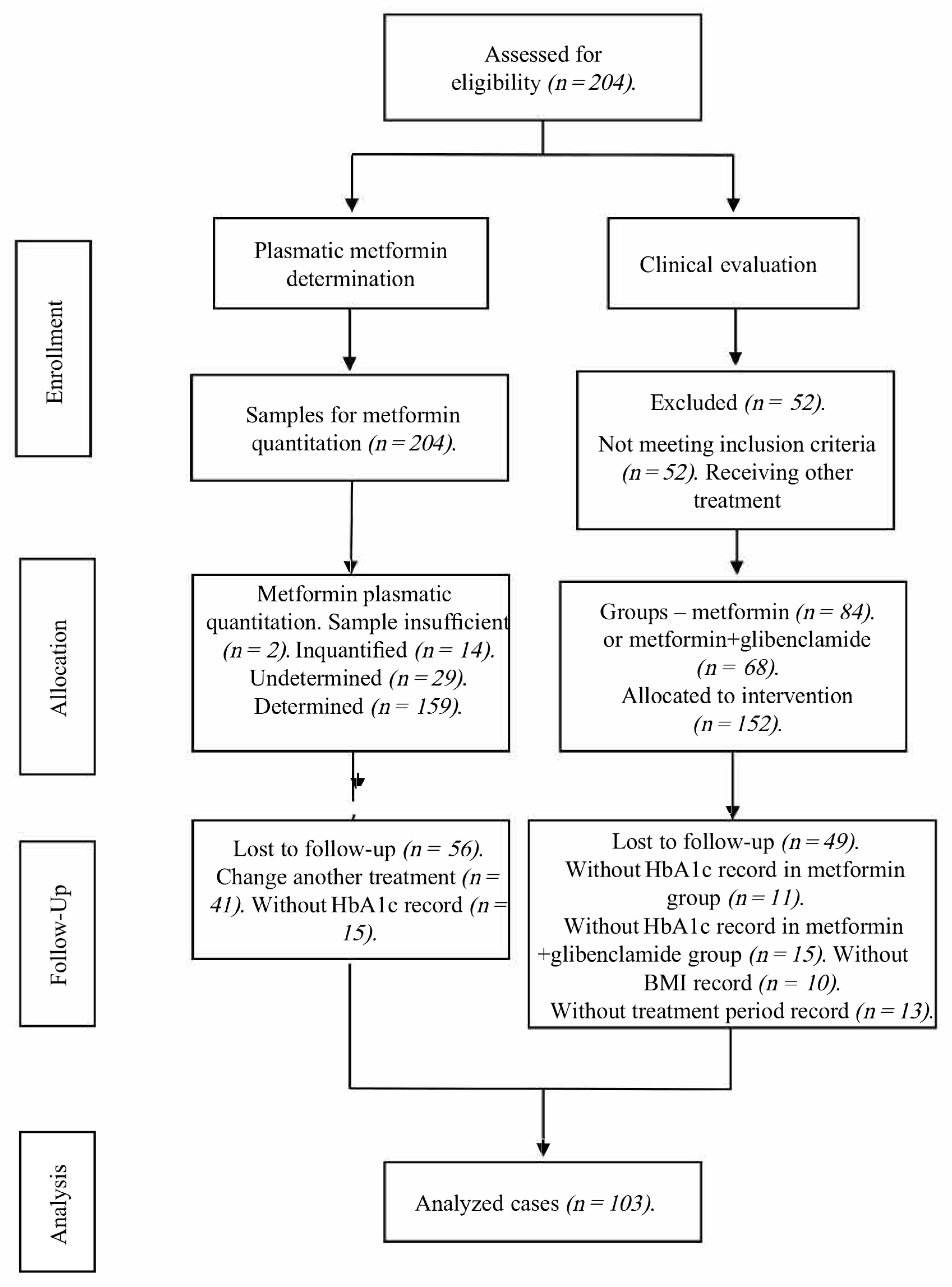
4.1. Study Design and Sample Description (DMT2 Patients)
4.2. Clinical Evaluation
4.3. Genotyping Procedure
4.4. Plasmatic Metformin Determination
4.5. Statistical Analyses
4.6. Genotypic and Allelic Frequency Analysis
4.7. Logistic Regression
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Loganadan, N.K.; Huri, H.Z.; Vethakkan, S.R.; Hussein, Z. Genetic markers predicting sulphonylurea treatment outcomes in type 2 diabetes patients: Current evidence and challenges for clinical implementation. Pharmacogenom. J. 2016, 16, 209–219. Available online: https://pubmed-ncbi-nlm-nih-gov.pbidi.unam.mx:2443/26810132/ (accessed on 2 May 2022). [CrossRef] [PubMed]
- Fowler, M.J. Microvascular and Macrovascular Complications of Diabetes. Clin. Diabetes 2008, 26, 77–82. Available online: https://diabetesjournals.org/clinical/article/26/2/77/1823/Microvascular-and-Macrovascular-Complications-of (accessed on 12 July 2021). [CrossRef] [Green Version]
- WHO. The Top 10 Causes of Death; WHO: Geneva, Switzerland, 2020; Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 2 May 2022).
- Guariguata, L.; Whiting, D.R.; Hambleton, I.; Beagley, J.; Linnenkamp, U.; Shaw, J.E. Global estimates of diabetes prevalence for 2013 and projections for 2035. Diabetes Res. Clin. Pract. 2014, 103, 137–149. Available online: https://pubmed-ncbi-nlm-nih-gov.pbidi.unam.mx:2443/24630390/ (accessed on 2 May 2022). [CrossRef] [PubMed]
- IDF. IDF Diabetes Atlas, 8th ed.; International Diabetes Federation: Brussels, Belgium, 2017. [Google Scholar]
- CENAPRESE. Declaratorias de Emergencia. 2018. Available online: http://www.cenaprece.salud.gob.mx/programas/interior/emergencias/declaratorias_emergencia.html (accessed on 2 May 2022).
- Secretaría de Salud. NORMA Oficial Mexicana NOM-015-SSA2-2010, Para la Prevención, Tratamiento y Control de la Diabetes Mellitus. DOF2010. Available online: http://www.dof.gob.mx/normasOficiales/4215/salud/salud.htm (accessed on 2 May 2022).
- Wang, Z.J.; Yin, O.Q.P.; Tomlinson, B.; Chow, M.S.S. OCT2 polymorphisms and in-vivo renal functional consequence: Studies with metformin and cimetidine. Pharmacogenet. Genom. 2008, 18, 637–645. Available online: https://pubmed-ncbi-nlm-nih-gov.pbidi.unam.mx:2443/18551044/ (accessed on 2 May 2022). [CrossRef] [PubMed]
- Chen, E.C.; Liang, X.; Yee, S.W.; Geier, E.G.; Stocker, S.; Chen, L.; Giacomini, K.M. Targeted Disruption of Organic Cation Transporter 3 Attenuates the Pharmacologic Response to Metformin. Mol. Pharmacol. 2015, 88, 75–83. Available online: https://pubmed-ncbi-nlm-nih-gov.pbidi.unam.mx:2443/25920679/ (accessed on 2 May 2022). [CrossRef] [Green Version]
- Seitz, T.; Stalmann, R.; Dalila, N.; Chen, J.; Pojar, S.; Pereira, J.N.D.S.; Krätzner, R.; Brockmöller, J.; Tzvetkov, M.V. Global genetic analyses reveal strong inter-ethnic variability in the loss of activity of the organic cation transporter OCT1. Genome Med. 2015, 7, 1–23. Available online: https://pubmed-ncbi-nlm-nih-gov.pbidi.unam.mx:2443/26157489/ (accessed on 2 May 2022). [CrossRef] [Green Version]
- Mato, E.P.M.; Guewo-Fokeng, M.; Essop, M.F.; Owira, P.M.O. Genetic polymorphisms of organic cation transporter 1 (OCT1) and responses to metformin therapy in individuals with type 2 diabetes: A systematic review. Medicine 2018, 97, e11349. Available online: https://pubmed-ncbi-nlm-nih-gov.pbidi.unam.mx:2443/29979413/ (accessed on 2 May 2022). [CrossRef]
- Becker, M.L.; Visser, L.E.; van Schaik, R.H.N.; Hofman, A.; Uitterlinden, A.G.; Stricker, B.H.C. Interaction between polymorphisms in the OCT1 and MATE1 transporter and metformin response. Pharmacogenet. Genom. 2010, 20, 38–44. Available online: https://pubmed-ncbi-nlm-nih-gov.pbidi.unam.mx:2443/19898263/ (accessed on 2 May 2022). [CrossRef]
- Umamaheswaran, G.; Praveen, R.G.; Damodaran, S.E.; Das, A.K.; Adithan, C. Influence of SLC22A1 rs622342 genetic polymorphism on metformin response in South Indian type 2 diabetes mellitus patients. Clin. Exp. Med. 2014, 15, 511–517. Available online: https://pubmed-ncbi-nlm-nih-gov.pbidi.unam.mx:2443/25492374/ (accessed on 2 May 2022). [CrossRef]
- Hemauer, S.J.; Patrikeeva, S.L.; Nanovskaya, T.N.; Hankins, G.D.; Ahmed, M.S. Role of human placental apical membrane transporters in the efflux of glyburide, rosiglitazone, and metformin. Am. J. Obstet. Gynecol. 2010, 202, 383.e1–383.e7. Available online: https://pubmed-ncbi-nlm-nih-gov.pbidi.unam.mx:2443/20350646/ (accessed on 2 May 2022). [CrossRef] [Green Version]
- Kim, H.G.; Hien, T.T.; Han, E.H.; Hwang, Y.P.; Choi, J.H.; Kang, K.W.; Kwon, K.; Kim, B.-H.; Kim, S.K.; Song, G.Y.; et al. Metformin inhibits P-glycoprotein expression via the NF-κB pathway and CRE transcriptional activity through AMPK activation. Br. J. Pharmacol. 2011, 162, 1096–1108. Available online: https://pubmed-ncbi-nlm-nih-gov.pbidi.unam.mx:2443/21054339/ (accessed on 2 May 2022). [CrossRef] [PubMed] [Green Version]
- Cuautle-Rodríguez, P.; Rodríguez-Rivera, N.; de Andrés, F.; Castillo-Nájera, F.; Llerena, A.; Molina-Guarneros, J.A. Frequency of CYP2C9 (*2, *3 and IVS8-109A>T) allelic variants, and their clinical implications, among Mexican patients with diabetes mellitus type 2 undergoing treatment with glibenclamide and metformin. Biomed. Rep. 2019, 10, 283–295. Available online: https://pubmed-ncbi-nlm-nih-gov.pbidi.unam.mx:2443/31086662/ (accessed on 2 May 2022). [PubMed] [Green Version]
- Marta, M.; Sánchez-Pozos, K.; Jaimes-Santoyo, J.; Monroy-Escutia, J.; Rivera- Santiago, C.; de los Ángeles Granados-Silvestre, M.; Ortiz-López, M.G. Pharmacogenetic Evaluation of Metformin and Sulphonylurea Response in Mexican Mestizos with Type 2 Diabetes. Curr. Drug Metab. 2020, 21, 291–300. Available online: https://pubmed-ncbi-nlm-nih-gov.pbidi.unam.mx:2443/32407269/ (accessed on 2 May 2022). [CrossRef] [PubMed]
- Jimenez-Sanchez, G. Developing a platform for genomic medicine in Mexico. Science 2003, 300, 295–296. Available online: https://pubmed-ncbi-nlm-nih-gov.pbidi.unam.mx:2443/12690190/ (accessed on 2 May 2022). [CrossRef]
- Guillausseau, P.-J.; Meas, T.; Virally, M.; Laloi Michelin, M.; Médeau, V.; Kevorkian, J.-P. Abnormalities in insulin secretion in type 2 diabetes mellitus. Diabetes Metab. 2008, 34, S43–S48. [Google Scholar] [CrossRef]
- Hatta, F.H.; Teh, L.K.; Helldén, A.; Hellgren, K.E.; Roh, H.K.; Salleh, M.Z.; Aklillu, E.; Bertilsson, L. Search for the molecular basis of ultra-rapid CYP2C9-catalysed metabolism: Relationship between SNP IVS8-109A>T and the losartan metabolism phenotype in Swedes. Eur. J. Clin. Pharmacol. 2012, 68, 1033–1042. [Google Scholar] [CrossRef]
- Ortega-Vázquez, A.; Dorado, P.; Fricke-Galindo, I.; Jung-Cook, H.; Monroy-Jaramillo, N.; E Martínez-Juárez, I.; Familiar-López, I.; Peñas-Lledó, E.; Llerena, A.; López-López, M. CYP2C9, CYP2C19, ABCB1 genetic polymorphisms and phenytoin plasma concentrations in Mexican-Mestizo patients with epilepsy. Pharmacogenom. J. 2015, 16, 286–292. Available online: https://pubmed-ncbi-nlm-nih-gov.pbidi.unam.mx:2443/26122019/ (accessed on 2 May 2022). [CrossRef]
- Clarke, L.; Fairley, S.; Zheng-Bradley, X.; Streeter, I.; Perry, E.; Lowy, E.; Tassé, A.-M.; Flicek, P. The international Genome sample resource (IGSR): A worldwide collection of genome variation incorporating the 1000 Genomes Project data. Nucleic Acids Res. 2016, 45, D854–D859. Available online: https://0-academic-oup-com.brum.beds.ac.uk/nar/article/45/D1/D854/2770649 (accessed on 2 May 2022). [CrossRef] [Green Version]
- Kahn, S.E.; Haffner, S.M.; Heise, M.A.; Herman, W.H.; Holman, R.R.; Jones, N.P.; Kravitz, B.G.; Lachin, J.M.; O’Neill, M.C.; Zinman, B.; et al. Glycemic durability of rosiglitazone, metformin, or glyburide monotherapy. N. Engl. J. Med. 2006, 355, 2427–2443. Available online: https://pubmed-ncbi-nlm-nih-gov.pbidi.unam.mx:2443/17145742/ (accessed on 2 May 2022). [CrossRef] [Green Version]
- Al-Eitan, L.N.; Almomani, B.A.; Nassar, A.M.; Elsaqa, B.Z.; Saadeh, N.A. Metformin Pharmacogenetics: Effects of SLC22A1, SLC22A2, and SLC22A3 Polymorphisms on Glycemic Control and HbA1c Levels. J. Pers. Med. 2019, 9, 17. Available online: https://pubmed-ncbi-nlm-nih-gov.pbidi.unam.mx:2443/30934600/ (accessed on 2 May 2022). [CrossRef] [Green Version]
- Yan, R.; Luo, J.; He, X.; Li, S. Association between ABC family variants rs1800977, rs4149313, and rs1128503 and susceptibility to type 2 diabetes in a Chinese Han population. J. Int. Med. Res. 2020, 48, 0300060520941347. Available online: https://pubmed-ncbi-nlm-nih-gov.pbidi.unam.mx:2443/32762489/ (accessed on 2 May 2022).
- Llaudó, I.; Colom, H.; Giménez-Bonafé, P.; Torras, J.; Caldés, A.; Sarrias, M.; Cruzado, J.M.; Oppenheimer, F.; Sánchez-Plumed, J.; Gentil, M.; et al. Do drug transporter (ABCB1) SNPs and P-glycoprotein function influence cyclosporine and macrolides exposure in renal transplant patients? Results of the pharmacogenomic substudy within the symphony study. Transpl. Int. 2012, 26, 177–186. Available online: https://pubmed-ncbi-nlm-nih-gov.pbidi.unam.mx:2443/23216707/ (accessed on 2 May 2022). [CrossRef] [PubMed]
- Ebid, A.H.I.M.; Ehab, M.; Ismail, A.; Soror, S.; Mahmoud, M.A. The influence of SLC22A1 rs622342 and ABCC8 rs757110 genetic variants on the efficacy of metformin and glimepiride combination therapy in Egyptian patients with type 2 diabetes. J. Drug Assess. 2019, 8, 115–121. Available online: https://pubmed-ncbi-nlm-nih-gov.pbidi.unam.mx:2443/31231590/ (accessed on 2 May 2022). [CrossRef] [PubMed] [Green Version]
- Msc, C.A.R.; Flores-Alfaro, E.; Suárez-Sánchez, F.; Cruz, M.; Valladares-Salgado, A.; Alarcón-Romero, L.D.C.; Msc, M.A.V.; Wacher-Rodarte, N.A.; Gómez-Zamudio, J.H. Altered Glycemic Control Associated With Polymorphisms in the SLC22A1 (OCT1) Gene in a Mexican Population With Type 2 Diabetes Mellitus Treated With Metformin: A Cohort Study. J. Clin. Pharmacol. 2019, 59, 1384–1390. Available online: https://pubmed-ncbi-nlm-nih-gov.pbidi.unam.mx:2443/31012983/ (accessed on 2 May 2022).
- Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2020. Diabetes Care 2020, 43, S14–S31. Available online: https://pubmed-ncbi-nlm-nih-gov.pbidi.unam.mx:2443/31862745/ (accessed on 12 July 2021). [CrossRef] [PubMed] [Green Version]
- WHO. Physical Status: The Use of and Interpretation of Anthropometry, Report of a WHO Expert Committee. 1995. Available online: https://apps.who.int/iris/handle/10665/37003 (accessed on 12 July 2021).
- Secretaría de Salud. NORMA Oficial Mexicana NOM-177-SSA1-2013 [Internet]. DOF2013. Available online: http://www.dof.gob.mx/nota_detalle.php?codigo=5314833&fecha=20/09/2013 (accessed on 12 July 2021).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Metformin n = 59 (57.3%) | Metformin + Glibenclamide n = 44 (42.7%) | p = |
|---|---|---|---|
| Age (years) | 55.8 ± 10.83 | 53.11 ± 11.28 | 0.225 t |
| Weight (Kg) | 78.83 ± 16.73 | 71.72 ± 13.39 | 0.022 *,t |
| Sex “n” (%) Female | 42 (71.2%) | 31 (70.5%) | 0.936 Xi |
| Male | 17 (28.8 %) | 13 (29.5%) | |
| Treatment period (years) | 3 (1.25–7.5) | 7.5 (3–14.5) | <0.001 *,U |
| BMI | 31.92 ± 6.29 | 29.23 ± 4.81 | 0.020 *,t |
| Normal weight Overweight Obesity type I II III | 4 (6.8%) 20 (33.9%) 18 (30.5%) 12 (20.3%) 5 (8.5%) | 7 (15.9%) 19 (43.2%) 8 (18.2%) 8 (18.2%) 2 (4.5%) | 0.074 U |
| Metformin plasmatic concentration ng/mL | 290.75 (107.69–815.02) | 570.91 (170.58–1043.33) | 0.203 U |
| Glucose mg/dL | 115.5 (102–157) | 192.5 (139–238.5) | <0.001 *,U |
| HbA1c % | 6.4 (5.9–7.3) | 9.05 (7.55–10.9) | <0.001 *,U |
| control | 43 (72.9%) | 5 (11.4%) | <0.001 *,Xi |
| non-control | 16 (27.1%) | 39 (88.6%) | |
| Total cholesterol mg/dL | 175.05 ± 39.46 | 182.1 ± 33.78 | 0.360 t |
| control | 41 (70.7%) | 27 (67.5%) | 0.736 Xi |
| non-control | 17 (29.3%) | 13 (32.5%) | |
| LDL cholesterol mg/dL | 91.41 ± 32.43 | 103.69 ± 29.89 | 0.105 t |
| HDL cholesterol mg/dL | 41 (34.55–45.75) | 41.5 (36.8–47.2) | 0.806 U |
| Triglycerides mg/dL | 194 (131–223.5) | 157 (131–252) | 0.925 U |
| control | 16 (29.1%) | 17 (44.7%) | 0.121 Xi |
| non-control | 39 (70.9%) | 21 (55.3%) | |
| Glomerular filtration rate (MDRD-4) | 93.4 (87.81–115.16) | 103.4 (89.23–131.7) | 0.329 U |
| Metformin dose mg/day | 1700 (850–1700) | 2125 (1700–2550) | 0.001 *,U |
| Daily metformin dose mg/kg/day | 19.25 (11.92–25.84) | 29.2 (21.55–34.21) | <0.001 *,U |
| Gen | SNP | Genotype Frequencies | Allelic Frequencies | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SLC22A1 (OCT1) | rs72552763 | GAT/GAT | del/GAT | del/del | GAT | del | * p = | ||||||
| 0.427 (44) | 0.447 (46) | 0.126 (13) | 0.650 | 0.349 | 0.984 | ||||||||
| rs622342 | AA | AC | CC | A | C | ||||||||
| 0.398 (41) | 0.388 (40) | 0.214 (22) | 0.592 | 0.407 | 0.138 | ||||||||
| SLC22A2 (OCT2) | rs316019 | C/C | C/A | A/A | C | A | |||||||
| 0.913 (94) | 0.078 (8) | 0.01 (1) | 0.951 | 0.048 | 0.265 | ||||||||
| SLC22A3 (OCT3) | rs2076828 | C/C | C/G | G/G | C | G | |||||||
| 0.757 (78) | 0.204 (21) | 0.039 (4) | 0.859 | 0.140 | 0.280 | ||||||||
| ABCB1 | rs1128503 | CC | CT | TT | C | T | |||||||
| 0.262(27) | 0.437 (45) | 0.301 (31) | 0.48 | 0.519 | 0.447 | ||||||||
| rs1045642 | CC | CT | TT | C | T | ||||||||
| 0.35 (36) | 0.447 (46) | 0.204 (21) | 0.556 | 0.443 | 0.674 | ||||||||
| rs2032582 | GG | GT | TT | TA | GA | G | T | A | |||||
| 0.330 (34) | 0.417 (43) | 0.165 (17) | 0.019 (2) | 0.058 (6) | 0.573 | 0.387 | 0.039 | 0.879 | |||||
| CYP2C9 | rs1799853 (*2) | *1/*1 | *1/*2 | *1/*3 | *2/*3 | *1 | *2 | *3 | |||||
| rs1057910 (*3) | 0.825 (85) | 0.097 (10) | 0.068 (7) | 0.01 (1) | 0.907 | 0.053 | 0.038 | 0.848 | |||||
| rs1934969 (IVS8-109A > T) | A/T | A/T | T/T | A | T | ||||||||
| 0.661 (69) | 0.328 (27) | 0.041 (7) | 0.81 | 0.19 | 0.197 | ||||||||
| Gene | SNP | Genotype | Control (n = 48) HbA1c < 7 (%) | Non-Control (n = 55) HbA1c > 7 (%) | * p = |
|---|---|---|---|---|---|
| SLC22A1 (OCT1) | rs72552763 | GAT/GAT | 23 (47.9%) | 21 (38.2%) | 0.392 |
| del/GAT | 18 (37.5%) | 28 (50.9%) | |||
| del/del | 7 (14.6%) | 6 (10.9%) | |||
| rs622342 | A/A | 22 (45.8%) | 19 (34.5%) | 0.324 | |
| A/C | 15 (31.3%) | 25 (45.5%) | |||
| C/C | 11 (22.9%) | 11 (20%) | |||
| SLC22A2 (OCT2) | rs316019 | C/C | 43 (89.6%) | 51 (92.7%) | 0.425 |
| A/C | 5 (10.4%) | 3 (5.5%) | |||
| A/A | 0 (0%) | 1 (1.8%) | |||
| SLC22A3 (OCT3) | rs2076828 | C/C | 40 (83.3%) | 38 (69.1%) | 0.232 |
| C/G | 7 (14.6%) | 14 (25.5%) | |||
| G/G | 1 (2.1%) | 3 (5.5%) | |||
| ABCB1 | rs1128503 | C/C | 13 (27.1%) | 14 (25.5%) | 0.710 |
| C/T | 19 (39.6%) | 26 (47.3%) | |||
| T/T | 16 (33.3%) | 15 (27.3%) | |||
| rs2032582 | G/G | 17 (35.4%) | 17 (31.5%) | 0.662 | |
| G/T | 21 (43.8%) | 22 (40.7%) | |||
| T/T | 8 (16.7%) | 9 (16.7%) | |||
| T/A | 0 (0%) | 2 (3.7%) | |||
| G/A | 2 (4.2%) | 4 (7.4%) | |||
| rs1045642 | C/C | 15 (31.3%) | 21 (38.2%) | 0.520 | |
| C/T | 21 (43.8%) | 25 (45.5%) | |||
| T/T | 12 (25%) | 9 (16.4%) | |||
| CYP2C9 | rs1799853 rs1057910 | *1/*1 | 39 (81.3%) | 46 (83.6%) | 0.261 |
| *1/*2 | 7 (14.6%) | 3 (5.5%) | |||
| *1/*3 | 2 (4.2%) | 5 (9.1%) | |||
| *2/*3 | 0 | 1 (1.8%) | |||
| rs1934969 | A/A | 30 (62.5%) | 39 (70.9%) | 0.643 | |
| A/T | 14 (29.2%) | 13 (23.6%) | |||
| T/T | 4 (8.3%) | 3 (5.5%) |
| Gene | SNP | Genotype | Control (ng/mL) Median (IQR 25–75%) (n) | Non-Control (ng/mL) Median (IQR 25–75%) (n) | * p = |
|---|---|---|---|---|---|
| SLC22A1 (OCT1) | rs72552763 | GAT/GAT | 376.9 (133.4–763) (17) | 481.7 (185.9–971) (17) | 0.812 |
| del/GAT | 137.1 (66.47 687.4) (14) | 790.6 (228.8–1030.2) (27) | 0.115 | ||
| del/del | 139.1 (107.6–264.3) (6) | 785.6 (70.2–1642.7) (5) | 0.792 | ||
| * p = | 0.358 | 0.820 | |||
| rs622342 | A/A | 339.7 (129.8–700.9) (16) | 526.3 (169–1000.9) (16) | 0.616 | |
| A/C | 102.6 (57.2–737.7) (12) | 725 (254.5–969) (23) | 0.141 | ||
| C/C | 157.8 (132.1–687.4) (9) | 795.4 (70.2–1642.7) (10) | 0.604 | ||
| * p = | 0.381 | 0.821 | |||
| SLCA22A2 (OCT2) | rs316019 | C/C | 151.9 (105.2–687.4) (34) | 648.2 (183.3–1030.9) (46) | 0.098 |
| A/C | 302.5 (283.4–589.5) (3) | 804 (507.4–1025.8) (3) | 0.827 | ||
| A/A | (0) | (0) | - | ||
| * p = | 0.373 | 0.646 | |||
| SLC22A3 (OCT3) | rs2076828 | C/C | 144.3 (105.2–763) (30) | 685.7 (126.9–1030.2) (35) | 0.286 |
| C/G | 320.6 (157.8–618.8) (6) | 611 (386.1–880.8) (11) | 0.122 | ||
| G/G | 1321.6 (1) | 1030.9 (723.9–1336.8) (3) | - | ||
| * p = | 0.734 | 0.634 | |||
| ABCB1 | rs1128503 | C/C | 763 (264.3–1321.6) (9) | 526.3 (146–1004.7) (14) | 0.450 |
| C/T | 139.8 (90.3–649.7) (16) | 844.7 (481.7–1095.1) (22) | 0.011 * | ||
| T/T | 150.1 (113.9–402.6) (12) | 219.8 (70.2–530.7) (13) | 0.624 | ||
| * p = | 0.233 | 0.066 | |||
| rs2032582 | G/G | 496.5 (107.6–815) (13) | 788.1 (146–1055.6) (16) | 0.539 | |
| G/T | 181.1 (118.2–768.5) (17) | 491.4 (185.9–884.2) (18) | 0.041 * | ||
| T/T | 526.3 (142.5–752.7) (6) | 210.8 (72.9–869.7) (9) | 0.955 | ||
| T/A | (0) | 2286 (1348.7–3223.2) (2) | - | ||
| G/A | 105.2 (1) | 428.9 (199.6–1158.2) (3) | - | ||
| * p = | 0.584 | 0.733 | |||
| rs1045642 | C/C | 700.9 (133.4–1321.6) (10) | 785.6 (233.3–1017.8) (19) | 0.891 | |
| C/T | 116.3 (85.7–157.8) (17) ¥ | 530.7 (185.9–1095.1) (21) | 0.002 * | ||
| T/T | 414.4 (264.3–876.5) (10) | 290.5 (72.9–901.4) (9) | 0.568 | ||
| * p = | 0.014 κ | 0.692 | |||
| CYP2C9 | rs1799853 (*2) rs1057910 (*3) | *1/*1 | 200.68 (111.5–815) (29) | 725 (210.8–1030.9) (41) | 0.222 |
| *1/*2 | 278.9 (92.9–481.5) (7) | 107.8 (89–126.9) (3) | 0.425 | ||
| *2/*2 | (0) | (0) | - | ||
| *1/*3 | 157.85 (1) | 712.3 (376.7–2078.2) (4) | - | ||
| *2/*3 | (0) | 1705.38 (1) | - | ||
| *3/*3 | (0) | (0) | - | ||
| * p = | 0.753 | 0.077 | |||
| rs1934969 | A/A | 151.9 (106.4–649.7) (24) | 530.7 (210.8–1088.9) (33) | 0.051 | |
| A/T | 451.6 (80.5–1321.3) (10) | 785.6 (290.5–971) (13) | 0.620 | ||
| T/T | 133.4 (122.5–474.2) (3) | 22.817 (15.9–539.2) (3) | 0.513 | ||
| * p = | 0.770 | 0.374 |
| Gene | SNP | Genotype | Metformin (%HbA1c) Median (IQR 25–75%) (n) | Metformin + Glibenclamide (%HbA1c) Median (IQR 25–75%) (n) | * p = |
|---|---|---|---|---|---|
| SLC22A1 (OCT1) | rs72552763 | GAT/GAT | 6 (5.7–6.8) (28) ¥ | 9.4 (8.5–11.2) (16) | <0.001 * |
| del/GAT | 6.5 (6.2–9.2) (22) | 8.3 (7.3–10.4) (24) | 0.023 * | ||
| del/del | 6.5 (6.4–6.8) (9) | 10.1 (8.4–11.3) (4) | 0.045 * | ||
| p = | 0.022 κ | 0.221 | |||
| rs622342 | A/A | 6 (5.8–6.5) (25) | 9.4 (8.5–11.2) (16) | <0.001 * | |
| A/C | 6.4 (6.1–7.7) (19) | 8.7 (7.5–10.9) (21) | 0.001 * | ||
| C/C | 6.8 (6.4–9.3) (15) ¥ | 8.3 (7.1–9.8) (7) | 0.397 | ||
| p = | 0.009 κ | 0.332 | |||
| SLCA22A2 (OCT2) | rs316019 | C/C | 6.4 (5.9–7.2) (52) | 9 (7.6–10.9) (42) | <0.001 * |
| A/C | 6.2 (5.8–8.1) (6) | 8.4 (7.3–9.5) (2) | 0.180 | ||
| A/A | 8.1 (1) | (0) | - | ||
| p = | 0.818 | 0.573 | |||
| SLC22A3 (OCT3) | rs2076828 | C/C | 6.3 (5.9–6.9) (46) | 8.9 (7.5–10.5) (32) | <0.001 * |
| C/G | 6.4 (5.9–8.2) (11) | 9.9 (7.7–12.2) (10) | 0.022 * | ||
| G/G | 8.6 (6.6–10.7) (2) | 8.6 (7.3–9.9) (2) | 1.000 | ||
| p = | 0.336 | 0.452 | |||
| ABCB1 | rs1128503 | C/C | 6.1 (5.7–6.3) (15) | 10.1 (9–11.8) (12) | <0.001 * |
| C/T | 6.6 (6.2–8.4) (28) ¥ | 8.5 (7.5 -10.5) (17) | 0.007 * | ||
| T/T | 6.2 (5.9–6.7) (16) | 8.5 (7.3–10.1) (15) | 0.007 * | ||
| * p = | 0.021 κ | 0.056 | |||
| rs2032582 | G/G | 6.1 (5.7–6.3) (19) | 9.9 (8.2–11.1) (15) | <0.001 * | |
| G/T | 6.8 (6.4–8.1) (27) ¥ | 8.6 (7–9.4) (16) | 0.058 | ||
| T/T | 6.2 (6–6.3) (9) | 8.8 (7.4–10.1) (8) | 0.002 * | ||
| T/A | 14.9 (1) | 8.3 (1) | - | ||
| G/A | 6.5 (6.2–7.4) (3) | 11 (10.9–13.3) (3) | 0.050 | ||
| * p = | 0.009 κ | 0.156 | |||
| rs1045642 | C/C | 6.1 (5.9–6.6) (17) | 9.9 (7.9–10.9) (19) | <0.001 * | |
| C/T | 6.5 (6.1–8.1) (29) | 8.7 (7.3–9.4) (17) | 0.024 * | ||
| T/T | 6.2 (6.1–6.4) (13) | 8.8 (8–10.1) (8) | 0.001 * | ||
| * p = | 0.160 | 0.511 | |||
| CYP2C9 | rs1799853 (*2) rs1057910 (*3) | *1/*1 | 6.4 (5.9–7.3) (50) | 9.2 (7.5–10.7) (35) | <0.001 * |
| *1/*2 | 6.2 (5.5–6.5) (6) | 8.8 (6.7–10.7) (4) | 0.165 | ||
| *2/*2 | (0) | (0) | - | ||
| *1/*3 | 8.3 (7.2–8.4) (3) | 8.3 (7–10.6) (4) | 1.000 | ||
| *2/*3 | (0) | 11 (1) | - | ||
| * p = | 0.352 | 0.811 | |||
| rs1934969 | A/A | 6.4 (6.1–7.6) (35) | 8.7 (7.5–11) (34) | <0.001 * | |
| A/T | 6.5 (5.9–7.3) (19) | 9.4 (8–10.2) (8) | 0.003 * | ||
| T/T | 6.2 (6–6.2) (5) | 10.4 (10.3–10.5) (2) | 0.051 | ||
| * p = | 0.808 | 0.611 |
| Gene (SNP) | Control | No Control | OR (IC95%) | p-Value |
|---|---|---|---|---|
| OCT1 (rs72552763) | ||||
| GAT/GAT | 23 | 21 | 1.0 (ref) | |
| del/GAT | 18 | 28 | 1.704 (0.738–3.935) | 0.212 |
| del/del | 7 | 6 | 0.939 (0.272–3.246) | 0.920 |
| Dominant genotype model | ||||
| Del/del + del/GAT vs. GAT/GAT | 25/23 | 34/21 | 1.490 (0.679–3.266) | 0.320 |
| aDel/del + del/GAT vs. GAT/GAT | 25/23 | 34/21 | 1.207 (0.395–3.691) | 0.741 |
| OCT1 (rs622342) | ||||
| AA | 22 | 19 | 1.0 (ref.) | |
| AC | 15 | 25 | 1.930 (0.795–4.685) | 0.146 |
| CC | 11 | 11 | 1.158 (0.411–3.266) | 0.782 |
| Dominant genotype model | ||||
| CC + AC vs. AA | 26/22 | 36/19 | 1.603 (0.724–3.549) | 0.244 |
| aCC + AC vs. AA | 26/22 | 36/19 | 1.914 (0.603–6.080) | 0.271 |
| ABCB1 (rs1128503) | ||||
| Genotype | ||||
| CC | 13 | 14 | 1.0 (ref.) | |
| CT | 19 | 26 | 1.271 (0.487–3.316) | 0.624 |
| TT | 16 | 15 | 0.871 (0.310–2.445) | 0.792 |
| Dominant genotype model | ||||
| TT + CT vs. CC | 35/13 | 41/14 | 1.088 (0.451–2.621) | 0.851 |
| aTT + CT vs. CC | 35/13 | 41/14 | 1.817 (0.494–6.691) | 0.369 |
| ABCB1 (rs2032582) | ||||
| GG | 17 | 17 | 1.0 (ref.) | |
| GT | 21 | 22 | 1.048 (0.426–2.576) | 0.919 |
| TT | 8 | 9 | 1.125 (0.351–3.609) | 0.843 |
| TA | 0 | 2 | - | |
| GA | 2 | 4 | 2 (0.322–12.414) | 0.457 |
| Dominant genotype model | ||||
| GA + TA + TT+ GT vs. GG | 31/17 | 37/17 | 1.194 (0.523–2.722) | 0.674 |
| aGA + TA + TT+ GT vs. GG | 31/17 | 37/17 | 1.933 (0.582–6.425) | 0.282 |
| OCT 1 | |||||
| Variable | B | Standard Error | p-Value | OR (IC95%) | |
| Age (years) | −0.066 | 0.030 | 0.026 * | 0.936 (0.883–0.992) | |
| BMI ≥ 25 Kg/m2 | 1.953 | 0.967 | 0.043 * | 7.049 (1.059–46.895) | |
| rs72552763 GAT | rs622342 A | −0.642 | 0.593 | 0.279 | 0.526 (0.165–1.683) |
| Treatment (metformin + glibenclamide) | 2.893 | 0.653 | <0.001 * | 18.05 (5.015–64.969) | |
| Treatment period (years) | 0.232 | 0.072 | 0.001 * | 1.261 (1.094–1.452) | |
| ABCB1 | |||||
| Age (years) | −0.072 | 0.030 | 0.017 * | 0.930 (0.877–0.987) | |
| BMI ≥ 25 Kg/m2 | 2.211 | 1.088 | 0.042 * | 9.128 (1.083–76.966) | |
| rs1128503 C | rs2032582 G | −1.026 | 0.738 | 0.164 | 0.358 (0.084–1.522) |
| Treatment (metformin + glibenclamide) | 2.887 | 0.666 | <0.001 * | 17.933 (4.858–66.205) | |
| Treatment period (years) | 0.240 | 0.072 | 0.001 * | 1.271 (1.105–1.462) | |
| Gene | SNP | Genotype | Metformin (mg/kg/day) Median (IQR 25–75%) (n) | Metformin + Glibenclamide (mg/kg/day) Median (IQR 25–75%) (n) | p = |
|---|---|---|---|---|---|
| ABCB1 | rs1128503 | C/C | 18.78 (12.28–25.41) (14) | 26.98 (18.19–34.53) (12) | 0.057 |
| C/T | 19.12 (11.92–26.08) (27) | 29.27 (23.16–35.31) (17) | 0.001 * | ||
| T/T | 20 (11.78–24.42) (15) | 29.7 (16.66–31.95) (14) | 0.127 | ||
| p = | 0.969 | 0.971 | |||
| rs2032582 | G/G | 16.48 (11.93–23.28) (17) | 26.98 (21.35–32.04) (15) | 0.011 * | |
| G/T | 19.78 (12.99–27.33) (26) | 24.35 (15.34–32.83) (16) | 0.170 | ||
| T/T | 20 (16.48–21.19) (9) | 31.95 (29.77–29.15) (7) | 0.064 | ||
| T/A | 27.82 (1) | 29.51 (1) | - | ||
| G/A | 10.24 (10.02–10.85) (3) | 32.11 (28.44–34.03) (3) | 0.050 | ||
| p = | 0.118 | 0.356 | |||
| rs1045642 | C/C | 12.29 (11–22.65) (16) | 27.86 (23.21–33.71) (19) | 0.001 * | |
| C/T | 19.56 (12.93–27.39) (27) | 25.55 (16.66–30.35) (17) | 0.152 | ||
| T/T | 20 (14.5–21.19) (13) | 37.5 (29.77–39.71) (7) | 0.019 * | ||
| p = | 0.298 | 0.156 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ortega-Ayala, A.; Rodríguez-Rivera, N.S.; Andrés, F.d.; LLerena, A.; Pérez-Silva, E.; Espinosa-Sánchez, A.G.; Molina-Guarneros, J.A. Pharmacogenetics of Metformin Transporters Suggests No Association with Therapeutic Inefficacy among Diabetes Type 2 Mexican Patients. Pharmaceuticals 2022, 15, 774. https://0-doi-org.brum.beds.ac.uk/10.3390/ph15070774
Ortega-Ayala A, Rodríguez-Rivera NS, Andrés Fd, LLerena A, Pérez-Silva E, Espinosa-Sánchez AG, Molina-Guarneros JA. Pharmacogenetics of Metformin Transporters Suggests No Association with Therapeutic Inefficacy among Diabetes Type 2 Mexican Patients. Pharmaceuticals. 2022; 15(7):774. https://0-doi-org.brum.beds.ac.uk/10.3390/ph15070774
Chicago/Turabian StyleOrtega-Ayala, Adiel, Nidia Samara Rodríguez-Rivera, Fernando de Andrés, Adrián LLerena, Eliseo Pérez-Silva, Adriana Guadalupe Espinosa-Sánchez, and Juan Arcadio Molina-Guarneros. 2022. "Pharmacogenetics of Metformin Transporters Suggests No Association with Therapeutic Inefficacy among Diabetes Type 2 Mexican Patients" Pharmaceuticals 15, no. 7: 774. https://0-doi-org.brum.beds.ac.uk/10.3390/ph15070774