
Head-to-Head Comparison between Peptide-Based Radiopharmaceutical for PET and SPECT in the Evaluation of Neuroendocrine Tumors: A Systematic Review
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results and Discussion
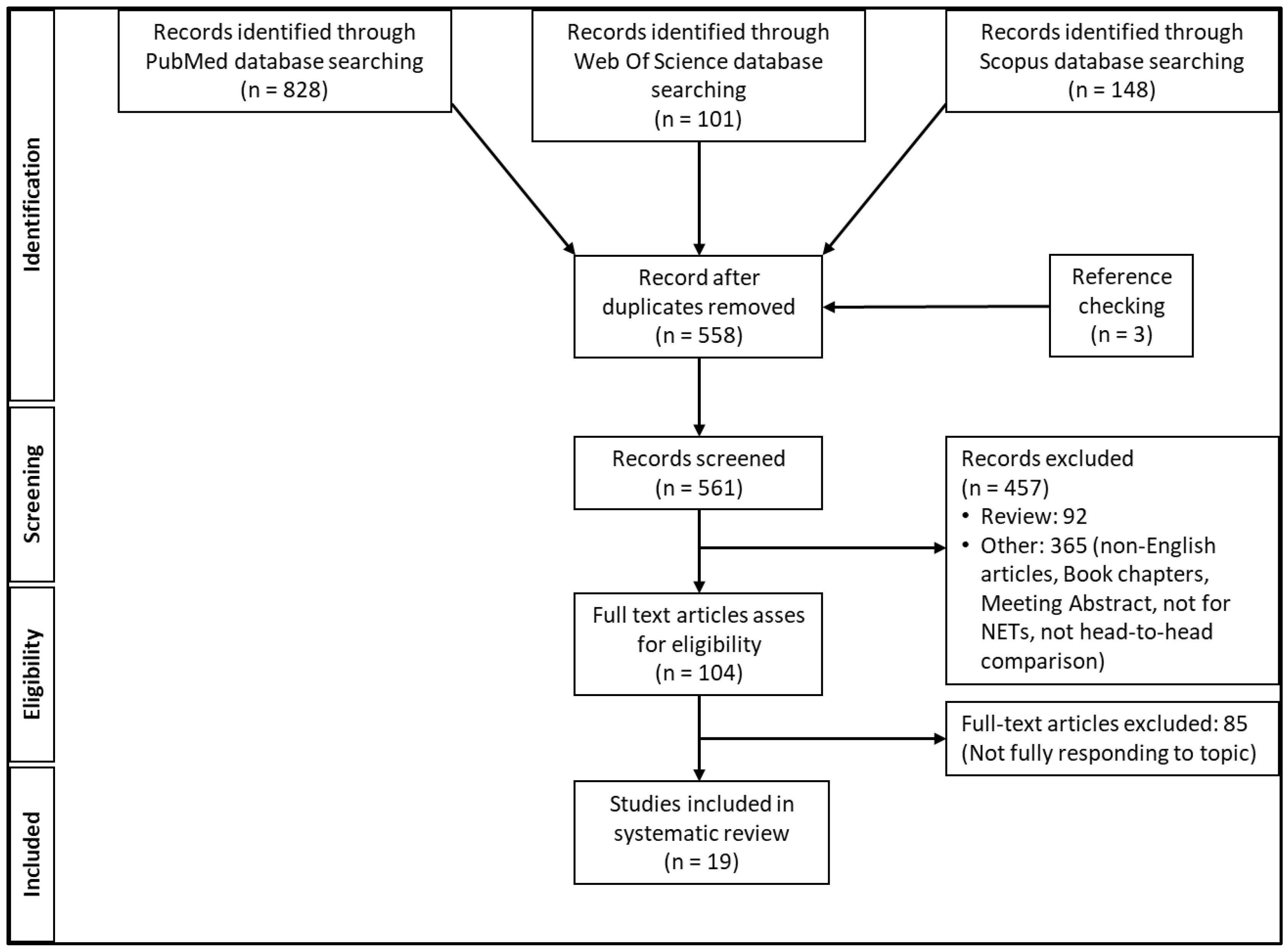
3.1. Literature Search Analysis
3.2. Comparative Perfomances
3.3. The Theragnostic Role of Radiopharmaceuticals for NET
4. Discussion and Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Desai, H.; Borges-Neto, S.; Wong, T.Z. Molecular Imaging and Therapy for Neuroendocrine Tumors. Curr. Treat. Options Oncol. 2019, 20, 78. [Google Scholar] [CrossRef] [PubMed]
- Werner, R.; Bluemel, C.; Lassmann, M.; Kudlich, T.; Higuchi, T.; Lopci, E.; Allen-Auerbach, M.; Colletti, P.M.; Rubello, D.; Zatelli, M.C.; et al. SPECT- and PET-Based Patient-Tailored Treatment in Neuroendocrine Tumors. Clin. Nucl. Med. 2015, 40, e271–e277. [Google Scholar] [CrossRef] [PubMed]
- Kjaer, A.; Knigge, U. Use of radioactive substances in diagnosis and treatment of neuroendocrine tumors. Scand. J. Gastroenterol. 2015, 50, 740–747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dearling, J.L.J.; van Dam, E.M.; Harris, M.J.; Packard, A.B. Detection and therapy of neuroblastoma minimal residual disease using [64/67Cu]Cu-SARTATE in a preclinical model of hepatic metastases. EJNMMI Res. 2021, 11, 20. [Google Scholar] [CrossRef] [PubMed]
- Cullinane, C.; Jeffery, C.M.; Roselt, P.D.; van Dam, E.M.; Jackson, S.; Kuan, K.; Jackson, P.; Binns, D.; van Zuylekom, J.; Harris, M.J.; et al. Peptide receptor radionuclide therapy with 67Cu-CuSarTATE is highly efficacious against a somatostatin-positive neuroendocrine tumor model. J. Nucl. Med. 2020, 61, 1800–1805. [Google Scholar] [CrossRef] [PubMed]
- Hicks, R.J.; Jackson, P.; Kong, G.; Ware, R.E.; Hofman, M.S.; Pattison, D.A.; Akhurst, T.A.; Drummond, E.; Roselt, P.; Callahan, J.; et al. 64Cu-sartaTE PET imaging of patients with neuroendocrine tumors demonstrates high tumor uptake and retention, potentially allowing prospective dosimetry for peptide receptor radionuclide therapy. J. Nucl. Med. 2019, 60, 777–785. [Google Scholar] [CrossRef] [Green Version]
- Cives, M.; Strosberg, J. Radionuclide Therapy for Neuroendocrine Tumors. Curr. Oncol. Rep. 2017, 19, 9. [Google Scholar] [CrossRef]
- Bodei, L.; Cremonesi, M.; Paganelli, G. Yttrium-based therapy for neuroendocrine tumors. PET Clin. 2014, 9, 71–82. [Google Scholar] [CrossRef]
- Bangard, M.; Behe, M.; Guhlke, S.; Otte, R.; Bender, H.; Maecke, H.R.; Biersack, H.J. Detection of somatostatin receptor-positive tumours first results in patients and comparison with 111In-DTPA-D-Phe1-octreotide. Eur. J. Nucl. Med. 2000, 27, 628–637. [Google Scholar] [CrossRef]
- Decristoforo, C.; Mather, S.J.; Cholewinski, W.; Donnemiller, E.; Riccabona, G.; Moncayo, R. Original article a new 99m Tc-labelled radiopharmaceutical for imaging somatostatin receptor-positive tumours: First clinical results and intra-patient comparison with 111In-labelled octreotide derivatives. Eur. J. Nucl. Med. 2000, 27, 1318–1325. [Google Scholar] [CrossRef]
- Hofmann, M.; Maecke, H.; Börner, A.; Weckesser, E.; Schöffski, P.; Oei, M.; Schumacher, J.; Henze, M.; Heppeler, A.; Meyer, J.; et al. Biokinetics and imaging with the somatostatin receptor PET radioligand 68Ga-DOTATOC: Preliminary data. Eur. J. Nucl. Med. 2001, 28, 1751–1757. [Google Scholar] [CrossRef] [PubMed]
- Kowalski, J.; Henze, M.; Schuhmacher, J.; Mäcke, H.R.; Hofmann, M.; Haberkorn, U. Evaluation of positron emission tomography imaging using [68Ga]-DOTA-D Phe1-Tyr3- octreotidein comparison to [111In]-DTPAOC SPECT. First results in patients with neuroendocrine tumors. Mol. Imaging Biol. 2003, 5, 42–48. [Google Scholar] [CrossRef]
- Gabriel, M.; Decristoforo, C.; Donnemiller, E.; Ulmer, H.; Rychlinski, C.W.; Mather, S.J.; Moncayo, R. An intrapatient comparison of 99mTc-EDDA/HYNIC-TOC with 111In-DTPA-octreotide for diagnosis of somatostatin receptor-expressing tumors. J. Nucl. Med. 2003, 44, 708–716. [Google Scholar]
- Buchmann, I.; Henze, M.; Engelbrecht, S.; Eisenhut, M.; Runz, A.; Schäfer, M.; Schilling, T.; Haufe, S.; Herrmann, T.; Haberkorn, U. Comparison of 68Ga-DOTATOC PET and 111In-DTPAOC (Octreoscan) SPECT in patients with neuroendocrine tumours. Eur. J. Nucl. Med. Mol. Imaging 2007, 34, 1617–1626. [Google Scholar] [CrossRef] [PubMed]
- Gabriel, M.; Decristoforo, C.; Kendler, D.; Dobrozemsky, G.; Heute, D.; Uprimny, C.; Kovacs, P.; von Guggenberg, E.; Bale, R.; Virgolini, I.J. 68Ga-DOTA-Tyr3-octreotide PET in neuroendocrine tumors: Comparison with somatostatin receptor scintigraphy and CT. J. Nucl. Med. 2007, 48, 508–518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Müssig, K.; Öksüz, M.; Dudziak, K.; Ueberberg, B.; Wehrmann, M.; Horger, M.; Schulz, S.; Häring, H.; Pfannenberg, C.; Bares, R.; et al. Association of somatostatin receptor 2 immunohistochemical expression with [111In]-DTPA octreotide scintigraphy and [68Ga]-DOTATOC PET/CT in neuroendocrine tumors. Horm. Metab. Res. 2010, 42, 599–606. [Google Scholar] [CrossRef] [PubMed]
- Srirajaskanthan, R.; Kayani, I.; Quigley, A.M.; Soh, J.; Caplin, M.E.; Bomanji, J. The role of 68Ga-DOTATATE PET in patients with neuroendocrine tumors and negative or equivocal findings on 111In-DTPA-octreotide scintigraphy. J. Nucl. Med. 2010, 51, 875–882. [Google Scholar] [CrossRef] [Green Version]
- Krausz, Y.; Freedman, N.; Rubinstein, R.; Lavie, E.; Orevi, M.; Tshori, S.; Salmon, A.; Glaser, B.; Chisin, R.; Mishani, E.; et al. 68Ga-DOTA-NOC PET/CT imaging of neuroendocrine tumors: Comparison with 111In-DTPA-octreotide (OctreoScan®). Mol. Imaging Biol. 2011, 13, 583–593. [Google Scholar] [CrossRef]
- Hofman, M.S.; Kong, G.; Neels, O.C.; Eu, P.; Hong, E.; Hicks, R.J. High management impact of Ga-68 DOTATATE (GaTate) PET/CT for imaging neuroendocrine and other somatostatin expressing tumours. J. Med. Imaging Radiat. Oncol. 2012, 56, 40–47. [Google Scholar] [CrossRef]
- Van Binnebeek, S.; Vanbilloen, B.; Baete, K.; Terwinghe, C.; Koole, M.; Mottaghy, F.M.; Clement, P.M.; Mortelmans, L.; Bogaerts, K.; Haustermans, K.; et al. Comparison of diagnostic accuracy of 111In-pentetreotide SPECT and 68Ga-DOTATOC PET/CT: A lesion-by-lesion analysis in patients with metastatic neuroendocrine tumours. Eur. Radiol. 2016, 26, 900–909. [Google Scholar] [CrossRef]
- Pfeifer, A.; Knigge, U.; Binderup, T.; Mortensen, J.; Oturai, P.; Loft, A.; Berthelsen, A.K.; Langer, S.W.; Rasmussen, P.; Elema, D.; et al. 64Cu-DOTATATE PET for neuroendocrine tumors: A prospective head-to-head comparison with 111In-DTPA-octreotide in 112 patients. J. Nucl. Med. 2015, 56, 847–854. [Google Scholar] [CrossRef] [PubMed]
- Sadowski, S.M.; Millo, C.; Cottle-Delisle, C.; Merkel, R.; Yang, L.A.; Herscovitch, P.; Pacak, K.; Simonds, W.F.; Marx, S.J.; Kebebew, E. Results of 68Gallium-DOTATATE PET/CT Scanning in Patients with Multiple Endocrine Neoplasia Type 1. J. Am. Coll. Surg. 2015, 221, 509–517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madrzak, D.; Mikołajczak, R.; Kaminski, G. Influence of PET/CT 68Ga somatostatin receptor imaging on proceeding with patients, who were previously diagnosed with 99mTc-EDDA/HYNIC-TOC SPECT. Nucl. Med. Rev. 2016, 19, 88–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnbeck, C.B.; Knigge, U.; Loft, A.; Berthelsen, A.K.; Mortensen, J.; Oturai, P.; Langer, S.W.; Elema, D.R.; Kjaer, A. Head-to-Head Comparison of 64Cu-DOTATATE and 68Ga-DOTATOC PET/CT: A prospective study of 59 patients with neuroendocrine tumors. J. Nucl. Med. 2017, 58, 451–457. [Google Scholar] [CrossRef] [Green Version]
- Kunikowska, J.; Lewington, V.; Krolicki, L. Optimizing somatostatin receptor imaging in patients with neuroendocrine tumors: The impact of 99mTc-HYNICTOC SPECT/SPECT/CT versus 68Ga-DOTATATE PET/CT upon clinical management. Clin. Nucl. Med. 2017, 42, 905–911. [Google Scholar] [CrossRef]
- Hope, T.A.; Calais, J.; Zhang, L.; Dieckmann, W.; Millo, C. 111In-pentetreotide scintigraphy versus 68Ga-DOTATATE PET: Impact on krenning scores and effect of tumor burden. J. Nucl. Med. 2019, 60, 1266–1269. [Google Scholar] [CrossRef] [Green Version]
- Jha, A.; Patel, M.; Carrasquillo, J.A.; Chen, C.C.; Millo, C.; Maass-Moreno, R.; Ling, A.; Lin, F.I.; Lechan, R.M.; Hope, T.A.; et al. Chice is a ggod time: The emergence of [64Cu]Cu-DOTATATE based somatostatin receptor imaging in the era of [68Ga]Ga-DOTATATE. J. Nucl. Med. 2022, 63, 1300–1301. [Google Scholar] [CrossRef]
- Johnbeck, C.B.; Knigge, U.; Kjær, A. PET tracers for somatostatin receptor imaging of neuroendocrine tumors: Current status and review of the literature. Futur. Oncol. 2014, 10, 2259–2277. [Google Scholar] [CrossRef] [Green Version]
- Treglia, G.; Castaldi, P.; Rindi, G.; Giordano, A.; Rufini, V. Diagnostic performance of Gallium-68 somatostatin receptor PET and PET / CT in patients with thoracic and gastroenteropancreatic neuroendocrine tumours: A meta-analysis. Endocrine 2012, 42, 80–87. [Google Scholar] [CrossRef]
- Wild, D.; Bomanji, J.B.; Benkert, P.; Maecke, H.; Ell, P.J.; Reubi, J.C.; Caplin, M.E. Comparison of 68Ga-DOTANOC and 68Ga-DOTATATE PET/CT within patients with gastroenteropancreatic neuroendocrine tumors. J. Nucl. Med. 2013, 54, 364–372. [Google Scholar] [CrossRef] [Green Version]
- Schreiter, N.F.; Brenner, W.; Nogami, M.; Buchert, R.; Huppertz, A.; Pape, U.-F.; Prasad, V.; Hamm, B.; Maurer, M.H. Cost comparison of 111In-DTPA-octreotide scintigraphy and 68Ga-DOTATOC PET/CT for staging enteropancreatic neuroendocrine tumours. Eur. J. Nucl. Med. Mol. Imaging 2012, 39, 72–82. [Google Scholar] [CrossRef] [PubMed]
- Panzuto, F.; Nasoni, S.; Falconi, M.; Corleto, V.D.; Capurso, G.; Cassetta, S.; Di Fonzo, M.; Tornatore, V.; Milione, M.; Angeletti, S.; et al. Prognostic factors and survival in endocrine tumor patients: Comparison between gastrointestinal and pancreatic localization. Endocr. Relat. Cancer 2005, 12, 1083–1092. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, S.; Johnson, M.M.; Murthy, R.; Ahrar, K.; Wallace, M.J.; Madoff, D.C.; McRae, S.E.; Hicks, M.E.; Rao, S.; Vauthey, J.-N.; et al. Hepatic Arterial Embolization and Chemoembolization for the Treatment of Patients with Metastatic. Cancer 2005, 104, 1590–1602. [Google Scholar] [CrossRef] [PubMed]
- Vandecaveye, V.; van Binnebeek, S.; Mottaghy, F.M.; van Cutsem, E. Early Whole-Body Diffusion-weighted MRI Helps Predict Long-term Outcome Following Peptide Receptor Radionuclide Therapy for Metastatic Neuroendocrine. Radiol. Imaging Cancer 2022, 1, 1–12. [Google Scholar] [CrossRef]
- Pauwels, E.; Van Binnebeek, S.; Vandecaveye, V.; Baete, K.; Vanbilloen, H.; Koole, M.; Mottaghy, F.M.; Haustermans, K.; Clement, P.M.; Nackaerts, K.; et al. Inflammation-Base Index and 68Ga-DOTATOC PET-Derived Uptake and Volumetric Parameters Predict Outcome in Neuroendocrine Tumor Patients Treated with 90Y-DOTATOC. J. Nucl. Med. 2020, 61, 1014–1020. [Google Scholar] [CrossRef]
- Zaknun, J.J.; Bodei, L. The joint IAEA, EANM, and SNMMI practical guidance on peptide receptor radionuclide therapy (PRRNT) in neuroendocrine tumours. Eur. J. Nucl. Med. Mol. Imaging 2013, 40, 800–816. [Google Scholar] [CrossRef] [Green Version]
- Abrantes, A.M.; Pires, A.S.; Monteiro, L.; Teixo, R.; Neves, A.R.; Tavares, N.T.; Marques, I.A.; Botelho, M.F. Tumour functional imaging by PET. Biochim. Biophys. Acta-Mol. Basis Dis. 2020, 1866, 165717. [Google Scholar] [CrossRef]
- Piccardo, A.; Fiz, F.; Bottoni, G.; Ugolini, M.; Noordzij, W.; Trimboli, P. Head-to-head comparison between 18F-DOPA PET/CT and 68Ga-DOTA peptides PET/CT in detecting intestinal neuroendocrine tumours: A systematic review and meta-analysis. Clin. Endocrinol. 2021, 95, 595–605. [Google Scholar] [CrossRef]
- Liu, X.; Li, N.; Jiang, T.; Xu, H.; Ran, Q.; Shu, Z.; Wu, J.; Li, Y.; Zhou, S.; Zhang, B. Comparison of gallium-68 somatostatin receptor and 18 F-fluorodeoxyglucose positron emission tomography in the diagnosis of neuroendocrine tumours: A systematic review and meta-analysis. Hell. J. Nucl. Med. 2020, 23, 188–200. [Google Scholar]
- Zhu, W.; Cheng, Y.; Wang, X.; Yao, S.; Bai, C.; Zhao, H.; Jia, R.; Xu, J.; Huo, L. Head-to-head comparison of 68Ga-DOTA-JR11 and 68Ga-DOTATATE PET/CT in patients with metastatic, well-differentiated neuroendocrine tumors: A prospective study. J. Nucl. Med. 2020, 61, 897–903. [Google Scholar] [CrossRef]
- Nicolas, G.P.; Schreiter, N.; Kaul, F.; Uiters, J.; Bouterfa, H.; Kaufmann, J.; Erlanger, T.E.; Cathomas, R.; Christ, E.; Fani, M.; et al. Sensitivity comparison of 68Ga-OPS202 and 68Ga-DOTATOC PET/CT in patients with gastroenteropancreatic neuroendocrine tumors: A prospective phase II imaging study. J. Nucl. Med. 2018, 59, 915–921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mansi, R.; Fani, M. Design and development of the theranostic pair 177Lu-OPS201/68Ga-OPS202 for targeting somatostatin receptor expressing tumors. J. Label. Compd. Radiopharm. 2019, 62, 635–645. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author, Ref | Year of Pub | Country | N pts | Comparative RF | SOR | Interpretation | Outcome | |
|---|---|---|---|---|---|---|---|---|
| 1 | Bangard et al. [9] | 2000 | Germany | 9 | 111In-DTPA-OC vs. 99mTc-EDDA/HYNIC-TOC | None | Visual ans semiquantitative analysis | Both tracers outperform similarly for the detection of tumors, although 99mTc-EDDA/HYNIC-TOC detects more abdominal lesions and 111In-DTPA-OC more liver metastases |
| 2 | Decristoforo et al. [10] | 2000 | Austria | 10 | 111In-DTPA-Octreotide/111In-DTPA-TOC vs. 99mTc-EDDA/HYNIC-TOC | None | Visual ans semiquantitative analysis | Both tracers outperform similarly for the detection of tumor |
| 3 | Hofmann et al. [11] | 2001 | Germany | 8 | 111In-DTPA-Octreotide vs. 68Ga-DOTATOC | None | Visual analysis by three observers | 68Ga-DOTATOC outperformed 111In-DTPA-Octretide detecting more lesions |
| 4 | Kowalski et al. [12] | 2003 | Germany | 4 | 111In-DTPA-Octreotide vs. 68Ga-DOTATOC | None | Visual analysis | 68Ga-DOTATOC outperformed 111In-DTPA-Octretide detecting more lesions |
| 5 | Gabriel et al. [13] | 2003 | Austria | 41 | 111In-DTPA-Octreotide vs. 99mTc-EDDA/HYNIC-TOC. | Imaging | Visual analysis by two observers | 99mTc- EDDA/HYNIC- TOC outperformed 111In-DTPA-Octretide detecting more lesions |
| 6 | Buchmann et al. [14] | 2007 | Germany | 27 | 111In-DTPA-Octreotide vs. 68Ga-DOTATOC | Histology and imaging | Visual analysis by two observers | 68Ga-DOTATOC outperformed 111In-DTPA-Octretide detecting more lesions and changing the management |
| 7 | Gabriel et al. [15] | 2007 | Austria | 84 | 111In-DTPA-Octreotide vs. 68Ga-DOTATOC | Histology and imaging | Visual analysis by two observers (third in discordant case) | 68Ga-DOTATOC outperformed 111In-DTPA-Octretide detecting more lesions and changing the management |
| 8 | Mussig K et al. [16] | 2010 | USA | 36 | 111In-DTPA-Octreotide vs. 68Ga-DOTATOC | Histology | Visual analysis by two observers | 111In-DTPA-Octreotide and 68Ga-DOTATOC both correlate with SSTR expression |
| 9 | Srirajaskanthan et al. [17] | 2010 | UK | 51 | 111In-DTPA-Octreotide vs. 68Ga-DOTATATE | None | Visual analysis | 68Ga-DOTATATE outperformed 111In-DTPA-Octretide detecting more lesions and changing the management |
| 10 | Krausz et al. [18] | 2011 | Israel | 19 | 111In-DTPA-Octreotide vs. 68Ga-DOTANOC | None | Visual analysis | 68Ga-DOTANOC outperformed 111In-DTPA-Octretide detecting more lesions and changing the management |
| 11 | Hofman et al. [19] | 2012 | Australia | 40 | 111In-DTPA-Octretide vs. 68Ga-DOTATATE | None | Visual analysis | 68Ga-DOTATATE outperformed 111In-DTPA-Octretide detecting more lesions |
| 12 | Van Binnebeek et al. [20] | 2016 | Belgium | 53 | 111In-DTPA-Octreotide vs. 68Ga-DOTATOC | Imaging | Visual analysis | 68Ga-DOTATOC outperformed 111In-DTPA-Octretide detecting more lesions |
| 13 | Pfeifer et al. [21] | 2015 | Denmark | 112 | 111In-DTPA-Octretide vs. 64Cu-DOTATATE | Histology and imaging | Visual analysis by two observers | 64Cu-DOTATATE outperformed 111In-DTPA-Octretide detecting more lesions |
| 14 | Sadowski et al. [22] | 2015 | Austria | 26 | 111In-DTPA-Octreotide vs. 68Ga-DOTATOC | Histology and imaging | Visual analysis | 68Ga-DOTATOC outperformed 111In-DTPA-Octretide detecting more lesions without changing the management |
| 15 | Madrzak et al. [23] | 2016 | Poland | 24 | 99mTc-EDDA/HYNIC-TOC vs. 68Ga-DOTATOC/TATE | Not clear | No data | 68Ga-DOTATOC outperformed 99mTc-EDDA/HYNIC-TOC by detecting more lesions and by changing the management |
| 16 | Johnbeck et al. [24] | 2017 | Denmark | 59 | 64Cu-DOTATATE vs. 68Ga-DOTATOC | Clinical follow-up | Visual analysis by one observer | 64Cu-DOTATATE outperformed 68Ga-DOTATOC detecting more lesions |
| 17 | Kunikowska et al. [25] | 2017 | Poland | 68 | 99mTc-HYNIC-TOC vs. 68Ga-DOTATATE | Imaging | Visual analysis | 68Ga-DOTATATE outperformed 99Tc-HYNIC-TOC detecting more lesions, and by changing the management |
| 18 | Hope et al. [26] | 2019 | USA | 150 | 111In-DTPA-Octreotide vs. 68Ga-DOTATOC | None | Visual and semiquantitative analysis | 68Ga-DOTATOC outperformed 111In-DTPA-Octreotide in higher Krenning score lesions (mainly for size < 2 cm |
| 19 | Jha et al. [27] | 2022 | USA | 5 | 64Cu-DOTATATE vs. 68Ga-DOTATATE | None | Visual analysis | Both 64Cu-DOTATATE and 68Ga-DOTATATE can be interchangeably |
| Author, Ref | N pts | 111In-DTPA Octreotide | 99mTc-EDDA/HYNIC-TOC | 68Ga-DOTATATE/NOC/TOC | 64Cu-DOTATATE | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| TP | TN | FP | FN | TP | TN | FP | FN | TP | TN | FP | FN | TP | TN | FP | FN | |||
| 1 | Gabriel et al. [13] | 41 | 21 | 4 | 1 | 15 | 27 | 2 | 3 | 9 | - | - | - | - | - | - | - | - |
| 2 | Gabriel et al. [15] | 84 | 37 | 12 | 1 | 34 | ** | ** | ** | ** | 69 | 12 | 1 | 2 | - | - | - | - |
| 3 | Srirajaskanthan et al. [17] | 51 | 15 | 3 | 1 | 32 | - | - | - | - | 42 | 3 | 1 | 5 | - | - | - | - |
| 4 | Krausz et al. [18] | 19 | 19 | 0 | 0 | 0 | - | - | - | - | 19 | 0 | 0 | 0 | - | - | - | - |
| 5 | Pfeifer et al. [21] | 112 | 87 | 12 | 0 | 13 | - | - | - | - | - | - | - | - | 97 | 12 | 0 | 3 |
| 6 | Madrzak et al. [23] | 24 | - | - | - | - | 11 | 11 | 1 | 1 | 12 | 12 | 0 | 0 | - | - | - | - |
| 7 | Johnbeck et al. * [24] | 59 | - | - | - | - | - | - | - | - | 43 | 9 | 1 | 5 | 43 | 14 | 1 | 0 |
| Author, Ref | 111In-DTPA-Octreotide | 99mTc-EDDA/HYNIC-TOC | 68Ga-DOTATATE/NOC/TOC | 64Cu-DOTATATE | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sens (95% CI) | Spec (95% CI) | Acc (95% CI) | Sens (95% CI) | Spec (95% CI) | Acc (95% CI) | Sens (95% CI) | Spec (95% CI) | Acc (95% CI) | Sens (95% CI) | Spec (95% CI) | Acc (95% CI) | ||
| 1 | Gabriel et al. [13] | 58.3 (42–73) | 80 (64–90) | 61 | 75 (58–87) | 40 (25–56) | 70.7 | - | - | - | - | - | - |
| 2 | Gabriel et al. [15] | 52.1 (41–63) | 92.3 (84–97) | 58.3 | ** | ** | ** | 97.2 (90–99) | 92.3 (84–97) | 96.4 | - | - | - |
| 3 | Srirajaskanthan et al. [17] | 31.9 (20–46) | 75 (61–86) | 35 | - | - | - | 89.4 (77–96) | 75 (61–86) | 88 | - | - | - |
| 4 | Pfeifer et al. [21] | 87 (79–92) | 100 (96–100) | 88.4 | - | - | - | - | - | - | 97 (91–99) | 100 (96–100) | 97.3 |
| 5 | Madrzak et al. [23] | - | - | - | 91.7 (72–99) | 91.7 (72–99) | 91.7 | 100 (83–100) | 100 (83–100) | 100 | - | - | - |
| 6 | Johnbeck et al. * [24] | - | - | - | - | - | - | 89.6 (78–96) | 90 (79–96) | 89.7 | 100 (92–100) | 93 (83–98) | 98.3 |
| PROS | CONS | ||
|---|---|---|---|
| SPECT | PET | SPECT | PET |
|
|
| |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Poletto, G.; Cecchin, D.; Sperti, S.; Filippi, L.; Realdon, N.; Evangelista, L. Head-to-Head Comparison between Peptide-Based Radiopharmaceutical for PET and SPECT in the Evaluation of Neuroendocrine Tumors: A Systematic Review. Curr. Issues Mol. Biol. 2022, 44, 5516-5530. https://0-doi-org.brum.beds.ac.uk/10.3390/cimb44110373
Poletto G, Cecchin D, Sperti S, Filippi L, Realdon N, Evangelista L. Head-to-Head Comparison between Peptide-Based Radiopharmaceutical for PET and SPECT in the Evaluation of Neuroendocrine Tumors: A Systematic Review. Current Issues in Molecular Biology. 2022; 44(11):5516-5530. https://0-doi-org.brum.beds.ac.uk/10.3390/cimb44110373
Chicago/Turabian StylePoletto, Giulia, Diego Cecchin, Stefania Sperti, Luca Filippi, Nicola Realdon, and Laura Evangelista. 2022. "Head-to-Head Comparison between Peptide-Based Radiopharmaceutical for PET and SPECT in the Evaluation of Neuroendocrine Tumors: A Systematic Review" Current Issues in Molecular Biology 44, no. 11: 5516-5530. https://0-doi-org.brum.beds.ac.uk/10.3390/cimb44110373