Which Should Be Used First for ALK-Positive Non-Small-Cell Lung Cancer: Chemotherapy or Targeted Therapy? A Meta-Analysis of Five Randomized Trials


Abstract
:1. Introduction
2. Methods
2.1. Study Selection
2.2. Data Extraction
2.3. Statistical Analysis
3. Results
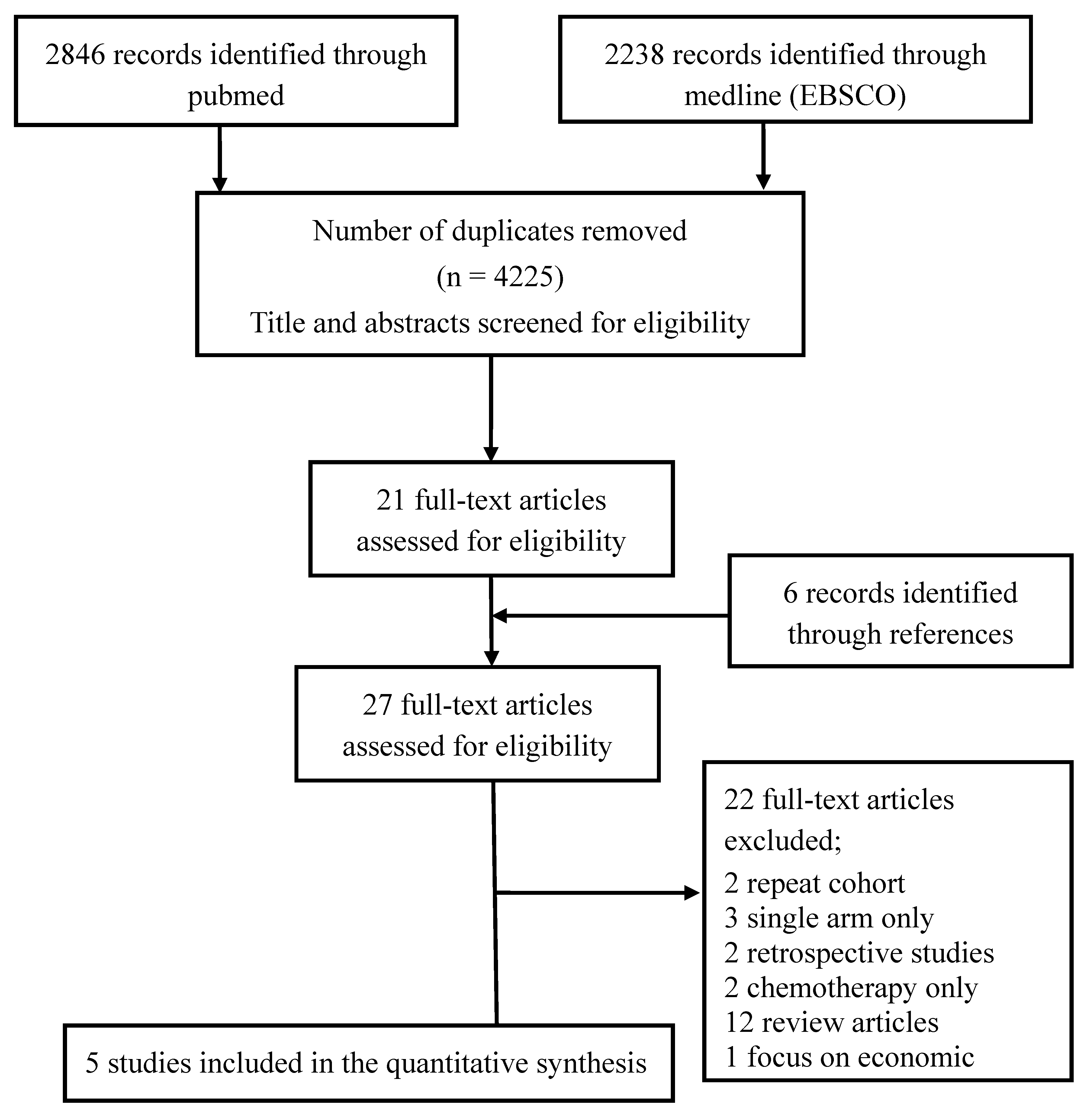
Search Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Solomon, B.J.; Mok, T.; Kim, D.W.; Wu, Y.L.; Nakagawa, K.; Mekhail, T.; Felip, E.; Cappuzzo, F.; Paolini, J.; Usari, T.; et al. First-line crizotinib versus chemotherapy in ALK-positive lung cancer. N. Engl. J. Med. 2014, 371, 2167–2177. [Google Scholar] [CrossRef] [PubMed]
- Shaw, A.T.; Yeap, B.Y.; Solomon, B.J.; Riely, G.J.; Gainor, J.; Engelman, J.A.; Shapiro, G.I.; Costa, D.B.; Ou, S.H.; Butaney, M.; et al. Effect of crizotinib on overall survival in patients with advanced non-small-cell lung cancer harbouring ALK gene rearrangement: A retrospective analysis. Lancet Oncol. 2011, 12, 1004–1012. [Google Scholar] [CrossRef]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Novello, S.; Mazieres, J.; Oh, I.J.; de Castro, J.; Migliorino, M.R.; Helland, A.; Dziadziuszko, R.; Griesinger, F.; Kotb, A.; Zeaiter, A.; et al. Alectinib versus chemotherapy in crizotinib-pretreated anaplastic lymphoma kinase (ALK)-positive non-small-cell lung cancer: Results from the phase III ALUR study. Ann. Oncol. 2018, 29, 1409–1416. [Google Scholar] [CrossRef] [PubMed]
- Soria, J.C.; Tan, D.S.W.; Chiari, R.; Wu, Y.L.; Paz-Ares, L.; Wolf, J.; Geater, S.L.; Orlov, S.; Cortinovis, D.; Yu, C.J.; et al. First-line ceritinib versus platinum-based chemotherapy in advanced ALK-rearranged non-small-cell lung cancer (ASCEND-4): A randomised, open-label, phase 3 study. Lancet 2017, 389, 917–929. [Google Scholar] [CrossRef]
- Shaw, A.T.; Kim, D.W.; Nakagawa, K.; Seto, T.; Crino, L.; Ahn, M.J.; De Pas, T.; Besse, B.; Solomon, B.J.; Blackhall, F.; et al. Crizotinib versus chemotherapy in advanced ALK-positive lung cancer. N. Engl. J. Med. 2013, 368, 2385–2394. [Google Scholar] [CrossRef] [PubMed]
- Shaw, A.T.; Kim, T.M.; Crino, L.; Gridelli, C.; Kiura, K.; Liu, G.; Novello, P.S.; Bearz, A.; Gautschi, O.; Mok, T.; et al. Ceritinib versus chemotherapy in patients with ALK-rearranged non-small-cell lung cancer previously given chemotherapy and crizotinib (ASCEND-5): A randomised, controlled, open-label, phase 3 trial. Lancet Oncol. 2017, 18, 874–886. [Google Scholar] [CrossRef]
- Camidge, D.R.; Kono, S.A.; Lu, X.; Okuyama, S.; Baron, A.E.; Oton, A.B.; Davies, A.M.; Varella-Garcia, M.; Franklin, W.; Doebele, R.C. Anaplastic lymphoma kinase gene rearrangements in non-small cell lung cancer are associated with prolonged progression-free survival on pemetrexed. J. Thorac. Oncol. 2011, 6, 774–780. [Google Scholar] [CrossRef] [PubMed]
- Kron, A.; Alidousty, C.; Scheffler, M.; Merkelbach-Bruse, S.; Seidel, D.; Riedel, R.; Ihle, M.A.; Michels, S.; Nogova, L.; Fassunke, J.; et al. Impact of TP53 mutation status on systemic treatment outcome in ALK-rearranged non-small-cell lung cancer. Ann. Oncol. 2018, 29, 2068–2075. [Google Scholar] [CrossRef] [PubMed]
- Peters, S.; Camidge, D.R.; Shaw, A.T.; Gadgeel, S.; Ahn, J.S.; Kim, D.W.; Ou, S.I.; Pérol, M.; Dziadziuszko, R.; Rosell, R.; et al. Alectinib versus crizotinib in untreated alk-positive non-small-cell lung cancer. N. Engl. J. Med. 2017, 377, 829–838. [Google Scholar] [CrossRef] [PubMed]
- Gainor, J.F.; Dardaei, L.; Yoda, S.; Friboulet, L.; Leshchiner, I.; Katayama, R.; Dagogo-Jack, I.; Gadgeel, S.; Schultz, K.; Singh, M.; et al. Molecular Mechanisms of Resistance to First- and Second-Generation ALK Inhibitors in ALK-Rearranged Lung Cancer. Cancer Discov. 2016, 6, 1118–1133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thai, A.A.; Solomon, B.J. Treatment of ALK-positive nonsmall cell lung cancer: Recent advances. Curr. Opin. Oncol. 2018, 30, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Leprieur, E.G.; Fallet, V.; Cadranel, J.; Wislez, M. Spotlight on crizotinib in the first-line treatment of ALK-positive advanced non-small-cell lung cancer: Patients selection and perspectives. Lung Cancer 2016, 7, 83–90. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Trials, Year | Setting | Regiment | Patient No. | Age (Median) | Cross-Over (%) | Initial Brain Meta (%) | Follow-Up Median Time (m) | PFS (m) | OS (m) |
|---|---|---|---|---|---|---|---|---|---|
| PROFILE 1014, 2014 [1] | First-line | Crizotinib vs. PEM + cisplatin | 172 171 | 52 54 | Yes (70%) | 26 27 | 17.4 16.7 | 10.9 7 | 17.4 16.7 |
| ASCEND-4, 2017 [6] | First-line | Ceritinib vs. PEM + platinum | 189 187 | 55 54 | Yes ((105/187)56%) | 31 33 | NA NA | 16.6 8.1 | NR 26.2 |
| PROFILE 1007, 2013 [5] | Second-line | Crizotinib vs. PEM or TXT | 173 174 | 51 49 | Yes ((112/174)64%) | 35 34 | 12.2 12.1 | 7.7 3.0 | NR NR |
| ALUR, 2018 [4] | Two prior lines, crizotinib, platinum-based doublet | Alectinib vs. PEM or TXT | 72 35 (2:1 block) | 55.5 59 | Yes (70.6%) | 65.3 74.3 | 6.5 5.8 | 7.1 1.6 | 12.6 NR |
| ASCEND-5, 2017 [7] | 1 or 2 chemotherapy, and crizotinib resistance | Ceritinib vs. PEM or TXT | 115 116 | 54 54 | Yes (64.7%) | 57 59 | 19.7 | 5.4 1.6 | 18.1 20.1 |
| Trials, Year | Was the Study Described as Randomized? | Method to Generate the Sequence of Randomization was Described and Appropriate | Was the Study Described as a Double Blind? | Method of Double Blinding was Described and Appropriate | Was There a Description of Withdrawal and Dropouts? | Score |
|---|---|---|---|---|---|---|
| PROFILE 1014, 2014 [1] | * | - | - | - | * | 2 |
| ASCEND-4, 2017 [6] | * | * | - | - | * | 3 |
| PROFILE 1007, 2013 [5] | * | - | - | - | * | 2 |
| ALUR, 2018 [4] | * | - | - | - (note) | - | 1 |
| ASCEND-5, 2017 [7] | * | * | - | - (note) | * | 3 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, Y.-C.; Hsieh, C.-C.; Lee, Y.-L.; Li, C.-Y. Which Should Be Used First for ALK-Positive Non-Small-Cell Lung Cancer: Chemotherapy or Targeted Therapy? A Meta-Analysis of Five Randomized Trials. Medicina 2019, 55, 29. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55020029
Lee Y-C, Hsieh C-C, Lee Y-L, Li C-Y. Which Should Be Used First for ALK-Positive Non-Small-Cell Lung Cancer: Chemotherapy or Targeted Therapy? A Meta-Analysis of Five Randomized Trials. Medicina. 2019; 55(2):29. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55020029
Chicago/Turabian StyleLee, Yen-Chien, Chung-Cheng Hsieh, Yen-Ling Lee, and Chung-Yi Li. 2019. "Which Should Be Used First for ALK-Positive Non-Small-Cell Lung Cancer: Chemotherapy or Targeted Therapy? A Meta-Analysis of Five Randomized Trials" Medicina 55, no. 2: 29. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55020029