Hypercholesterolemia in Two Siblings with Resistance to Thyroid Hormones Due to Disease-Causing Variant in Thyroid Hormone Receptor (THRB) Gene

 , ,
, ,
Abstract
:1. Introduction
2. Case Reports
3. Discussion
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Weiss, R.E.; Refetoff, S. Resistance to Thyroid Hormone. Rev. Endocr. Metab. Disord. 2000, 1, 97–108. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Kim, E.Y. Resistance to thyroid hormone due to a novel mutation of thyroid hormone receptor beta gene. Ann. Pediatr. Endocrinol. Metab. 2014, 19, 229–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Işık, E.; Beck Peccoz, P.; Campi, I.; Özön, A.; Alikaşifoğlu, A.; Gönç, N.; Kandemir, N. Thyroid hormone resistance: A novel mutation in thyroid hormone receptor beta (THRB) gene—Case report. Turk. J. Pediatr. 2013, 55, 322–327. [Google Scholar] [PubMed]
- Onigata, K.; Szinnai, G. Resistance to thyroid hormone. Endocr. Dev. 2014, 26, 118–129. [Google Scholar]
- Ortiga-Carvalho, T.M.; Sidhaye, A.R.; Wondisford, F.E. Thyroid hormone receptors and resistance to thyroid hormone disorders. Nat. Rev. Endocrinol. 2014, 10, 582–591. [Google Scholar] [CrossRef] [Green Version]
- Gonçalves, A.P.; Aragüés, J.M.; Nobre, E.; Barbosa, A.P.; Mascarenhas, M. A case of thyroid hormone resistance: A rare mutation. Arq. Bras. Endocrinol. Metabol. 2014, 58, 962–966. [Google Scholar] [CrossRef] [Green Version]
- Reutrakul, S.; Sadow, P.M.; Pannain, S.; Pohlenz, J.; Carvalho, G.A.; Macchia, P.E.; Weiss, R.E.; Refetoff, S. Search for abnormalities of nuclear corepressors, coactivators, and a coregulator in families with resistance to thyroid hormone without mutations in thyroid hormone receptor beta or alpha genes. J. Clin. Endocrinol. Metab. 2000, 85, 3609–3617. [Google Scholar]
- Weiss, R.E.; Hayashi, Y.; Nagaya, T.; Petty, K.J.; Murata, Y.; Tunca, H.; Seo, H.; Refetoff, S. Dominant inheritance of resistance to thyroid hormone not linked to defects in the thyroid hormone receptor alpha or beta genes may be due to a defective cofactor. J. Clin. Endocrinol. Metab. 1996, 81, 4196–4203. [Google Scholar]
- Kim, J.H.; Park, T.S.; Baek, H.S.; Kim, G.H.; Yoo, H.W.; Park, J.H. A newly identified insertion mutation in the thyroid hormone receptor-beta gene in a Korean family with generalized thyroid hormone resistance. J. Korean Med. Sci. 2007, 22, 560–563. [Google Scholar] [CrossRef]
- Pramfalk, C.; Pedrelli, M.; Parini, P. Role of thyroid receptor β in lipid metabolism. Biochim. Biophys. Acta 2011, 1812, 929–937. [Google Scholar] [CrossRef] [Green Version]
- Clinical Variation for Gene Symbols, HGVS Expressions, Condition, and More. NCBI. Last Evaluated 31 May 2018. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/clinvar/variation/12567/#clinical-assertions (accessed on 5 October 2020).
- Amor, A.J.; Halperin, I.; Alfayate, R.; Borrás, V.M.; Escribano, A.; González, C.; Gutiérrez, A.; Mauri, M.; Pérez, P.; Picó, A.; et al. Identification of four novel mutations in the thyroid hormone receptor-β gene in 164 Spanish and 2 Greek patients with resistance to thyroid hormone. Hormones 2014, 13, 74–78. [Google Scholar] [CrossRef] [PubMed]
- Ditudompo, S.; Ongphiphadhanakul, B.; Chanprasertyotin, S.; Rajatanavin, R. A de novo L330S point mutation in thyroid hormone receptor beta gene in a Thai female with resistance to thyroid hormone. Endocr. J. 1999, 46, 825–829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, S. Thyroid hormone receptor mutations and disease: Beyond thyroid hormone resistance. Trends Endocrinol. Metab. 2005, 16, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Sinha, R.A.; Singh, B.K.; Yen, P.M. Direct effects of thyroid hormones on hepatic lipid metabolism. Nat. Rev. Endocrinol. 2018, 14, 259–269. [Google Scholar] [CrossRef]
- Mitchell, C.S.; Savage, D.B.; Dufour, S.; Schoenmakers, N.; Murgatroyd, P.; Befroy, D.; Halsall, D.; Northcott, S.; Raymond-Barker, P.; Curran, S.; et al. Resistance to thyroid hormone is associated with raised energy expenditure, muscle mitochondrial uncoupling, and hyperphagia. J. Clin. Investig. 2010, 120, 1345–1354. [Google Scholar] [CrossRef] [Green Version]
- Owen, P.J.D.; Chatterjee, V.K.; John, R.; Halsall, D.; Lazarus, J.H. Augmentation index in resistance to thyroid hormone (RTH). Clin. Endocrinol. 2009, 70, 650–654. [Google Scholar] [CrossRef]
- Klančar, G.; Grošelj, U.; Kovač, J.; Bratanič, N.; Bratina, N.; Trebušak Podkrajšek, K.; Battelino, T. Universal screening for familial hypercholesterolemia in children. J. Am. Coll. Cardiol. 2015, 66, 1250–1257. [Google Scholar] [CrossRef] [Green Version]
- Groselj, U.; Kovac, J.; Sustar, U.; Mlinaric, M.; Fras, Z.; Podkrajsek, K.T.; Battelino, T. Universal screening for familial hypercholesterolemia in children: The Slovenian model and literature review. Atherosclerosis 2018, 277, 383–391. [Google Scholar] [CrossRef]
- Shamir, R.; Lerner, A.; Fisher, E. Hypercholesterolemia in children. Isr. Med. Assoc. J. 2000, 2, 767–771. [Google Scholar]
- Iqbal, A.M.; Lteif, A.N.; Kumar, S. Association between mild hyperthyrotropinemia and hypercholesterolemia in children with severe obesity. J. Ped. Endorcinol. Metab. 2019, 32, 561–568. [Google Scholar] [CrossRef]
- Sedej, K.; Kotnik, P.; Avbelj Stefanija, M.; Grošelj, U.; Širca Čampa, A.; Lusa, L.; Battelino, T.; Bratina, N. Decreased prevalence of hypercholesterolaemia and stabilisation of obesity trends in 5-year-old children: Possible effects of changed public health policies. Eur. J. Endocrinol. 2014, 170, 293–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El Shafie, K.; Ouhtit, A.; Al Farsi, Y.; Al Sayegh, A.; Al Shafaee, M. A rare thyroid hormone receptor beta (THRβ) gene mutation in a 15-year-old girl with thyroid hormone resistance syndrome: A case report. J. Med. Case Rep. 2014, 8, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Siblings with Confirmed THRB Mutation | |||
|---|---|---|---|
| Index Patient | Younger Sister | Younger Brother | |
| Clinical signs and symptoms | Malaise, subfebrile state, weight loss, marginal tachycardia | Asymptomatic, marginal tachycardia | Asymptomatic, marginal tachycardia |
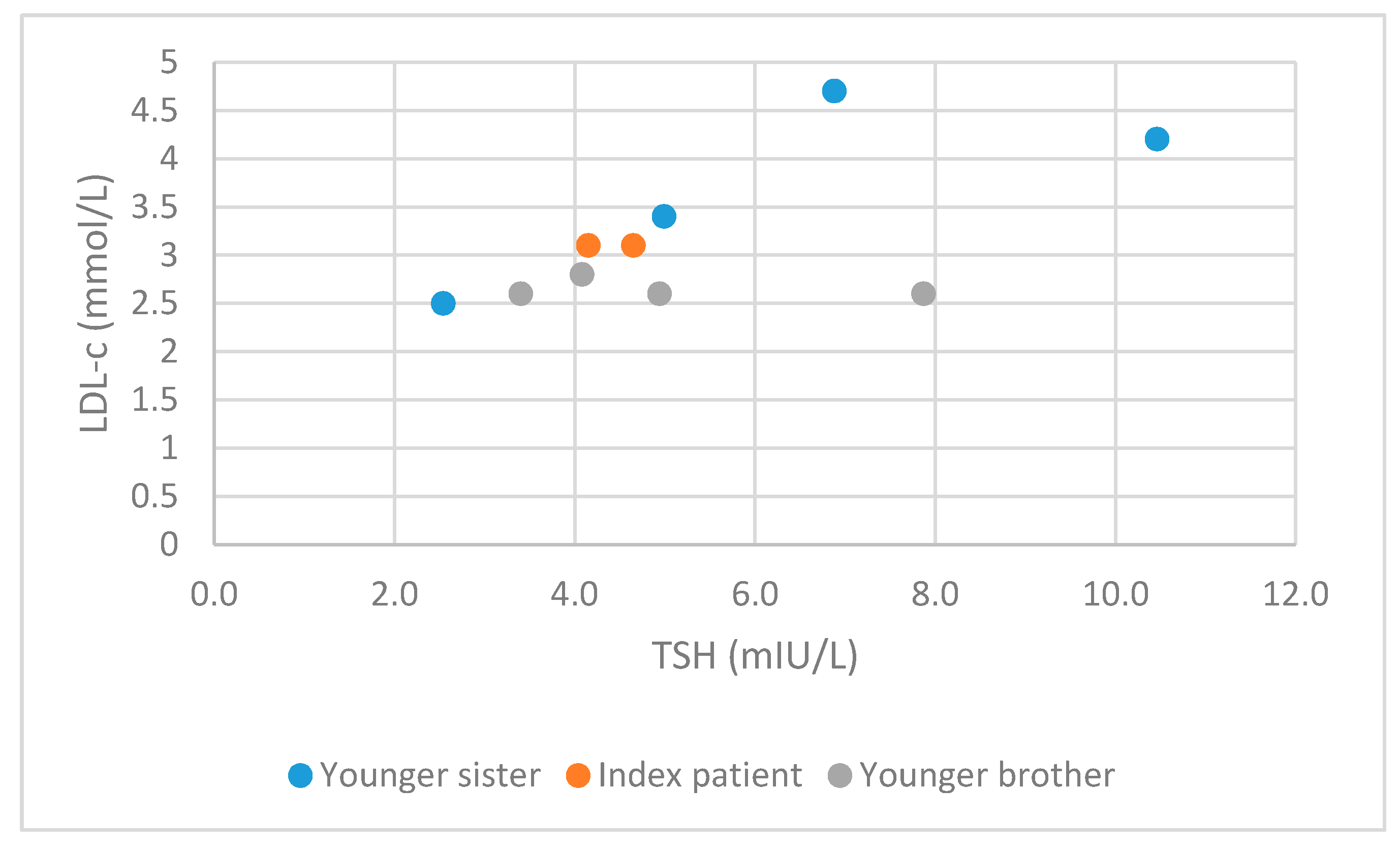
| Peak thyroid hormone levels | TSH 4.65 mIU/L (B) | TSH 10.46 mIU/L (E) | TSH 7,87 mIU/L (E) |
| fT4 39.9 pmol/L (E) | fT4 35.81 pmol/L (E) | fT4 32.68 pmol/L (E) | |
| fT3 10.11 pmol/L (E) | fT3 14.16 pmol/L (E) | fT3 12.28 pmol/L (E) | |
| Thyroid antibodies | Absent | Absent | Absent |
| Peak cholesterol levels | TC 5.5 mmol/L (E) | TC 6.6 mmol/L (E) | TC 4.5 mmol/L (N) |
| LDL-c 3.1. mmol/L (B) | LDL-c 4.2 mmol/L (E) | LDL-c 2.6 mmol/L (N) | |
| HDL-c 1.7 mmol/L (N) | HDL-c 1.5 mmol/L (N) | HDL-c 1.3 mmol/L (N) | |
| TG 1.5 mmol/L (N) | TG 1.2 mmol/L (N) | TG 1.4 mmol/L (N) | |
| Thyroid ultrasound examination | Enlarged, thickened thyroid gland, isoechogenic, fine granular structure, without nodules, with normal perfusion | Normal ultrasound report | Slightly enlarged, without nodules |
| Treatment needed | No | No | No |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pajek, M.; Avbelj Stefanija, M.; Trebusak Podkrajsek, K.; Suput Omladic, J.; Zerjav Tansek, M.; Battelino, T.; Groselj, U. Hypercholesterolemia in Two Siblings with Resistance to Thyroid Hormones Due to Disease-Causing Variant in Thyroid Hormone Receptor (THRB) Gene. Medicina 2020, 56, 699. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56120699
Pajek M, Avbelj Stefanija M, Trebusak Podkrajsek K, Suput Omladic J, Zerjav Tansek M, Battelino T, Groselj U. Hypercholesterolemia in Two Siblings with Resistance to Thyroid Hormones Due to Disease-Causing Variant in Thyroid Hormone Receptor (THRB) Gene. Medicina. 2020; 56(12):699. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56120699
Chicago/Turabian StylePajek, Maja, Magdalena Avbelj Stefanija, Katarina Trebusak Podkrajsek, Jasna Suput Omladic, Mojca Zerjav Tansek, Tadej Battelino, and Urh Groselj. 2020. "Hypercholesterolemia in Two Siblings with Resistance to Thyroid Hormones Due to Disease-Causing Variant in Thyroid Hormone Receptor (THRB) Gene" Medicina 56, no. 12: 699. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56120699