Submuscular and Pre-pectoral ADM Assisted Immediate Breast Reconstruction: A Literature Review


Santa Maria Alle Scotte Hospital, Plastic and Reconstructive Surgery Unit, Department of Medicine, Surgery and Neuroscience, University of Siena, Mario Bracci Street, 53100 Siena, Italy
Medicina 2020, 56(6), 256; https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56060256
Submission received: 7 April 2020
/
Revised: 22 May 2020
/
Accepted: 23 May 2020
/
Published: 26 May 2020
(This article belongs to the Special Issue Updates in Breast Reconstruction: Review from Evidence)
{kind=link}
{kind=link}
Abstract
:Background and objectives: Breast cancer treatment has deeply changed in the last fifty years. Acellular dermal matrices (ADMs) were introduced for breast reconstruction, with encouraging results, but with conflicting reports too. The present paper aims to summarize the current data on breast reconstruction using acellular dermal matrices. Materials and Methods: We reviewed the literature regarding the use of ADM-assisted implant-based breast reconstruction. Results: The main techniques were analyzed and described. Conclusions: Several authors have recently reported positive results. Nevertheless, an increased complications’ rate has been reported by other authors. Higher cost compared to not-ADM-assisted breast reconstruction is another concern.
1. Introduction
The use of acellular dermal matrix (ADM) for breast reconstruction was described by Salzberg in 2006 [1] and by Dieterich in 2015 [2,3]. Acellular dermal matrices (ADMs) are made from fetal bovine, porcine or human cadaver and represent a sort of scaffold that autologous cells can colonize [4,5].
Immediate breast reconstruction (IBR) received an important boost in popularity as a consequence of the advent of ADMs [2,6,7,8,9,10,11,12,13,14,15,16,17,18,19]. The use of ADMs showed encouraging results but conflicting reports as well [20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42]. ADMs-assisted breast reconstruction can be divided into pre-pectoral and submuscular. The present narrative review summarizes the current evidences on immediate breast reconstruction using ADM.
2. Materials and Methods
We performed a review of literature, starting from 2006, by searching on PubMed “acellular dermal matrix” and “breast reconstruction”, focusing on surgical techniques, outcomes and complications’ rate, in order to better understand the evidences on this topic.
3. Results
3.1. Acellular Dermal Matrix (ADM) and Breast Reconstruction
Immediate breast reconstruction (IBR) has radically changed the concept of breast cancer to the extent that a patient admitted to surgery for breast cancer is discharged without the impact of breast amputation.
The main advantages of IBR can be summarized as lower costs for the healthcare system (shorter healing time and fewer hospitalizations) and the elimination of tissue expansion time [43,44,45,46,47]. Despite this, several studies have reported high rates of complications linked to immediate breast reconstruction [2,7,48,49,50,51]. Many authors analyzed these aspects, underlining the safety of IBR and the good outcomes reached with careful patient selection and adherence to surgical techniques [2,52,53,54,55,56,57,58,59,60,61,62,63]. IBR has similar postoperative complications to delayed breast reconstructions with tissue expander and implant, although tissue expander/submuscular implant has been the most popular reconstruction strategy [43,44,64,65,66,67].
The American Society of Plastic Surgeons reported the use of ADMs in about 50% of breast reconstruction in 2012 [68], and these data were confirmed over time [69].
Recent research confirmed good outcomes for ADMs assisted IBR as underlined by Negeborn et al. [35,70] and Carminati et al. [21], with acceptable risks of infection. This risk is higher in obese patients [21]. Improved aesthetic outcomes following ADM use in tissue expander/implant-based breast reconstruction was assessed by Ibrahim et al. [71]. ADM may improve breast volume, placement and inframammary fold definition [72].
The main disadvantage of this kind of procedure is the high costs, as shown by Gravina et al. [24]. They analyzed the different characteristics of the main ADMs and their alternatives, underlining the good aesthetic outcomes and the benefits of single-stage procedures, but these aspects are balanced with high costs and an increased risk of infection and overall surgical complication [24].
3.2. Submuscular ADM-Assisted Breast Reconstruction
In submuscular breast reconstruction, the surgeon can place an ADM to cover the inferior pole of the implant [73,74,75,76]. This is helpful in the following situations:
(1) The breast has a good volume, and the surgeon needs to use an implant of adequate volume for immediate reconstruction, but the inferior pole of the implant cannot be completely covered by the Pectoralis Major [9,10,57,77,78].
Partial muscle coverage is important to obtain a more natural shape, releasing the constriction of the inferior aspect of pectoralis muscle but less coverage of prostheses in the lateral-inferior aspect can occur in some cases [77,82].
Lateral control of the implant position can be obtained by using Serratus or minimizing the lateral dissection during the mastectomy, but this may not be enough. In these cases, the use of an ADM allows surgeons to better control the stability of the breast implant both in immediate and delayed breast reconstruction [77,83,84,85,86].
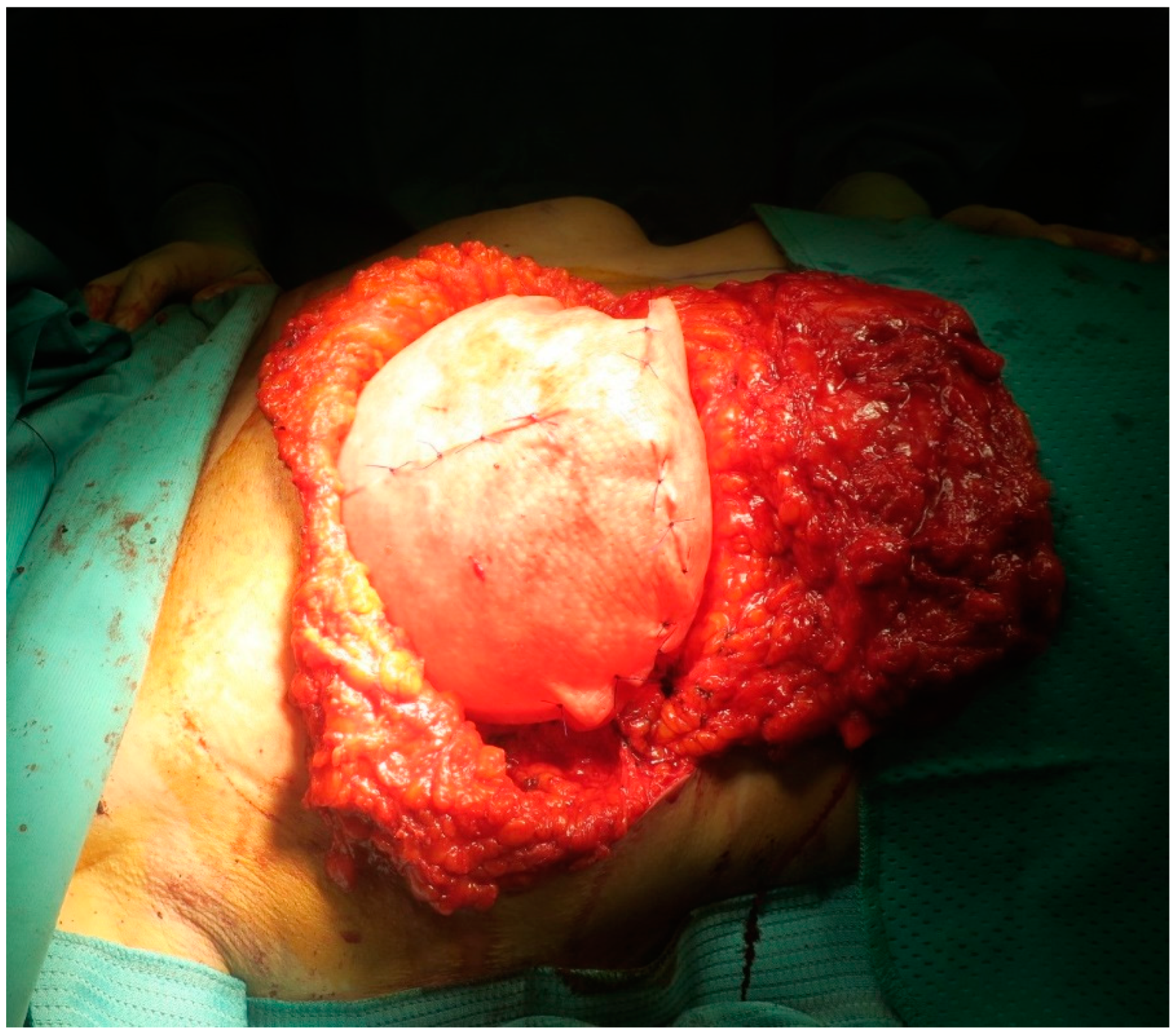
The submuscular breast reconstruction performed using ADM to cover the lateral or the inferior pole of neo-breast is routinely referred to as dual-plane reconstruction (see Figure 1). The most common anti-aesthetic reports is the muscle retraction deformity; this can be avoided by suturing the ADM at the inferior border of the muscle, from the four to eight o’clock position [77,84,87].
Lateral sutures can be used between the skin flap and the chest wall to better close the dead space and improve the lateral contour, but the skin thickness should be carefully evaluated, in order to avoid quilting sutures [8,64,88,89,90,91,92].
Many authors agree that this kind of reconstruction has excellent long-term cosmetic results; the main unexpected event is the distortion or the movement of the implant with flexion of the muscle. Compared to pre-pectoral reconstruction, it is less expensive and can lead to better coverage of the upper pole of the breast. Nevertheless, it is burdened by the risk of upper migration of the implant and more pain due to muscle detachment [2,7,77,83,89,90,91].
3.3. Pre-Pectoral ADM-Assisted Breast Reconstruction
The concept of pre-pectoral breast reconstruction (see Figure 2) can be considered as the “evolution” of breast reconstruction in terms of “tissue sparing”: As nipple-skin sparing mastectomy for the oncologic surgery, pre-pectoral breast reconstruction focuses on sparing the Pectoralis Major Muscle. ADM has a key role in this kind of procedure because it wraps (at least in the front) the implant for a complete integration in the host [93,94].
Pre-pectoral breast reconstruction was suggested in those cases where implants less than 500 cc were requested [95]. Actually, this indication has been modified, and some authors describe pre-pectoral breast reconstruction with implants over 600 cc [77].
Many authors choose the pre-pectoral breast reconstruction because the submuscular placement of the implant can lead to a result described as “contrived breast” [82,91,95,96]. This aspect is relevant and linked to a loss of muscle function; many authors, in fact, underline that patients, in particular after tissue expansion, need physiotherapy. The muscle-spearing breast reconstruction was proposed by many authors over time.
In 2013, Cheng proposed the treatment of capsular contracture using an ADM; he did not perform pre-pectoral reconstruction, but removed the contracted capsule and put ADM to cover the anterior aspect of the implant on 16 breasts. He reported only one infection by coagulase negative Staphylococcus and Mycobacterium fortuitum [97]. The reduction of incidence in capsular contracture using ADMs was underlined in time by Lardi et al., in 2017 [30], and confirmed by Liu et al., with a meta-analysis in 2020 [33].
Becker et al. (2015) reported the experience on 62 breasts covering the anterior aspect of saline implant with an ADM sutured to the muscle. The complications reported were three flap necrosis, one seroma, one infection, one hematoma and two capsular contractures [98].
In 2017, Berna firstly proposed a complete ADM coverage of the implant [93]; the implant stability was guaranteed by suturing the implant and its “envelope” to the muscle. On 100 reconstructions with this procedure, Vidya et al. underlined two hematoma, three dehiscence, one necrosis, five seromas and two implant losses [95].
The main purpose of pre-pectoral reconstruction is to save the function of Pectoralis Major, decreasing the postoperative pain and reducing the follow-up time. Other advantages are represented by minor risk in the upper migration of the implant and a better breast projection [99,100].
The main disadvantages are the high costs of these devices (which are to be added to the cost of breast implants) and the higher risk of symmastia, the rippling and an irregularity of the highest limit of the upper pole of the breast and the high risk of seroma. Several authors suggest not removing the drains until finding a maximum of 30cc for three consecutive days [18,77,101].
3.4. Complications and Outcomes
Tasoulis et al. observed that ADM-assisted breast reconstruction reduces the complications’ rate [105]. Onesti et al. observed that the use of ADM reduces the inflammatory response, along with the likelihood of capsular contracture [36].
On the other hand, Lohmander et al. [106] observed that immediate IBR with ADM carried a risk of implant loss equal to conventional IBR without ADM, but was associated with more adverse outcomes, requiring surgical intervention, through an open-label, multicenter, randomized, controlled trial on 135 women. Antony et al. [107]. observed that acellular human dermis is useful in immediate tissue expander reconstruction but can lead to an increased risk of complications (seroma and reconstructive failure).
The literature data show that the complications’ rate is similar for subcutaneous and submuscular reconstruction ADM assisted, without statistical significance for major adverse events (explantation, wide infections, Baker grade III or IV contracture, and complete nipple–areola complex necrosis) [22]. Overall, the most described complications for ADMs-assisted reconstruction are seroma (up to 9% of cases), explantation (up to 6.5%) and partial nipple–areola complex (NAC) necrosis (up to 5.3%) [2,37,65,83,108,109,110,111,112].
In 2017, Kim and Bang linked the use of ADM and the mastectomy flap necrosis [28]. Powell-Brett and Goh [113] reported 10.4% cases of skin necrosis in a study with ADM-assisted immediate breast reconstruction.
This last complication should be interpreted as follows: It can occur (in some cases) for tissue ischemia during the cancer removing and the implant. Intraoperative tools to evaluate NAC viability can lower this complication’s rate, but these devices are expensive, time-consuming and not available in all centers [41,114,115,116].
The pre-pectoral breast reconstruction is burdened by the following patient complaints: rippling (up to 4.5%) and visible implants (4.3%). The submuscular breast reconstruction is burdened by postoperative pain with significant impact on daily activities (5%), implant deformity and less-natural cosmetic outcomes (until 7%) [6,93,108,117,118,119,120,121,122,123,124]. Onesti et al. suggested a modified technique in obesity patients with large breasts, using a dermal flap to cover the ADM-implant in the pre-pectoral plane, in order to improve the outcomes. Obesity and smoking are always linked to a higher risk of complications [125,126,127].
4. Conclusions
Pre-pectoral and submuscular breast reconstruction with the use of ADMs have no significant difference in complication rate. Particular care must be taken for seroma formation. Obesity and smoking are linked to higher risks of complication. The cost/benefit ratio should be carefully reviewed.
Funding
This research received no external funding.
Conflicts of Interest
The author declares no conflict of interest.
References
- Salzberg, C.A. Nonexpansive immediate breast reconstruction using human acellular tissue matrix graft (AlloDerm). Ann. Plast. Surg. 2006, 57, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Bertozzi, N.; Pesce, M.; Santi, P.; Raposio, E. One-Stage Immediate Breast Reconstruction: A Concise Review. Biomed. Res. Int. 2017. [Google Scholar] [CrossRef] [PubMed]
- Dieterich, M.; Angres, J.; Stubert, J.; Stachs, A.; Reimer, T.; Gerber, B. Patient-Reported Outcomes in Implant-Based Breast Reconstruction Alone or in Combination with a Titanium-Coated Polypropylene Mesh—A Detailed Analysis of the BREAST-Q and Overview of the Literature. Geburtshilfe Frauenheilkd. 2015, 75, 692–701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butler, C.E.; Selber, J.C. Discussion: The use of acellular dermal matrix in immediate two-stage tissue expander breast reconstruction. Plast. Reconstr. Surg. 2012, 129, 1059–1060. [Google Scholar] [CrossRef]
- Margulies, I.G.; Salzberg, C.A. The use of acellular dermal matrix in breast reconstruction: Evolution of techniques over 2 decades. Gland Surg. 2019, 8, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Basta, M.N.; Gerety, P.A.; Serletti, J.M.; Kovach, S.J.; Fischer, J.P. A Systematic Review and Head-to-Head Meta-Analysis of Outcomes following Direct-to-Implant versus Conventional Two-Stage Implant Reconstruction. Plast. Reconstr. Surg. 2015, 136, 1135–1144. [Google Scholar] [CrossRef] [PubMed]
- Colwell, A.S.; Damjanovic, B.; Zahedi, B.; Medford-Davis, L.; Hertl, C.; Austen, W.G., Jr. Retrospective review of 331 consecutive immediate single-stage implant reconstructions with acellular dermal matrix: Indications, complications, trends, and costs. Plast. Reconstr. Surg. 2011, 128, 1170–1178. [Google Scholar] [CrossRef]
- Cordeiro, P.G. Discussion: Focus on technique: Two-stage implant-based breast reconstruction. Plast. Reconstr. Surg. 2012, 130, 116S–117S. [Google Scholar] [CrossRef]
- Cordeiro, P.G.; McCarthy, C.M. A single surgeon’s 12-year experience with tissue expander/implant breast reconstruction: Part II. An analysis of long-term complications, aesthetic outcomes, and patient satisfaction. Plast. Reconstr. Surg. 2006, 118, 832–839. [Google Scholar] [CrossRef]
- Cordeiro, P.G.; McCarthy, C.M. A single surgeon’s 12-year experience with tissue expander/implant breast reconstruction: Part I. A prospective analysis of early complications. Plast. Reconstr. Surg. 2006, 118, 825–831. [Google Scholar] [CrossRef]
- Glasberg, S.B. The Economics of Prepectoral Breast Reconstruction. Plast. Reconstr. Surg. 2017, 140, 49S–52S. [Google Scholar] [CrossRef] [PubMed]
- Glasberg, S.B.; Light, D. AlloDerm and Strattice in breast reconstruction: A comparison and techniques for optimizing outcomes. Plast. Reconstr. Surg. 2012, 129, 1223–1233. [Google Scholar] [CrossRef] [PubMed]
- Lennox, P.A.; Bovill, E.S.; Macadam, S.A. Evidence-Based Medicine: Alloplastic Breast Reconstruction. Plast. Reconstr. Surg. 2017, 140, 94e–108e. [Google Scholar] [CrossRef]
- Lindford, A.J.; Meretoja, T.J.; von Smitten, K.A.; Jahkola, T.A. Skin-sparing mastectomy and immediate breast reconstruction in the management of locally recurrent breast cancer. Ann. Surg. Oncol. 2010, 17, 1669–1674. [Google Scholar] [CrossRef] [PubMed]
- Meretoja, T.J.; von Smitten, K.A.; Kuokkanen, H.O.; Suominen, S.H.; Jahkola, T.A. Complications of skin-sparing mastectomy followed by immediate breast reconstruction: A prospective randomized study comparing high-frequency radiosurgery with conventional diathermy. Ann. Plast. Surg. 2008, 60, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Sbitany, H.; Lee, K.R. Optimizing Outcomes in 2-Stage Prepectoral Breast Reconstruction Utilizing Round Form-Stable Implants. Plast. Reconstr. Surg. 2019, 144, 43S–50S. [Google Scholar] [CrossRef] [PubMed]
- Srinivasa, D.R.; Holland, M.; Sbitany, H. Optimizing perioperative strategies to maximize success with prepectoral breast reconstruction. Gland Surg. 2019, 8, 19–26. [Google Scholar] [CrossRef]
- Vidya, R.; Berna, G.; Sbitany, H.; Nahabedian, M.; Becker, H.; Reitsamer, R.; Rancati, A.; Macmillan, D.; Cawthorn, S. Prepectoral implant-based breast reconstruction: A joint consensus guide from UK, European and USA breast and plastic reconstructive surgeons. Ecancermedicalscience 2019, 13, 927. [Google Scholar] [CrossRef] [Green Version]
- Sisti, A.; Huayllani, M.T.; Boczar, D.; Restrepo, D.J.; Spaulding, A.C.; Emmanuel, G.; Bagaria, S.P.; McLaughlin, S.A.; Parker, A.S.; Forte, A.J. Breast cancer in women: A descriptive analysis of the national cancer database. Acta Biomed. 2020, 91, 332–341. [Google Scholar] [CrossRef]
- Ball, J.F.; Huayllani, M.T.; Boczar, D.; Restrepo, D.J.; Spaulding, A.C.; Emmanuel, G.; Bagaria, S.P.; McLaughlin, S.A.; Parker, A.S.; Forte, A.J. A direct comparison of porcine (Strattice) and bovine (Surgimend) acellular dermal matrices in implant-based immediate breast reconstruction. JPRAS 2017, 70, 1076–1082. [Google Scholar] [CrossRef] [PubMed]
- Carminati, M.; Sempf, D.; Bonfirraro, P.P.; Devalle, L.; Verga, M.; Righi, B.; Mevio, G.; Leone, F.; Fenaroli, P.; Robotti, E. Immediate Implant-based Breast Reconstruction with Acellular Dermal Matrix Compared with Tissue-expander Breast Reconstruction: Rate of Infection. Plast. Reconstr. Surg. Glob. Open 2018, 6, e1949. [Google Scholar] [CrossRef] [PubMed]
- Chandarana, M.; Harries, S.; National Braxon Audit Study, G. Multicentre study of prepectoral breast reconstruction using acellular dermal matrix. BJS Open 2020, 4, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Eichler, C.; Schulz, C.; Vogt, N.; Warm, M. The Use of Acellular Dermal Matrices (ADM) in Breast Reconstruction: A Review. Surg. Technol. Int. 2017, 31, 53–60. [Google Scholar] [PubMed]
- Gravina, P.R.; Pettit, R.W.; Davis, M.J.; Winocour, S.J.; Selber, J.C. Evidence for the Use of Acellular Dermal Matrix in Implant-Based Breast Reconstruction. Semin. Plast. Surg. 2019, 33, 229–235. [Google Scholar] [CrossRef] [PubMed]
- Greig, H.; Roller, J.; Ziaziaris, W.; Van Laeken, N. A retrospective review of breast reconstruction outcomes comparing AlloDerm and DermaCELL. JPRAS Open 2019, 22, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Hinchcliff, K.M.; Orbay, H.; Busse, B.K.; Charvet, H.; Kaur, M.; Sahar, D.E. Comparison of two cadaveric acellular dermal matrices for immediate breast reconstruction: A prospective randomized trial. JPRAS 2017, 70, 568–576. [Google Scholar] [CrossRef] [Green Version]
- Kim, A.; Jung, J.H.; Choi, Y.L.; Pyon, J.K. Capsule biopsy of acellular dermal matrix (ADM) to predict future capsular contracture in two-stage prosthetic breast reconstruction. JPRAS 2019, 72, 1576–1606. [Google Scholar] [CrossRef]
- Kim, S.Y.; Bang, S.I. Impact of Acellular Dermal Matrix (ADM) Use under Mastectomy Flap Necrosis on Perioperative Outcomes of Prosthetic Breast Reconstruction. Aesthet. Plast. Surg. 2017, 41, 275–281. [Google Scholar] [CrossRef]
- Knabben, L.; Kanagalingam, G.; Imboden, S.; Gunthert, A.R. Acellular Dermal Matrix (Permacol®) for Heterologous Immediate Breast Reconstruction after Skin-Sparing Mastectomy in Patients with Breast Cancer: A Single-Institution Experience and a Review of the Literature. Front. Med. 2016, 3, 72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lardi, A.M.; Ho-Asjoe, M.; Junge, K.; Farhadi, J. Capsular contracture in implant based breast reconstruction-the effect of porcine acellular dermal matrix. Gland Surg. 2017, 6, 49–56. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.U.; Bobr, A.; Torres-Mora, J. Radiologic-Pathologic Correlation: Acellular Dermal Matrix (Alloderm®) Used in Breast Reconstructive Surgery. J. Clin. Imaging Sci. 2017, 7, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.S.; Kim, J.S.; Lee, J.H.; Lee, J.W.; Lee, J.; Park, H.Y.; Yang, J.D. Prepectoral breast reconstruction with complete implant coverage using double-crossed acellular dermal matrixs. Gland Surg. 2019, 8, 748–757. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Hou, J.; Li, Z.; Wang, B.; Sun, J. Efficacy of Acellular Dermal Matrix in Capsular Contracture of Implant-Based Breast Reconstruction: A Single-Arm Meta-analysis. Aesthet. Plast. Surg. 2020. [Google Scholar] [CrossRef] [PubMed]
- Mendenhall, S.D.; Anderson, L.A.; Ying, J.; Boucher, K.M.; Neumayer, L.A.; Agarwal, J.P. The BREASTrial Stage II: ADM Breast Reconstruction Outcomes from Definitive Reconstruction to 3 Months Postoperative. Plast. Reconstr. Surg. Glob. Open 2017, 5, e1209. [Google Scholar] [CrossRef] [PubMed]
- Negenborn, V.L.; Dikmans, R.E.G.; Bouman, M.B.; Wilschut, J.A.; Mullender, M.G.; Salzberg, C.A. Patient-reported Outcomes after ADM-assisted Implant-based Breast Reconstruction: A Cross-sectional Study. Plast. Reconstr. Surg. Glob. Open 2018, 6, e1654. [Google Scholar] [CrossRef] [PubMed]
- Onesti, M.G.; Di Taranto, G.; Ribuffo, D.; Scuderi, N. ADM-assisted prepectoral breast reconstruction and skin reduction mastectomy: Expanding the indications for subcutaneous reconstruction. JPRAS 2019. [Google Scholar] [CrossRef]
- Paprottka, F.J.; Krezdorn, N.; Sorg, H.; Konneker, S.; Bontikous, S.; Robertson, I.; Schlett, C.L.; Dohse, N.K.; Hebebrand, D. Evaluation of Complication Rates after Breast Surgery Using Acellular Dermal Matrix: Median Follow-Up of Three Years. Plast. Surg. Int. 2017, 2017, 1283735. [Google Scholar] [CrossRef] [Green Version]
- Singla, A.; Singla, A.; Lai, E.; Caminer, D. Subcutaneously Placed Breast Implants after a Skin-Sparing Mastectomy: Do We Always Need ADM? Plast. Reconstr. Surg. Glob. Open 2017, 5, e1371. [Google Scholar] [CrossRef]
- Tsay, C.; Zhu, V.; Sturrock, T.; Shah, A.; Kwei, S. A 3D Mammometric Comparison of Implant-Based Breast Reconstruction with and Without Acellular Dermal Matrix (ADM). Aesthet. Plast. Surg. 2018, 42, 49–58. [Google Scholar] [CrossRef]
- Vela-Lasagabaster, A.; Benito-Duque, P.; Ordonez-Maygua, J. Breast Prosthetic Reconstruction: Tips and Tricks on ADM Position. Aesthet. Plast. Surg. 2019, 43, 559–561. [Google Scholar] [CrossRef]
- Zenn, M.; Venturi, M.; Pittman, T.; Spear, S.; Gurtner, G.; Robb, G.; Mesbahi, A.; Dayan, J. Optimizing Outcomes of Postmastectomy Breast Reconstruction with Acellular Dermal Matrix: A Review of Recent Clinical Data. Eplasty 2017, 17, e18. [Google Scholar] [PubMed]
- Chao, A.H. A Review of the Use of Acellular Dermal Matrices in Postmastectomy Immediate Breast Reconstruction. Plast. Surg. Nurs. 2015, 35, 131–134. [Google Scholar] [CrossRef] [PubMed]
- Frey, J.D.; Salibian, A.A.; Karp, N.S.; Choi, M. Implant-Based Breast Reconstruction: Hot Topics, Controversies, and New Directions. Plast. Reconstr. Surg. 2019, 143, 404e–416e. [Google Scholar] [CrossRef]
- Frey, J.D.; Salibian, A.A.; Levine, J.P.; Karp, N.S.; Choi, M. Evolution of the Surgical Technique for “Breast in a Day” Direct-to-Implant Breast Reconstruction: Transitioning from Dual-Plane to Prepectoral Implant Placement. Plast. Reconstr. Surg. 2020, 145, 647e–648e. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, N.M.; Fischer, J.P.; Basta, M.N.; Nahabedian, M.Y. Is Single-Stage Prosthetic Reconstruction Cost Effective? A Cost-Utility Analysis for the Use of Direct-to-Implant Breast Reconstruction Relative to Expander-Implant Reconstruction in Postmastectomy Patients. Plast. Reconstr. Surg. 2016, 138, 537–547. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, N.M.; Purnell, C.; Nahabedian, M.Y.; Freed, G.L.; Nigriny, J.F.; Rosen, J.M.; Rosson, G.D. The cost effectiveness of the DIEP flap relative to the muscle-sparing TRAM flap in postmastectomy breast reconstruction. Plast. Reconstr. Surg. 2015, 135, 948–958. [Google Scholar] [CrossRef] [PubMed]
- Salibian, A.A.; Frey, J.D.; Choi, M.; Karp, N.S. Subcutaneous Implant-based Breast Reconstruction with Acellular Dermal Matrix/Mesh: A Systematic Review. Plast. Reconstr. Surg. Glob. Open 2016, 4, e1139. [Google Scholar] [CrossRef]
- Delgado, J.F.; Garcia-Guilarte, R.F.; Palazuelo, M.R.; Mendez, J.I.; Perez, C.C. Immediate breast reconstruction with direct, anatomic, gel-cohesive, extra-projection prosthesis: 400 cases. Plast. Reconstr. Surg. 2010, 125, 1599–1605. [Google Scholar] [CrossRef]
- Gschwantler-Kaulich, D.; Schrenk, P.; Bjelic-Radisic, V.; Unterrieder, K.; Leser, C.; Fink-Retter, A.; Salama, M.; Singer, C. Mesh versus acellular dermal matrix in immediate implant-based breast reconstruction—A prospective randomized trial. Eur. J. Surg. Oncol. 2016, 42, 665–671. [Google Scholar] [CrossRef]
- Salzberg, C.A.; Ashikari, A.Y.; Koch, R.M.; Chabner-Thompson, E. An 8-year experience of direct-to-implant immediate breast reconstruction using human acellular dermal matrix (AlloDerm). Plast. Reconstr. Surg. 2011, 127, 514–524. [Google Scholar] [CrossRef]
- Agusti, A.; Ward, A.; Montgomery, C.; Mohammed, K.; Gui, G.P. Aesthetic and oncologic outcomes after one-stage immediate breast reconstruction using a permanent biodimensional expandable implant. J. Plast. Reconstr. Aesthet. Surg. 2016, 69, 211–220. [Google Scholar] [CrossRef]
- Bailey, C.R.; Ogbuagu, O.; Baltodano, P.A.; Simjee, U.F.; Manahan, M.A.; Cooney, D.S.; Jacobs, L.K.; Tsangaris, T.N.; Cooney, C.M.; Rosson, G.D. Quality-of-Life Outcomes Improve with Nipple-Sparing Mastectomy and Breast Reconstruction. Plast. Reconstr. Surg. 2017, 140, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Bailey, M.H.; Smith, J.W.; Casas, L.; Johnson, P.; Serra, E.; de la Fuente, R.; Sullivan, M.; Scanlon, E.F. Immediate breast reconstruction: Reducing the risks. Plast. Reconstr. Surg. 1989, 83, 845–851. [Google Scholar] [CrossRef] [PubMed]
- Fischer, J.P.; Cleveland, E.C.; Nelson, J.A.; Kovach, S.J.; Serletti, J.M.; Wu, L.C.; Kanchwala, S. Breast reconstruction in the morbidly obese patient: Assessment of 30-day complications using the 2005 to 2010 National Surgical Quality Improvement Program data sets. Plast. Reconstr. Surg. 2013, 132, 750–761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fischer, J.P.; Wes, A.M.; Tuggle, C.T.; Serletti, J.M.; Wu, L.C. Risk analysis and stratification of surgical morbidity after immediate breast reconstruction. J. Am. Coll. Surg. 2013, 217, 780–787. [Google Scholar] [CrossRef]
- Fischer, J.P.; Wes, A.M.; Tuggle, C.T.; Serletti, J.M., 3rd; Wu, L.C. Risk analysis of early implant loss after immediate breast reconstruction: A review of 14,585 patients. J. Am. Coll. Surg. 2013, 217, 983–990. [Google Scholar] [CrossRef]
- Hvilsom, G.B.; Friis, S.; Frederiksen, K.; Steding-Jessen, M.; Henriksen, T.F.; Lipworth, L.; McLaughlin, J.K.; Elberg, J.J.; Damsgaard, T.E.; Holmich, L.R. The clinical course of immediate breast implant reconstruction after breast cancer. Acta Oncol. 2011, 50, 1045–1052. [Google Scholar] [CrossRef]
- Hvilsom, G.B.; Holmich, L.R.; Frederiksen, K.; Steding-Jessen, M.; Friis, S.; Dalton, S.O. Socioeconomic position and breast reconstruction in Danish women. Acta Oncol. 2011, 50, 265–273. [Google Scholar] [CrossRef] [Green Version]
- Hvilsom, G.B.; Holmich, L.R.; Steding-Jessen, M.; Frederiksen, K.; Henriksen, T.F.; Lipworth, L.; McLaughlin, J.; Elberg, J.J.; Damsgaard, T.E.; Friis, S. Delayed breast implant reconstruction: Is radiation therapy associated with capsular contracture or reoperations? Ann. Plast. Surg. 2012, 68, 246–252. [Google Scholar] [CrossRef]
- Hvilsom, G.B.; Holmich, L.R.; Steding-Jessen, M.; Frederiksen, K.; Henriksen, T.F.; Lipworth, L.; McLaughlin, J.K.; Elberg, J.J.; Damsgaard, T.E.; Friis, S. Delayed breast implant reconstruction: A 10-year prospective study. J. Plast. Reconstr. Aesthet. Surg. 2011, 64, 1466–1474. [Google Scholar] [CrossRef]
- Jansen, L.A.; Macadam, S.A. The use of AlloDerm in postmastectomy alloplastic breast reconstruction: Part I. A systematic review. Plast. Reconstr. Surg. 2011, 127, 2232–2244. [Google Scholar] [CrossRef]
- Jansen, L.A.; Macadam, S.A. The use of AlloDerm in postmastectomy alloplastic breast reconstruction: Part II. A cost analysis. Plast. Reconstr. Surg. 2011, 127, 2245–2254. [Google Scholar] [CrossRef]
- Menez, T.; Michot, A.; Tamburino, S.; Weigert, R.; Pinsolle, V. Multicenter evaluation of quality of life and patient satisfaction after breast reconstruction, a long-term retrospective study. Ann. Chir. Plast. Esthet. 2018, 63, 126–133. [Google Scholar] [CrossRef]
- Cemal, Y.; Albornoz, C.R.; Disa, J.J.; McCarthy, C.M.; Mehrara, B.J.; Pusic, A.L.; Cordeiro, P.G.; Matros, E. A paradigm shift in U.S. breast reconstruction: Part 2. The influence of changing mastectomy patterns on reconstructive rate and method. Plast. Reconstr. Surg. 2013, 131, 320e–326e. [Google Scholar] [CrossRef]
- Cuomo, R.; Nisi, G.; Grimaldi, L.; Brandi, C.; D’Aniello, C. Silicone breast implants and echocardiographic interactions: A brand new study. Indian J. Plast. Surg. 2016, 49, 430–431. [Google Scholar] [CrossRef]
- Hirsch, E.M.; Seth, A.K.; Dumanian, G.A.; Kim, J.Y.; Mustoe, T.A.; Galiano, R.D.; Fine, N.A. Outcomes of immediate tissue expander breast reconstruction followed by reconstruction of choice in the setting of postmastectomy radiation therapy. Ann. Plast. Surg. 2014, 72, 274–278. [Google Scholar] [CrossRef] [Green Version]
- Hirsch, E.M.; Seth, A.K.; Fine, N.A. Outcomes of immediate tissue expander breast reconstruction followed by reconstruction of choice in the setting of postmastectomy radiation therapy: Reply. Ann. Plast. Surg. 2015, 74, 271–272. [Google Scholar] [CrossRef]
- 2012 Plastic Surgery Statistics Report. Available online: https://www.plasticsurgery.org/news/plastic-surgery-statistics?sub=2012+Plastic+Surgery+Statistics (accessed on 26 May 2020).
- 2018 Plastic Surgery Statistics Report. Available online: https://www.plasticsurgery.org/news/plastic-surgery-statistics (accessed on 26 May 2020).
- Negenborn, V.L.; Smit, J.M.; Dikmans, R.E.G.; Winters, H.A.H.; Twisk, J.W.R.; Ruhe, P.Q.; Mureau, M.A.M.; Tuinder, S.; Eltahir, Y.; Posch, N.A.S.; et al. Short-term cost-effectiveness of one-stage implant-based breast reconstruction with an acellular dermal matrix versus two-stage expander-implant reconstruction from a multicentre randomized clinical trial. Br. J. Surg. 2019, 106, 586–595. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, A.M.; Koolen, P.G.; Ganor, O.; Markarian, M.K.; Tobias, A.M.; Lee, B.T.; Lin, S.J.; Mureau, M.A. Does acellular dermal matrix really improve aesthetic outcome in tissue expander/implant-based breast reconstruction? Aesthet. Plast. Surg. 2015, 39, 359–368. [Google Scholar] [CrossRef]
- Nguyen, K.T.; Mioton, L.M.; Smetona, J.T.; Seth, A.K.; Kim, J.Y. Esthetic Outcomes of ADM-Assisted Expander-Implant Breast Reconstruction. Eplasty 2012, 12, e58. [Google Scholar]
- Ho, A.L.; Klassen, A.F.; Cano, S.; Scott, A.M.; Pusic, A.L. Optimizing patient-centered care in breast reconstruction: The importance of preoperative information and patient-physician communication. Plast. Reconstr. Surg. 2013, 132, 212e–220e. [Google Scholar] [CrossRef]
- Ho, A.L.; Tyldesley, S.; Macadam, S.A.; Lennox, P.A. Skin-sparing mastectomy and immediate autologous breast reconstruction in locally advanced breast cancer patients: A UBC perspective. Ann. Surg. Oncol. 2012, 19, 892–900. [Google Scholar] [CrossRef]
- Ho, G.; Nguyen, T.J.; Shahabi, A.; Hwang, B.H.; Chan, L.S.; Wong, A.K. A systematic review and meta-analysis of complications associated with acellular dermal matrix-assisted breast reconstruction. Ann. Plast. Surg. 2012, 68, 346–356. [Google Scholar] [CrossRef]
- Tom, L.; Broer, N.; Hoang, D.; Narayan, D. Novel use of acellularized dermis for breast reconstruction. Plast. Reconstr. Surg. 2011, 128, 31e–33e. [Google Scholar] [CrossRef]
- Colwell, A.S.; Taylor, E.M. Recent Advances in Implant-Based Breast Reconstruction. Plast. Reconstr. Surg. 2020, 145, 421e–432e. [Google Scholar] [CrossRef]
- Elliott, L.F.; Hartrampf, C.R., Jr. Breast reconstruction: Progress in the past decade. World J. Surg. 1990, 14, 763–775. [Google Scholar] [CrossRef]
- Cuomo, R.; Zerini, I.; Botteri, G.; Barberi, L.; Nisi, G.; D’Aniello, C. Postsurgical pain related to breast implant: Reduction with lipofilling procedure. In Vivo 2014, 28, 993–996. [Google Scholar]
- Juhl, A.A.; Christensen, S.; Zachariae, R.; Damsgaard, T.E. Unilateral breast reconstruction after mastectomy—Patient satisfaction, aesthetic outcome and quality of life. Acta Oncol. 2017, 56, 225–231. [Google Scholar] [CrossRef] [Green Version]
- Juhl, A.A.; Damsgaard, T.E.; O’Connor, M.; Christensen, S.; Zachariae, R. Personality Traits as Predictors of Quality of Life and Body Image after Breast Reconstruction. Plast. Reconstr. Surg. Glob. Open 2017, 5, e1341. [Google Scholar] [CrossRef]
- Breuing, K.H.; Colwell, A.S. Immediate breast tissue expander-implant reconstruction with inferolateral AlloDerm hammock and postoperative radiation: A preliminary report. Eplasty 2009, 9, e16. [Google Scholar]
- Colwell, A.S.; Tessler, O.; Lin, A.M.; Liao, E.; Winograd, J.; Cetrulo, C.L.; Tang, R.; Smith, B.L.; Austen, W.G., Jr. Breast reconstruction following nipple-sparing mastectomy: Predictors of complications, reconstruction outcomes, and 5-year trends. Plast. Reconstr. Surg. 2014, 133, 496–506. [Google Scholar] [CrossRef]
- Margulies, I.G.; Zoghbi, Y.; Jacobs, J.; Cate, S.P.; Salzberg, C.A. Direct to implant breast reconstruction: Visualized technique. Gland Surg. 2019, 8, S247–S250. [Google Scholar] [CrossRef]
- Salzberg, C.A.; Ashikari, A.Y.; Berry, C.; Hunsicker, L.M. Acellular Dermal Matrix-Assisted Direct-to-Implant Breast Reconstruction and Capsular Contracture: A 13-Year Experience. Plast. Reconstr. Surg. 2016, 138, 329–337. [Google Scholar] [CrossRef]
- Scheflan, M.; Colwell, A.S. Tissue Reinforcement in Implant-based Breast Reconstruction. Plast. Reconstr. Surg. Glob. Open 2014, 2, e192. [Google Scholar] [CrossRef]
- Maisel Lotan, A.; Ben Yehuda, D.; Allweis, T.M.; Scheflan, M. Comparative Study of Meshed and Nonmeshed Acellular Dermal Matrix in Immediate Breast Reconstruction. Plast. Reconstr. Surg. 2019, 144, 1045–1053. [Google Scholar] [CrossRef]
- Nelson, J.A.; Allen, R.J., Jr.; Polanco, T.; Shamsunder, M.; Patel, A.R.; McCarthy, C.M.; Matros, E.; Dayan, J.H.; Disa, J.J.; Cordeiro, P.G.; et al. Long-term Patient-reported Outcomes Following Postmastectomy Breast Reconstruction: An 8-year Examination of 3268 Patients. Ann. Surg. 2019, 270, 473–483. [Google Scholar] [CrossRef]
- Baxter, R.A. Update on the split-muscle technique for breast augmentation: Prevention and correction of animation distortion and double-bubble deformity. Aesthet. Plast. Surg. 2011, 35, 426–429. [Google Scholar] [CrossRef]
- Baxter, R.A. Long-term Follow-up with AlloDerm in Breast Reconstruction. Plast. Reconstr. Surg. Glob. Open 2013, 1, 1–2. [Google Scholar] [CrossRef]
- Breuing, K.H.; Colwell, A.S. Inferolateral AlloDerm hammock for implant coverage in breast reconstruction. Ann. Plast. Surg. 2013, 59, 250–255. [Google Scholar] [CrossRef]
- D’Aniello, C.; Cuomo, R.; Grimaldi, L.; Brandi, C.; Sisti, A.; Tassinari, J.; Nisi, G. Superior Pedicle Mammaplasty without Parenchymal Incisions after Massive Weight Loss. J. Investig. Surg. 2017, 30, 410–420. [Google Scholar] [CrossRef]
- Berna, G.; Cawthorn, S.J.; Papaccio, G.; Balestrieri, N. Evaluation of a novel breast reconstruction technique using the Braxon® acellular dermal matrix: A new muscle-sparing breast reconstruction. ANZ J. Surg. 2017, 87, 493–498. [Google Scholar] [CrossRef] [PubMed]
- Wazir, U.; Mokbel, K. The evolving role of pre-pectoral ADM-assisted implant-based immediate breast reconstruction following skin-sparing mastectomy. Am. J. Surg. 2018, 216, 639–640. [Google Scholar] [CrossRef] [PubMed]
- Vidya, R.; Masia, J.; Cawthorn, S.; Berna, G.; Bozza, F.; Gardetto, A.; Kolacinska, A.; Dell’Antonia, F.; Tiengo, C.; Bassetto, F.; et al. Evaluation of the effectiveness of the prepectoral breast reconstruction with Braxon dermal matrix: First multicenter European report on 100 cases. Breast J. 2017, 23, 670–676. [Google Scholar] [CrossRef]
- Kuwahara, M.; Hatoko, M.; Tada, H.; Tanaka, A.; Yurugi, S.; Mashiba, K. Distortion and movement of the expander during skin expansion. Scand. J. Plast. Reconstr. Surg. Hand Surg. 2003, 37, 22–27. [Google Scholar] [CrossRef]
- Cheng, H.M.; McMillan, C.; Lipa, J.E.; Snell, L. A Qualitative Assessment of the Journey to Delayed Breast Reconstruction. Plast. Surg. 2017, 25, 157–162. [Google Scholar] [CrossRef]
- Becker, H.; Lind, J.G., 2nd; Hopkins, E.G. Immediate Implant-based Prepectoral Breast Reconstruction Using a Vertical Incision. Plast. Reconstr. Surg. Glob. Open 2015, 3, e412. [Google Scholar] [CrossRef] [PubMed]
- Baker, B.G.; Irri, R.; MacCallum, V.; Chattopadhyay, R.; Murphy, J.; Harvey, J.R. A Prospective Comparison of Short-Term Outcomes of Subpectoral and Prepectoral Strattice-Based Immediate Breast Reconstruction. Plast. Reconstr. Surg. 2018, 141, 1077–1084. [Google Scholar] [CrossRef]
- Sigalove, S. Prepectoral breast reconstruction and radiotherapy—A closer look. Gland Surg. 2019, 8, 67–74. [Google Scholar] [CrossRef]
- Walia, G.S.; Aston, J.; Bello, R.; Mackert, G.A.; Pedreira, R.A.; Cho, B.H.; Carl, H.M.; Rada, E.M.; Rosson, G.D.; Sacks, J.M. Prepectoral Versus Subpectoral Tissue Expander Placement: A Clinical and Quality of Life Outcomes Study. Plast. Reconstr. Surg. Glob. Open 2018, 6, e1731. [Google Scholar] [CrossRef]
- Fracol, M.; Qiu, C.S.; Feld, L.N.; Chiu, W.K.; Kim, J.Y.S. Myotomy-Capsulotomy with Intramuscular Fat Grafting: A Novel Technique for Secondary Treatment of Prepectoral Upper Pole Defects in Breast Reconstruction. Aesthet. Surg. J. Am. Soc. Aesthet. Plast. Surg. 2019, 39, 454–459. [Google Scholar] [CrossRef]
- Cuomo, R.; Giardino, F.R.; Neri, A.; Nisi, G.; Brandi, C.; Zerini, I.; Han, J.; Grimaldi, L. Optimization of Prepectoral Breast Reconstruction. Breast Care 2020. [Google Scholar] [CrossRef]
- Pittman, T.A.; Abbate, O.A.; Economides, J.M. The P1 Method: Prepectoral Breast Reconstruction to Minimize the Palpable Implant Edge and Upper Pole Rippling. Ann. Plast. Surg. 2018, 80, 487–492. [Google Scholar] [CrossRef]
- Tasoulis, M.K.; Teoh, V.; Khan, A.; Montgomery, C.; Mohammed, K.; Gui, G. Acellular dermal matrices as an adjunct to implant breast reconstruction: Analysis of outcomes and complications. Eur. J. Surg. Oncol. 2020, 46, 511–515. [Google Scholar] [CrossRef]
- Lohmander, F.; Lagergren, J.; Roy, P.G.; Johansson, H.; Brandberg, Y.; Eriksen, C.; Frisell, J. Implant Based Breast Reconstruction with Acellular Dermal Matrix: Safety Data from an Open-label, Multicenter, Randomized, Controlled Trial in the Setting of Breast Cancer Treatment. Ann. Surg. 2019, 269, 836–841. [Google Scholar] [CrossRef]
- Antony, A.K.; McCarthy, C.M.; Cordeiro, P.G.; Mehrara, B.J.; Pusic, A.L.; Teo, E.H.; Arriaga, A.F.; Disa, J.J. Acellular human dermis implantation in 153 immediate two-stage tissue expander breast reconstructions: Determining the incidence and significant predictors of complications. Plast. Reconstr. Surg. 2010, 125, 1606–1614. [Google Scholar] [CrossRef]
- Bernini, M.; Calabrese, C.; Cecconi, L.; Santi, C.; Gjondedaj, U.; Roselli, J.; Nori, J.; Fausto, A.; Orzalesi, L.; Casella, D. Subcutaneous Direct-to-Implant Breast Reconstruction: Surgical, Functional, and Aesthetic Results after Long-Term Follow-Up. Plast. Reconstr. Surg. Glob. Open 2015, 3, e574. [Google Scholar] [CrossRef]
- Ibrahim, A.M.; Shuster, M.; Koolen, P.G.; Kim, K.; Taghinia, A.H.; Sinno, H.H.; Lee, B.T.; Lin, S.J. Analysis of the National Surgical Quality Improvement Program database in 19,100 patients undergoing implant-based breast reconstruction: Complication rates with acellular dermal matrix. Plast. Reconstr. Surg. 2013, 132, 1057–1066. [Google Scholar] [CrossRef]
- Kamali, P.; Koolen, P.G.; Ibrahim, A.M.; Paul, M.A.; Dikmans, R.E.; Schermerhorn, M.L.; Lee, B.T.; Lin, S.J. Analyzing Regional Differences over a 15-Year Trend of One-Stage versus Two-Stage Breast Reconstruction in 941,191 Postmastectomy Patients. Plast. Reconstr. Surg. 2016, 138, 1e–14e. [Google Scholar] [CrossRef]
- Abedi, N.; Ho, A.L.; Knox, A.; Tashakkor, Y.; Omeis, T.; Van Laeken, N.; Lennox, P.; Macadam, S.A. Predictors of Mastectomy Flap Necrosis in Patients Undergoing Immediate Breast Reconstruction: A Review of 718 Patients. Ann. Plast. Surg. 2016, 76, 629–634. [Google Scholar] [CrossRef]
- Rubino, C.; Brongo, S.; Pagliara, D.; Cuomo, R.; Abbinante, G.; Campitiello, N.; Santanelli, F.; Chessa, D. Infections in breast implants: A review with a focus on developing countries. J. Infect. Dev. Ctries 2014, 8, 1089–1095. [Google Scholar] [CrossRef] [Green Version]
- Powell-Brett, S.; Goh, S. Clinical and patient reported outcomes in breast reconstruction using acellular dermal matrix. JPRAS Open 2018, 17, 31–38. [Google Scholar] [CrossRef]
- Bindingnavele, V.; Gaon, M.; Ota, K.S.; Kulber, D.A.; Lee, D.J. Use of acellular cadaveric dermis and tissue expansion in postmastectomy breast reconstruction. J. Plast. Reconstr. Aesthet. Surg. 2007, 60, 1214–1218. [Google Scholar] [CrossRef]
- Disa, J.J.; Ad-El, D.D.; Cohen, S.M.; Cordeiro, P.G.; Hidalgo, D.A. The premature removal of tissue expanders in breast reconstruction. Plast. Reconstr. Surg. 1999, 104, 1662–1665. [Google Scholar] [CrossRef]
- Munabi, N.C.; Olorunnipa, O.B.; Goltsman, D.; Rohde, C.H.; Ascherman, J.A. The ability of intra-operative perfusion mapping with laser-assisted indocyanine green angiography to predict mastectomy flap necrosis in breast reconstruction: A prospective trial. J. Plast. Reconstr. Aesthet. Surg. 2014, 67, 449–455. [Google Scholar] [CrossRef]
- Apte, A.; Walsh, M.; Balaji, P.; Khor, B.; Chandrasekharan, S.; Chakravorty, A. Single stage immediate breast reconstruction with acellular dermal matrix and implant: Defining the risks and outcomes of post-mastectomy radiotherapy. Surgeon 2019. [Google Scholar] [CrossRef]
- Apte, A.; Walsh, M.; Chandrasekharan, S.; Chakravorty, A. Single-stage immediate breast reconstruction with acellular dermal matrix: Experience gained and lessons learnt from patient reported outcome measures. Eur. J. Surg. Oncol. 2016, 42, 39–44. [Google Scholar] [CrossRef]
- Endara, M.; Chen, D.; Verma, K.; Nahabedian, M.Y.; Spear, S.L. Breast reconstruction following nipple-sparing mastectomy: A systematic review of the literature with pooled analysis. Plast. Reconstr. Surg. 2013, 132, 1043–1054. [Google Scholar] [CrossRef]
- Hammond, D.C.; Schmitt, W.P.; O’Connor, E.A. Treatment of breast animation deformity in implant-based reconstruction with pocket change to the subcutaneous position. Plast. Reconstr. Surg. 2015, 135, 1540–1544. [Google Scholar] [CrossRef]
- Pittman, T.A.; Fan, K.L.; Knapp, A.; Frantz, S.; Spear, S.L. Comparison of Different Acellular Dermal Matrices in Breast Reconstruction: The 50/50 Study. Plast. Reconstr. Surg. 2017, 139, 521–528. [Google Scholar] [CrossRef]
- Spear, S.L.; Masden, D.; Rao, S.S.; Nahabedian, M.Y. Long-term outcomes of failed prosthetic breast reconstruction. Ann. Plast. Surg. 2013, 71, 286–291. [Google Scholar] [CrossRef]
- Spear, S.L.; Schwartz, J.; Dayan, J.H.; Clemens, M.W. Outcome assessment of breast distortion following submuscular breast augmentation. Aesthet. Plast. Surg. 2009, 33, 44–48. [Google Scholar] [CrossRef]
- Spear, S.L.; Sher, S.R.; Al-Attar, A.; Pittman, T. Applications of acellular dermal matrix in revision breast reconstruction surgery. Plast. Reconstr. Surg. 2014, 133, 1–10. [Google Scholar] [CrossRef]
- Nelson, J.A.; Sobti, N.; Patel, A.; Matros, E.; McCarthy, C.M.; Dayan, J.H.; Disa, J.J.; Cordeiro, P.G.; Mehrara, B.J.; Pusic, A.L.; et al. The Impact of Obesity on Patient-Reported Outcomes Following Autologous Breast Reconstruction. Ann. Surg. Oncol. 2019. [Google Scholar] [CrossRef]
- Sadok, N.; Krabbe-Timmerman, I.S.; de Bock, G.H.; Werker, P.M.N.; Jansen, L. The Effect of Smoking and Body Mass Index on the Complication Rate of Alloplastic Breast Reconstruction. Scand. J. Surg. 2019. [Google Scholar] [CrossRef] [Green Version]
- Srinivasa, D.R.; Clemens, M.W.; Qi, J.; Hamill, J.B.; Kim, H.M.; Pusic, A.L.; Wilkins, E.G.; Butler, C.E.; Garvey, P.B. Obesity and Breast Reconstruction: Complications and Patient-Reported Outcomes in a Multicenter, Prospective Study. Plast. Reconstr. Surg. 2020, 145, 481e–490e. [Google Scholar] [CrossRef]
Figure 1.
Meshed ADM used to cover the inferolateral aspect of the implant in submuscular breast reconstruction. ADM: Acellular dermal matrix.
Figure 1.
Meshed ADM used to cover the inferolateral aspect of the implant in submuscular breast reconstruction. ADM: Acellular dermal matrix.

Figure 2.
ADM-assisted pre-pectoral breast reconstruction with vertical scar.

© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Cuomo, R. Submuscular and Pre-pectoral ADM Assisted Immediate Breast Reconstruction: A Literature Review. Medicina 2020, 56, 256. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56060256
AMA Style
Cuomo R. Submuscular and Pre-pectoral ADM Assisted Immediate Breast Reconstruction: A Literature Review. Medicina. 2020; 56(6):256. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56060256
Chicago/Turabian StyleCuomo, Roberto. 2020. "Submuscular and Pre-pectoral ADM Assisted Immediate Breast Reconstruction: A Literature Review" Medicina 56, no. 6: 256. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56060256