Tumor Suppressors—HTRA Proteases and Interleukin-12—in Pediatric Asthma and Allergic Rhinitis Patients

 , , , , , , , ,
, , , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients
2.3. Control Group
2.4. HTRA and IL-12 Levels Analysis
2.5. Statistical Analysis
3. Results
3.1. Patients Characteristics
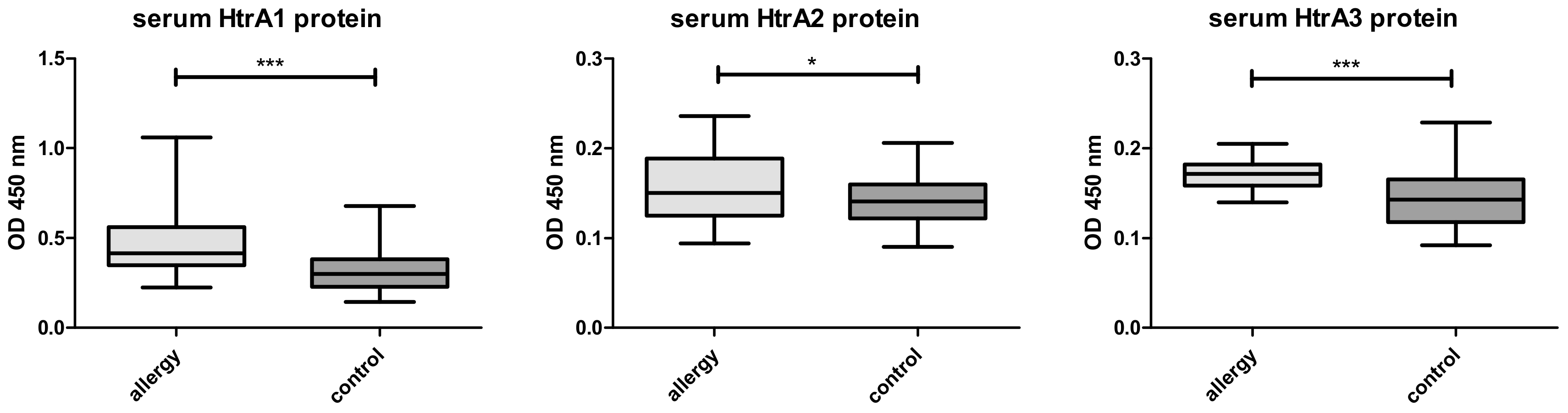
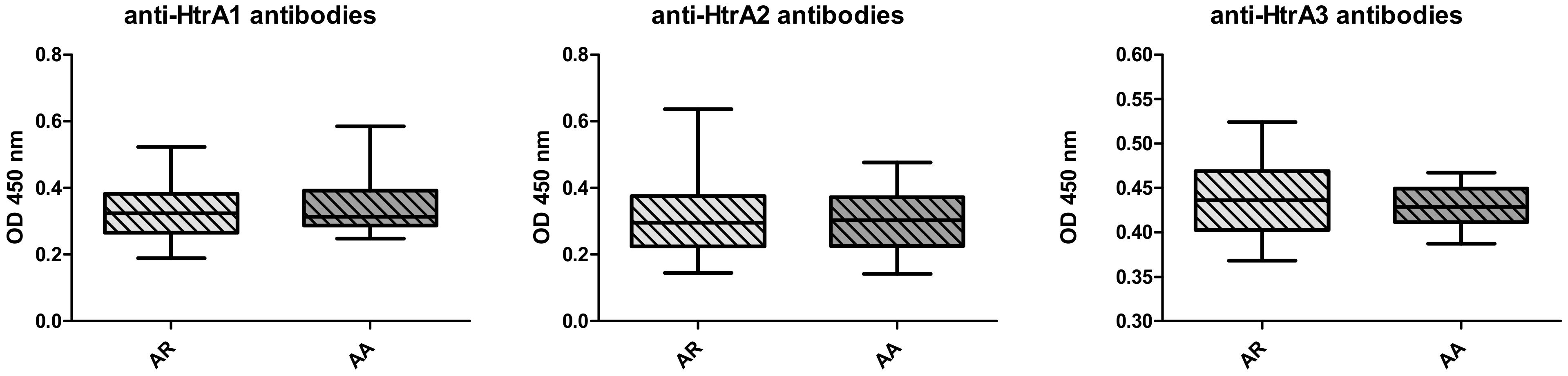
3.2. Serum HTRA Analysis
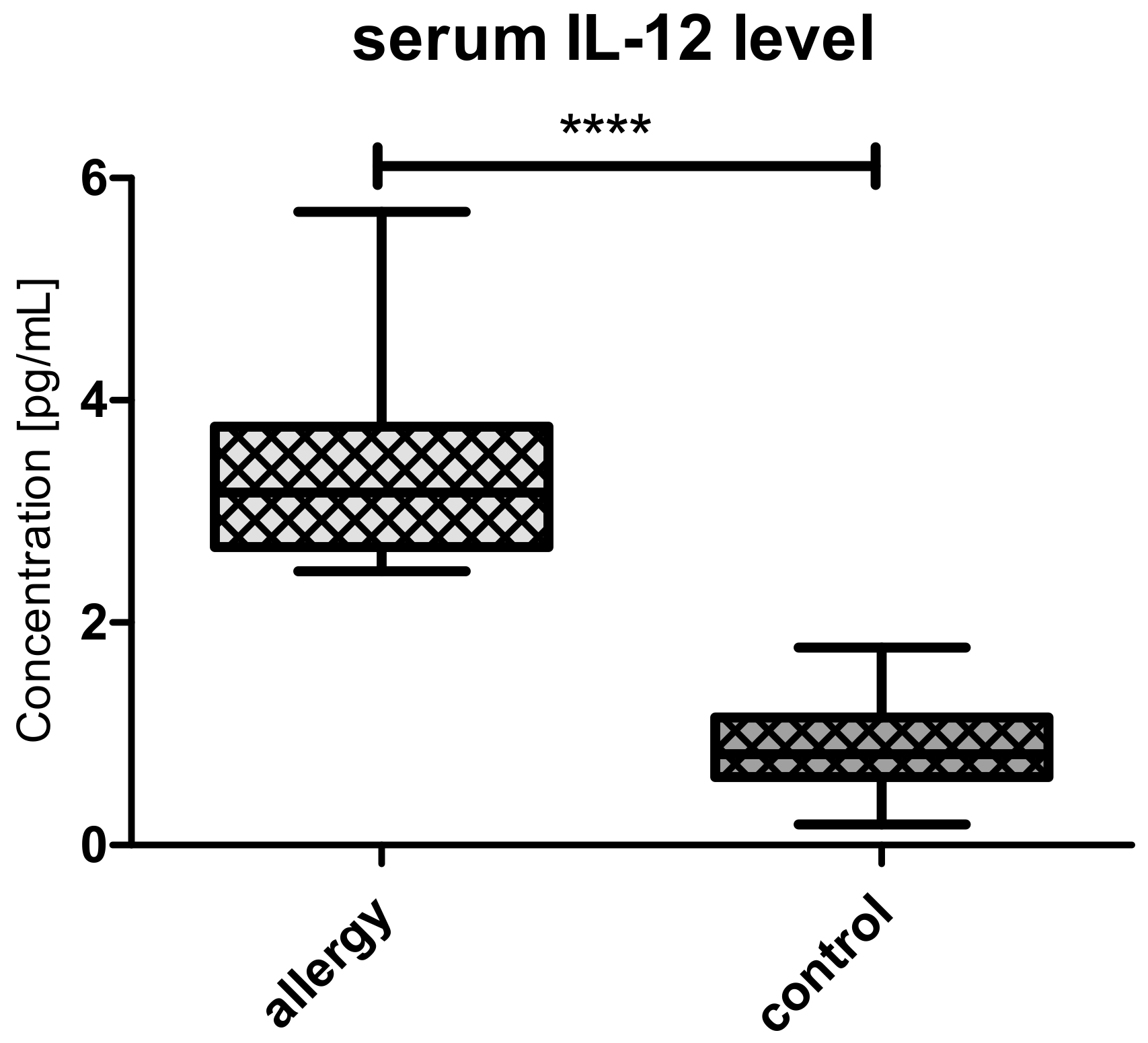
3.3. Serum Il-12 Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cui, A.H.; Zhao, J.; Liu, S.H.; Hao, Y.S. Associations of Il-4, Il-6, and Il-12 levels in peripheral blood with lung function, cellular immune function, and quality of life in children with moderate-to-severe asthma. Medicine 2017, 96, 12. [Google Scholar] [CrossRef] [PubMed]
- Zicari, A.M.; De Castro, G.; Leonardi, L.; Duse, M. Update on rhinitis and rhinosinusitis. Pediatr. Allergy Immunol. 2020, 31, 32–33. [Google Scholar] [CrossRef] [PubMed]
- Cui, Y.; Hill, A.W. Atopy and specific cancer sites: a review of epidemiological studies. Clinic. Rev. Allerg. Immunol. 2016, 51, 338–352. [Google Scholar] [CrossRef] [PubMed]
- Muir, A.B.; Whelan, K.A.; Dougherty, M.K.; Aaron, B.; Navarre, B.; Aceves, S.S.; Dellon, E.S.; Jensen, E.T. The potential for malignancy from atopic disorders and allergic inflammation: A systematic review and meta-analysis. Clin. Exp. Allergy. 2020, 50, 147–159. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi, F.; Shirkhoda, M. Allergy-related diseases and risk of breast cancer: the role of skewed immune system on this association. Allerg. Rhinol. 2019, 10, 1–14. [Google Scholar]
- Singer, J.; Achatz-Straussberger, G.; Bentley-Lukschal, A.; Fazekas-Singer, J.; Achatz, G.; Karagiannis, S.N.; Jensen-Jarolim, E. Allergooncology: High innate IgE levels are decisive for the survival of cancer-bearing mice. World Allergy Organ. J. 2019, 12, 100044. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gomez-Rubio, P.; Zock, J.P.; Rava, M.; Marquez, M.; Sharp, L.; Hidalgo, M.; Carrato, A.; Ilzarbe, L.; Michalski, C.; Molero, X.; et al. Reduced risk of pancreatic cancer associated with asthma and nasal allergies. Gut. 2017, 66, 314–322. [Google Scholar] [CrossRef] [PubMed]
- Kozłowska, R.; Bożek, A.; Jarząb, J. Association between cancer and allergies. Allergy Asthma Clin. Immunol. 2016, 12, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sherman, P.W.; Holland, E.; Sherman, J.S. Allergies: their role in cancer prevention. Q. Rev. Biol. 2008, 83, 339–362. [Google Scholar] [CrossRef] [PubMed]
- Coussens, L.M.; Werb, Z. Inflammation and cancer. Nature 2002, 420, 860–867. [Google Scholar] [CrossRef]
- Profet, M. The function of allergy: immunological defense against toxins. Q. Rev. Biol. 1991, 66, 23–62. [Google Scholar] [CrossRef] [PubMed]
- Qu, J.; Cheng, T.; Liu, L.; Heng, J.; Liu, X.; Un, Z.; Wang, W.; Li, K.; Yang, N. Mast cells induce epithelial –to—mesenchymal transition and migration in non-small cell lung cancer through Il-8/Wnt/β-catenin pathway. J. Cancer 2019, 10, 3830–3841. [Google Scholar] [CrossRef] [PubMed]
- Komi, D.E.A.; Redegeld, F.A. Role of mast cells in shaping the tumor microenvironment. Clin. Rev. Allergy Immunol. 2019, 58, 313–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zurawa-Janicka, D.; Wenta, T.; Jarząb, M.; Skorko-Glonek, J.; Glaza, P.; Gieldon, A.; Ciarkowski, J.; Lipinska, B. Structural insights into the activation mechanisms of human HtrA serine proteases. Arch. Biochem. Biophys. 2017, 621, 6–23. [Google Scholar] [CrossRef] [PubMed]
- Ngiow, S.F.; Teng, M.W.L.; Smyth, M.J. A balance of interleukin-12 and -23 in cancer. Trends Immunol. 2013, 34, 548–555. [Google Scholar] [CrossRef]
- Gilicze, A.; Kohalmi, B.; Pocza, P.; Keszei, M.; Jaeger, J.; Gorbe, E.; Papp, Z.; Toth, S.; Falus, A.; Wiener, Z. HtrA1 is a novel mast cell serine protease of mice and men. Mol. Immunol. 2007, 44, 2961–2968. [Google Scholar] [CrossRef] [PubMed]
- Chien, J.; He, X.; Shridhar, V. Identification of tubilins as substrates of serine protease trA1 by mixture-based oriented peptide library screening. J. Cell Biochem. 2009, 107, 253–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Z.; Li, H.; Derouet, M.; Berezkin, A.; Sasazuki, T.; Shirasawa, S.; Rosen, K. Oncogenic Ras inhibits anoikis of intestinal epithelial cells by preventing the release of a mitochondrial pro-apoptotic protein Omi/HtrA2 into the cytoplasm. J. Biol. Chem. 2006, 281, 14738–14747. [Google Scholar] [CrossRef] [Green Version]
- Skorko-Glonek, J.; Zurawa-Janicka, D.; Koper, T.; Figaj, D.; Glaza, P.; Lipinska, B. HtrA protease family as therapeutic targets. Curr. Pharm. Des. 2013, 19, 977–1009. [Google Scholar] [CrossRef]
- Kang, S.; Louboutin, J.P.; Datta, P.; Landel, C.P.; Martinez, D.; Zervos, A.S.; Strayer, D.S.; Fernandes-Alnemri, T.; Alnemri, E.S. Loss of HtrA2/Omi activity in non-neuronal tissues of adult mice causes premature aging. Cell Death Differ. 2013, 20, 259–269. [Google Scholar] [CrossRef]
- Tocharus, J.; Tsuchiya, A.; Kajikawa, M.; Ueta, Y.; Oka, C.; Kawaichi, M. Developmentally regulated expression of mouse HtrA3 and its role as an inhibitor of TGF-beta signaling. Dev. Growth Differ. 2004, 46, 257–274. [Google Scholar] [CrossRef] [PubMed]
- Singh, H.; Li, Y.; Fuller, P.J.; Harrison, C.; Rao, J.; Stephens, A.N.; Nie, G. HtrA3 is downregulated in cancer cell lines and significantly reduced in primary serous and granulosa cell ovarian tumors. J. Cancer 2013, 4, 152–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, J.; Feng, M.; Liu, D.; Liu, H.; Shi, M.; Zhang, J.; Qu, J. Antagonism between HTRA3 and TGFβ1 contributes to metastasis in non-small cell lung cancer. Cancer Res. 2019, 79, 2853–2864. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suzukawa, M.; Matsumoto, H.; Ohshima, N.; Tashimo, H.; Asari, I.; Tajiri, T.; Niimi, A.; Nagase, H.; Matsui, H.; Kobayashi, N.; et al. Baseline serum CXCL10 and Il-12 levels may predict severe asthmatics’ responsiveness to omalizumab. Respir. Med. 2018, 134, 95–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention. 2019. Available online: https://ginasthma.org/wp-content/uploads/2019/06/GINA-2019-main-report-June-2019-wms.pdf (accessed on 22 September 2019).
- Brozek, J.L.; Bousquet, J.; Agache, I.; Agarwal, A.; Bachert, C.; Bosnic-Anticevich, S.; Brignardello-Petersen, R.; Walter Canonica, G.; Casale, T.; Chavannes, N.H. Allergic Rhinitis and its Impact on Asthma (ARIA)guidelines—2016 revision. J. Allergy. Clin. Immunol. 2017, 140, 950–958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, M.R.; Crapo, R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Enright, P.; van der Grinten, C.P.M.; Gustafssonet, P.; et al. General consideration for lung function testing. Eur. Respir. J. 2005, 26, 153–161. [Google Scholar] [CrossRef] [Green Version]
- Laemmli, U.K. Cleavage of the structural protein during assembly of the head of bacteriophage T4. Nature 1970, 227, 680–685. [Google Scholar] [CrossRef]
- Wollweber, L. Antibodies: A Laboratory Manual; Harlow, E., Lane, D., Eds.; Cold Spring Harbor: New York, NY, USA, 1988; pp. 23–43. [Google Scholar]
- Renke, J.; Kędzierska-Mieszkowska, S.; Lange, M.; Nedoszytko, B.; Liberek, A.; Plata-Nazar, K.; Renke, M.; Wenta, T.; Żurawa-Janicka, D.; Skórko- Glonek, J.; et al. Immune response against HtrA proteases in children with cutaneous mastocytosis. Acta Biochim. Pol. 2018, 65, 471–478. [Google Scholar] [CrossRef]
- Matito, A.; Azana, J.M.; Torrelo, A.; Alvarez-Twose, I. Cutaneous mastocytosis in adults and children: new classification and prognostic factors. Immunol. Allergy Clin. North Am. 2018, 38, 351–363. [Google Scholar] [CrossRef]
- Derakhshani, A.; Vahidian, F.; Alihasanzadeh, M.; Mokhtarzadeh, A.; Nezhad, P.L.; Baradaran, B. Mast cells: a double-edged sword in cancer. Immunol. Lett. 2019, 209, 28–35. [Google Scholar] [CrossRef]
- Sammarco, G.; Varricchi, G.; Ferraro, V.; Ammendola, M.; De Fazio, M.; Altomare, D.F.; Luposella, M.; Maltese, L.; Curro, G.; Marone, G.; et al. Mast cells, angiogenesis and lymphangiogenesis in human gastric cancer. Int. J. Mol. Sci. 2019, 20, 2106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Broesby-Olsen, S.; Farkas, D.K.; Vestergaard Hermann, A.P.; Boe Moller, M.; Gotthard Mortz, C.; Kielsgaard Kristensen, T.; Bindslev-Jensen, C.; Toft Sorensen, H.; Frederiksen, H. Risk of solid cancer, cardiovascular disease, anaphylaxis, osteoporosis and fractures in patients with systemic mastocytosis: A nationwide population-based study. Am. J. Hematol. 2016, 91, 1069–1075. [Google Scholar] [CrossRef] [PubMed]
- Rigoni, A.; Colombo, M.P.; Pucillo, C. Mast cells, basophils and eosinophils: From allergy to cancer. Semin. Immunol. 2017, 35, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Saito, A.; Horie, M.; Nagase, T. TGF-β signaling in Lung Health and Disease. Int. J. Mol. Sci. 2018, 19, 2460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yao, Y.S.; Chang, W.W.; He, L.P.; Jin, Y.L.; Li, C.P. An updated meta-analysis of transforming growth factor - β1 gene: Three well-characterized polymorphisms with asthma. Hum. Immunol. 2016, 77, 1291–1299. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Li, J.; Wang, K.; Tan, Q.; Tan, W.; Guo, G. Association between TGF-β1 polymorphisms and asthma susceptibility among the Chinese: A meta-analysis. Genet. Test. Mol. Biomarkers 2018, 22, 433–442. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients with Allergy (n = 40) | Control Group (n = 39) | |
|---|---|---|
| Age (years) | ||
| range (median) | 6–18 (13.5) | 1–17 (9) |
| Gender F/M (n) | 18/22 | 21/18 |
| Diagnosis | ||
| Atopic Asthma (n) | 19 | - |
| Allergic Rhinitis (n) | 21 | - |
| Positive Skin Prick Test (n) | 40 | - |
| Spirometry pv (mean ± SD) | ||
| FEV1% (p < 0.001; T = − 7,5; df = 77) | 83.1 ± 13.8 | 101.7 ± 7.1 |
| FVC% (p < 0.001; T = − 3,5; df = 77) | 90.1 ± 13.4 | 100.1 ± 11.9 |
| FEV1/FVC (p < 0.001; T = − 6,41; df = 77) | 87.7 ± 10.5 | 101.3 ± 8.2 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Renke, J.; Wasilewska, E.; Kędzierska-Mieszkowska, S.; Zorena, K.; Barańska, S.; Wenta, T.; Liberek, A.; Siluk, D.; Żurawa-Janicka, D.; Szczepankiewicz, A.; et al. Tumor Suppressors—HTRA Proteases and Interleukin-12—in Pediatric Asthma and Allergic Rhinitis Patients. Medicina 2020, 56, 298. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56060298
Renke J, Wasilewska E, Kędzierska-Mieszkowska S, Zorena K, Barańska S, Wenta T, Liberek A, Siluk D, Żurawa-Janicka D, Szczepankiewicz A, et al. Tumor Suppressors—HTRA Proteases and Interleukin-12—in Pediatric Asthma and Allergic Rhinitis Patients. Medicina. 2020; 56(6):298. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56060298
Chicago/Turabian StyleRenke, Joanna, Eliza Wasilewska, Sabina Kędzierska-Mieszkowska, Katarzyna Zorena, Sylwia Barańska, Tomasz Wenta, Anna Liberek, Danuta Siluk, Dorota Żurawa-Janicka, Aleksandra Szczepankiewicz, and et al. 2020. "Tumor Suppressors—HTRA Proteases and Interleukin-12—in Pediatric Asthma and Allergic Rhinitis Patients" Medicina 56, no. 6: 298. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56060298