A Multistep Iter for Functional Reconstruction in Mangled Upper Limb: A Retrospective Analysis of Integrated Surgical and Medical Approach

 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Database
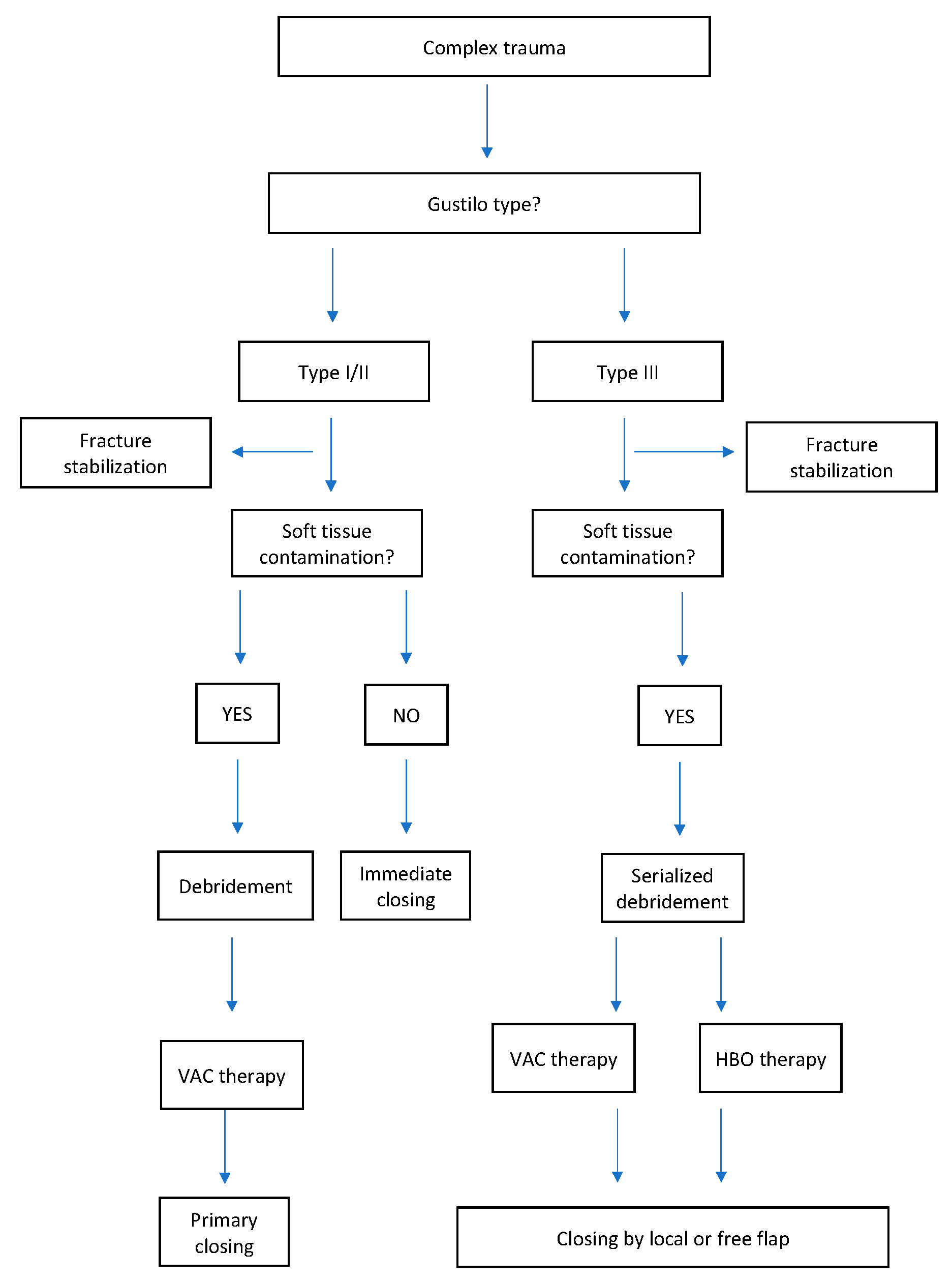
2.2. Treatment
3. Results
3.1. Case Study #1
3.2. Case Study #2
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gregory, R.T.; Gould, R.J.; Peclet, M.; Wagner, J.S.; Gilbert, D.A.; Wheeler, J.R.; Snyder, S.O.; Gayle, R.G.; Schwab, C.W. The mangled extremity syndrome (MES): A severity grading system for multisystem injury of the extremity. J. Trauma 1985, 3, 226–236. [Google Scholar]
- Guo, S.; DiPietro, L.A. Factors Affecting Wound Healing. J. Dent. Res. 2010, 89, 219–229. [Google Scholar] [CrossRef]
- Robson, M.C. Wound Infection. A failure of wound healing caused by an imbalance of bacteria. Surg. Clin. North Am. 1997, 77, 637–650. [Google Scholar] [CrossRef]
- Battiston, B.; Tos, P.; Pontini, I.; Ferrero, S. Lower limb replantations: Indications and a new scoring system. Microsurgery 2002, 22, 187–192. [Google Scholar] [CrossRef]
- Monticelli, A.; Ciclamini, D.; Boffano, M.; Boux, E.; Titolo, P.; Panero, B.; Battiston, B.; Piana, R.; Tos, P. Lower Limb Core Scale: A new application to evaluate and compare the outcomes of bone and soft-tissuetumours resection and reconstruction. Res. Int. 2014, 2014, 652141. [Google Scholar] [CrossRef]
- Helfet, D.L.; Howey, T.; Sanders, R.; Johansen, K. Limb salvage versus amputation. Preliminary results of the Mangled Extremity Severity Score. Clin. OrthopRelat Res. 1990, 250, 80–86. [Google Scholar]
- Loja, M.N.; Sammann, A.; DuBose, J.; Li, C.S.; Liu, Y.; Savage, S.; Scalea, T.; Holcomb, J.B.; Rasmussen, T.E.; Knudson, M.M.; et al. The mangled extremity score and amputazion: Time for revision. J. Trauma Acute Care Surg. 2017, 82, 518–523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horgan, O.; MacLachlan, M. Psychosocial adjustment to lower-limb amputation: A review. Disabil. Rehabil. 2004, 26, 837–850. [Google Scholar] [CrossRef] [PubMed]
- Kearns, N.T.; Jackson, W.T.; Elliott, T.R.; Ryan, T.; Armstrong, T.W. Differences in level of upper limb loss on functional impairment, psychological well-being, and substance use. Rehabil. Psychol. 2018, 63, 141–147. [Google Scholar] [CrossRef]
- Godina, M. Early microsurgical reconstruction of complex trauma of the extremities. Orthop. Trauma Dir. 1986, 78, 285–292. [Google Scholar] [CrossRef]
- Hertel, R.; Lambert, S.M.; Muller, S.; Ballmer, F.T.; Ganz, R. On the timing of soft-tissue reconstruction for oper fractures on the lower leg. Arch. Orthop. Trauma Surg. 1999, 119, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Karanas, Y.L.; Nigriny, J.; Chang, J. The timing of microsurgical reconstruction in lower extremity trauma. Microsurgery 2008, 28, 632–634. [Google Scholar] [CrossRef] [PubMed]
- McDonald, W.S.; Nichter, L.S. Debridement of bacterial and particulate-contaminated wounds. Ann. Plast. Surg. 1994, 33, 142–147. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, R.D.; Adams, B.D. The role of antibiotics in the management of elective and post-traumatic hand surgery. Hand Clin. 1998, 14, 657–666. [Google Scholar]
- Manna, B.; Morrison, C.A. Wound Debridement; StatPearls Publishing: St. Petersburg, FL, USA, 2018. [Google Scholar]
- Herscovici, D.; Sanders, R.W., Jr.; Scaduto, J.M.; Infante, A.; DiPasquale, T. Vacuum-assisted wound closure (VAC therapy) for the management of patients with high-energy soft tissue injuries. J. Orthop. Trauma 2003, 17, 683–688. [Google Scholar] [CrossRef]
- Memar, M.Y.; Yekani, M.; Alizadeh, N.; Baghi, H.B. Hyperbaric oxygen therapy: Antimicrobial mechanisms and clinical application for infections. Biomed. Pharmacother. 2019, 109, 440–447. [Google Scholar] [CrossRef]
- Torbrand, C.; Ugander, M.; Engblom, H.; Arheden, H.; Ingemansson, R.; Malmsjo, M. Wound contraction and macro-deformation during negative presure therapy of sternotomy wounds. J. Cardiothorac. Surg. 2010, 5, 75. [Google Scholar] [CrossRef] [Green Version]
- Krug, E.; Berg, L.; Lee, C.; Hudson, D.; Birke-Sorensen, H.; Depoorter, M.; Dunn, R.; Jeffery, S.; Duteille, F.; Bruhin, A.; et al. International Expert Panel on Negative Pressure Wound Therapy [NPWT-EP]. Evidence-based recommendations for the use of Negative Pressure Wound Therapy in traumatic wounds and reconstructive surgery: Steps towards an international consensus. Injury 2011, 42 (Suppl. 1), S1–S2. [Google Scholar] [CrossRef]
- Kanakaris, N.K.; Thanasas, C.; Keramaris, N.; Kontaris, G.; Granick, M.S.; Giannoudis, P.V. The efficacy of negative pressure wound therapy in the management of lower extremity trauma: Review of clinical evidence. Injury 2007, 38 (Suppl. 5), S9–S18. [Google Scholar] [CrossRef]
- Hammarlung, C. The physiologic effects of hyperbaric oxygen. In Hyperbaric Medicine Practice; Kindwall, E.P., Ed.; Best Publishing Company: North Palm Beach, FL, USA, 1995; pp. 17–32. [Google Scholar]
- Bird, A.D.; Telfer, H.B. Effect of hyperbaric oxygen on limb circulation. Lancet 1965, 13, 355–356. [Google Scholar] [CrossRef]
- Gustilo, R.B.; Anderson, J.T. Prevention of infection in the treatment of one thousand and twenty-five open fractures of long bones: Retrospective and prospective analyses. J. Bone Joint Surg. Am. 1976, 58, 453–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shawen, S.B.; Keeling, J.J.; Branstetter, J.; Kirk, K.L.; Ficke, J.R. The mangled foot and leg: Salvage versus amputation. Foot Ankle Clin. 2010, 15, 63–75. [Google Scholar] [CrossRef] [PubMed]
- Strauss, M.B. Crush injury and other acute traumatic peripheral ischemias. In Hyperbaric Medicine Practice; Kindwall, E.P., Ed.; Best Publishing Company: North Palm Beach, FL, USA, 1995; pp. 525–549. [Google Scholar]
- Panattoni, J.B.; Ahmed, M.M.; Busel, G.A. An ABC technical algorithm to treat the mangled upper extremity: Systematic surgical approach. J. Hand Surg. Am. 2017, 42, 934.e1–934.e10. [Google Scholar] [CrossRef] [PubMed]
- Howe, H.R., Jr.; Poole, G.V., Jr.; Hansen, K.J.; Clark, T.; Plonk, G.W.; Koman, L.A.; Pennell, T.C. Salvage of lower extremities following combined orthopaedic and vascular trauma: A predicitive salvage index. Am Surg. 1987, 53, 205–208. [Google Scholar]
- Hopf, H.W.; Humphrey, L.M.; Puzziferri, N.; West, J.M.; Attinger, C.E.; Hunt, T.K. Adjuncts to preparing wounds for closure: Hyperbaric oxygen, growth factors, skin substitutes, negative pressure wound therapy (vacuum- assisted closure). Foot Ankle Clin. 2001, 6, 661–682. [Google Scholar] [CrossRef]
- Saxena, V.; Hwang, C.W.; Huang, S.; Eichbaum, Q.; Ingber, D.; Orgill, D.P. Vacuum-assisted closure: Microdeformations of wounds and cell proliferation. Plast. Reconstr. Surg. 2004, 114, 1086–1096. [Google Scholar] [CrossRef]
- Schraibman, I.G.; Ledingham, I.M. Hyperbaric oxygen and local vasodilation in pheripheral vascular disease. Br. J. Surg. 1969, 56, 295–299. [Google Scholar] [CrossRef]
- Godman, C.A.; Chheda, K.P.; Hightower, L.E.; Perdrizet, G.; Shin, D.G.; Giardina, C. Hyperbaric oxygen induces a cytoprotective and angiogenic response in human microvascular endothelial cells. Cell Stress Chaperones. 2010, 15, 431–442. [Google Scholar] [CrossRef] [Green Version]
- Kaufman, H.; Gurevich, M.; Tamir, E.; Keren, E.; Alexander, L.; Hayes, P. Topical oxygen therapy stimulates healing in difficult, chronic wounds: A tertiary centre experience. J. Wound Care 2018, 27, 426–433. [Google Scholar] [CrossRef]
- Kranke, P.; Bennett, M.H.; Martyn-St James, M.; Schnabel, A.; Debus, S.E.; Weibel, S. Hyperbaric oxygen therapy for chronic wounds. Cochrane Database Syst. Rev. 2015, 6, CD004123. [Google Scholar] [CrossRef]
- Hunt, T.K.; Niinikoski, J.; Zderfeld, B.H.; Silver, I.A. Oxygen in wound healing enhancement: Cellular effects of oxygen. In Hyperbaric Oxygen Terapy; Davis, J.C., Hunt, T.K., Eds.; University Media Services (UMS): Bethesda, MD, USA, 1977; p. 112. [Google Scholar]
- Schirò, G.R.; Sessa, S.; Piccioli, A.; Maccauro, G. Primary amputation vs limb salvage in mangled extremity: A systematic review of the current scoring system. BMC Musculoskelet. Disord. 2015, 16, 372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrison, B.L.; Lakhiani, C.; Lee, M.R.; Saint-Cyr, M. Timing of traumatic upper extremity free flap reconstruction: A systematic review and progress report. Plast. Reconstr. Surg. 2013, 132, 591–598. [Google Scholar] [CrossRef] [PubMed]
- Kolbenschlag, J.; Klinkenberg, M.; Hellmich, S.; Germann, G.; Megerle, K. Impact of timing of admission and microvascular reconstruction on free flap success rates in traumatic upper extremity defects. J. Reconstr. Microsurg. 2015, 31, 414–419. [Google Scholar] [PubMed]
- Millar, I.L.; McGinnes, R.A.; Williamson, O.; Lind, F.; Jansson, K.A.; Hajek, M.; Smart, D.; Fernandes, T.; Miller, R.; Myles, P.; et al. Hyperbaric oxygen in lower limb trauma (HOLLT); protocol for a randomized controlled trial. BMJ Open 2015, 5, e008381. [Google Scholar] [CrossRef] [Green Version]
- Virani, S.R.; Dahapute, A.A.; Bava, S.S.; Muni, S.R. Impact of negative pressure wound therapy on open diaphyseal tibial fractures: A prospective randomized trial. J. Clin. Orthop. Trauma 2016, 7, 256–259. [Google Scholar] [CrossRef] [Green Version]
- Lee, Z.H.; Stranix, J.T.; Rifkin, W.J.; Daar, D.A.; Anzai, L.; Ceradini, D.J.; Thanik, V.T.; Saadeh, P.B.; Levine, J.P. Timing of microsurgical reconstruction in lower extremity trauma: An update of the Godina Paradigm. Plast. Reconstr. Surg. 2019, 144, 759–767. [Google Scholar] [CrossRef]
- Haykal, S.; Roy, M.; Patel, A. Meta-analysis of timing for microsurgical free-flap reconstruction for lower limb injury: Evaluation of the Godina Principles. J. Reconstr. Microsurg. 2018, 34, 277–292. [Google Scholar]
- Qiu, E.; Kurlander, D.E.; Ghaznavi, A.M. Godina revisited: A systematic review of traumatic lower extremity wound reconstruction timing. J. Plast. Surg. Hand Surg. 2018, 52, 259–264. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Patients | Percentage | |
|---|---|---|
| n (patients) | 179 | |
| Gender | ||
| Male | 129 | 72% |
| Female | 50 | 28% |
| Smokers | 20 | 11% |
| Medical disease | ||
| Hypertension | 8 | 4% |
| Diabetes mellitus | 14 | 8% |
| Immunosuppressed | 2 | 1% |
| Mechanism injury | ||
| Auto versus pedestrian | 7 | 4% |
| Motor vehicle accidents | 39 | 22% |
| Motorcycle collisions | 33 | 18% |
| Work crushing | 77 | 43% |
| Work blast | 5 | 3% |
| Gunshot wound | 8 | 5% |
| Animal attacks | 10 | 6% |
| Post traumatic loss injuries | ||
| Skin | 28 | 15% |
| Tendon and muscles | 76 | 43% |
| Bone | 75 | 42% |
| Associated injuries | ||
| Head injury | 5 | 3% |
| Clavicle fracture | 3 | 2% |
| Lung insult and Rib fracture | 5 | 3% |
| Lower limb fracture | 20 | 11% |
| Number of Patients | Percentage | |
|---|---|---|
| n (patients) | 179 | |
| Skin loss | 28 | 15% |
| Soft tissue loss only | 76 | 43% |
| Bone fractures | 75 | 42% |
| Debridement | 179 | 100% |
| Microorganism infection (%) | ||
| Staphylococcus aureus | 63% | |
| Staphylococcus aureus MRSA | 23% | |
| Pseudomonas Aeruginosas | 7% | |
| Acinetobacter baumanii | 4% | |
| Others | 3% | |
| Systemic antibiotics | 179 | 100% |
| Fracture severity | ||
| Gustilo II | 32 | 42% |
| Gustilo III | 43 | 58% |
| Location of fracture | ||
| Medical Support Methods (%) | ||
| NPT | 32 | 42% |
| NPT + HBOT | 43 | 58% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Francesco, F.; Marchesini, A.; Campodonico, A.; Neuendorf, A.D.; Pangrazi, P.P.; Riccio, M. A Multistep Iter for Functional Reconstruction in Mangled Upper Limb: A Retrospective Analysis of Integrated Surgical and Medical Approach. Medicina 2020, 56, 398. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56080398
De Francesco F, Marchesini A, Campodonico A, Neuendorf AD, Pangrazi PP, Riccio M. A Multistep Iter for Functional Reconstruction in Mangled Upper Limb: A Retrospective Analysis of Integrated Surgical and Medical Approach. Medicina. 2020; 56(8):398. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56080398
Chicago/Turabian StyleDe Francesco, Francesco, Andrea Marchesini, Andrea Campodonico, Alexander Dietrich Neuendorf, Pier Paolo Pangrazi, and Michele Riccio. 2020. "A Multistep Iter for Functional Reconstruction in Mangled Upper Limb: A Retrospective Analysis of Integrated Surgical and Medical Approach" Medicina 56, no. 8: 398. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56080398