
A Higher Polygenic Risk Score Is Associated with a Higher Recurrence Rate of Atrial Fibrillation in Direct Current Cardioversion-Treated Patients

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Group
2.2. Genetic Analysis
2.3. Statistical Analysis
3. Results
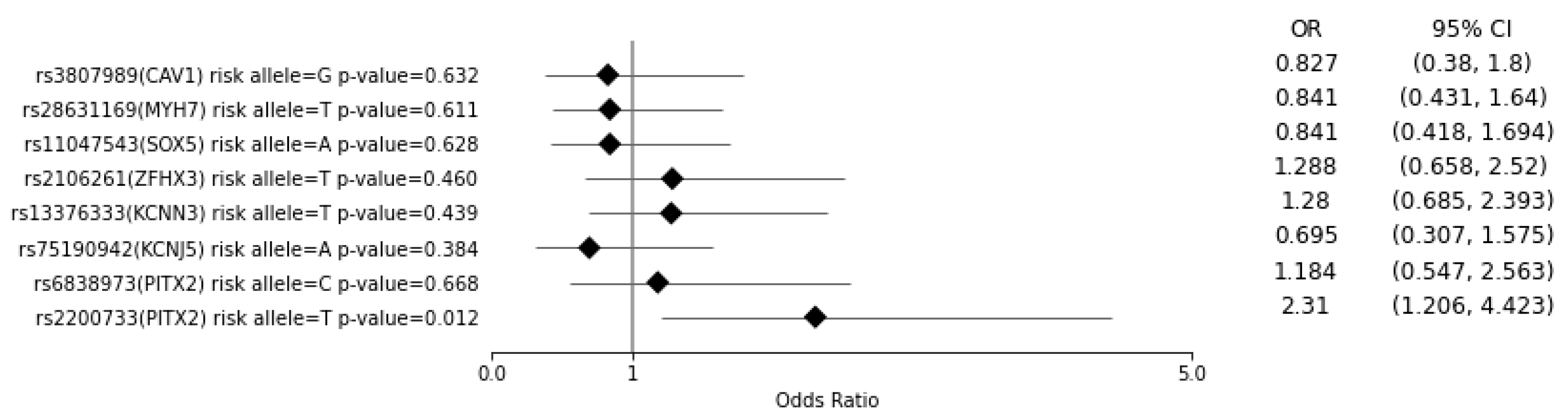
3.1. Multiple Regression Analysis of the Case and Control Groups Regarding the Risk of Developing AF for Each SNV and for a PRS of >7
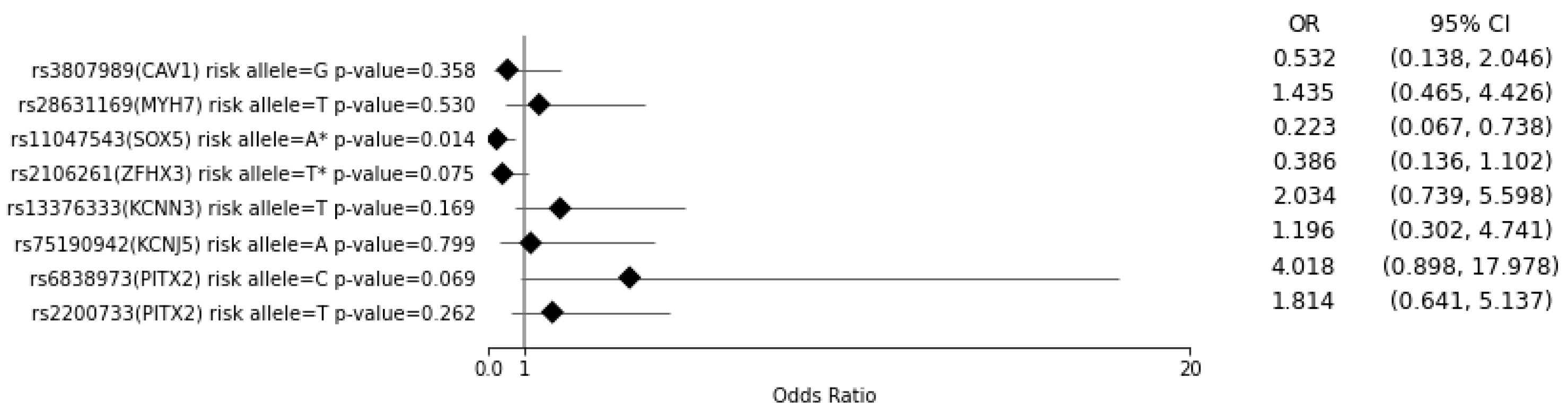
3.2. Multiple Regression Analysis of AF Patients with Known DCC Outcomes for the Risk of AF Recurrence for Each SNV and for a PRS of >7
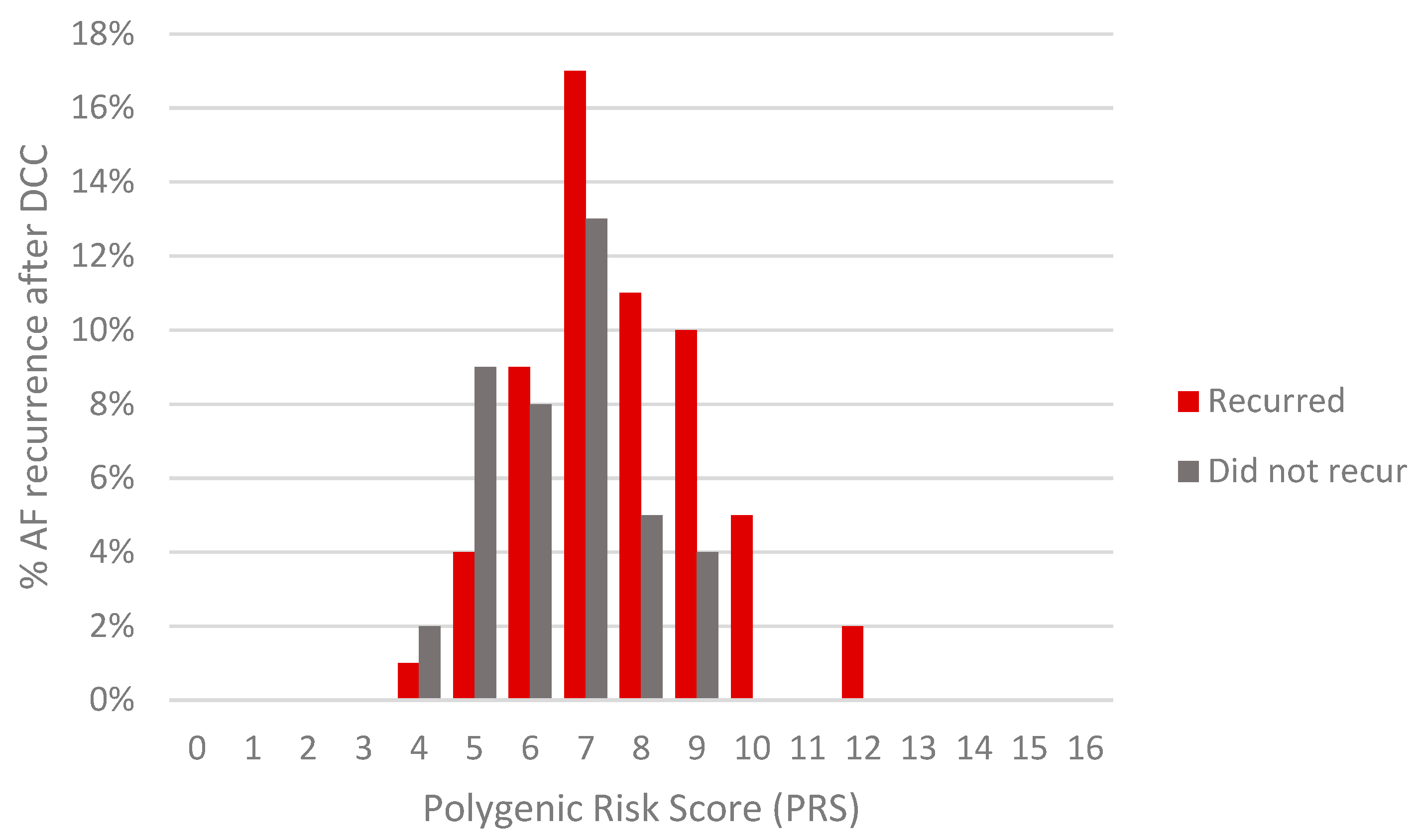
3.3. Multiple Regression Analysis of AF Patients with Known DCC Outcomes and Transthoracic Echocardiography Data (n = 50) for the Risk of AF Recurrence for a PRS of >7
4. Discussion
4.1. Discussion of Results
4.2. Limitations
4.3. Broad View
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Garrey, W.E. Auricular Fibrillation. Physiol. Rev. 1924, 4, 215–250. [Google Scholar] [CrossRef]
- Ganesan, A.N.; Chew, D.P.; Hartshorne, T.; Selvanayagam, J.B.; Aylward, P.E.; Sanders, P.; McGavigan, A.D. The impact of atrial fibrillation type on the risk of thromboembolism, mortality, and bleeding: A systematic review and meta-analysis. Eur. Heart J. 2016, 37, 1591–1602. [Google Scholar] [CrossRef]
- Ellinor, P.T.; Lunetta, K.L.; Albert, C.M.; Glazer, N.L.; Ritchie, M.D.; Smith, A.V.; Arking, D.E.; Müller-Nurasyid, M.; Krijthe, B.P.; Lubitz, S.A.; et al. Meta-analysis identifies six new susceptibility loci for atrial fibrillation. Nat. Genet. 2012, 44, 670–675. [Google Scholar] [CrossRef] [Green Version]
- Pfeufer, A.; Van Noord, C.; Marciante, K.D.; Arking, D.E.; Larson, M.G.; Smith, A.V.; Tarasov, K.V.; Müller, M.; Sotoodehnia, N.; Sinner, M.F.; et al. Genome-wide association study of PR interval. Nat. Genet. 2010, 42, 153–159. [Google Scholar] [CrossRef]
- Roselli, C.; Chaffin, M.D.; Weng, L.-C.; Aeschbacher, S.; Ahlberg, G.; Albert, C.M.; Almgren, P.; Alonso, A.; Anderson, C.D.; Aragam, K.G.; et al. Multi-ethnic genome-wide association study for atrial fibrillation. Nat. Genet. 2018, 50, 1225–1233. [Google Scholar] [CrossRef]
- Thorolfsdottir, R.B.; Sveinbjornsson, G.; Sulem, P.; Helgadottir, A.; Gretarsdottir, S.; Benonisdottir, S.; Magnusdottir, A.; Davidsson, O.B.; Rajamani, S.; Roden, D.M.; et al. A Missense Variant in PLEC Increases Risk of Atrial Fibrillation. J. Am. Coll. Cardiol. 2017, 70, 2157–2168. [Google Scholar] [CrossRef]
- Christophersen, I.E.; Rienstra, M.; Roselli, C.; Yin, X.; Geelhoed, B.; Barnard, J.; Lin, H.; Arking, D.E.; Smith, A.V.; Albert, C.M.; et al. Large-scale analyses of common and rare variants identify 12 new loci associated with atrial fibrillation. Nat. Genet. 2017, 49, 946–952. [Google Scholar] [CrossRef] [Green Version]
- Gudbjartsson, D.F.; Arnar, D.O.; Helgadottir, A.; Gretarsdottir, S.; Holm, H.; Sigurdsson, A.; Jonasdottir, A.; Baker, A.; Thorleifsson, G.; Kristjansson, K.; et al. Variants conferring risk of atrial fibrillation on chromosome 4q25. Nature 2007, 448, 353–357. [Google Scholar] [CrossRef]
- Rudaka, I.; Rots, D.; Uzars, A.; Kalçjs, O.; Gailîte, L. Association between 4q25 variants, risk of atrial fibrillation and echocardiographic parameters. Proc. Latv. Acad. Sci. Sect. B Nat. Exact. Appl. Sci. 2020, 74, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Kiliszek, M.; Franaszczyk, M.; Kozluk, E.; Lodzinski, P.; Piatkowska, A.; Broda, G.; Ploski, R.; Opolski, G. Association between variants on Chromosome 4q25, 16q22 and 1q21 and Atrial fibrillation in the polish population. PLoS ONE 2011, 6, e21790. [Google Scholar] [CrossRef] [Green Version]
- Parvez, B.; Vaglio, J.; Rowan, S.; Muhammad, R.; Kucera, G.; Stubblefield, T.; Carter, S.; Roden, D.; Darbar, D. Symptomatic Response to Antiarrhythmic Drug Therapy Is Modulated by a Common Single Nucleotide Polymorphism in Atrial Fibrillation. J. Am. Coll. Cardiol. 2012, 60, 539–545. [Google Scholar] [CrossRef] [Green Version]
- Parvez, B.; Shoemaker, M.B.; Muhammad, R.; Richardson, R.; Jiang, L.; Blair, M.A.; Roden, D.M.; Darbar, D. Common genetic polymorphism at 4q25 locus predicts atrial fibrillation recurrence after successful cardioversion. Hear. Rhythm. 2013, 10, 849–855. [Google Scholar] [CrossRef] [Green Version]
- Choe, W.S.; Kang, J.H.; Choi, E.K.; Shin, S.Y.; Lubitz, S.A.; Ellinor, P.T.; Oh, S.; Lim, H.E. A genetic risk score for atrial fibrillation predicts the response to catheter ablation. Korean Circ. J. 2019, 49, 338–349. [Google Scholar] [CrossRef]
- Abushouk, A.I.; Ali, A.A.; Mohamed, A.A.; El-Sherif, L.; Abdelsamed, M.; Kamal, M.; Sayed, M.K.; Mohamed, N.A.; Osman, A.A.; Shaheen, S.M.; et al. Rhythm versus rate control for atrial fibrillation: A meta-analysis of randomized controlled trials. Biomed. Pharmacol. J. 2018, 11, 609–620. [Google Scholar] [CrossRef]
- Klein, A.L.; Grimm, R.A.; Jasper, S.E.; Murray, R.D.; Apperson-Hansen, C.; Lieber, E.A.; Black, I.W.; Davidoff, R.; Erbel, R.; Halperin, J.L.; et al. Efficacy of transesophageal echocardiography-guided cardioversion of patients with atrial fibrillation at 6 months: A randomized controlled trial. Am. Heart J. 2006, 151, 380–389. [Google Scholar] [CrossRef]
- Ellinor, P.T.; Lunetta, K.L.; Glazer, N.L.; Pfeufer, A.; Alonso, A.; Chung, M.K.; Sinner, M.F.; de Bakker, P.I.W.; Mueller, M.; Lubitz, S.A.; et al. Common variants in KCNN3 are associated with lone atrial fibrillation. Nat. Genet. 2010, 42, 240–244. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, E.J.; Levy, D.; Vaziri, S.M.; D’agostino, R.B.; Belanger, A.J.; Wolf, P.A. Independent Risk Factors for Atrial Fibrillation in a Population-Based Cohort: The Framingham Heart Study. JAMA J. Am. Med. Assoc. 1994, 271, 840–844. [Google Scholar] [CrossRef]
- Kamel, H.; Okin, P.M.; Elkind, M.S.V.; Iadecola, C. Atrial Fibrillation and Mechanisms of Stroke: Time for a New Model. Stroke 2016, 47, 895–900. [Google Scholar] [CrossRef] [Green Version]
- Wanamaker, B.; Cascino, T.; McLaughlin, V.; Oral, H.; Latchamsetty, R.; Siontis, K.C. Atrial arrhythmias in pulmonary hypertension: Pathogenesis, prognosis and management. Arrhythm. Electrophysiol. Rev. 2018, 7, 43–48. [Google Scholar] [CrossRef]
- Alonso, A.; Yin, X.; Roetker, N.S.; Magnani, J.W.; Kronmal, R.A.; Ellinor, P.T.; Chen, L.Y.; Lubitz, S.A.; McClelland, R.L.; McManus, D.D.; et al. Blood lipids and the incidence of atrial fibrillation: The multi-ethnic study of atherosclerosis and the framingham heart study. J. Am. Heart Assoc. 2014, 3, e001211. [Google Scholar] [CrossRef] [Green Version]
- Michniewicz, E.; Mlodawska, E.; Lopatowska, P.; Tomaszuk-Kazberuk, A.; Malyszko, J. Patients with atrial fibrillation and coronary artery disease–Double trouble. Adv. Med. Sci. 2018, 63, 30–35. [Google Scholar] [CrossRef]
- Cepelis, A.; Brumpton, B.M.; Malmo, V.; Laugsand, L.E.; Loennechen, J.P.; Ellekjær, H.; Langhammer, A.; Janszky, I.; Strand, L.B. Associations of asthma and asthma control with atrial fibrillation risk results from the nord-trøndelag health study (HUNT). JAMA Cardiol. 2018, 3, 721–728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matarese, A.; Sardu, C.; Shu, J.; Santulli, G. Why is chronic obstructive pulmonary disease linked to atrial fibrillation? A systematic overview of the underlying mechanisms. Int. J. Cardiol. 2019, 276, 149–151. [Google Scholar] [CrossRef] [PubMed]
- Vittinghoff, E.; McCulloch, C.E. Relaxing the rule of ten events per variable in logistic and cox regression. Am. J. Epidemiol. 2007, 165, 710–718. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; Qian, F.; Zheng, Y.; Ogundiran, T.; Ojengbede, O.; Zheng, W.; Blot, W.; Nathanson, K.L.; Hennis, A.; Nemesure, B.; et al. Genetic variants demonstrating flip-flop phenomenon and breast cancer risk prediction among women of African ancestry. Breast Cancer Res. Treat. 2018, 168, 703–712. [Google Scholar] [CrossRef]
- Lin, P.-I.; Vance, J.M.; Pericak-Vance, M.A.; Martin, E.R. No Gene Is an Island: The Flip-Flop Phenomenon. Am. J. Hum. Genet. 2007, 80, 531–538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, J.J.; Kim, E.; Woo, E.; Song, S.H.; Kim, J.K.; Lee, H.; Lee, S.; Hong, S.K.; Byun, S.S. Evaluation of Polygenic Risk Scores for Prediction of Prostate Cancer in Korean Men. Front. Oncol. 2020, 10, 583625. [Google Scholar] [CrossRef]
- Lei, X.; Huang, S. Enrichment of minor allele of SNPs and genetic prediction of type 2 diabetes risk in British population. PLoS ONE 2017, 12, e0187644. [Google Scholar] [CrossRef] [PubMed]
- Ferrán, A.; Alegret, J.M.; Subirana, I.; Aragonès, G.; Lluis-Ganella, C.; Romero-Menor, C.; Planas, F.; Joven, J.; Elosua, R. Association Between rs2200733 and rs7193343 Genetic Variants and Atrial Fibrillation in a Spanish Population, and Meta-analysis of Previous Studies. Rev. Esp. Cardiol. 2014, 67, 822–829. [Google Scholar] [CrossRef] [PubMed]
- Shoemaker, M.B.; Bollmann, A.; Lubitz, S.A.; Ueberham, L.; Saini, H.; Montgomery, J.; Edwards, T.; Yoneda, Z.; Sinner, M.F.; Arya, A.; et al. Common Genetic Variants and Response to Atrial Fibrillation Ablation. Circ. Arrhythm. Electrophysiol. 2015, 8, 296–302. [Google Scholar] [CrossRef] [Green Version]
- Feghaly, J.; Zakka, P.; London, B.; Macrae, C.A.; Refaat, M.M. Genetics of atrial fibrillation. J. Am. Heart Assoc. 2018, 7, 9884. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daubert, J.P.; Pitt, G.S. Can Polymorphisms Predict Response to Antiarrhythmic Drugs in Atrial Fibrillation? J. Am. Coll. Cardiol. 2012, 60, 546–547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Husser, D.; Adams, V.; Piorkowski, C.; Hindricks, G.; Bollmann, A. Chromosome 4q25 Variants and Atrial Fibrillation Recurrence After Catheter Ablation. J. Am. Coll. Cardiol. 2010, 55, 747–753. [Google Scholar] [CrossRef] [Green Version]
- Szirák, K.; Soltész, B.; Hajas, O.; Urbancsek, R.; Nagy-Baló, E.; Penyige, A.; Csanádi, Z.; Nagy, B. PITX2 and NEURL1 SNP polymorphisms in Hungarian atrial fibrillation patients determined by quantitative real-time PCR and melting curve analysis. J. Biotechnol. 2019, 299, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.; Darbar, D. Genetic heterogeneity of atrial fibrillation susceptibility loci across racial or ethnic groups. Eur. Heart J. 2017, 38, 2595–2598. [Google Scholar] [CrossRef] [Green Version]
- Nelis, M.; Esko, T.; Mägi, R.; Zimprich, F.; Toncheva, D.; Karachanak, S.; Piskáčková, T.; Balaščák, I.; Peltonen, L.; Jakkula, E.; et al. Genetic structure of europeans: A view from the north-east. PLoS ONE 2009, 4, 5472. [Google Scholar] [CrossRef] [Green Version]
- Choi, S.W.; Mak, T.S.H.; O’Reilly, P.F. Tutorial: A guide to performing polygenic risk score analyses. Nat. Protoc. 2020, 15, 2759–2772. [Google Scholar] [CrossRef]
- O’Sullivan, J.W.; Shcherbina, A.; Justesen, J.M.; Turakhia, M.; Perez, M.; Wand, H.; Tcheandjieu, C.; Clarke, S.L.; Rivas, M.A.; Ashley, E.A. Combining Clinical and Polygenic Risk Improves Stroke Prediction among Individuals with Atrial Fibrillation. Circ. Genom. Precis. Med. 2021, 339–347. [Google Scholar] [CrossRef]
- Pulit, S.L.; Weng, L.C.; McArdle, P.F.; Trinquart, L.; Choi, S.H.; Mitchell, B.D.; Rosand, J.; De Bakker, P.I.W.; Benjamin, E.J.; Ellinor, P.T.; et al. Atrial fibrillation genetic risk differentiates cardioembolic stroke from other stroke subtypes. Neurol. Genet. 2018, 4, e293. [Google Scholar] [CrossRef] [Green Version]
- Kertai, M.D.; Mosley, J.D.; He, J.; Ramakrishnan, A.; Abdelmalak, M.J.; Hong, Y.; Shoemaker, M.B.; Roden, D.M.; Bastarache, L. Predictive Accuracy of a Polygenic Risk Score for Postoperative Atrial Fibrillation After Cardiac Surgery. Circ. Genom. Precis. Med. 2021, 14, 3269. [Google Scholar] [CrossRef]
- Gladding, P.A.; Legget, M.; Fatkin, D.; Larsen, P.; Doughty, R. Polygenic Risk Scores in Coronary Artery Disease and Atrial Fibrillation. Heart Lung Circ. 2020, 29, 634–640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shoemaker, M.B.; Shah, R.L.; Roden, D.M.; Perez, M.V. How Will Genetics Inform the Clinical Care of Atrial Fibrillation? Circ. Res. 2020, 127, 111–127. [Google Scholar] [CrossRef] [PubMed]
- Andersen, J.H.; Andreasen, L.; Olesen, M.S. Atrial fibrillation—A complex polygenetic disease. Eur. J. Hum. Genet. 2020, 29, 1051–1060. [Google Scholar] [CrossRef]
- Von Ende, A.; Casadei, B.; Hopewell, J. Improving prediction of atrial fibrillation: The impact of polygenic risk scores over conventional risk factors amongst 270,000 individuals in UK Biobank. Eur. Heart J. 2020, 41, 491. [Google Scholar] [CrossRef]
- Börschel, C.S.; Ohlrogge, A.H.; Geelhoed, B.; Niiranen, T.; Havulinna, A.S.; Palosaari, T.; Jousilahti, P.; Rienstra, M.; Van Der Harst, P.; Blankenberg, S.; et al. Risk prediction of atrial fibrillation in the community combining biomarkers and genetics. Europace 2021, 23, 674–681. [Google Scholar] [CrossRef]
- Purcell, S.M.; Wray, N.R.; Stone, J.L.; Visscher, P.M.; O’Donovan, M.C.; Sullivan, P.F.; Ruderfer, D.M.; McQuillin, A.; Morris, D.W.; Oĝdushlaine, C.T.; et al. Common polygenic variation contributes to risk of schizophrenia and bipolar disorder. Nature 2009, 460, 748–752. [Google Scholar] [CrossRef]
- Agerbo, E.; Sullivan, P.F.; Vilhjálmsson, B.J.; Pedersen, C.B.; Mors, O.; Børglum, A.D.; Hougaard, D.M.; Hollegaard, M.V.; Meier, S.; Mattheisen, M.; et al. Polygenic risk score, parental socioeconomic status, family history of psychiatric disorders, and the risk for schizophrenia: A Danish population-based study and meta-analysis. JAMA Psychiatry 2015, 72, 635–641. [Google Scholar] [CrossRef]
- Mavaddat, N.; Michailidou, K.; Dennis, J.; Lush, M.; Fachal, L.; Lee, A.; Tyrer, J.P.; Chen, T.H.; Wang, Q.; Bolla, M.K.; et al. Polygenic Risk Scores for Prediction of Breast Cancer and Breast Cancer Subtypes. Am. J. Hum. Genet. 2019, 104, 21–34. [Google Scholar] [CrossRef] [Green Version]
- Choi, S.H.; Jurgens, S.J.; Weng, L.C.; Pirruccello, J.P.; Roselli, C.; Chaffin, M.; Lee, C.J.Y.; Hall, A.W.; Khera, A.V.; Lunetta, K.L.; et al. Monogenic and polygenic contributions to atrial fibrillation risk results from a national biobank. Circ. Res. 2020, 126, 200–209. [Google Scholar] [CrossRef]
- Turner, J.L.; Lyons, A.; Shah, R.U.; Zenger, B.; Hess, R.; Steinberg, B.A. Accuracy of Patient Identification of Electrocardiogram-Verified Atrial Arrhythmias. JAMA Netw. Open 2020, 3, 3–6. [Google Scholar] [CrossRef]
- Rienstra, M.; Lubitz, S.A.; Mahida, S.; Magnani, J.W.; Fontes, J.D.; Sinner, M.F.; Van Gelder, I.C.; Ellinor, P.T.; Benjamin, E.J. Symptoms and Functional Status of Patients With Atrial Fibrillation. Circulation 2012, 125, 2933–2943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barsky, A.J.; Cleary, P.D.; Barnett, M.C.; Christiansen, C.L.; Ruskin, J.N. The accuracy of symptom reporting by patients complaining of palpitations. Am. J. Med. 1994, 97, 214–221. [Google Scholar] [CrossRef]
- Roselli, C.; Roselli, C.; Rienstra, M.; Ellinor, P.T.; Ellinor, P.T. Genetics of Atrial Fibrillation in 2020: GWAS, Genome Sequencing, Polygenic Risk, and beyond. Circ. Res. 2020, 127, 21–33. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Gene | Locus | SNV | Risk Allele | MAF | Location | GWAS Reporting an AF Link |
|---|---|---|---|---|---|---|
| CAV1 | 7q31 | rs3807989 | G | 0.61 | Intron | Ellinor et al., 2012 [3] |
| SOX5 | 12p12 | rs11047543 | A | 0.10 | Upstream | Pfeufer et al., 2010 [4] |
| MYH7 | 14q11 | rs28631169 | T | 0.12 | Intron | Roselli et al., 2018 [5] |
| ZFHX3 | 16q22 | rs2106261 | T | 0.24 | Intron | Ellinor et al., 2012 [3] |
| KCNN3 | 1q21 | rs13376333 | T | 0.27 | Intron | Ellinor et al., 2010 [16] |
| KCNJ5 | 11q24 | rs75190942 | A | 0.09 | Downstream | Christophersen et al., 2017 [7] |
| PITX2 | 4q25 | rs2200733 | T | 0.15 | Upstream | Gudbjartsson et al., 2007 [8] |
| PITX2 | 4q25 | rs6838973 | C | 0.43 | Upstream | Other studies: Rudaka et al., 2020, Kiliszek et al., 2011 [9,10] |
| Variable | Cases (n = 259) | Controls (n = 108) | p Value 1 | OR 2 | 95% Confidence Interval |
|---|---|---|---|---|---|
Sex
| 99 (38.2) 160 (61.8) | 39 (36.1) 69 (63.9) | <0.001 | 0.350 | 0.219–0.557 |
| Age 3, years | 64.5 ± 9.77 | 61.4 ± 9.92 | 0.007 | 1.032 | 1.009–1.056 |
| Body Mass Index 3, kg/m2 | 31.3 ± 5.41 | 29.5 ± 5.44 | 0.005 | 1.066 | 1.019–1.116 |
| Pulmonary Arterial Hypertension, n (%) | 201 (77.6) | 80 (74.1) | 0.467 | 1.213 | 0.721–2.040 |
| Congestive Heart Failure, n (%) | 161 (62.2) | 14 (13.0) | <0.001 | 11.031 | 5.963–20.404 |
| Coronary Heart Disease, n (%) | 50 (19.3) | 3 (2.8) | <0.001 | 8.373 | 2.551–27.479 |
| Stroke, n (%) | 11 (4.2) | 8 (7.4) | 0.213 | 0.554 | 0.217–1.419 |
| Diabetes (Type 1 and 2), n (%) | 24 (9.3) | 20 (18.5) | 0.013 | 0.449 | 0.236–0.854 |
| Dyslipidemia, n (%) | 86 (33.2) | 64 (59.3) | <0.001 | 0.342 | 0.215–0.543 |
| Chronic Respiratory Disorders, n (%) | 17 (6.6) | 5 (4.6) | 0.477 | 1.447 | 0.520–4.027 |
| Variable 1 | AF Recurred (n = 58) | AF Did Not Recur (n = 39) | p Value 2 | OR 3 | 95% Confidence Interval |
|---|---|---|---|---|---|
Sex
| 35 (60.3) 23 (39.7) | 31 (79.5) 8 (20.5) | 0.047 | 2.546 | 0.996–6.509 |
| Age 4, years | 61.7 ± 10.1 | 62.1 ± 10.4 | 0.882 | 0.997 | 0.958–1.038 |
| Body Mass Index 4, kg/m2 | 31.5 ± 5.66 | 31.6 ± 5.77 | 0.954 | 0.998 | 0.929–1.072 |
| Duration Since Initial Diagnosis 4, months | 58.6 ± 95.8 | 27.9 ± 43.2 | 0.059 | 1.010 | 1.000–1.021 |
| Age At Initial Diagnosis 4, years | 56.9 ± 12.6 | 59.8 ± 10.4 | 0.247 | 0.979 | 0.945–1.015 |
| Pulmonary Arterial Hypertension, n (%) | 43 (74.1) | 27 (69.2) | 0.597 | 1.274 | 0.519–3.130 |
| Congestive Heart Failure, n (%) | 38 (65.5) | 26 (66.7) | 0.768 | 0.877 | 0.367–2.098 |
| Coronary Heart Disease, n (%) | 7 (12.1) | 7 (17.9) | 0.419 | 0.627 | 0.201–1.956 |
| Stroke, n (%) | 3 (5.2) | 2 (5.1) | 0.992 | 1.009 | 0.161–6.335 |
| Diabetes (Type 1 and 2), n (%) | 4 (6.9) | 7 (17.9) | 0.339 | 0.092 | 0.092–1.247 |
| Dyslipidemia, n (%) | 21 (36.2) | 16 (41.0) | 0.632 | 0.816 | 0.355–1.877 |
| Chronic Respiratory Disorders, n (%) | 3 (5.2) | 4 (10.3) | 0.343 | 0.477 | 0.101–2.262 |
| CHA2DS2–VASc, n (%) | 50 (86.2) | 37 (94.9) | 0.169 | 0.338 | 0.068–1.685 |
| Non-CHA2DS2–VASc Comorbidities, n (%) | 47 (81.0) | 36 (92.3) | 0.121 | 0.356 | 0.092–1.371 |
| Variable 1 | AF Recurred (n = 35) | AF Did Not Recur (n = 15) | p Value | OR 2 | 95% Confidence Interval |
|---|---|---|---|---|---|
Sex
| 14 (40.0) 21 (60.0) | 2 (13.3) 13 (86.7) | 0.064 | 4.333 | 0.845–22.230 |
| Comorbidities, n (%) | 30 (85.7) | 15 (100) | 0.123 | 1.500 | 1.220–1.844 |
| Body Mass Index 3, kg/m2 | 32.5 ± 5.95 | 33.8 ± 6.35 | 0.484 | 0.965 | 0.872–1.067 |
| Duration Since Initial Diagnosis 3, months | 58.3 ± 112 | 31.6 ± 60.0 | 0.425 | 1.005 | 0.993–1.018 |
| Age At Initial Diagnosis 3, years | 56.1 ± 12.9 | 61.2 ± 12.9 | 0.206 | 0.967 | 0.919–1.019 |
| Left Atrial Volume Index 3, mL/m2 | 41.6 ± 11.8 | 40.8 ± 8.44 | 0.818 | 1.007 | 0.950–1.066 |
| Ejection Fraction 3, % | 54.1 ± 11.7 | 53.9 ± 8.45 | 0.956 | 1.002 | 0.946–1.060 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vogel, S.; Rudaka, I.; Rots, D.; Isakova, J.; Kalējs, O.; Vīksne, K.; Gailīte, L. A Higher Polygenic Risk Score Is Associated with a Higher Recurrence Rate of Atrial Fibrillation in Direct Current Cardioversion-Treated Patients. Medicina 2021, 57, 1263. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57111263
Vogel S, Rudaka I, Rots D, Isakova J, Kalējs O, Vīksne K, Gailīte L. A Higher Polygenic Risk Score Is Associated with a Higher Recurrence Rate of Atrial Fibrillation in Direct Current Cardioversion-Treated Patients. Medicina. 2021; 57(11):1263. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57111263
Chicago/Turabian StyleVogel, Simon, Irina Rudaka, Dmitrijs Rots, Jekaterīna Isakova, Oskars Kalējs, Kristīne Vīksne, and Linda Gailīte. 2021. "A Higher Polygenic Risk Score Is Associated with a Higher Recurrence Rate of Atrial Fibrillation in Direct Current Cardioversion-Treated Patients" Medicina 57, no. 11: 1263. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57111263