
Genetic Pattern, Orthodontic and Surgical Management of Multiple Supplementary Impacted Teeth in a Rare, Cleidocranial Dysplasia Patient: A Case Report

 ,
,  ,
,  , , ,
, , ,  , , , ,
, , , ,  , , ,
, , ,  ,
,  , , and add
Show full author list
, , and add
Show full author list
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Clinical Report
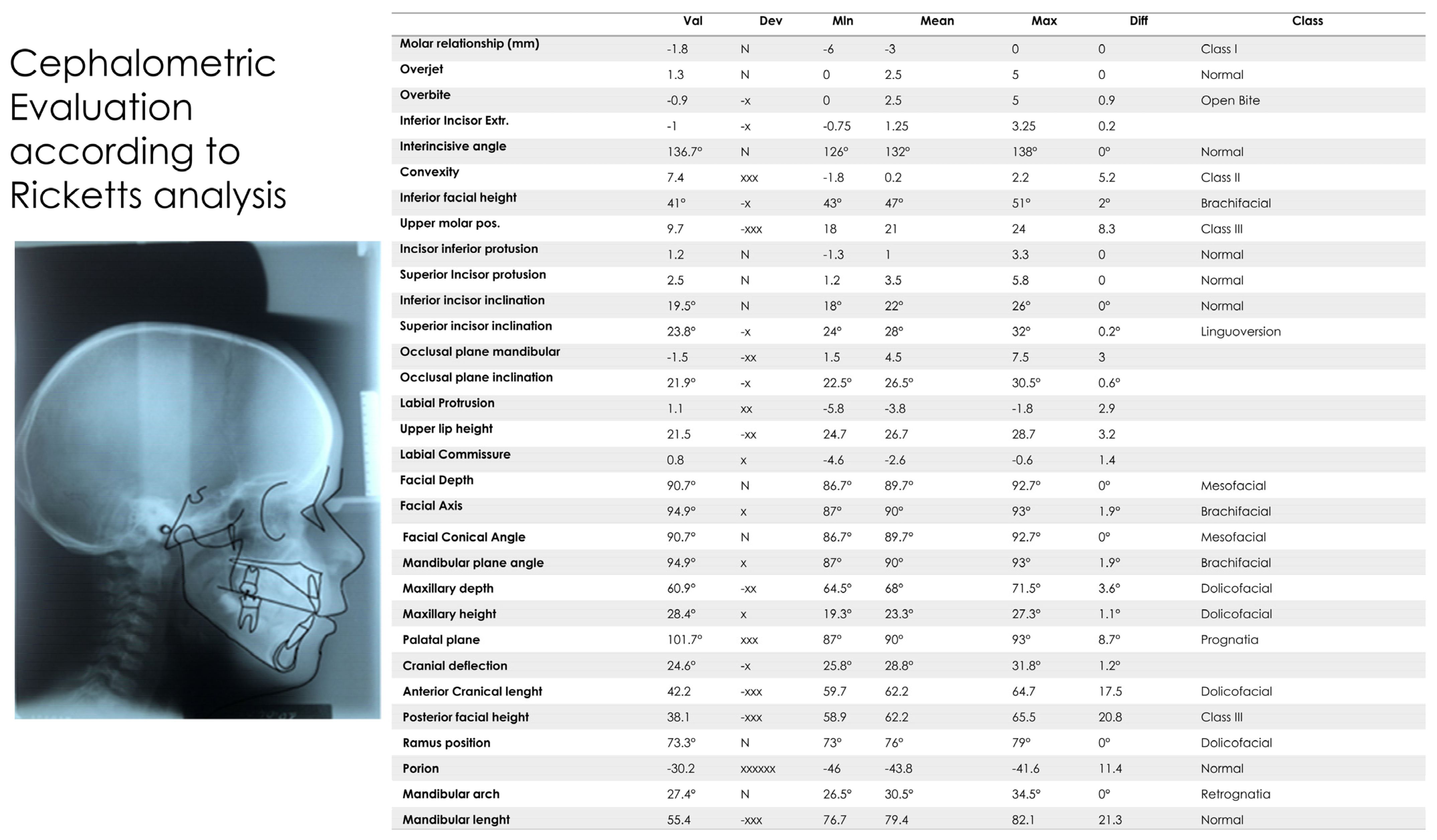
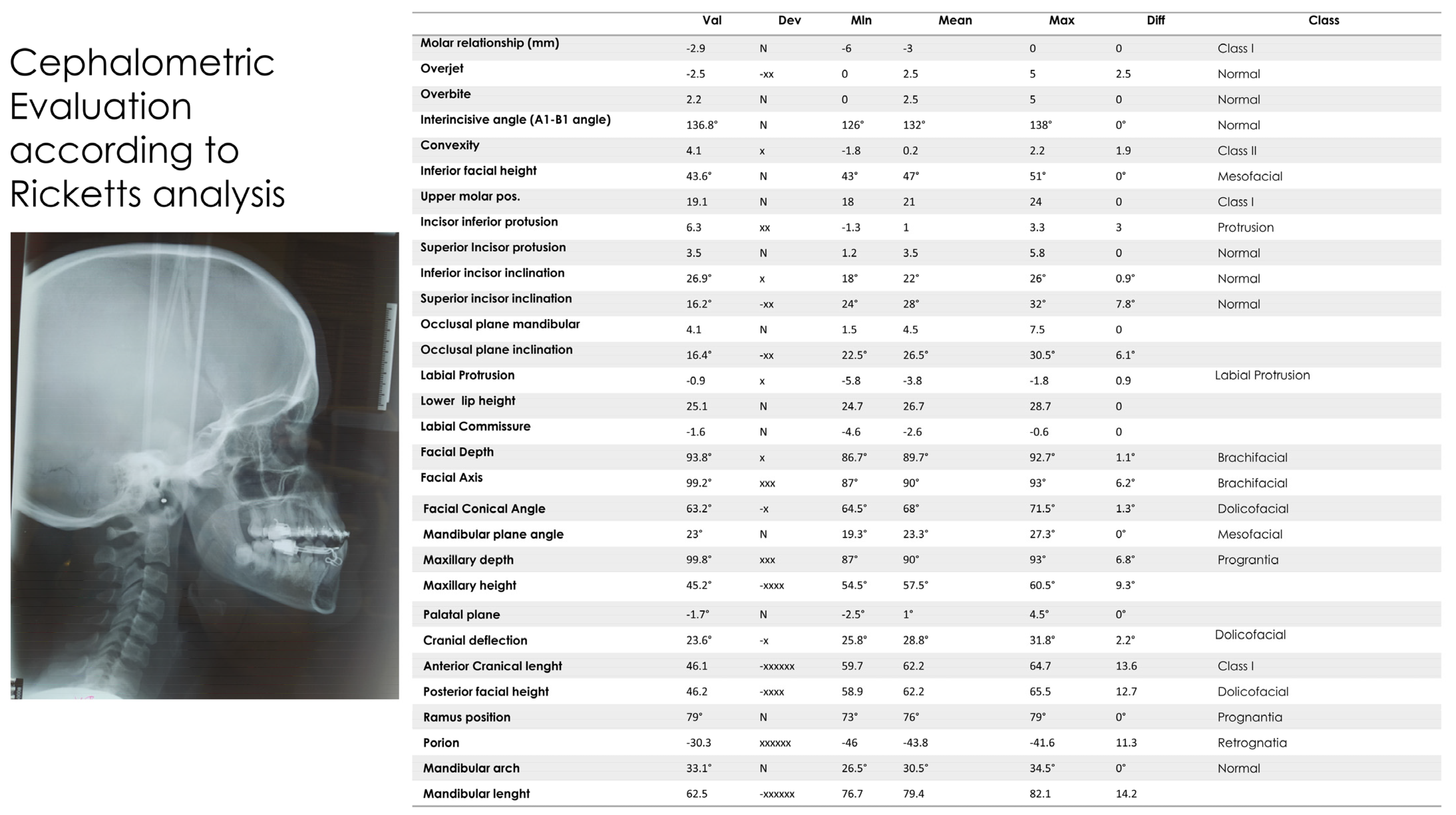
2.1. Cephalometric Analysis
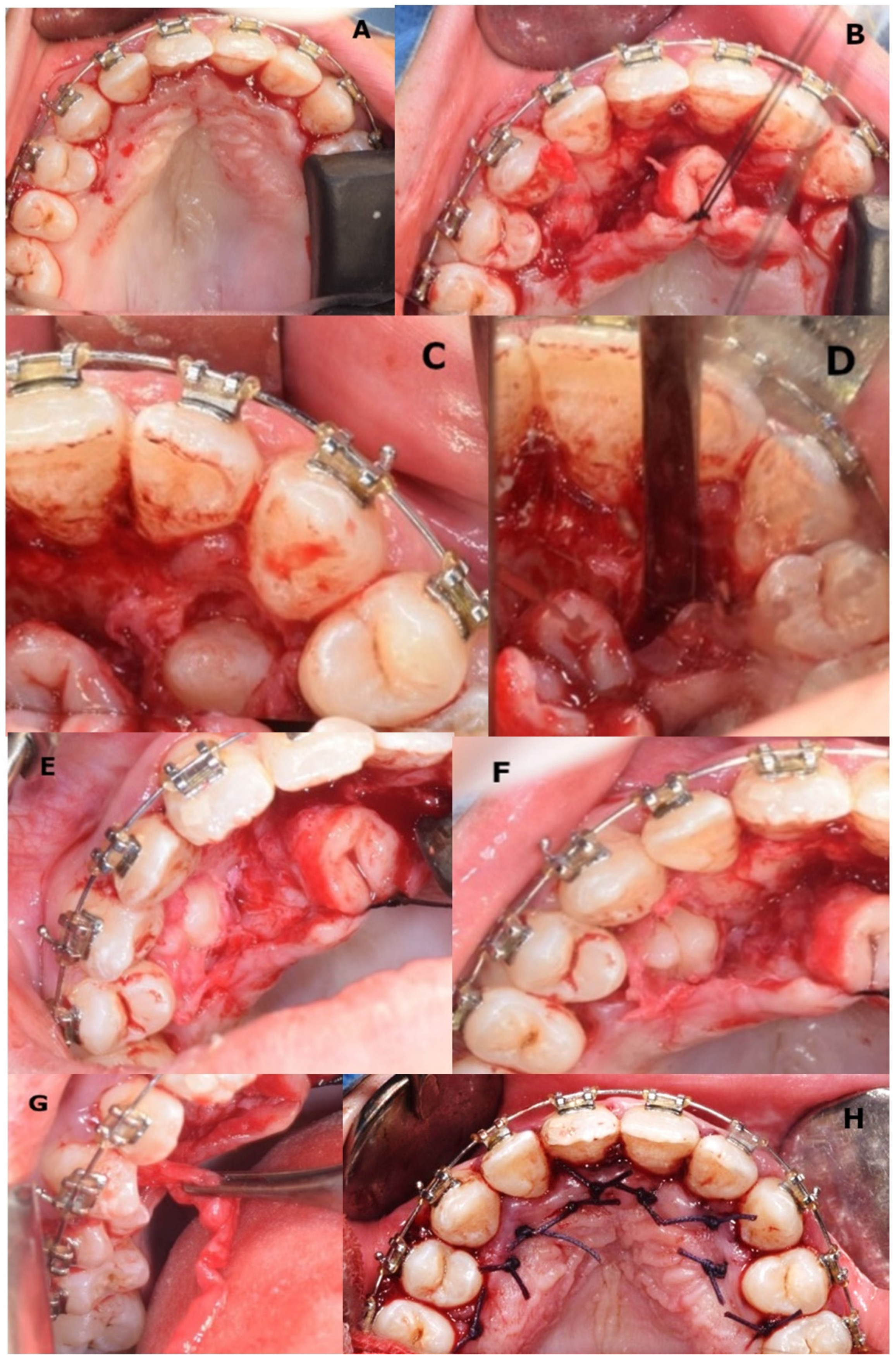
2.2. Considerations for Supranumerary Teeth Extraction
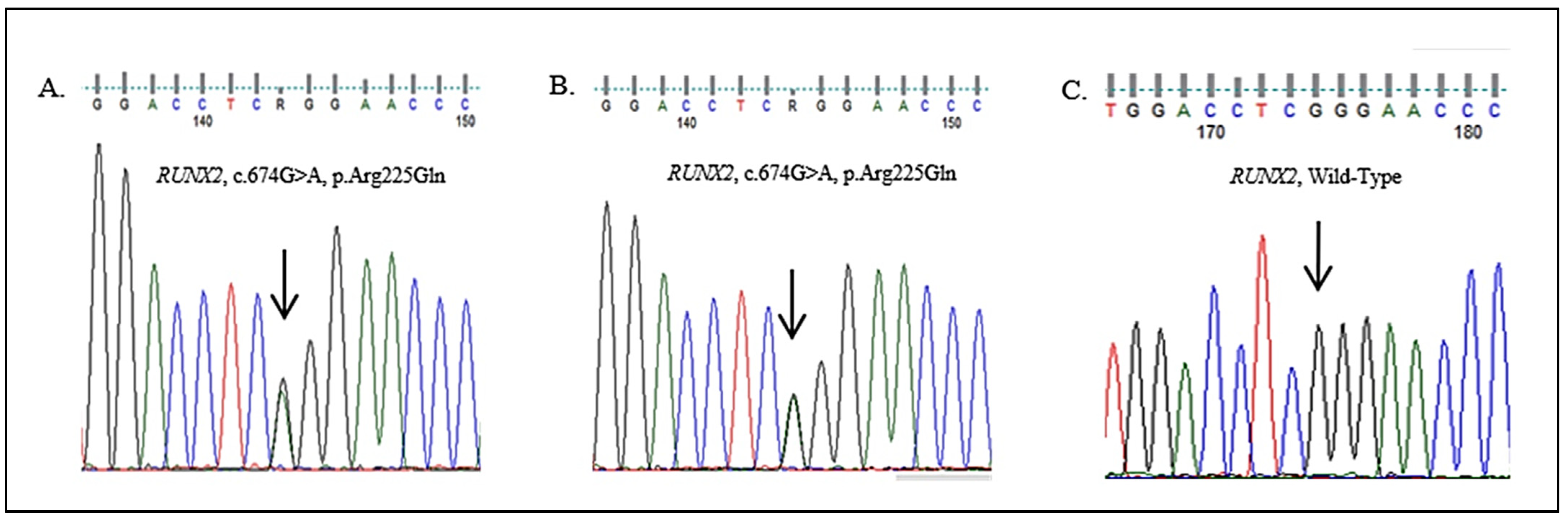
2.3. Genetic Analysis
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Impellizzeri, A.; Midulla, G.; Romeo, U.; La Monaca, C.; Barbato, E.; Galluccio, G. Delayed Eruption of Permanent Dentition and Maxillary Contraction in Patients with Cleidocranial Dysplasia: Review and Report of a Family. Int. J. Dent. 2018, 2018, 1–25. [Google Scholar] [CrossRef] [Green Version]
- Morikava, F.S.; Scariot, R.; Morosini, I.d.A.C.; Sebastiani, A.; Costa, D.J.; Fraiz, F.C.; Ferreira, F.M. Cleidocranial Dysplasia: Diagnosis, Surgical and Orthodontic Planning and Interventions in a Pediatric Patient. Int. J. Odontostomat. 2016, 10, 325–331. [Google Scholar] [CrossRef] [Green Version]
- Roberts, T.; Stephen, L.; Beighton, P. Cleidocranial Dysplasia: A Review of the Dental, Historical, and Practical Implications with an Overview of the South African Experience. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 115, 46–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, C.; Zheng, S.; Wang, Y.; Zhao, Y.; Zhu, J.; Ge, L. Mutational Analysis of RUNX2 Gene in Chinese Patients with Cleidocranial Dysplasia. Mutagenesis 2010, 25, 589–594. [Google Scholar] [CrossRef] [PubMed]
- Azevedo Almeida, L.C.; Faraj de Lima, F.B.; Matushita, H.; Valença, M.M.; Ferreira Castro, T.L.; de Mendonça, R.N. Cleidocranial Dysplasia, a Rare Skeletal Disorder with Failure of the Cranial Closure: Case-Based Update. Childs Nerv. Syst. 2020, 36, 2913–2918. [Google Scholar] [CrossRef] [PubMed]
- Cleidocraneal, D. Cleidocranial Dysostosis, a Case Report. Int. J. Odontostomat 2012, 6, 385–390. [Google Scholar]
- Adina, S. Orthopedic Joint Stability Influences Growth and Maxillary Development: Clinical Aspects. J. Biol. Regul. Homeost. Agents 2020, 34. [Google Scholar] [CrossRef]
- Takenouchi, T.; Sato, W.; Torii, C.; Kosaki, K. Progressive Cognitive Decline in an Adult Patient with Cleidocranial Dysplasia. Eur. J. Med Genet. 2014, 57, 319–321. [Google Scholar] [CrossRef]
- Hermann, N.V.; Hove, H.D.; Jørgensen, C.; Larsen, P.; Darvann, T.A.; Kreiborg, S.; Sundberg, K. Prenatal 3D Ultrasound Diagnostics in Cleidocranial Dysplasia. Fetal Diagn. Ther. 2009, 25, 36–39. [Google Scholar] [CrossRef] [PubMed]
- Hassan, N.M.M.; Dhillon, A.; Huang, B. Cleidocranial Dysplasia: Clinical Overview and Genetic Considerations. Pediatr. Dent. J. 2016, 26, 45–50. [Google Scholar] [CrossRef]
- Balaton, G.; Tarján, I.; Balaton, P.; Barabási, Z.; Nagy, K.; Vajó, Z. Orthodontic and Oral Surgery Therapy in Cleidocranial Dysplasia. Fogorv. Szle. 2007, 100, 17–21. [Google Scholar]
- Choudhary, S.; Kale, L.; Mishra, S.; Zaidi, N. Clinical and Radiological Spectrum of Cleidocranial Dysplasia: A Rare Case Report. J. Indian Acad. Oral Med. Radiol. 2017, 29, 231. [Google Scholar] [CrossRef]
- Zhao, W.; Ye, G.; Yu, X.; Xu, J.; Li, Z. Identification of a Novel Mutation in the Runt-Related Transcription Factor 2 Gene in a Chinese Family With Cleidocranial Dysplasia. J. Craniofacial Surg. 2021, 32, e541–e544. [Google Scholar] [CrossRef]
- Levanon, D.; Negreanu, V.; Bernstein, Y.; Bar-Am, I.; Avivi, L.; Groner, Y. AML1, AML2, and AML3, the Human Members of the Runt Domain Gene-Family: CDNA Structure, Expression, and Chromosomal Localization. Genomics 1994, 23, 425–432. [Google Scholar] [CrossRef]
- Cohen, M.M. RUNX Genes, Neoplasia, and Cleidocranial Dysplasia. Am. J. Med. Genet. 2001, 104, 185–188. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.M., Jr. Perspectives on RUNX Genes: An Update. Am. J. Med. Genet. 2009, 149A, 2629–2646. [Google Scholar] [CrossRef]
- Bufalino, A.; Paranaíba, L.; Gouvêa, A.; Gueiros, L.; Martelli-Júnior, H.; Junior, J.; Lopes, M.; Graner, E.; de Almeida, O.; Vargas, P.; et al. Cleidocranial Dysplasia: Oral Features and Genetic Analysis of 11 Patients: Clinical and Genetic Features of Cleidocranial Dysplasia. Oral Dis. 2012, 18, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Mundlos, S.; Mulliken, J.B.; Abramsom, D.L.; Warman, M.L.; Knoll, J.H.M.; Olsen, B.R. Genetic Mapping of Cleidocranial Dysplasia and Evidence of a Microdeletion in One Family. Hum. Mol. Genet. 1995, 4, 71–75. [Google Scholar] [CrossRef]
- Chalala, C.; Noujeim, Z.E.F.; Abou Chebel, N.; Saadé, A. Multidisciplinary Management of Cleidocranial Dysplasia. J. World Fed. Orthod. 2015, 4, 31–39. [Google Scholar] [CrossRef]
- Machuca-Tzili, L.; Monroy-Jaramillo, N.; González-del Angel, A.; Kofman-Alfaro, S. New Mutations in the CBFA1 Gene in Two Mexican Patients with Cleidocranial Dysplasia: New Mutations in the CBFA1 Gene. Clin. Genet. 2002, 61, 349–353. [Google Scholar] [CrossRef]
- Jaruga, A.; Hordyjewska, E.; Kandzierski, G.; Tylzanowski, P. Cleidocranial Dysplasia and RUNX2-Clinical Phenotype-Genotype Correlation: Cleidocranial Dysplasia and RUNX2. Clin. Genet. 2016, 90, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Anthonappa, R.P.; King, N.M.; Mahmoud Rabie, A.-B. RUNX2 Gene Status in a Cleidocranial Dysplasia Patient without Supernumerary Teeth. J. Investig. Clin. Dent. 2013, 4, 124–127. [Google Scholar] [CrossRef] [PubMed]
- Pan, C.-Y.; Tseng, Y.-C.; Lan, T.-H.; Chang, H.-P. Craniofacial Features of Cleidocranial Dysplasia. J. Dent. Sci. 2017, 12, 313–318. [Google Scholar] [CrossRef] [PubMed]
- Jirapinyo, C.; Deraje, V.; Huang, G.; Gue, S.; Anderson, P.J.; Moore, M.H. Cleidocranial Dysplasia: Management of the Multiple Craniofacial and Skeletal Anomalies. J. Craniofacial Surg. 2020, 31, 908–911. [Google Scholar] [CrossRef]
- Pourtaheri, N.; Allam, O.; Chandler, L.; Steinbacher, D.M. Orthognathic Surgery in Cleidocranial Dysplasia. J. Craniofacial Surg. 2021, 32, e290–e292. [Google Scholar] [CrossRef]
- Li, J.; Shen, J.; Xu, J.; Weng, L.; Pan, J.; Lin, J. The Treatment Strategy of Cleidocranial Dysplasia: Combined Orthodontic and Orthognathic Treatment. J. Craniofacial Surg. 2019, 30, 1767–1771. [Google Scholar] [CrossRef]
- Golan, I.; Baumert, U.; Hrala, B.P.; MUssIg, D. Early Craniofacial Signs of Cleidocranial Dysplasia. Int. J. Paediatr. Dent. 2004, 14, 49–53. [Google Scholar] [CrossRef]
- Sagisaka, T.; Tai, K.; Flores, G.; Park, J.H. Management of Cleidocranial Dysplasia. J. World Fed. Orthod. 2015, 4, 23–30. [Google Scholar] [CrossRef]
- Gömleksiz, C.; Arslan, E.; Arslan, S.; Pusat, S.; Arslan, E.A. Delayed Diagnosis of Cleidocranial Dysplasia in an Adult: A Case Report. Acta Med. Acad. 2014, 43, 92–96. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.-J.; Wang, J.-Y.; Gao, M.-F.; Wu, D.-L.; Chang, X. Orthodontic Treatment of a Patient with Cleidocranial Dysplasia: A Case Report. Exp. Ther. Med. 2016, 12, 690–694. [Google Scholar] [CrossRef] [Green Version]
- Kshar, A.; Umarji, H. Cleidocranial Dysplasia: Report of Two Cases. JIAOMR 2010, 22, S69–S72. [Google Scholar] [CrossRef]
- Patel, D.; Patel, N.; Brennan, P.A.; Kwok, J. Multidisciplinary Team Approach in the Oral Rehabilitation of Patients with Cleidocranial Dysplasia to Achieve a Functional Aesthetic Outcome. Br. J. Oral Maxillofac. Surg. 2017, 55, 932–936. [Google Scholar] [CrossRef]
- Mabrouk, Y.; Ammar, S.; Labidi, A.; Mansour, L.; Ghoul, S. Dental Prosthetic Treatments in Cleidocranial Dysplasia: Case Report and Literature Review. Case Rep. Dent. 2020, 2020, 8910798. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, G.E.; Caruso, P.A.; Small, J.E.; Jyung, R.W.; Troulis, M.J.; Curtin, H.D. Craniofacial and Temporal Bone CT Findings in Cleidocranial Dysplasia. Pediatr. Radiol. 2008, 38, 892–897. [Google Scholar] [CrossRef]
- Da Cunha, L.F.; Caetano, I.M.; Dalitz, F.; Gonzaga, C.C.; Mondelli, J. Cleidocranial Dysplasia Case Report: Remodeling of Teeth as Aesthetic Restorative Treatment. Case Rep. Dent. 2014, 2014, 901071. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inchingolo, I.; Tatullo, M.; Abenavoli, F.M.; Marrelli, M.; Inchingolo, A.D.; Gentile, M.; Inchingolo, A.M.; Dipalma, G. Non-syndromic multiple supernumerary teeth in a family unit with a normal karyotype: Case report. Int. J. Med. Sci. 2010, 7, 378–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coloccia, G.; Inchingolo, A.D.; Inchingolo, A.M.; Malcangi, G.; Montenegro, V.; Patano, A.; Marinelli, G.; Laudadio, C.; Limongelli, L.; Di Venere, D.; et al. Effectiveness of Dental and Maxillary Transverse Changes in Tooth-Borne, Bone-Borne, and Hybrid Palatal Expansion through Cone-Beam Tomography: A Systematic Review of the Literature. Medicina (Lithuania) 2021, 57, 288. [Google Scholar] [CrossRef]
- Inchingolo, F.; Tatullo, M.; Marrelli, M.; Inchingolo, A.M.; Picciariello, V.; Inchingolo, A.D.; Dipalma, G.; Vermesan, D.; Cagiano, R. Clinical trial with bromelain in third molar exodontia. Eur. Rev. Med. Pharmacol. Sci. 2010, 14, 771–774. [Google Scholar]
- Scarano, A.; Lorusso, F.; Noumbissi, S. Infrared Thermographic Evaluation of Temperature Modifications Induced during Implant Site Preparation with Steel vs. Zirconia Implant Drill. J. Clin. Med. 2020, 9, 148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maglione, M.; Bevilacqua, L.; Dotto, F.; Costantinides, F.; Lorusso, F.; Scarano, A. Observational Study on the Preparation of the Implant Site with Piezosurgery vs. Drill: Comparison between the Two Methods in Terms of Postoperative Pain, Surgical Times, and Operational Advantages. BioMed Res. Int. 2019, 2019, 8483658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dalessandri, D.; Laffranchi, L.; Tonni, I.; Zotti, F.; Piancino, M.G.; Paganelli, C.; Bracco, P. Advantages of Cone Beam Computed Tomography (CBCT) in the Orthodontic Treatment Planning of Cleidocranial Dysplasia Patients: A Case Report. Head Face Med. 2011, 7, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siriwat, P.P.; Jarabak, J.R. Malocclusion and Facial Morphology Is There a Relationship? An Epidemiologic Study. Angle Orthod. 1985, 55, 127–138. [Google Scholar]
- Ricketts, R.M. Cephalometric Analysis and Synthesis. Angle Orthod. 1961, 31, 141–156. [Google Scholar]
- Ricketts, R.M. Perspectives in the Clinical Application of Cephalometrics: The First Fifty Years. Angle Orthod. 1981, 51, 115–150. [Google Scholar]
- Steiner, C.C. Cephalometrics for You and Me. Am. J. Orthod. 1953, 39, 729–755. [Google Scholar] [CrossRef]
- Steiner, C.C. Cephalometrics in Clinical Practice. Angle Orthod. 1959, 29, 8–29. [Google Scholar]
- Inchingolo, F. Probiotics and EpiCor® in Human Health. J. Biol. Regul. Homeost. Agents 2019, 33. [Google Scholar] [CrossRef]
- Ballini, A.; Gnoni, A.; De Vito, D.; Dipalma, G.; Cantore, S.; Gargiulo Isacco, C.; Saini, R.; Santacroce, L.; Topi, S.; Scarano, A.; et al. Effect of Probiotics on the Occurrence of Nutrition Absorption Capacities in Healthy Children: A Randomized Double-Blinded Placebo-Controlled Pilot Study. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 8645–8657. [Google Scholar] [CrossRef] [PubMed]
- Ballini, A.; Dipalma, G.; Isacco, C.G.; Boccellino, M.; Di Domenico, M.; Santacroce, L.; Nguyễn, K.C.D.; Scacco, S.; Calvani, M.; Boddi, A.; et al. Oral Microbiota and Immune System Crosstalk: A Translational Research. Biology 2020, 9, 131. [Google Scholar] [CrossRef] [PubMed]
- Signorini, L. Probiotics May Modulate the Impact of Aging on Adults. J. Biol. Regul. Homeost. Agents 2020, 34. [Google Scholar] [CrossRef]
- Isacco, C.G.; Ballini, A.; De Vito, D.; Nguyen, K.C.D.; Cantore, S.; Bottalico, L.; Quagliuolo, L.; Boccellino, M.; Di Domenico, M.; Santacroce, L.; et al. Rebalancing the Oral Microbiota as an Efficient Tool in Endocrine, Metabolic and Immune Disorders. EMIDDT 2021, 21, 777–784. [Google Scholar] [CrossRef]
- Santacroce, L. The Pivotal Role of Oral Microbiota in Health and Disease. J. Biol. Regul. Homeost. Agents 2020, 34. [Google Scholar] [CrossRef]
- Scarano, A.; Noumbissi, S.; Gupta, S.; Inchingolo, F.; Stilla, P.; Lorusso, F. Scanning Electron Microscopy Analysis and Energy Dispersion X-ray Microanalysis to Evaluate the Effects of Decontamination Chemicals and Heat Sterilization on Implant Surgical Drills: Zirconia vs. Steel. Appl. Sci. 2019, 9, 2837. [Google Scholar] [CrossRef] [Green Version]
- Choi, J.; Doh, R.-M. Dental Treatment under General Anesthesia for Patients with Severe Disabilities. J. Dent. Anesth. Pain Med. 2021, 21, 87. [Google Scholar] [CrossRef] [PubMed]
- Román, M.d.P.V.; Bermudo, S.R.; Portillo, G.M. Dental Treatment under General Anesthesia: A Useful Procedure in the Third Millennium? Med. Oral Organo Of. Soc. Esp. Med. Oral Acad. Iberoam. Patol. Med. Bucal 2003, 8, 129–135. [Google Scholar]
- Pecci-Lloret, M.P.; Guerrero-Gironés, J.; López-González, B.; Rodríguez-Lozano, F.J.; Oñate-Cabrerizo, D.; Oñate-Sánchez, R.E.; Pecci-Lloret, M.R. Dental Treatments under General Anesthesia on Children with Special Health Care Needs Enrolled in the Spanish Dental Care Program. JCM 2021, 10, 182. [Google Scholar] [CrossRef] [PubMed]
- Mallineni, S.K.; Yiu, C.K.Y. A Retrospective Audit of Dental Treatment Provided to Special Needs Patients under General Anesthesia During a Ten-Year Period. J. Clin. Pediatr. Dent. 2018, 42, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Lim, M.A.W.T.; Borromeo, G.L. The Use of General Anesthesia to Facilitate Dental Treatment in Adult Patients with Special Needs. J. Dent. Anesth. Pain Med. 2017, 17, 91–103. [Google Scholar] [CrossRef] [Green Version]
- Boynes, S.G.; Lewis, C.L.; Moore, P.A.; Zovko, J.; Close, J. Complications Associated with Anesthesia Administered for Dental Treatment. Gen. Dent. 2010, 58, e20–e25. [Google Scholar] [PubMed]
- Nolan, J.; Chalkiadis, G.A.; Low, J.; Olesch, C.A.; Brown, T.C.K. Anaesthesia and Pain Management in Cerebral Palsy: Anaesthesia and Pain Management in Cerebral Palsy. Anaesthesia 2000, 55, 32–41. [Google Scholar] [CrossRef]
- Inchingolo, F.; Tatullo, M.; Abenavoli, F.M.; Marrelli, M.; Inchingolo, A.D.; Villabruna, B.; Inchingolo, A.M.; Dipalma, G. Severe Anisocoria after Oral Surgery under General Anesthesia. Int. J. Med. Sci. 2010, 7, 314–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sim, K.M.; Boey, S.K. Outpatient General Anaesthesia for Oral Surgery. Singap. Dent. J. 2000, 23, 29–37. [Google Scholar]
- Dhiman, N.K.; Singh, A.K.; Sharma, N.K.; Jaiswara, C. Cleidocranial Dysplasia. Natl. J. Maxillofac. Surg. 2014, 5, 206. [Google Scholar]
- Tri, W.M.; Triki, H.; Mansour, L.; Trabelsi, M. Cleidocranial Dysplasia: Keys to Diagnosis. IJDOS 2018, 5, 585–588. [Google Scholar] [CrossRef]
- Kolokitha, O.-E.G.; Papadopoulou, A.K. Cleidocranial Dysplasia: Etiology, Clinical Characteristics, Diagnostic Information and Treatment Approach. Hell. Orthod. Rev. 2008, 11, 21–33. [Google Scholar]
- Farronato, G.; Maspero, C.; Farronato, D.; Gioventù, S. Orthodontic Treatment in a Patient with Cleidocranial Dysostosis. Angle Orthod. 2009, 79, 178–185. [Google Scholar] [CrossRef] [PubMed]
- Matthews-Brzozowska, T.; Hojan-Jezierska, D.; Loba, W.; Worona, M.; Matthews-Brzozowski, A. Cleidocranial Dysplasia-Dental Disorder Treatment and Audiology Diagnosis. Open Med. 2018, 13, 1–8. [Google Scholar] [CrossRef] [Green Version]
- El-Gharbawy, A.H.; Peeden, J.N.; Lachman, R.S.; Graham, J.M.; Moore, S.R.; Rimoin, D.L. Severe Cleidocranial Dysplasia and Hypophosphatasia in a Child with Microdeletion of the C-Terminal Region of RUNX2. Am. J. Med. Genet. 2010, 152A, 169–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Witcher, T.P.; Brand, S.; Gwilliam, J.R.; McDonald, F. Assessment of the Anterior Maxilla in Orthodontic Patients Using Upper Anterior Occlusal Radiographs and Dental Panoramic Tomography: A Comparison. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 2010, 109, 765–774. [Google Scholar] [CrossRef]
- Tsuji, M.; Suzuki, H.; Suzuki, S.; Moriyama, K. Three-dimensional Evaluation of Morphology and Position of Impacted Supernumerary Teeth in Cases of Cleidocranial Dysplasia. Congenit. Anom. 2020, 60, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Anthonappa, R.P.; King, N.M.; Rabie, A.B.M.; Mallineni, S.K. Reliability of Panoramic Radiographs for Identifying Supernumerary Teeth in Children. Int. J. Paediatr. Dent. 2012, 22, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Toureno, L.; Park, J.H.; Cederberg, R.A.; Hwang, E.H.; Shin, J.-W. Identification of Supernumerary Teeth in 2D and 3D: Review of Literature and a Proposal. J. Dent. Educ. 2013, 77, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Kreiborg, S.; Jensen, B.L. Tooth Formation and Eruption—Lessons Learnt from Cleidocranial Dysplasia. Eur. J. Oral. Sci. 2018, 126, 72–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manjunath, K.; Kavitha, B.; Saraswathi, T.R.; Sivapathasundharam, B.; Manikandhan, R. Cementum Analysis in Cleidocranial Dysostosis. Indian J. Dent. Res. 2008, 19, 253. [Google Scholar] [PubMed]
- Counts, A.L.; Rohrer, M.D.; Prasad, H.; Bolen, P. An Assessment of Root Cementum in Cleidocranial Dysplasia. Angle Orthod. 2001, 71, 293–298. [Google Scholar] [CrossRef]
- Zhu, Y.; Zou, Y.; Yu, Q.; Sun, H.; Mou, S.; Xu, S.; Zhu, M. Combined Surgical-Orthodontic Treatment of Patients with Cleidocranial Dysplasia: Case Report and Review of the Literature. Orphanet. J. Rare Dis. 2018, 13, 217. [Google Scholar] [CrossRef]
- Shekhawat, V.; Gulati, Y. Cleidocranial Dysplasia—A Case Report Discussing the Clinical and Radiological Manifestations. J. Mar. Med. Soc. 2020, 22, 238. [Google Scholar] [CrossRef]
- Lu, H.; Zeng, B.; Yu, D.; Jing, X.; Hu, B.; Zhao, W.; Wang, Y. Complex Dental Anomalies in a Belatedly Diagnosed Cleidocranial Dysplasia Patient. Imaging Sci. Dent. 2015, 45, 187–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chae, Y.K.; Lee, H.; Jih, M.K.; Lee, H.-S.; Lee, J.-W.; Kim, S.-H.; Kim, G.-T.; Choi, S.C.; Nam, O.H. Validation of a Three-Dimensional Printed Model for Training of Surgical Extraction of Supernumerary Teeth. Eur. J. Dent. Educ. 2020, 24, 637–643. [Google Scholar] [CrossRef]
- Petropoulos, V.C.; Balshi, T.J.; Wolfinger, G.J.; Balshi, S.F. Treatment of a Patient with Cleidocranial Dysplasia Using a Single-Stage Implant Protocol: Treatment of a Patient with Cleidocranial Dysplasia. J. Prosthodont. 2011, 20, S26–S31. [Google Scholar] [CrossRef]
- Dohan Ehrenfest, D.M.; Del Corso, M.; Inchingolo, F.; Sammartino, G.; Charrier, J.-B. Platelet-Rich Plasma (PRP) and Platelet-Rich Fibrin (PRF) in Human Cell Cultures: Growth Factor Release and Contradictory Results. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 110, 418–421. [Google Scholar] [CrossRef]
- Dohan Ehrenfest, D.M.; Del Corso, M.; Inchingolo, F.; Charrier, J.-B. Selecting a Relevant in Vitro Cell Model for Testing and Comparing the Effects of a Choukroun’s Platelet-Rich Fibrin (PRF) Membrane and a Platelet-Rich Plasma (PRP) Gel: Tricks and Traps. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 110, 409–411. [Google Scholar] [CrossRef] [PubMed]
- Otto, F.; Kanegane, H.; Mundlos, S. Mutations in TheRUNX2 Gene in Patients with Cleidocranial Dysplasia. Hum. Mutat. 2002, 19, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Machol, K.; Mendoza-Londono, R.; Lee, B. Cleidocranial Dysplasia Spectrum Disorder; University of Washington: Seattle, WA, USA, 2017. [Google Scholar]
- Xuan, D.; Li, S.; Zhang, X.; Hu, F.; Lin, L.; Wang, C.; Zhang, J. Mutations in the RUNX2 Gene in Chinese Patients with Cleidocranial Dysplasia. Ann. Clin. Lab. Sci. 2008, 38, 15–24. [Google Scholar]
- Lin, W.-D.; Lin, S.-P.; Wang, C.-H.; Tsai, Y.; Chen, C.-P.; Tsai, F.-J. RUNX2 Mutations in Taiwanese Patients with Cleidocranial Dysplasia. Genet. Mol. Biol. 2011, 34, 201–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, L.Z.; Su, W.Q.; Liu, Y.F.; Ge, X.; Zhang, Y.; Wang, X.J. Role of the RUNX2 p.R225Q Mutation in Cleidocranial Dysplasia: A Rare Presentation and an Analysis of the RUNX2 Protein Structure. Genet. Mol. Res. 2014, 13, 1187–1194. [Google Scholar] [CrossRef]
- Yoshida, T.; Kanegane, H.; Osato, M.; Yanagida, M.; Miyawaki, T.; Ito, Y.; Shigesada, K. Functional Analysis of RUNX2 Mutations in Japanese Patients with Cleidocranial Dysplasia Demonstrates Novel Genotype-Phenotype Correlations. Am. J. Hum. Genet. 2002, 71, 724–738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stewart, M.; Terry, A.; Hu, M.; O’Hara, M.; Blyth, K.; Baxter, E.; Cameron, E.; Onions, D.E.; Neil, J.C. Proviral Insertions Induce the Expression of Bone-Specific Isoforms of PEBP2 A (CBFA1): Evidence for a New Myc Collaborating Oncogene. Proc. Natl. Acad. Sci. USA 1997, 94, 8646–8651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drissi, H.; Luc, Q.; Shakoori, R.; Chuva De Sousa Lopes, S.; Choi, J.Y.; Terry, A.; Hu, M.; Jones, S.; Neil, J.C.; Lian, J.B.; et al. Transcriptional Autoregulation of the Bone Related CBFA1/RUNX2 Gene. J. Cell Physiol. 2000, 184, 341–350. [Google Scholar] [CrossRef]
- Xiao, Z.S.; Liu, S.-G.; Hinson, T.K.; Quarles, L.D. Characterization of the Upstream MouseCbfa1/Runx2 Promoter. J. Cell. Biochem. 2001, 82, 647–659. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, C.; Javed, A.; Choi, J.-Y.; Green, J.; Rosen, V.; van Wijnen, A.J.; Stein, J.L.; Lian, J.B.; Stein, G.S. Differential Regulation of the Two Principal Runx2/Cbfa1 N-Terminal Isoforms in Response to Bone Morphogenetic Protein-2 during Development of the Osteoblast Phenotype. Endocrinology 2001, 142, 4026–4039. [Google Scholar] [CrossRef] [PubMed]
- Tamiya, H.; Ikeda, T.; Jeong, J.-H.; Saito, T.; Yano, F.; Jung, Y.-K.; Ohba, S.; Kawaguchi, H.; Chung, U.; Choi, J.-Y. Analysis of the Runx2 Promoter in Osseous and Non-Osseous Cells and Identification of HIF2A as a Potent Transcription Activator. Gene 2008, 416, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.C.; Lengner, C.J.; Gaur, T.; Lou, Y.; Hussain, S.; Jones, M.D.; Borodic, B.; Colby, J.L.; Steinman, H.A.; van Wijnen, A.J.; et al. Runx2 Protein Expression Utilizes the Runx2 P1 Promoter to Establish Osteoprogenitor Cell Number for Normal Bone Formation. J. Biol. Chem. 2011, 286, 30057–30070. [Google Scholar] [CrossRef] [Green Version]
- Bruderer, M.; Richards, R.; Alini, M.; Stoddart, M. Role and Regulation of RUNX2 in Osteogenesis. eCM 2014, 28, 269–286. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Z.-S.; Hjelmeland, A.B.; Quarles, L.D. Selective Deficiency of the “Bone-Related” Runx2-II Unexpectedly Preserves Osteoblast-Mediated Skeletogenesis. J. Biol. Chem. 2004, 279, 20307–20313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harada, H.; Tagashira, S.; Fujiwara, M.; Ogawa, S.; Katsumata, T.; Yamaguchi, A.; Komori, T.; Nakatsuka, M. Cbfa1 Isoforms Exert Functional Differences in Osteoblast Differentiation. J. Biol. Chem. 1999, 274, 6972–6978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, K.-Y.; Lee, S.-W.; Park, M.-H.; Bae, Y.-C.; Shin, H.-I.; Nam, S.-H.; Kim, Y.-J.; Kim, H.-J.; Ryoo, H.-M. Spatio-Temporal Expression Patterns of Runx2 Isoforms in Early Skeletogenesis. Exp. Mol. Med. 2002, 34, 426–433. [Google Scholar] [CrossRef] [Green Version]
- Stein, G.S.; Lian, J.B.; van Wijnen, A.J.; Stein, J.L.; Montecino, M.; Javed, A.; Zaidi, S.K.; Young, D.W.; Choi, J.-Y.; Pockwinse, S.M. Runx2 Control of Organization, Assembly and Activity of the Regulatory Machinery for Skeletal Gene Expression. Oncogene 2004, 23, 4315–4329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, T.M.; Lee, E.H. Transcriptional Regulatory Cascades in Runx2-Dependent Bone Development. Tissue Eng. Part. B Rev. 2013, 19, 254–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoda, S.; Suda, N.; Kitahara, Y.; Komori, T.; Ohyama, K. Delayed Tooth Eruption and Suppressed Osteoclast Number in the Eruption Pathway of Heterozygous Runx2/Cbfa1 Knockout Mice. Arch. Oral Biol. 2004, 49, 435–442. [Google Scholar] [CrossRef] [PubMed]
- Quack, I.; Vonderstrass, B.; Stock, M.; Aylsworth, A.; Becker, A.; Brueton, L.; Lee, P.; Majewski, F.; Mulliken, J.; Suri, M.; et al. Mutation Analysis of Core Binding Factor A1 in Patients with Cleidocranial Dysplasia. Am. J. Hum. Genet. 1999, 65, 1268–1278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goto, T.; Aramaki, M.; Yoshihashi, H.; Nishimura, G.; Hasegawa, Y.; Takahashi, T.; Ishii, T.; Fukushima, Y.; Kosaki, K. Large Fontanelles Are a Shared Feature of Haploinsufficiency of RUNX2 and Its Co-Activator CBFB. Congenit. Anom. (Kyoto) 2004, 44, 225–229. [Google Scholar] [CrossRef] [PubMed]


















Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inchingolo, A.D.; Patano, A.; Coloccia, G.; Ceci, S.; Inchingolo, A.M.; Marinelli, G.; Malcangi, G.; Montenegro, V.; Laudadio, C.; Palmieri, G.; et al. Genetic Pattern, Orthodontic and Surgical Management of Multiple Supplementary Impacted Teeth in a Rare, Cleidocranial Dysplasia Patient: A Case Report. Medicina 2021, 57, 1350. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57121350
Inchingolo AD, Patano A, Coloccia G, Ceci S, Inchingolo AM, Marinelli G, Malcangi G, Montenegro V, Laudadio C, Palmieri G, et al. Genetic Pattern, Orthodontic and Surgical Management of Multiple Supplementary Impacted Teeth in a Rare, Cleidocranial Dysplasia Patient: A Case Report. Medicina. 2021; 57(12):1350. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57121350
Chicago/Turabian StyleInchingolo, Alessio Danilo, Assunta Patano, Giovanni Coloccia, Sabino Ceci, Angelo Michele Inchingolo, Grazia Marinelli, Giuseppina Malcangi, Valentina Montenegro, Claudia Laudadio, Giulia Palmieri, and et al. 2021. "Genetic Pattern, Orthodontic and Surgical Management of Multiple Supplementary Impacted Teeth in a Rare, Cleidocranial Dysplasia Patient: A Case Report" Medicina 57, no. 12: 1350. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57121350