
Inflammatory Undifferentiated Pleomorphic Sarcoma Mimicking Bacteremia in an Elderly Patient: A Case Report


Abstract
:1. Introduction
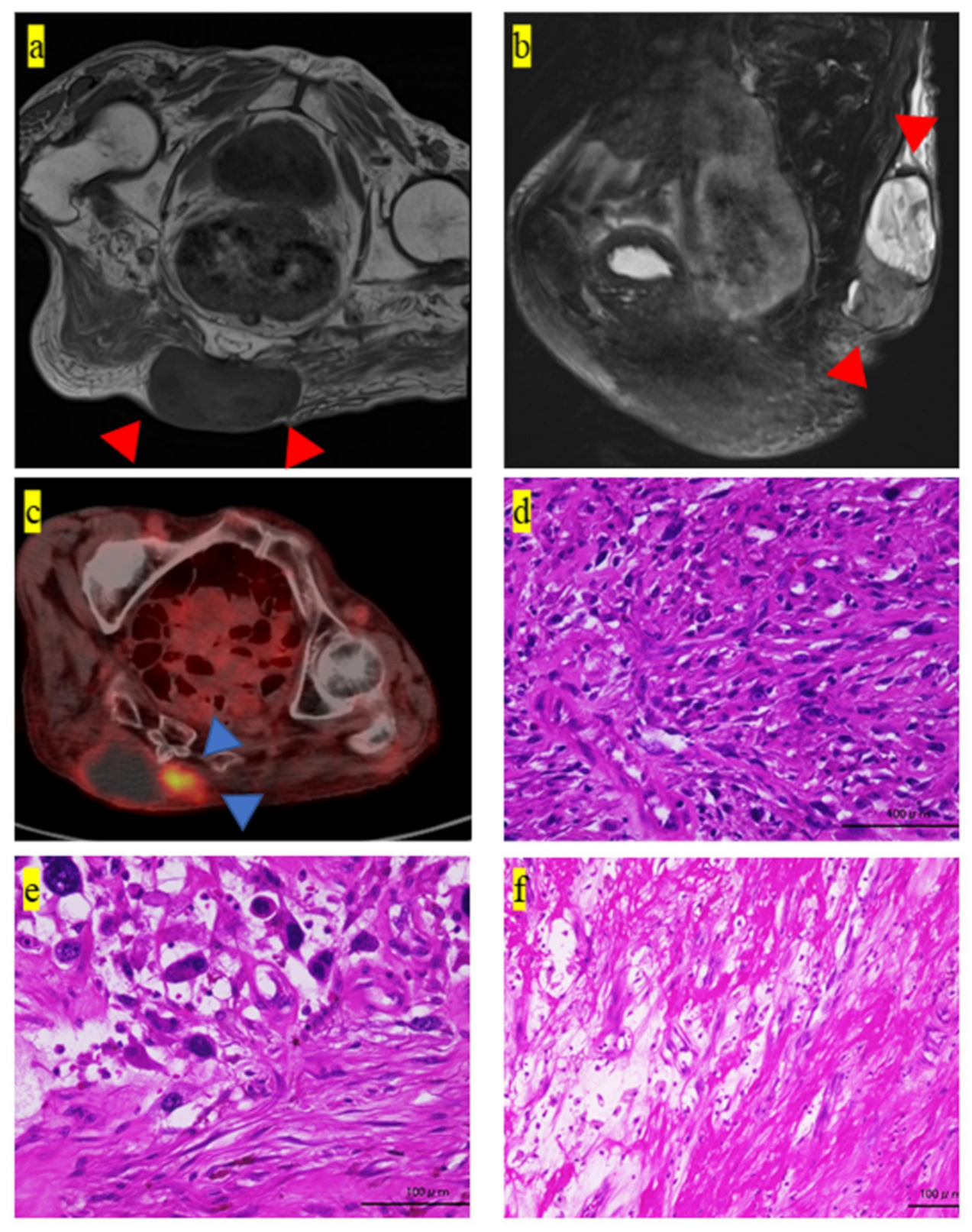
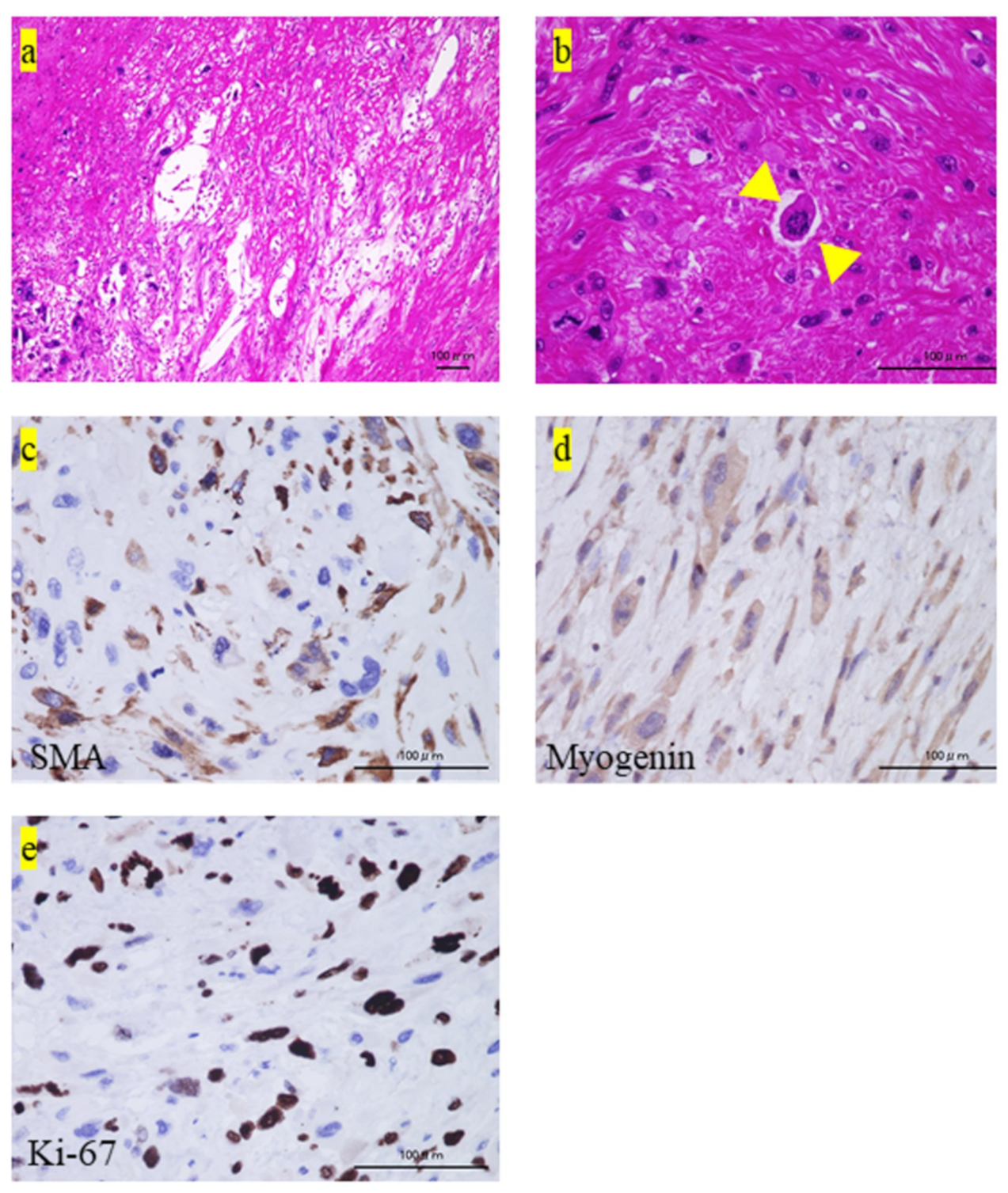
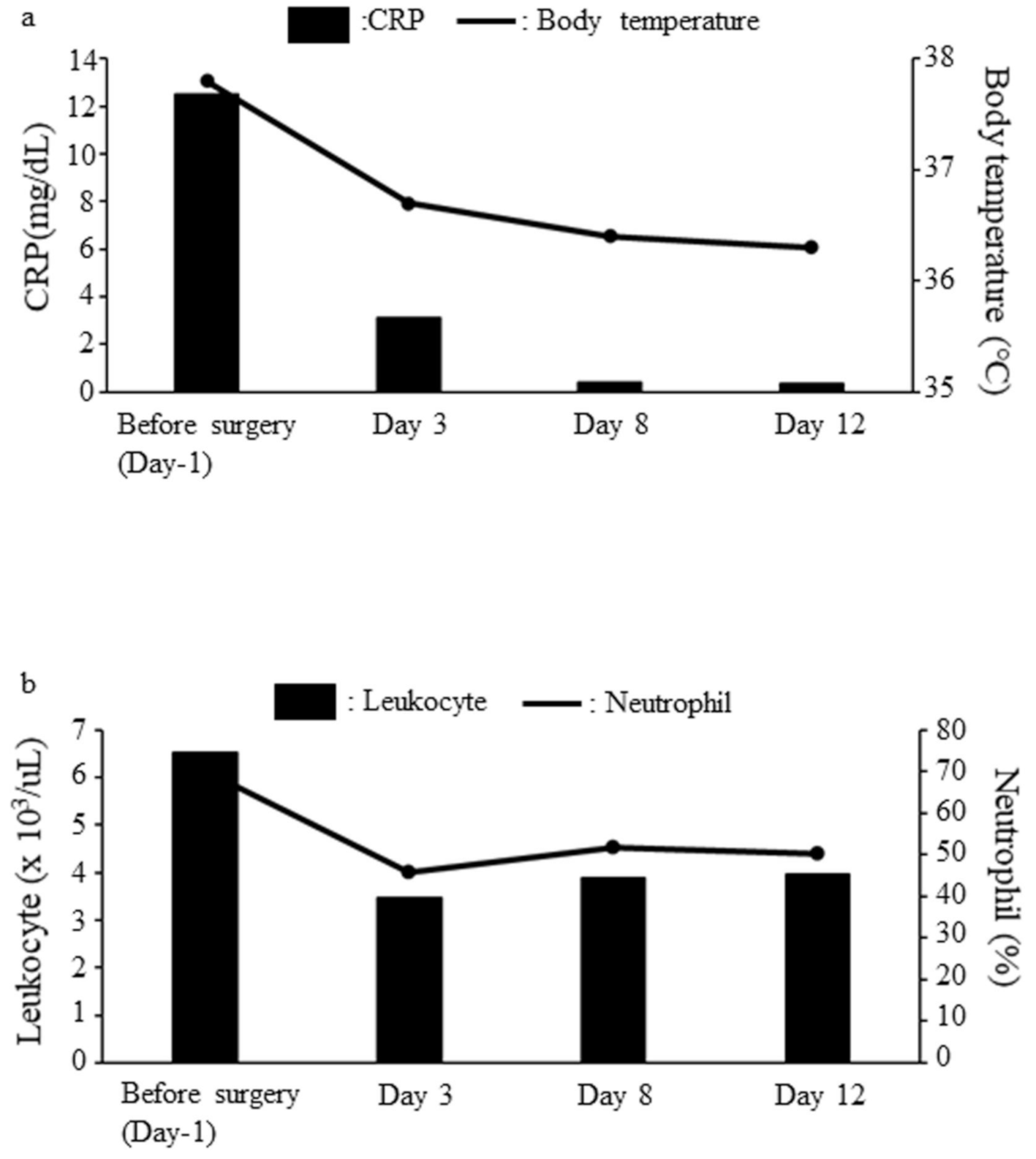
2. Case Presentation
3. Discussion
4. Conclusion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fletcher, C.D.; Lazar, A.J. WHO classification of tumors of soft tissue and bone. In Soft Tissue and Bone Tumours, 5th ed.; IARC Publications: Lyon, France, 2020. [Google Scholar]
- Weiss, S.W.; Enzinger, F.M. Malignant fibrous histiocytoma: an analysis of 200 cases. Cancer 1978, 41, 2250–2266. [Google Scholar] [CrossRef]
- Nakamura, T.; Matsumine, A.; Matsubara, T.; Asanuma, K.; Uchida, A.; Sudo, A. Clinical significance of pretreatment serum C-reactive protein level in soft tissue sarcoma. Cancer 2012, 118, 1055–1061. [Google Scholar] [CrossRef] [PubMed]
- Hayashida, K.; Kawabata, Y.; Kato, I.; Suzuki, M.; Takeyama, M.; Inaba, Y. G-CSF production by undifferentiated pleomorphic sarcoma with leukemoid reaction occurred in the lower leg: A case report. JBJS Case Connect. 2020, 10, e0624. [Google Scholar] [CrossRef]
- Gundle, K.R.; Kafchinski, L.; Gupta, S.; Griffin, A.M.; Dickson, B.C.; Chung, P.W.; Catton, C.N.; O’Sullivan, B.; Wunder, J.S.; Ferguson, P.C. Analysis of margin classification systems for assessing the risk of local recurrence after soft tissue sarcoma resection. J. Clin. Oncol. 2018, 36, 704–709. [Google Scholar] [CrossRef] [Green Version]
- Truong, L.D.; Rangdaeng, S.; Cagle, P.; Ro, J.Y.; Hawkins, H.; Font, R.L. The diagnostic utility of desmin. A study of 584 cases and review of the literature. Am. J. Clin. Pathol. 1990, 93, 305–314. [Google Scholar] [CrossRef]
- de Saint Aubain Somerhausen, N.; Fletcher, C.D. Leiomyosarcoma of soft tissue in children: Clinicopathologic analysis of 20 cases. Am. J. Surg. Pathol. 1999, 23, 755–763. [Google Scholar] [CrossRef]
- Dabbs, D.J.; Silverman, J.F.; Geisinger, K.R. Immunohistochemical study of uterine stromal sarcoma and rhabdomyosarcoma. Arch. Pathol. Lab. Med. 1989, 113, 1151–1154. [Google Scholar]
- Smith, T.A.; Machen, S.K.; Fisher, C.; Goldblum, J.R. Usefulness of cytokeratin subsets for distinguishing monophasic syn-ovial sarcoma from malignant peripheral nerve sheath tumor. Am. J. Clin. Pathol. 1999, 112, 641–648. [Google Scholar] [CrossRef] [Green Version]
- Kyriakos, M.; Kempson, R.L. Inflammatory fibrous histiocytoma. An aggressive and lethal lesion. Cancer 1976, 37, 1584–1606. [Google Scholar] [CrossRef]
- Nakanishi, H.; Araki, N.; Kudawara, I.; Kuratsu, S.; Matsumine, A.; Mano, M.; Naka, N.; Myoui, A.; Ueda, T.; Yoshikawa, H. Clinical implications of serum C-reactive protein levels in malignant fibrous histiocytoma. Int. J. Cancer 2002, 99, 167–170. [Google Scholar] [CrossRef]
- Hamada, T.; Komiya, S.; Hiraoka, K.; Zenmyo, M.; Morimatsu, M.; Inoue, A. IL-6 in a pleomorphic type of malignant fi-brous histiocytoma presenting high fever. Hum. Pathol. 1998, 29, 758–761. [Google Scholar] [CrossRef]
- Petitprez, F.; de Reyniès, A.; Keung, E.Z.; Chen, T.W.; Sun, C.M.; Calderaro, J.; Jeng, Y.M.; Hsiao, L.P.; Lacroix, L.; Bougoüin, A.; et al. B cells are associated with survival and immunotherapy response in sarcoma. Nature 2020, 577, 556–560. [Google Scholar] [CrossRef] [PubMed]
- Hurtado-Cordovi, J.; Avezbakiyev, B.; Frieri, M.; Freedman, L.; Gebre, W. Cutaneous inflammatory malignant fibrous histiocytoma presenting with a leukemoid reaction: A case report and review of the literature. Case Rep. Med. 2012, 798629. [Google Scholar] [CrossRef] [Green Version]
- Hurtado-Cordovi, J.; Pathak, P.; Avezbakiyev, B.; Frieri, M. Inflammatory malignant fibrous histiocytoma associated with leukemoid reaction or leukocytosis: A comprehensive review. ISRN Oncol. 2012, 946019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dillon, S.R.; Sprecher, C.; Hammond, A.; Bilsborough, J.; Rosenfeld-Franklin, M.; Presnell, S.R.; Haugen, H.S.; Maurer, M.; Harder, B.; Johnston, J.; et al. Interleukin 31, a cytokine produced by activated T cells, induces dermatitis in mice. Nat. Immunol. 2004, 5, 752–760. [Google Scholar] [CrossRef]
- Derouet, D.; Rousseau, F.; Alfonsi, F.; Froger, J.; Hermann, J.; Barbier, F.; Perret, D.; Diveu, C.; Guillet, C.; Preisser, L.; et al. Neuropoietin, a new IL-6-related cytokine signaling through the ciliary neurotrophic factor receptor. Proc. Natl. Acad. Sci. USA 2004, 101, 4827–4832. [Google Scholar] [CrossRef] [Green Version]
- Jones, S.A.; Richards, P.J.; Scheller, J.; Rose-John, S. IL-6 transsignaling: The in vivo consequences. J. Interferon. Cytokine Res. 2005, 25, 241–253. [Google Scholar] [CrossRef]
- Brouns, F.; Stas, M.; De Wever, I. Delay in diagnosis of soft tissue sarcomas. Eur. J. Surg. Oncol. 2003, 29, 440–445. [Google Scholar] [CrossRef]
- Iritani, S.; Tohgi, M.; Miyata, H.; Ohi, G. Impact of dementia on cancer discovery and pain. Psychogeriatrics 2011, 11, 6–13. [Google Scholar] [CrossRef] [PubMed]
- Dong, A.; Wang, Y.; Dong, H.; Gong, J.; Cheng, C.; Zuo, C.; Lu, J. Inflammatory myofibroblastic tumor: FDG PET/CT findings with pathologic correlation. Clin. Nucl. Med. 2014, 39, 113–121. [Google Scholar] [CrossRef]
- Liu, D.N.; Li, Z.W.; Wang, H.Y.; Zhao, M.; Zhao, W.; Hao, C.Y. Use of 18F-FDG-PET/CT for Retroperitoneal/Intra-Abdominal Soft Tissue Sarcomas. Contrast Media Mol. Imaging. 2018, 2601281. [Google Scholar] [CrossRef]
- Iwamoto, Y.; Tanaka, K.; Isu, K.; Kawai, A.; Tatezaki, S.; Ishii, T.; Kushida, K.; Beppu, Y.; Usui, M.; Tateishi, A.; et al. Multiinstitutional phase II study of neoadjuvant chemotherapy for osteosarcoma (NECO study) in Japan: NECO-93J and NECO-95J. J. Orthop. Sci. 2009, 14, 397–404. [Google Scholar] [CrossRef]
- Larrier, N.A.; Czito, B.G.; Kirsch, D.G. Radiation therapy for soft tissue sarcoma: Indications and controversies for neo-adjuvant therapy, adjuvant therapy, intraoperative radiation therapy, and brachytherapy. Surg. Oncol. Clin. North Am. 2016, 25, 841–860. [Google Scholar] [CrossRef]
- Weiskopf, D.; Weinberger, B.; Grubeck-Loebenstein, B. The aging of the immune system. Transpl. Int. 2009, 22, 1041–1050. [Google Scholar] [CrossRef]
- Hashimoto, K.; Nishimura, S.; Hara, Y.; Oka, N.; Tanaka, H.; Iemura, S.; Akagi, M. Clinical outcomes of patients with primary malignant bone and soft tissue tumor aged 65 years or older. Exp. Ther. Med. 2019, 17, 888–894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rutkowski, P.; Kaminska, J.; Kowalska, M.; Ruka, W.; Steffen, J. Cytokine serum levels in soft tissue sarcoma patients: Correlations with clinico-pathological features and prognosis. Int. J. Cancer 2002, 100, 463–471. [Google Scholar] [CrossRef] [PubMed]
- Osaka, S.; Sugita, H.; Osaka, E.; Yoshida, Y.; Ryu, J. Surgical management of malignant soft tissue tumours in patients aged 65 years or older. J. Orthop. Surg. 2003, 11, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Yoneda, Y.; Kunisada, T.; Naka, N.; Nishida, Y.; Kawai, A.; Morii, T.; Takeda, K.; Hasei, J.; Yamakawa, Y.; Ozaki, T. Japanese Musculoskeletal Oncology Group Favorable outcome after complete resection in elderly soft tissue sarcoma pa-tients: Japanese musculoskeletal oncology group study. Eur. J. Surg. Oncol. 2014, 40, 49–54. [Google Scholar] [CrossRef]
- Daigler, A.; Zmarsly, I.; Hirsch, T.; Goertz, O.; Steinau, H.U.; Lehnhardt, M.; Harati, K. Long-term outcome after local recurrence of soft tissue sarcoma: A retrospective analysis of factors predictive of survival in 135 patients with locally re-current soft tissue sarcoma. Br. J. Cancer 2014, 110, 1456–1464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitelman, F.; Johansson, B.; Mertens, F. The impact of translocations and gene fusions on cancer causation. Nat. Rev. Cancer 2007, 7, 233–245. [Google Scholar] [CrossRef]
- Rubin, B.P.; Nishijo, K.; Chen, H.I.; Yi, X.; Schuetze, D.P.; Pal, R.; Prajapati, S.I.; Abraham, J.; Arenkiel, B.R.; Chen, Q.R.; et al. Evidence for an unanticipated relationship between undifferentiated pleomorphic sarcoma and embryonal rhabdomyosarcoma. Cancer Cell 2011, 19, 177–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelleher, F.C.; Viterbo, A. Histologic and Genetic Advances in Refining the Diagnosis of “Undifferentiated Pleomorphic Sarcoma”. Cancers 2013, 5, 218–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Item | Value | Lower Limit | Upper Limit |
|---|---|---|---|
| CRP (mg/dL) | 12.51 | 0 | 0.14 |
| Cr (mg/dL) | 1.28 | 0.46 | 0.79 |
| Alb (g/dL) | 2.1 | 4.1 | 5.1 |
| AST (U/L) | 26 | 13 | 30 |
| ALT (U/L) | 23 | 7 | 23 |
| Leukocytes (x 103/µL) | 6.51 | 3.3 | 8.6 |
| Hb (g/dL) | 7.9 | 11.6 | 14.8 |
| PLT (x 104/uL) | 38.0 | 15.8 | 34.8 |
| Neutrophils (%) | 70.3 | 38 | 77 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hashimoto, K.; Nishimura, S.; Ito, T.; Oka, N.; Akagi, M. Inflammatory Undifferentiated Pleomorphic Sarcoma Mimicking Bacteremia in an Elderly Patient: A Case Report. Medicina 2021, 57, 175. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57020175
Hashimoto K, Nishimura S, Ito T, Oka N, Akagi M. Inflammatory Undifferentiated Pleomorphic Sarcoma Mimicking Bacteremia in an Elderly Patient: A Case Report. Medicina. 2021; 57(2):175. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57020175
Chicago/Turabian StyleHashimoto, Kazuhiko, Shunji Nishimura, Tomohiko Ito, Naohiro Oka, and Masao Akagi. 2021. "Inflammatory Undifferentiated Pleomorphic Sarcoma Mimicking Bacteremia in an Elderly Patient: A Case Report" Medicina 57, no. 2: 175. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57020175