
Primary Hepatic Extranodal Marginal Zone Lymphoma of Mucosa-Associated Lymphoid Tissue in a Patient with Chronic Hepatitis B Virus Infection: Case Report and Summary of the Literature

 , , ,
, , ,
Abstract
:1. Introduction
2. Case Presentation
3. Discussion

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Present Case | Common Findings of Previously Reported Cases [7,32,33,41,42] | Common Findings of Typical Hepatocellular Carcinoma [43,44,45] | |
|---|---|---|---|
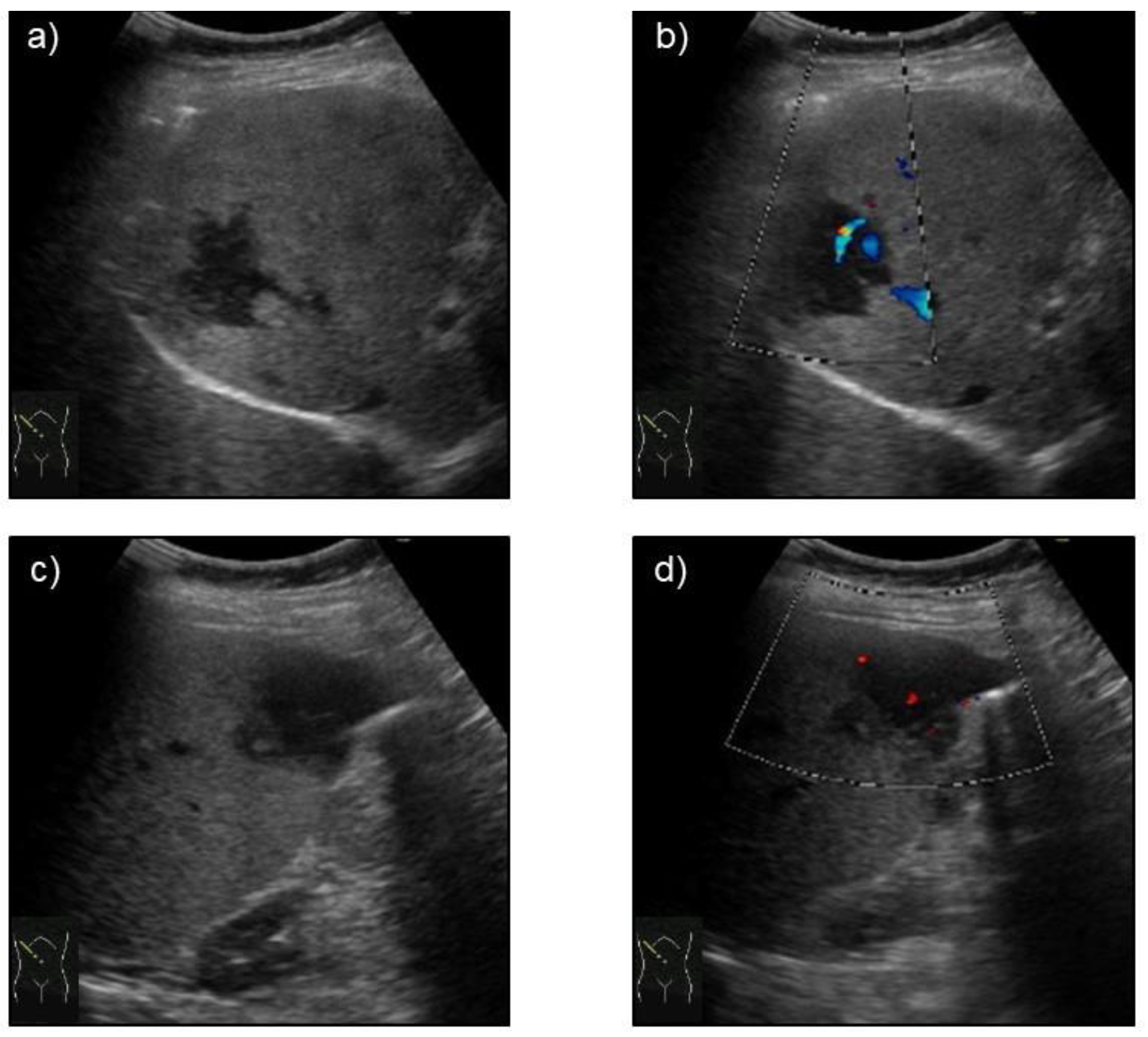
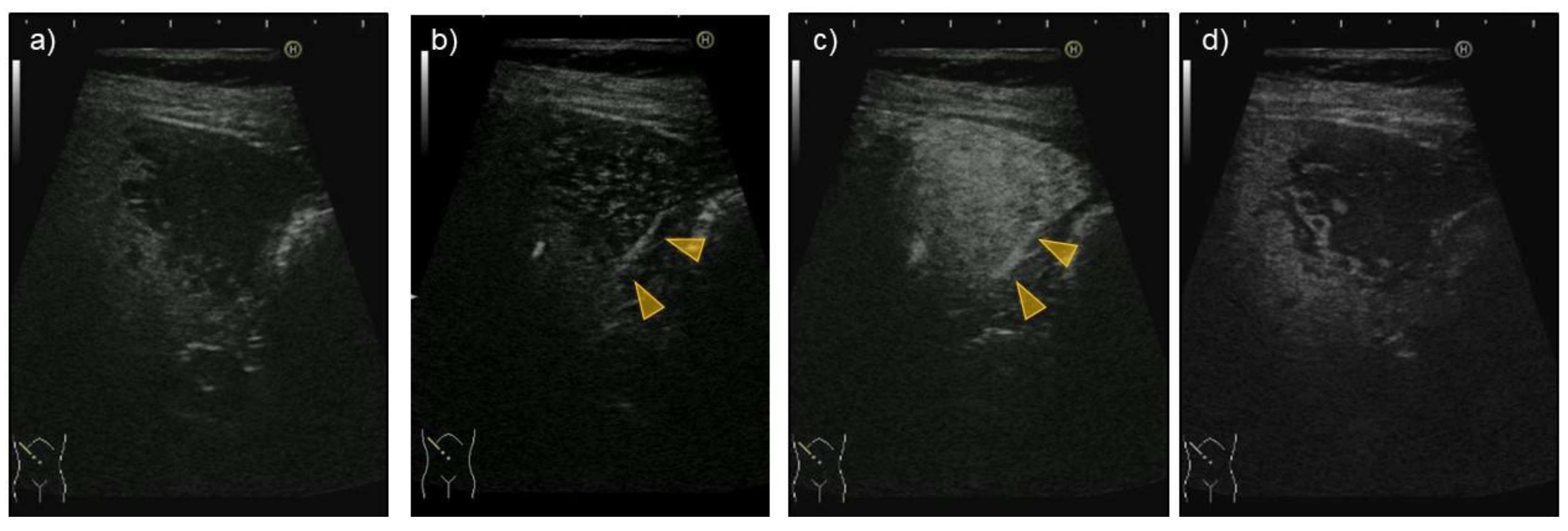
| US | Hypoechoic | Hypoechoic | Presence of halo and mosaic signs |
| CEUS | Arterial phase: hyper-enhanced Portal/late phase: hypo-enhanced | Arterial phase: hyper-enhanced Portal/late phase: hypo-enhanced | Arterial phase: hyper-enhanced Portal/late phase: hypo-enhanced |
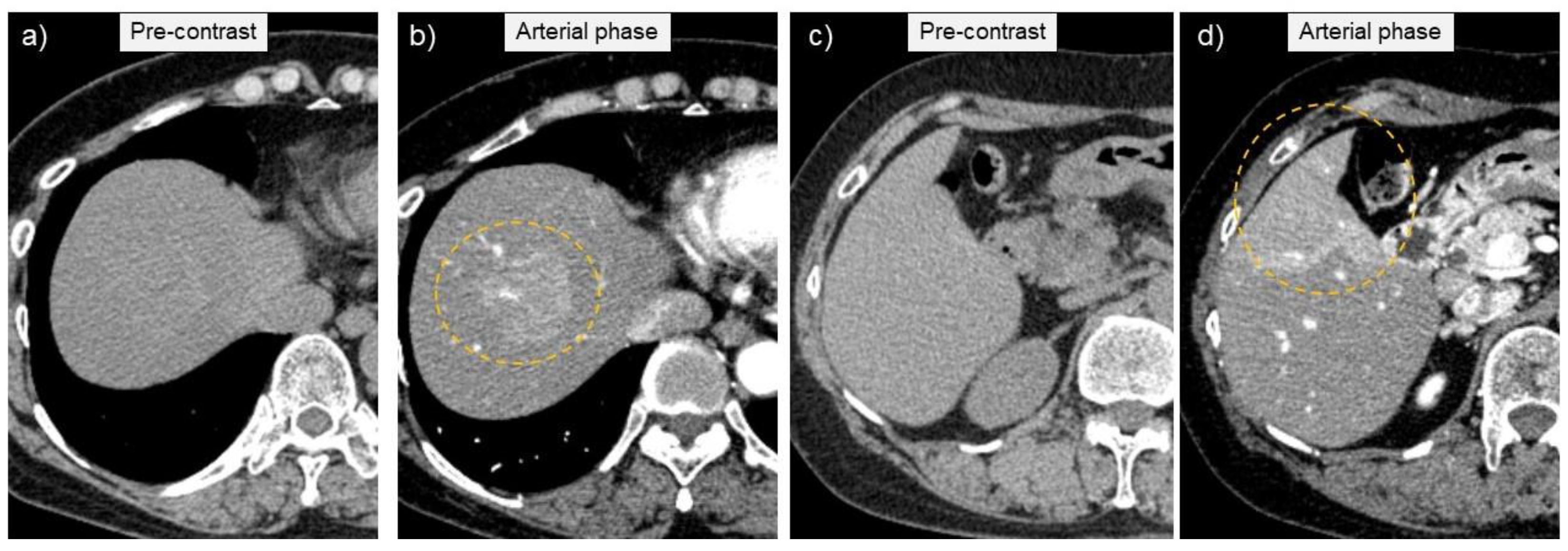
| CT | Low and iso-density | Low and iso-density | Low/iso-/high density |
| Dynamic CT | Ring enhancement pattern | Enhanced/ring enhancement pattern/not enhanced | Enhanced and washout |
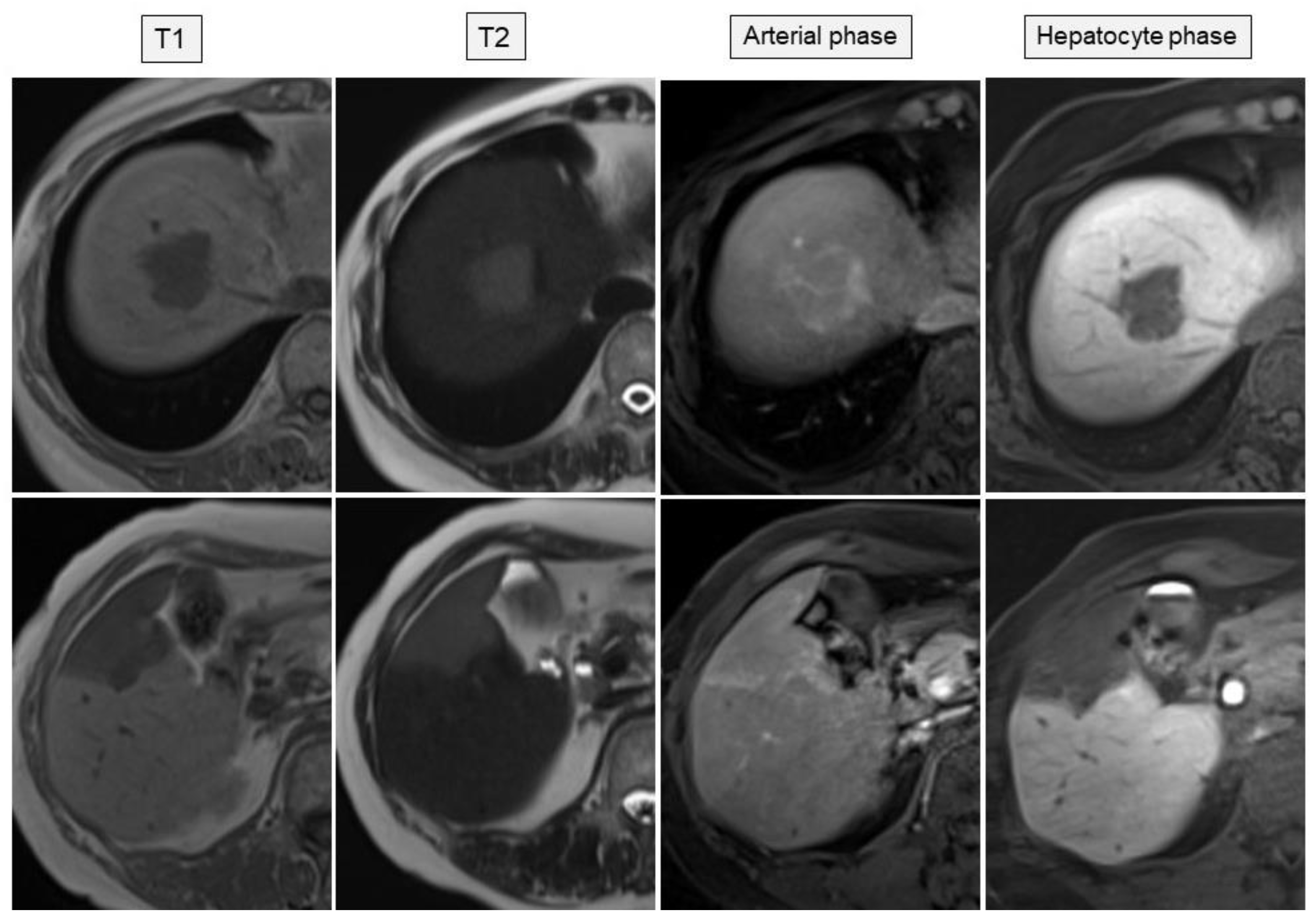
| MRI | T1-weighted: low intensity, T2-weighted: high intensity | T1-weighted: low intensity, T2-weighted: high intensity | T2-weighted: high intensity |
| Gd-EOB-MRI | Enhanced in arterial phase, low intensity in hepatocyte phase | Enhanced in arterial phase, low intensity in hepatocyte phase | Enhanced in arterial phase, low intensity in hepatocyte phase |
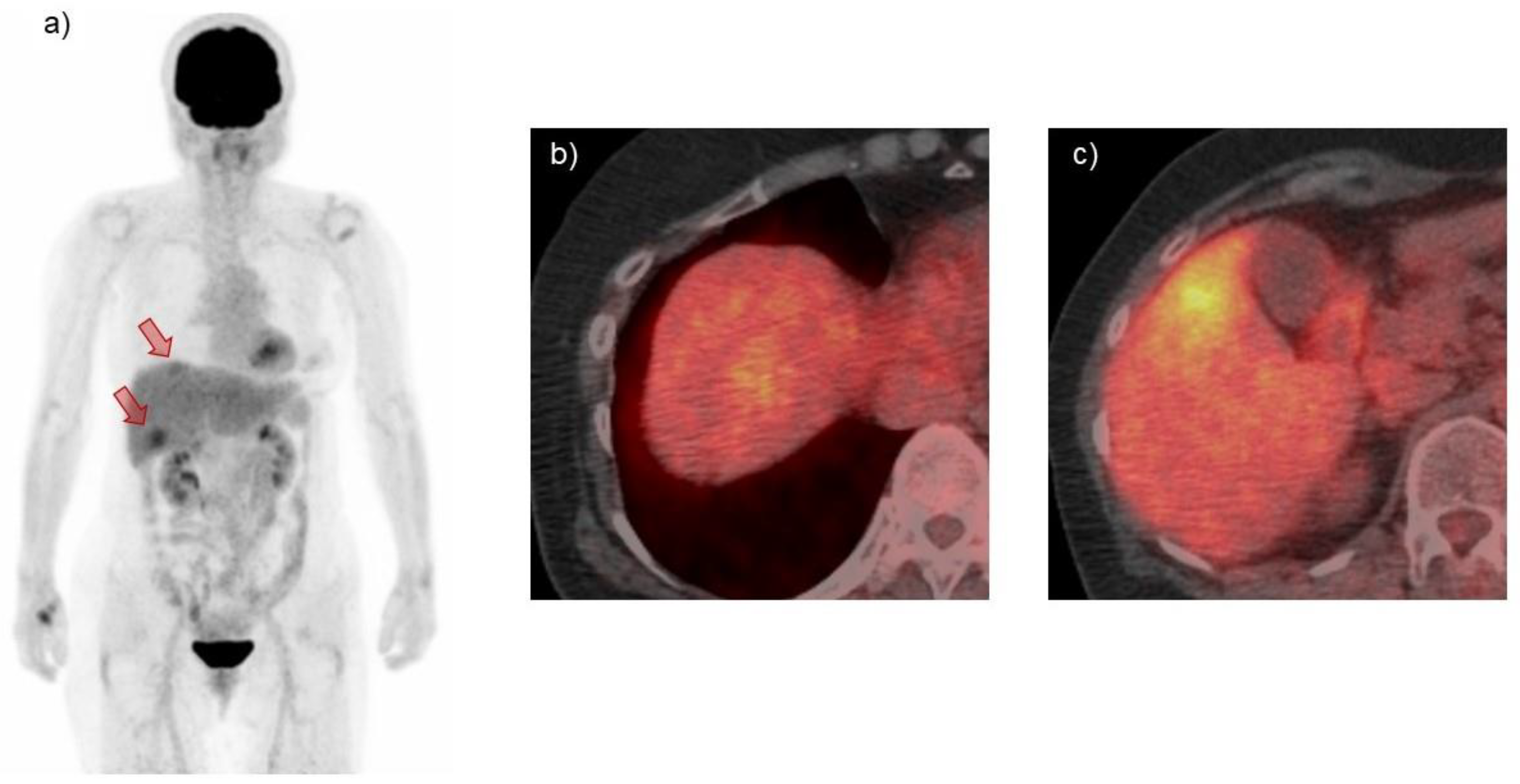
| PET | Abnormal accumulation | Abnormal accumulation | Nearly half of cases have no accumulation |
| Age (Years) | Sex | HBV | Treatment | Follow-Up (Months) | Reference |
|---|---|---|---|---|---|
| 37 | M | CH | R-CHOP | N/A | [15] |
| 73 | M | Carrier | Resection | 6 | [7] |
| 59 | F | CH | Observation | N/A | [14] |
| 52 | F | N/A | R-CVP | 60 | [42] |
| 54 | M | N/A | R-CVP, RT | 36 | [41] |
| 65 | M | N/A | Chemotherapy | 24 | [41] |
| 80 | M | N/A | Chemotherapy | 15 | [41] |
| 57 | F | N/A | Resection, rituximab | 72 | [46] |
| 50 | F | CH | Observation | 32 | [47] |
| 59 | M | CH | Resection | 48 | [13] |
| 53 | M | Carrier | Resection, R-CHOP | N/A | [12] |
| 38 | M | Carrier | Resection, CHOP | 15 | [11] |
| 59 | M | LC | Liver transplantation | 6 | [10] |
| 36 | M | Carrier | Resection, rituximab | 40 | [9] |
| 66 | F | Carrier | NUC, observation | Ongoing | Present case |
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The Non-Hodgkin’s Lymphoma Classification Project. A clinical evaluation of the International Lymphoma Study Group classification of non-Hodgkin’s lymphoma. Blood 1997, 89, 3909–3918. [Google Scholar]
- Ruskoné-Fourmestraux, A.; Fischbach, W.; Aleman, B.M.P.; Boot, H.; Du, M.Q.; Megraud, F.; Montalban, C.; Raderer, M.; Savio, A.; Wotherspoon, A.; et al. EGILS consensus report. Gastric extranodal marginal zone B-cell lymphoma of MALT. Gut 2011, 60, 747–758. [Google Scholar] [CrossRef] [Green Version]
- Aozasa, K. Hashimoto’s thyroiditis as a risk factor of thyroid lymphoma. Acta Pathol. Jpn. 1990, 40, 459–468. [Google Scholar] [CrossRef]
- Zintzaras, E.; Voulgarelis, M.; Moutsopoulos, H.M. The risk of lymphoma development in autoimmune diseases: A meta-analysis. Arch. Intern. Med. 2005, 165, 2337–2344. [Google Scholar] [CrossRef] [Green Version]
- Armand, M.; Besson, C.; Hermine, O.; Davi, F. Hepatitis C virus—Associated marginal zone lymphoma. Best Pract. Res. Clin. Haematol. 2017, 30, 41–49. [Google Scholar] [CrossRef]
- Zucca, E.; Conconi, A.; Pedrinis, E.; Cortelazzo, S.; Motta, T.; Gospodarowicz, M.K.; Patterson, B.J.; Ferreri, A.J.; Ponzoni, M.; Devizzi, L.; et al. Nongastric marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue. Blood 2003, 101, 2489–2495. [Google Scholar] [CrossRef]
- Xie, H.; Lv, J.; Ji, Y.; Du, X.; Yang, X. Primary hepatic mucosa-associated lymphoid tissue lymphoma: A case report and literature review. Medicine 2019, 98, e15034. [Google Scholar] [CrossRef]
- Sagaert, X.; Van Cutsem, E.; De Hertogh, G.; Geboes, K.; Tousseyn, T. Gastric MALT lymphoma: A model of chronic inflammation-induced tumor development. Nat. Rev. Gastroenterol. Hepatol. 2010, 7, 336–346. [Google Scholar] [CrossRef]
- Gockel, H.R.; Heidemann, J.; Lugering, A.; Mesters, R.M.; Parwaresch, R.; Domschke, W.; Lugering, N. Stable remission after administration of rituximab in a patient with primary hepatic marginal zone B-cell lymphoma. Eur. J. Haematol. 2005, 74, 445–447. [Google Scholar] [CrossRef]
- Nart, D.; Ertan, Y.; Yilmaz, F.; Yüce, G.; Zeytunlu, M.; Kilic, M. Primary hepatic marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue type in a liver transplant patient with hepatitis B cirrhosis. Transplant. Proc. 2005, 37, 4408–4412. [Google Scholar] [CrossRef]
- Yu, Y.D.; Kim, D.S.; Byun, G.Y.; Lee, J.H.; Kim, I.S.; Kim, C.Y.; Kim, Y.C.; Suh, S.O. Primary hepatic marginal zone B cell lymphoma: A case report and review of the literature. Indian J. Surg. 2013, 75, 331–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhong, Y.; Wang, X.; Deng, M.; Fang, H.; Xu, R. Primary hepatic mucosa-associated lymphoid tissue lymphoma and hemangioma with chronic hepatitis B virus infection as an underlying condition. Biosci. Trends 2014, 8, 185–188. [Google Scholar] [CrossRef] [Green Version]
- Chan, R.C.; Chu, C.M.; Chow, C.; Chan, S.L.; Chan, A.W. A concurrent primary hepatic MALT lymphoma and hepatocellular carcinoma. Pathology 2015, 47, 178–181. [Google Scholar] [CrossRef]
- Bao, C.; Wei, J.; Zhao, X.; Lin, L.; Chen, D.; Liu, K.; Qian, W.; Anas, J.M.; Zhao, K. Prognostic value of fluorine-18-fluorodeoxyglucose positron emission tomography/computed tomography in primary hepatic mucosa-associated lymphoid tissue lymphoma: A case report and review of the literature. Medicine 2018, 97, e9877. [Google Scholar] [CrossRef]
- Chen, Y.Y.; Chen, Y.F.; Chen, C.H. A long-term follow-up of primary hepatic mucosa-associated lymphoid tissue lymphoma. Dig. Liver Dis. 2020. [Google Scholar] [CrossRef]
- Clarke, G.; MacMathuna, P.; Fenlon, H.; Callagy, G.; O’Keane, J.C.; Carney, D.; Crowe, J. Primary hepatic lymphoma in a man with chronic hepatitis C. Eur. J. Gastroenterol. Hepatol. 1997, 9, 87–90. [Google Scholar] [CrossRef] [PubMed]
- Doi, H.; Horiike, N.; Hiraoka, A.; Koizumi, Y.; Yamamoto, Y.; Hasebe, A.; Ichikawa, S.; Yano, M.; Miyamoto, Y.; Ninomiya, T.; et al. Primary hepatic marginal zone B cell lymphoma of mucosa-associated lymphoid tissue type: Case report and review of the literature. Int. J. Hematol. 2008, 88, 418–423. [Google Scholar] [CrossRef]
- Hamada, T.; Kakizaki, S.; Koiso, H.; Irisawa, H.; Nobusawa, S.; Mori, M. Primary hepatic mucosa-associated lymphoid tissue (MALT) lymphoma. Clin. J. Gastroenterol. 2013, 6, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Takagawa, Y.; Kawabe, N.; Hashimoto, S.; Harata, M.; Murao, M.; Nitta, Y.; Nakano, T.; Shimazaki, H.; Mizuno, Y.; Kan, T.; et al. A case of multiple hepatic MALT lymphoma with cirrhosis related to hepatitis C virus. Kanzo 2014, 55, 274–283. [Google Scholar] [CrossRef] [Green Version]
- Rossotti, R.; Travi, G.; Pazzi, A.; Baiguera, C.; Morra, E.; Puoti, M. Rapid clearance of HCV-related splenic marginal zone lymphoma under an interferon-free, NS3/NS4A inhibitor-based treatment. A case report. J. Hepatol. 2015, 62, 234–237. [Google Scholar] [CrossRef]
- Gherlan, G.S.; Stoia, R.; Enyedi, M.; Dobrea, C.; Calistru, P.I. Primary Hepatic Marginal Zone Lymphoma in a Patient with Chronic Hepatitis C. Maedica 2016, 11, 250–254. [Google Scholar]
- De Luca, M.L.; Lombardi, L.; Tartaglia, G.; Fazio, F.; Di Prima, A.; Serrao, A.; Canichella, M.; Pulsoni, A. Response to Interferon-Free Direct Antivirals (DAAS) Treatment in Hcv-Related Subcutaneous Marginal Zone B-Cell Lymphoma with Lipoma-Like Presentation: Report of Two Cases. Mediterr. J. Hematol. Infect. Dis. 2019, 11, e2019053. [Google Scholar] [CrossRef] [Green Version]
- Yasuda, T.; Nakagawa, S.; Imai, K.; Okabe, H.; Hayashi, H.; Yamashita, Y.I.; Chikamoto, A.; Ozono, K.; Mikami, Y.; Baba, H. A case of primary hepatic mucosa-associated lymphoid tissue lymphoma incidentally found in the sustained virological response state of chronic hepatitis C: Review of the literature of this rare disease. Int. Cancer Conf. J. 2020, 9, 59–65. [Google Scholar] [CrossRef]
- Bohlok, A.; De Grez, T.; Bouazza, F.; De Wind, R.; El-Khoury, M.; Repullo, D.; Donckier, V. Primary Hepatic Lymphoma Mimicking a Hepatocellular Carcinoma in a Cirrhotic Patient: Case Report and Systematic Review of the Literature. Case Rep. Surg. 2018, 2018, 9183717. [Google Scholar] [CrossRef] [Green Version]
- Haefliger, S.; Milowich, D.; Sciarra, A.; Trimeche, M.; Bouilly, J.; Kaiser, J.; Volpi, S.; Brouland, J.P.; Sempoux, C.; de Leval, L. Primary hepatic marginal B cell lymphoma of mucosa-associated lymphoid tissue (MALT) and non-alcoholic steatohepatitis (NASH): More than a coincidence? Ann. Hematol. 2019, 98, 1513–1516. [Google Scholar] [CrossRef]
- Prabhu, R.M.; Medeiros, L.J.; Kumar, D.; Drachenberg, C.I.; Papadimitriou, J.C.; Appelman, H.D.; Johnson, L.B.; Laurin, J.; Heyman, M.; Abruzzo, L.V. Primary hepatic low-grade B-cell lymphoma of mucosa-associated lymphoid tissue (MALT) associated with primary biliary cirrhosis. Mod. Pathol. 1998, 11, 404–410. [Google Scholar]
- Nakayama, S.; Yokote, T.; Kobayashi, K.; Hirata, Y.; Akioka, T.; Miyoshi, T.; Oka, S.; Hiraoka, N.; Iwaki, K.; Takayama, A.; et al. Primary hepatic MALT lymphoma associated with primary biliary cirrhosis. Leuk. Res. 2010, 34, e17–e20. [Google Scholar] [CrossRef]
- Obiorah, I.E.; Johnson, L.; Ozdemirli, M. Primary mucosa-associated lymphoid tissue lymphoma of the liver: A report of two cases and review of the literature. World J. Hepatol. 2017, 9, 155–160. [Google Scholar] [CrossRef]
- Liu, J.; Guo, R.R.; Fang, J.C.; Zhong, L. Primary hepatic mucosa-associated lymphoid tissue lymphoma with hepatocellular carcinoma: A case report and literature review. J. Dig. Dis. 2020. [Google Scholar] [CrossRef]
- Carbone, P.P.; Kaplan, H.S.; Musshoff, K.; Smithers, D.W.; Tubiana, M. Report of the Committee on Hodgkin’s Disease Staging Classification. Cancer Res. 1971, 31, 1860–1861. [Google Scholar]
- Dong, S.; Chen, L.; Chen, Y.; Chen, X. Primary hepatic extranodal marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue type: A case report and literature review. Medicine 2017, 96, e6305. [Google Scholar] [CrossRef]
- Shiozawa, K.; Watanabe, M.; Ikehara, T.; Matsukiyo, Y.; Kikuchi, Y.; Kaneko, H.; Okubo, Y.; Shibuya, K.; Igarashi, Y.; Sumino, Y. A case of contiguous primary hepatic marginal zone B-cell lymphoma and hemangioma ultimately diagnosed using contrast-enhanced ultrasonography. Case Rep. Oncol. 2015, 8, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Foschi, F.G.; Dall’Aglio, A.C.; Marano, G.; Lanzi, A.; Savini, P.; Piscaglia, F.; Serra, C.; Cursaro, C.; Bernardi, M.; Andreone, P.; et al. Role of contrast-enhanced ultrasonography in primary hepatic lymphoma. J. Ultrasound. Med. 2010, 29, 1353–1356. [Google Scholar] [CrossRef]
- Rajesh, S.; Bansal, K.; Sureka, B.; Patidar, Y.; Bihari, C.; Arora, A. The imaging conundrum of hepatic lymphoma revisited. Insights Imaging 2015, 6, 679–692. [Google Scholar] [CrossRef] [Green Version]
- Kitahata, S.; Hiraoka, A.; Kudo, M.; Murakami, T.; Ochi, M.; Izumoto, H.; Ueki, H.; Kaneto, M.; Aibiki, T.; Okudaira, T.; et al. Abdominal Ultrasound Findings of Tumor-Forming Hepatic Malignant Lymphoma. Dig. Dis. 2017, 35, 498–505. [Google Scholar] [CrossRef]
- Yukisawa, S.; Ohto, M.; Masuya, Y.; Okabe, S.; Fukuda, H.; Yoshikawa, M.; Ebara, M.; Saisho, H.; Ohtsuka, M.; Miyazaki, M.; et al. Contrast-enhanced three-dimensional fusion sonography of small liver metastases with pathologic correlation. J. Clin. Ultrasound. 2007, 35, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Joshita, S.; Ichijo, T.; Suzuki, F.; Yokoyama, T.; Sugiyama, Y.; Fukushima, M.; Kamijo, A.; Komatsu, M.; Umemura, T.; Yoshizawa, K.; et al. A case of well-differentiated cholangiolocellular carcinoma visualized with contrast-enhanced ultrasonography using Sonazoid. Hepatol. Res. Off. J. Jpn. Soc. Hepatol. 2009, 39, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Guidoboni, M.; Ferreri, A.J.; Ponzoni, M.; Doglioni, C.; Dolcetti, R. Infectious agents in mucosa-associated lymphoid tissue-type lymphomas: Pathogenic role and therapeutic perspectives. Clin. Lymphoma Myeloma 2006, 6, 289–300. [Google Scholar] [CrossRef] [PubMed]
- Lai, M.; Hyatt, B.J.; Nasser, I.; Curry, M.; Afdhal, N.H. The clinical significance of persistently normal ALT in chronic hepatitis B infection. J. Hepatol. 2007, 47, 760–767. [Google Scholar] [CrossRef] [PubMed]
- Raderer, M.; Kiesewetter, B. How I treat MALT lymphoma: ‘A subjective interpretation of the gospel according to Isaacson…’. ESMO Open 2020, 5. [Google Scholar] [CrossRef]
- Albano, D.; Giubbini, R.; Bertagna, F. 18F-FDG PET/CT and primary hepatic MALT: A case series. Abdom. Radiol. 2016, 41, 1956–1959. [Google Scholar] [CrossRef]
- Dong, A.; Xiao, Z.; Yang, J.; Zuo, C. CT, MRI, and 18F-FDG PET/CT Findings in Untreated Pulmonary and Hepatic B-Cell Lymphoma of Mucosa-Associated Lymphoid Tissue (MALT) Over a Five-Year Period: A Case Report. Medicine 2016, 95, e3197. [Google Scholar] [CrossRef]
- Marrero, J.A.; Kulik, L.M.; Sirlin, C.B.; Zhu, A.X.; Finn, R.S.; Abecassis, M.M.; Roberts, L.R.; Heimbach, J.K. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2018, 68, 723–750. [Google Scholar] [CrossRef] [Green Version]
- Schellhaas, B.; Wildner, D.; Pfeifer, L.; Goertz, R.S.; Hagel, A.; Neurath, M.F.; Strobel, D. LI-RADS-CEUS—Proposal for a Contrast-Enhanced Ultrasound Algorithm for the Diagnosis of Hepatocellular Carcinoma in High-Risk Populations. Ultraschall Med. 2016, 37, 627–634. [Google Scholar] [CrossRef]
- Khan, M.A.; Combs, C.S.; Brunt, E.M.; Lowe, V.J.; Wolverson, M.K.; Solomon, H.; Collins, B.T.; Di Bisceglie, A.M. Positron emission tomography scanning in the evaluation of hepatocellular carcinoma. J. Hepatol. 2000, 32, 792–797. [Google Scholar] [CrossRef]
- Fujiwara, Y.; Sakamoto, K.; Tokuhisa, Y.; Tokumitsu, Y.; Nakajima, M.; Matsukuma, S.; Matsui, H.; Shindo, Y.; Kanekiyo, S.; Suzuki, N.; et al. Two Cases of Primary Hepatic Mucosa-Associated Lymphoid Tissue(MALT) Lymphoma. Gan Kagaku Ryoho 2016, 43, 1794–1796. [Google Scholar]
- Takata, N.; Terasaki, S.; Iwata, A.; Harada, K. Hepatic mucosa-associated lymphoid tissue lymphoma in a patient with chronic hepatitis B. J. Jpn. Soc. Gastroenterol. 2015, 112, 880–887. [Google Scholar]






| Hematology | Chemistry | Tumor Markers | ||||||
|---|---|---|---|---|---|---|---|---|
| While blood cells | 5503 | /μL | Total protein | 7.5 | g/dL | AFP | 4.5 | ng/mL |
| Neutrophils | 63.5 | % | Albumin | 4.8 | g/dL | PIVKA-II | 17 | mAU/mL |
| Lymphocytes | 28 | % | AST | 20 | U/L | CEA | 1.6 | ng/mL |
| Red blood cells | 447 × 104 | /µL | ALT | 17 | U/L | CA19-9 | 39.3 | U/mL |
| Hemoglobin | 13.9 | g/dL | LDH | 232 | U/L | CA12-5 | 18 | U/mL |
| Platelet count | 24.1 × 104 | /μL | ALP | 172 | U/L | CA15-3 | 12.8 | U/mL |
| <Coagulation> | GGT | 32 | U/L | sIL-2R | 385 | U/mL | ||
| Prothrombin% | 127.3 | % | T-Bil | 0.82 | mg/dL | <Infection markers> | ||
| APTT | 25.4 | s | BUN | 15 | mg/dL | HBs-Ag | 70.6 | IU/mL |
| Cre | 0.76 | mg/dL | HBe-Ag | 0.1 | C.O.I | |||
| Na | 141 | mEq/L | HBe-Ab | 100 | %INH | |||
| K | 4.4 | mEq/L | HBV DNA | 2.6 | Log IU/mL | |||
| CRP | 0.04 | mg/dL | HCV-Ab | (-) |
| Epidemiology | Predominantly in elderly individuals in their 60’s at a similar sex ratio |
| Clinical features | No symptoms, abdominal discomfort, poor appetite, gastrointestinal symptoms, B symptoms (fever, weight loss, and night sweats) |
| Radiological investigation | US, CEUS, CT, MRI, PET-CT |
| Treatment | Surgery, chemotherapy, radiotherapy, combined therapy |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamashita, Y.; Joshita, S.; Kobayashi, H.; Wakabayashi, S.-i.; Sugiura, A.; Yamazaki, T.; Umemura, T. Primary Hepatic Extranodal Marginal Zone Lymphoma of Mucosa-Associated Lymphoid Tissue in a Patient with Chronic Hepatitis B Virus Infection: Case Report and Summary of the Literature. Medicina 2021, 57, 280. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57030280
Yamashita Y, Joshita S, Kobayashi H, Wakabayashi S-i, Sugiura A, Yamazaki T, Umemura T. Primary Hepatic Extranodal Marginal Zone Lymphoma of Mucosa-Associated Lymphoid Tissue in a Patient with Chronic Hepatitis B Virus Infection: Case Report and Summary of the Literature. Medicina. 2021; 57(3):280. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57030280
Chicago/Turabian StyleYamashita, Yuki, Satoru Joshita, Hiroyuki Kobayashi, Shun-ichi Wakabayashi, Ayumi Sugiura, Tomoo Yamazaki, and Takeji Umemura. 2021. "Primary Hepatic Extranodal Marginal Zone Lymphoma of Mucosa-Associated Lymphoid Tissue in a Patient with Chronic Hepatitis B Virus Infection: Case Report and Summary of the Literature" Medicina 57, no. 3: 280. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57030280