
Serum BDNF Levels in Acute Stroke: A Systematic Review and Meta-Analysis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
2.2. Study Endpoints
2.3. Managing the Missing Data
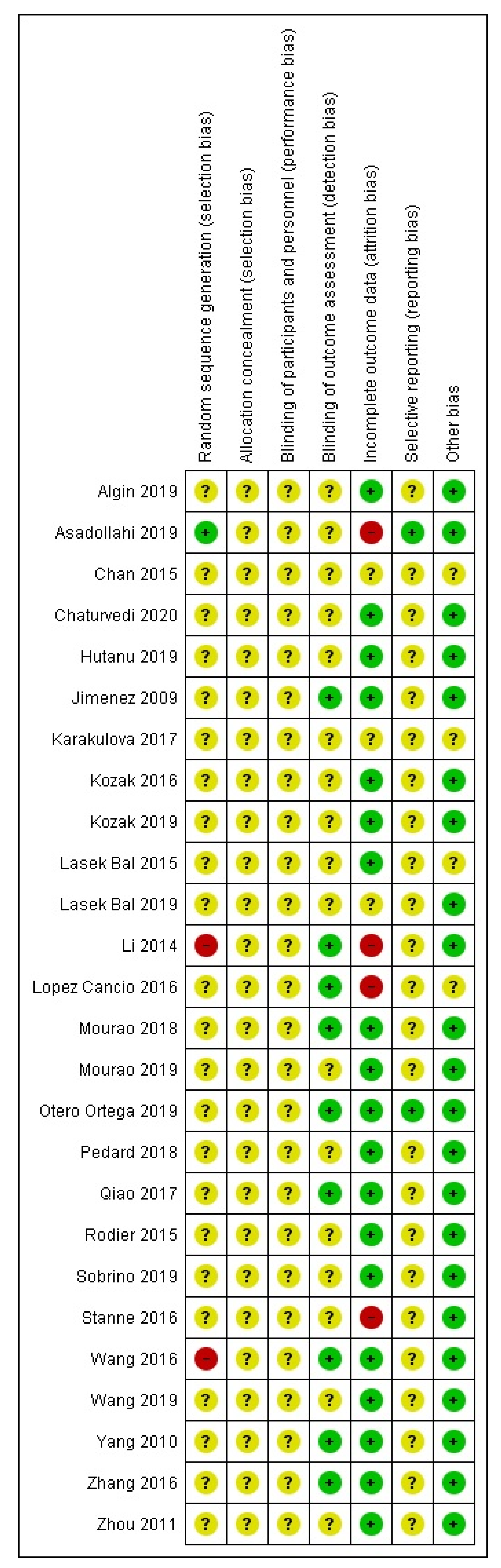
2.4. Risk of Bias Assessment
2.5. Statistical Analysis
3. Results
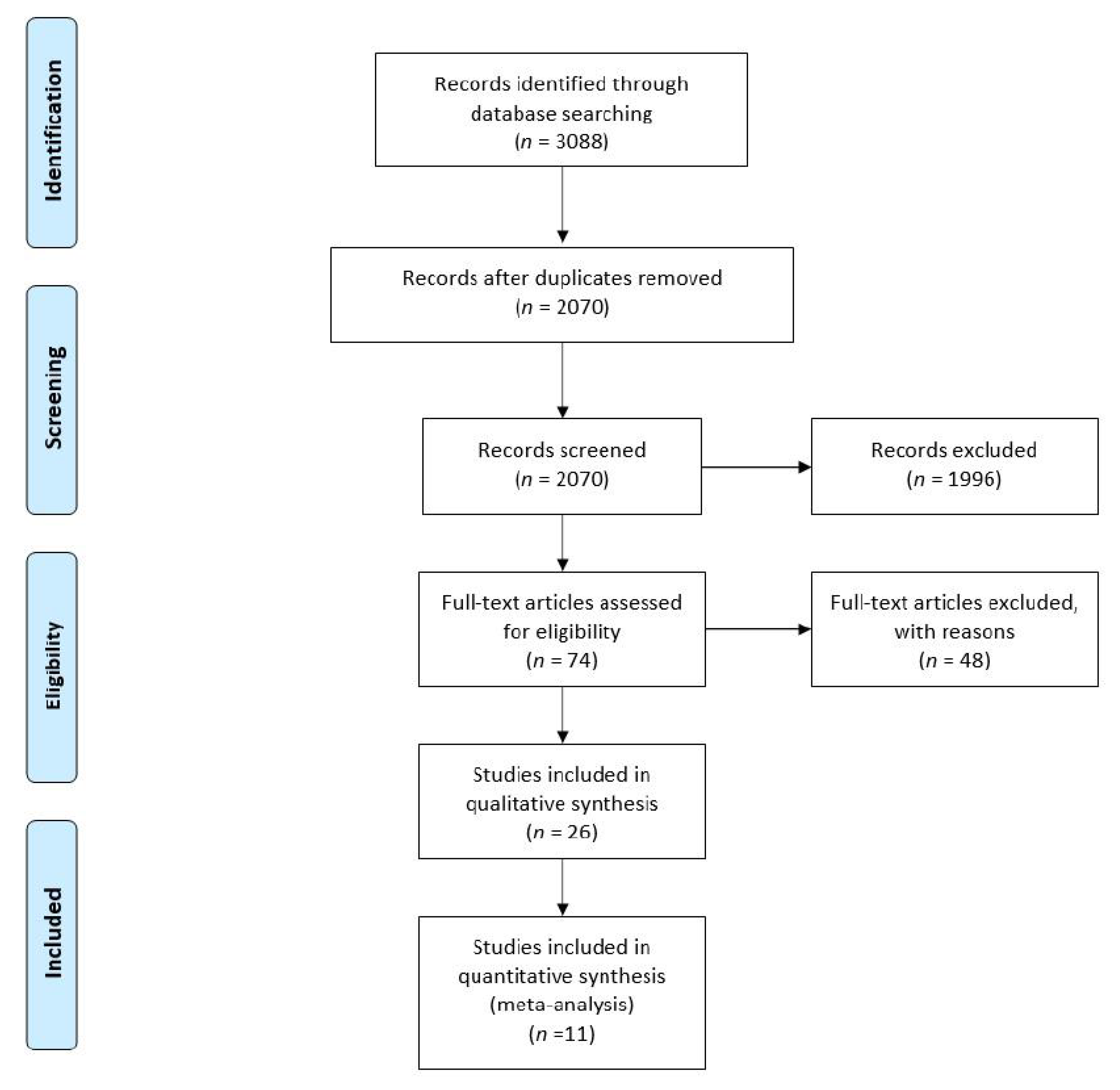
3.1. Study Selection—Quality Assessment
3.2. Functional Outcome at Follow-Up
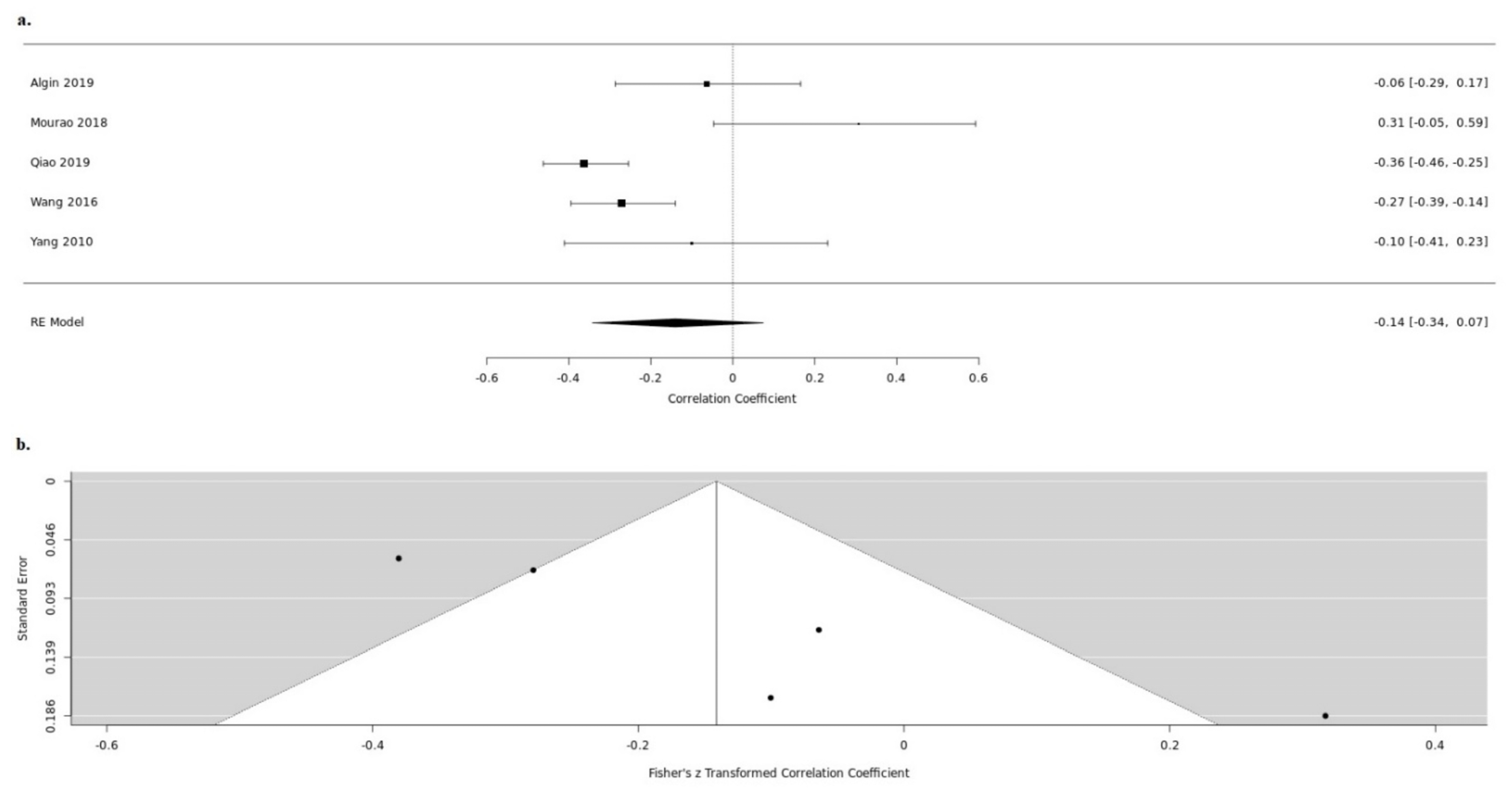
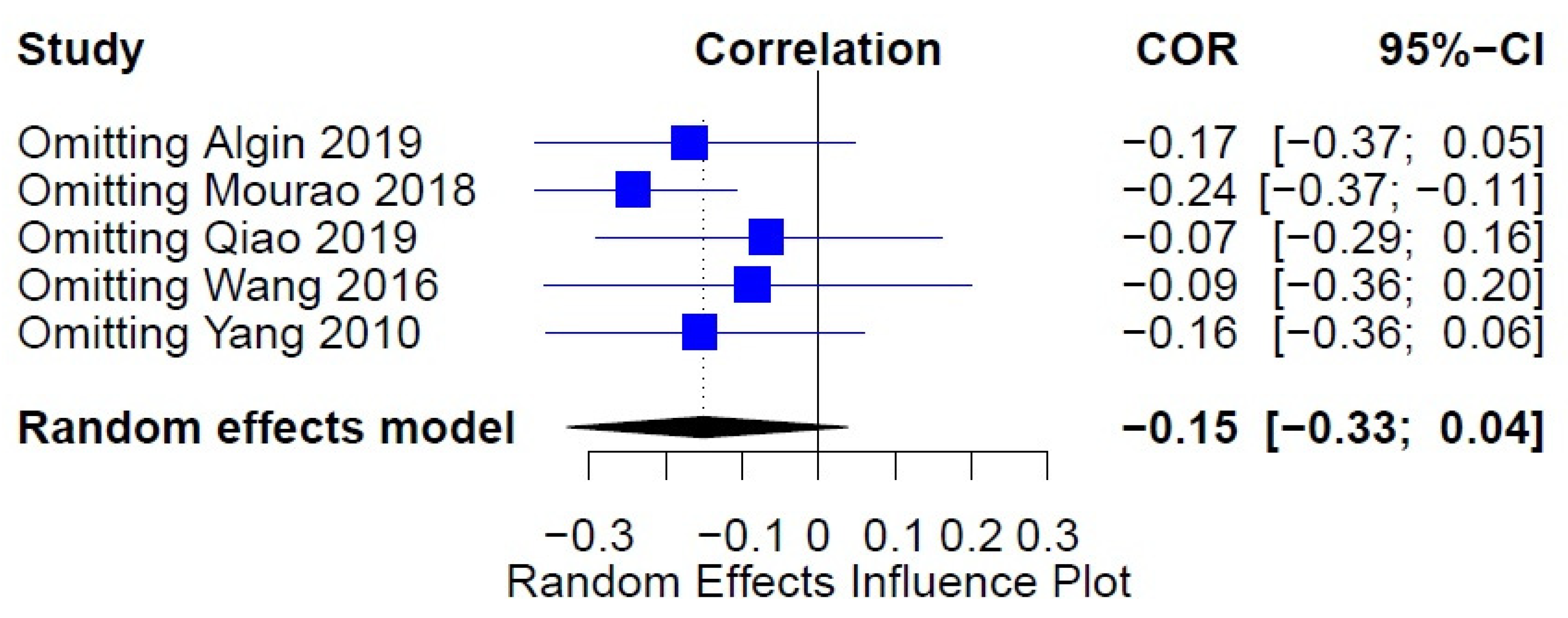
3.3. NIHSS
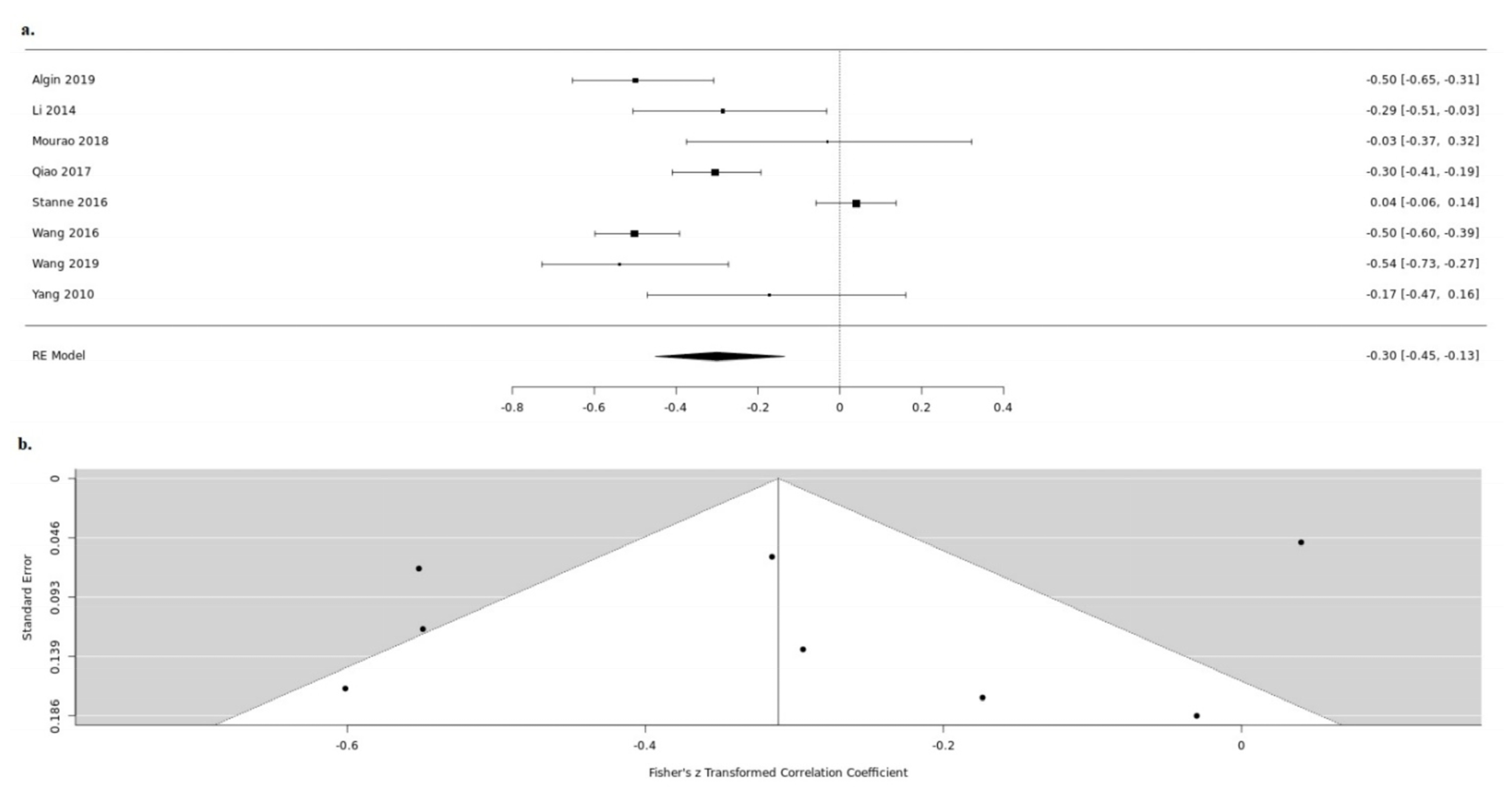
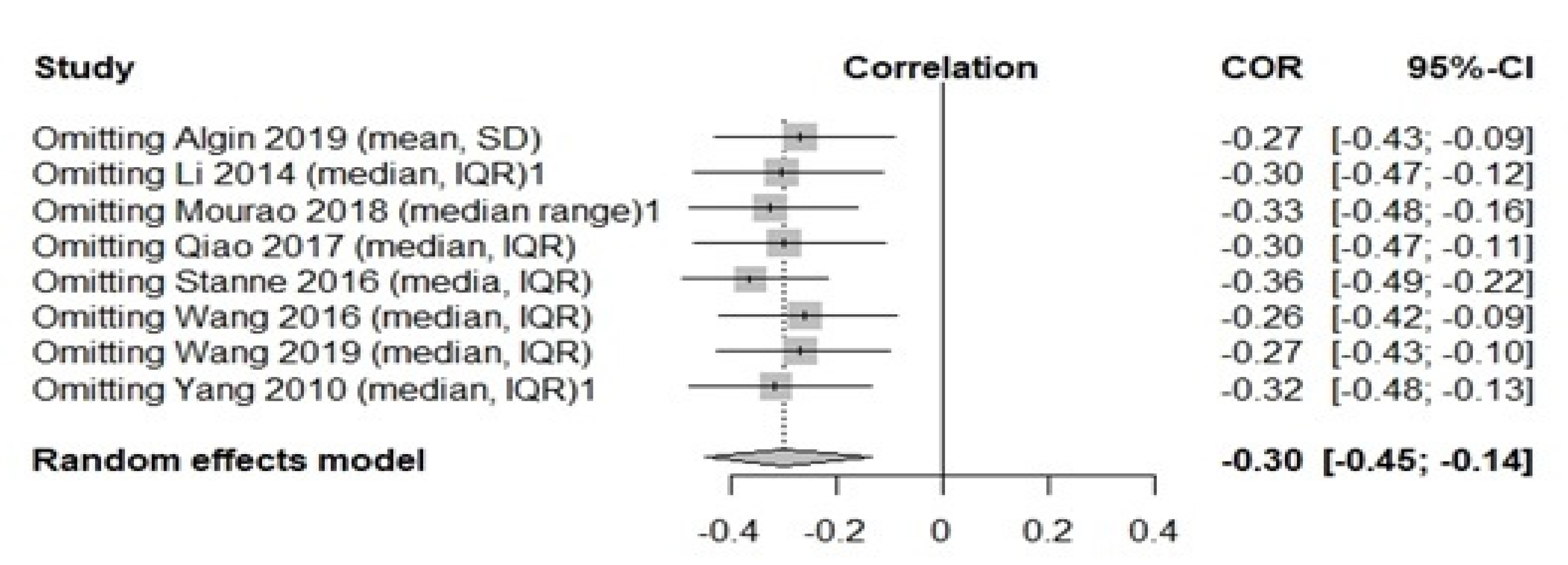
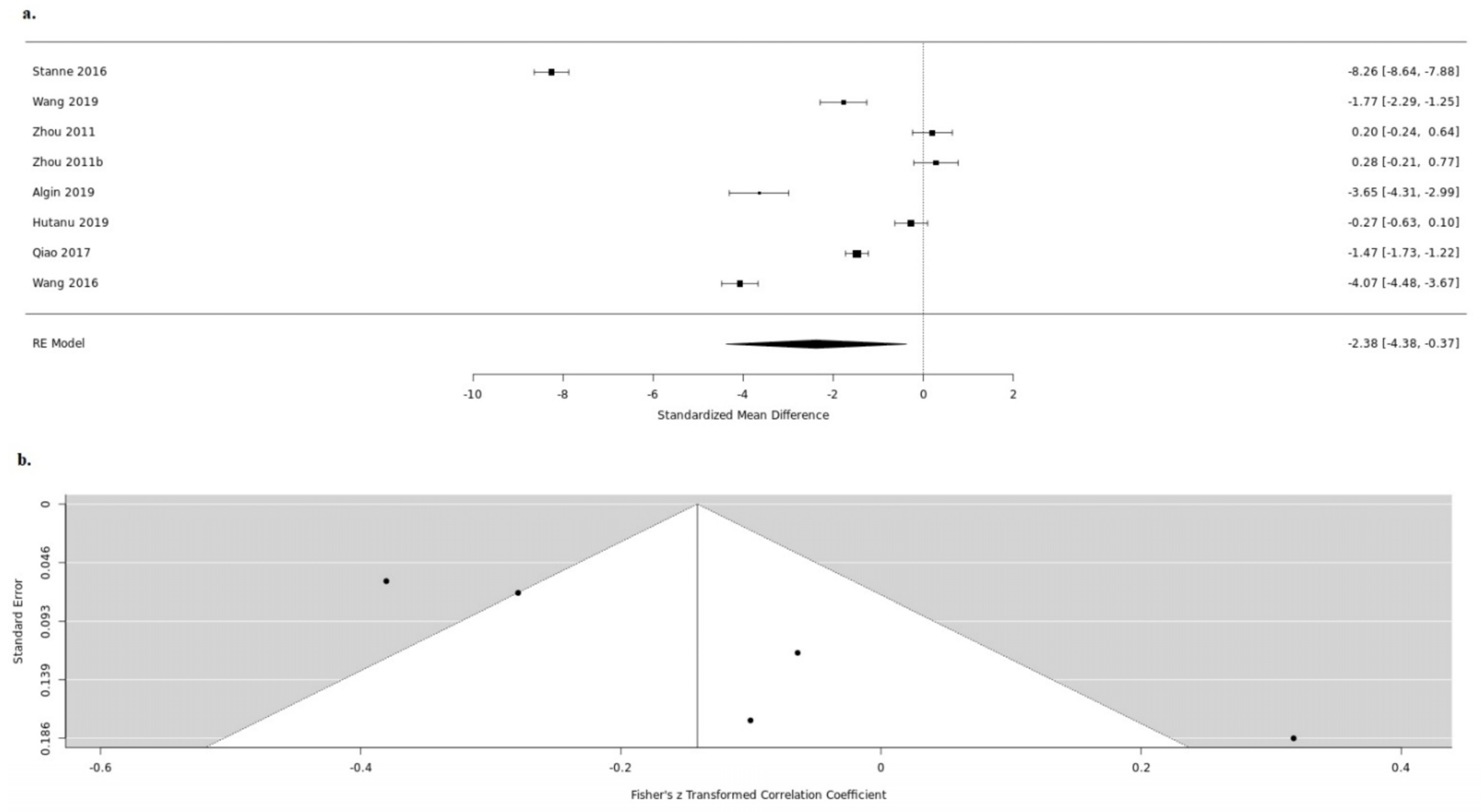
3.4. Infarct Volume
3.5. BDNF in Stroke Patients versus Controls
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. The Top 10 Causes of Death. Global Health Estimates; World Health Organization: Geneva, Switzerland, 2020; Available online: www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 29 December 2020).
- Stroke Alliance for Europe. The Burden of Stroke in Europe; Stroke Alliance for Europe: London, UK, 2017. [Google Scholar]
- Sato, C. Releasing Mechanism of Neurotrophic Factors via Polysialic Acid. Vitam. Horm. 2017, 104, 89–112. [Google Scholar] [PubMed]
- Lu, B.; Pang, P.T.; Woo, N.H. The Yin and Yang of Neurotrophin Action. Nat. Rev. Neurosci. 2005, 6, 603–614. [Google Scholar] [CrossRef] [Green Version]
- Berretta, A.; Tzeng, Y.C.; Clarkson, A.N. Post-stroke recovery: The role of activity-dependent release of brain-derived neurotrophic factor. Expert Rev. Neurother. 2014, 14, 1335–1344. [Google Scholar] [CrossRef] [PubMed]
- Hohlfeld, R. Neurotrophic cross-talk between the nervous and immune systems: Relevance for repair strategies in multiple sclerosis? J. Neurol. Sci. 2008, 265, 93–96. [Google Scholar] [CrossRef] [PubMed]
- Edelmann, E.; Lessmann, V.; Brigadski, T. Pre- and Postsynaptic Twists in BDNF Secretion and Action in Synaptic Plasticity. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/23791959 (accessed on 27 November 2019).
- Panja, D.; Bramham, C.R. BDNF mechanisms in late LTP formation: A synthesis and breakdown. Neuropharmacology 2014, 76, 664–676. [Google Scholar] [CrossRef] [PubMed]
- Polacchini, A.; Metelli, G.; Francavilla, R.; Baj, G.; Florean, M.; Mascaretti, L.G.; Tongiorgi, E. A method for reproducible measurements of serum BDNF: Comparison of the performance of six commercial assays. Sci. Rep. 2015, 5, 17989. [Google Scholar] [CrossRef] [Green Version]
- Lima, G.B.; Doorduin, J.; Klein, H.C.; Dierckx, R.A.J.O.; Bromberg, E.; de Vries, E.F.J. Brain-Derived neurotrophic factor in brain disorders: Focus on neuroinflammation. Mol. Neurobiol. 2019, 56, 3295–3312. [Google Scholar] [CrossRef] [Green Version]
- Golden, E.; Emiliano, A.; Maudsley, S.; Windham, B.G.; Carlson, O.D.; Egan, J.M. Circulating brain-derived neurotrophic factor and indices of metabolic and cardiovascular health: Data from the baltimore longitudinal study of aging. PLoS ONE 2010, 5, e10099. [Google Scholar] [CrossRef] [PubMed]
- Pikula, A.; Beiser, A.S.; Chen, T.C.; Preis, S.R.; Vorgias, D.; Decarli, C. Serum brain-derived neurotrophic factor and vascular endothelial growth factor levels are associated with risk of stroke and vascular brain injury framingham study. Stroke 2013, 44, 2768–2775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiao, H.J.; Li, Z.Z.; Wang, L.M.; Sun, W.; Yu, J.C.; Wang, B. Association of lower serum Brain-derived neurotrophic factor levels with larger infarct volumes in acute ischemic stroke. J. Neuroimmunol. 2017, 307, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Stanne, T.M.; Aberg, N.D.; Nilsson, S.; Jood, K.; Blomstrand, C.; Andreasson, U. Low circulating acute brain-derived neurotrophic factor levels are associated with poor long-term functional outcome after ischemic stroke. Stroke 2016, 47, 1943–1945. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA statement. The PRISMA Group. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews; The Cochrane Collaboration, 2008. [Google Scholar] [CrossRef]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asadollahi, M.; Nikdokht, P.; Hatef, B.; Sadr, S.S.; Sahraei, H.; Assarzadegan, F. Protective properties of the aqueous extract of saffron (Crocus sativus L.) in ischemic stroke, randomized clinical trial. J. Ethnopharmacol. 2019, 238, 111833. [Google Scholar] [CrossRef]
- Jiménez, I.; Sobrino, T.; Rodríguez-Yáñez, M.; Pouso, M.; Cristobo, I.; Sabucedo, M. High serum levels of leptin are associated with post-stroke depression. Psychol. Med. 2009, 39, 1201. [Google Scholar] [CrossRef] [PubMed]
- Karakulova, Y.V.; Selyanina, N.V.; Zhelnin, A.V.; Filimonova, T.A.; Tsepilov, S.V. Effects of Antioxidant Treatment on Neurotrophins and Rehabilitation Processes Following Stroke. Neurosci. Behav. Physiol. 2017, 48, 54–57. [Google Scholar] [CrossRef]
- Lasek-Bal, A.; Jedrzejowska-Szypulka, H.; Student, S.; Warsz-Wianecka, A.; Zareba, K.; Puz, P. The importance of selected markers of inflammation and blood-brain barrier damage for short-term ischemic stroke prognosis. J. Physiol. Pharmacol. 2019, 70, 209–217. [Google Scholar]
- Li, J.; Zhao, Y.D.; Zeng, J.W.; Chen, X.Y.; Wang, R.D.; Cheng, S.Y. Serum Brain-derived neurotrophic factor levels in post-stroke depression. J. Affect. Disord. 2014, 168, 373–379. [Google Scholar] [CrossRef] [PubMed]
- López-Cancio, E.; Ricciardi, A.C.; Sobrino, T.; Cortés, J.; de la Ossa, N.P.; Millán, M. Reported prestroke physical activity is associated with vascular endothelial growth factor expression and good outcomes after stroke. J. Stroke Cerebrovasc. Dis. 2017, 26, 425–430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Z.; Lu, T.; Xu, G.; Yue, X.; Zhu, W.; Ma, M. Decreased serum brain-derived neurotrophic factor (BDNF) is associated with post-stroke depression but not with BDNF gene Val66Met polymorphism. Clin. Chem. Lab. Med. 2011, 49, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Mourão, A.M.; Vicente, L.C.C.; Abreu, M.N.S.; Sant’anna, R.V.D.E.; Meira, F.C.A.; Xavier, R.M. Clinical and molecular correlates of the ASPECTS in the acute phase of stroke. Arq. Neuropsiquiatr 2020, 78, 262–268. Available online: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0004-282X2020000500262&lng=en&nrm=iso&tlng=en (accessed on 27 June 2020). [CrossRef]
- Chaturvedi, P.; Singh, A.; Tiwari, V.; Thacker, A. Diabetes mellitus type 2 impedes functional recovery, neuroplasticity and quality of life after stroke. J. Fam. Med. Prim. Care 2020, 9, 1035. Available online: https://pubmed.ncbi.nlm.nih.gov/32318463/ (accessed on 27 June 2020). [CrossRef]
- Algin, A.; Erdogan, M.O.; Aydin, I.; Poyraz, M.K.; Sirik, M. Clinical usefulness of brain-derived neurotrophic factor and visinin-like protein-1 in early diagnostic tests for acute stroke. Am. J. Emerg. Med. 2019, 37, 2501–2504. [Google Scholar] [CrossRef]
- Chan, A.; Yan, J.; Csurhes, P.; Greer, J.; McCombe, P. Circulating brain derived neurotrophic factor (BDNF) and frequency of BDNF positive T cells in peripheral blood in human ischemic stroke: Effect on outcome. J. Neuroimmunol. 2015, 286, 42–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hutanu, A.; Mihaela, I.; Smaranda, M.; Rodica, B.M.D. Plasma biomarkers as potential predictors of functional dependence in daily life activities after ischemic stroke: A single center study. Ann. Indian Acad. Neurol. 2019, 23, 496–503. [Google Scholar] [PubMed]
- Lasek-Bal, A.; Jędrzejowska-Szypułka, H.; Różycka, J.; Bal, W.; Holecki, M.; Duława, J. Low concentration of BDNF in the acute phase of ischemic stroke as a factor in poor prognosis in terms of functional status of patients. Med. Sci. Monit. 2015, 31, 3900–3905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mourão, A.M.; Vicente, L.C.C.; Abreu, M.N.S.; Vale Sant’Anna, R.; Vieira, E.L.M.; de Souza, L.C. Plasma levels of brain-derived neurotrophic factor are associated with prognosis in the acute phase of ischemic stroke. J. Stroke Cerebrovasc. Dis. 2019, 28, 735–740. [Google Scholar] [CrossRef]
- Otero-Ortega, L.; Gutiérrez-Fernández, M.; Gutiérrez-Zúñiga., R.; Madero-Jarabo, R.; Alonso de Leciñana, M.; Laso-García, F. The effect of post-stroke hyperglycaemia on the levels of brain damage and repair-related circulating biomarkers: The Glycaemia in Acute Stroke Study II. Eur. J. Neurol. 2019, 26, 1439–1446. [Google Scholar] [CrossRef]
- Pedard, M.; Brenière, C.; Pernet, N.; Vergely, C.; Béjot, Y.; Marie, C. Brain-derived neurotrophic factor in peripheral blood mononuclear cells and stroke outcome. Exp. Biol. Med. 2018, 243, 1207–1211. [Google Scholar] [CrossRef]
- Sobrino, T.; Rodríguez-Yáñez, M.; Campos, F.; Iglesias-Rey, R.; Millán, M.; de la Ossa, N.P. Association of High Serum Levels of Growth Factors with Good Outcome in Ischemic Stroke: A Multicenter Study. Transl. Stroke Res. 2020, 11, 653–663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.; Gao, L.; Yang, Y.L.; Li, Y.Q.; Chang, T.; Man, M.H. Low Serum Levels of Brain-Derived Neurotrophic Factor Were Associated with Poor Short-Term Functional Outcome and Mortality in Acute Ischemic Stroke. Mol. Neurobiol. 2017, 54, 7335–7442. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Zhang, Z.; Sun, D.; Xu, Z.; Yuan, Y.; Zhang, X. Low serum BDNF may indicate the development of PSD in patients with acute ischemic stroke. Int. J. Geriatr. Psychiatry 2011, 26, 495–502. [Google Scholar] [CrossRef]
- Zhang, J.; Mu, X.; Breker, D.A.; Li, Y.; Gao, Z.; Huang, Y. Atorvastatin treatment is associated with increased BDNF level and improved functional recovery after atherothrombotic stroke. Int. J. Neurosci. 2017, 127, 92–97. [Google Scholar] [CrossRef] [PubMed]
- Kozak, H.H.; Uğuz, F.; Kılınç, İ.; Uca, A.U.; Serhat Tokgöz, O.; Akpınar, Z. Delirium in patients with acute ischemic stroke admitted to the non-intensive stroke unit: Incidence and association between clinical features and inflammatory markers. Neurol. Neurochir. Pol. 2017, 51, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Kozak, H.H.; Uuz, F.; Kilinç, I.; Uca, A.U.; Tokgöz, O.S.; Güney, F. A cross-sectional study to assess the association between major depression and inflammatory markers in patients with acute ischemic stroke. Indian J. Psychiatry 2019, 61, 283–289. [Google Scholar] [CrossRef]
- Guan, Y.Z.; Li, J.; Zhang, X.W.; Wu, S.; Du, H.; Cui, L.Y. Effectiveness of repetitive transcranial magnetic stimulation (rTMS) after acute stroke: A one-year longitudinal randomized trial. CNS Neurosci. Ther. 2017, 23, 940–946. [Google Scholar] [CrossRef]
- Rodier, M.; Quirié, A.; Prigent-Tessier, A.; Béjot, Y.; Jacquin, A.; Mossiat, C. Relevance of post-stroke circulating BDNF levels as a prognostic biomarker of stroke outcome. Impact of rt-PA treatment. PLoS ONE 2015, 10, e0140668. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Huang, Q.; Ding, J.; Wang, X. Elevated serum levels of brain-derived neurotrophic factor and miR-124 in acute ischemic stroke patients and the molecular mechanism. 3 Biotech. 2019, 9, 386. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/31656724 (accessed on 23 February 2020). [CrossRef]
- Mamounas, L.A.; Altar, C.A.; Blue, M.E.; Kaplan, D.R.; Tessarollo, L.; Lyons, W.E. BDNF promotes the regenerative sprouting, but not survival, of injured serotonergic axons in the adult rat brain. J. Neurosci. 2000, 20, 771–782. [Google Scholar] [CrossRef]
- MacLellan, C.L.; Keough, M.B.; Granter-Button, S.; Chernenko, G.A.; Butt, S.; Corbett, D. A critical threshold of rehabilitation involving brain-derived neurotrophic factor is required for poststroke recovery. Neurorehabil. Neural Repair 2011, 25, 740–748. [Google Scholar] [CrossRef] [PubMed]
- Caplan, L.R. Caplan’s Stroke: A Clinical Approach, 5th ed.; Cambridge University Press: Cambridge, UK, 2016. [Google Scholar]
- Di Lazzaro, V.; Profice, P.; Pilato, F.; Dileone, M.; Florio, L.; Tonali, P.A. BDNF plasma levels in acute stroke. Neurosci. Lett. 2007, 422, 128–130. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Sample | Type of Stroke | Assay | Time of Blood Collection | No of Patients | NIHSS Baseline | BDNF (ng/mL) | Age (Years) | Outcome Assessment | Time of Follow-Up | Patients Who Received rtPA |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Algin 2019 | Serum | Ischemic stroke | ELISA | Within 4 h after stroke | 75 | 10.88 ± 7.72 | 3.89 ± 2.05 | 73.22 ± 11.57 | NA | No follow-up | NA |
| Asadollahi 2019 | Serum | Ischemic stroke | ELISA | 1st and 4th day after stroke | 19 saffron- treated | 11.35 (9.3–13.3) | 1.81 (1.1–2.5) | 70.16 ± 11.5 | BI | 3 months | None |
| 20 routine care | 11.26 (9.4–13) | 1.99 (1.2–2.7) | 72.25 ± 10 | ||||||||
| Chan 2015 | Serum | Ischemic stroke | ELISA | Day 1, week 1 and 3 | 75 | 3.5 (0–24) | NA | 69 (27–89) | mRS | 6 months | 6 |
| Chaturvedi 2020 | Serum | Any type | ELISA | Admission, week 2, 6th month | 104 diabetic | 9.36 ± 4.17 | 11.08 ± 3.85 | 56.29 ± 11.06 | FIM | 3 months | NA |
| 104 non-diabetic | 8.01 ± 4.14 | 8.77 ± 4.04 | 57.42 ± 10.35 | ||||||||
| Hutanu 2019 | Serum | Ischemic stroke | Xmap | Day 1and 5 | 114 | NA | 4.1 (2.73, 9.24) | 71.7 ± 10.2 | BI, mRS | No follow-up | none |
| Jimenez 2009 | Serum | Ischemic stroke | ELISA | Day 7 ± 2 and 30 ± 7 after stroke | 25 PSD | 3 (1–7) | 13.6 (9.8–20.1) | 76.6 ± 7.8 | BI, mRS | 1 month | NA |
| 109 non-PSD | 2 (1–5) | 12.9 (10.6–16.1) | 69.5 ± 9.6 | ||||||||
| Karakulova 2017 | Serum | Ischemic stroke | ELISA | Days after stroke not mentioned | 25 Cytoflavin | 6.70 ± 0.62 | 0.648 ± 0.095 | 52–74 years old | BI | 2 months | none |
| 27 routine care | 6.32 ± 0.26 | 0.598 ± 0.180 | |||||||||
| Kozak 2016 | Serum | Ischemic stroke | ELISA | On the 1st day of stroke | 11 with delirium | 10.36 ± 5.88 | 0.906 ± 0.654 | 64.63 ± 13.18 | NA | No follow-up | none |
| 49 without delirium | 6.10 ± 3.80 | 1.035 ± 0.761 | 72.91 ± 5.61 | ||||||||
| Kozak 2019 | Serum | Ischemic stroke | ELISA | On the 1st day of stroke | 17 PSD | 6.96 ± 4.75 | 0.751 ± 0.643 | 67.47 ± 11.20 | NA | No follow-up | none |
| 36 non-PSD | 0.729 ± 0.501 | 65.25 ± 13.98 | |||||||||
| Lasek-Bal 2015 | Serum | Ischemic stroke | ELISA | On the 1st day of stroke | 87 | NA | 9.96 ± 5.21 | 71.7 ± 11.8 | mRS | 90 days | none |
| Lasek-Bal 2019 | Serum | Ischemic stroke | ELISA | On the 1st day of stroke | 138 | 3 [1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18] | NA | 73.11 ± 11.48 | mRS | 30days | 53 |
| Li 2014 | Serum | Ischemic stroke | ELISA | On the 1st day of stroke | 59 PSD | 8 (4–14) | 8.1 (5.6–9.4) | 72.8 (11.2) | mRS | 3 months | NA |
| 157 non-PSD | 5 (2–8) | 13.7 (10.4–16.5) | 63.6 (9.1) | ||||||||
| Lopez Cancio 2016 | Serum | Ischemic stroke | ELISA | Day 1, 7 and 3 months | 83 | 17 [12,13,14,15,16,17,18,19,20,21] | 3.3 ± 0.9 | 69.6 ± 10.9 | mRS | 3 months | NA |
| Mourao 2018 | Serum | Ischemic stroke | ELISA | Up to 24 h, 72 h and discharge | 32 (length of stay ≤ 10 days) | 5.6 ± 3.8 | 9.715 ± 2.56 | 65.5 ± 11.7 | mRS | No follow-up | NA |
| 18 (length of stay > 10 days) | 12.4 ± 7.4 | 9.737 ± 2.87 | |||||||||
| Mourao 2019 | Serum | Ischemic stroke | ELISA | Admission | 26 ASPECTS < 10 | 10.5 ± 6.4 | 9.05 ± 2.29 | 67.1 ± 12 | mRS | No follow-up | None |
| 24 ASPECTS ≥ 10 | 5.8 ± 4.9 | 10.45 ± 2.86 | 63.8 ± 11.4 | ||||||||
| Otero Ortega 2019 | Serum | Ischemic stroke | ELISA | At 24–48 h and 72–96 h | 95 Non-PSHG | 5 (3–11) | 12.3 (6.5) | 69.7 (12.5) | mRS | 72–96 h | NA |
| 79 PSHG | 4 (2–8) | 11.6 (6.6) | 72.1 (9.3) | ||||||||
| Pedard 2018 | Serum and PBMC | Ischemic stroke | ELISA | Before fibrinolysis—day 1 and 3 | 25 mRS 0–2 | 7 (4–9) | 30.4 (27.8–34.0) | 76 (65.8–83.5) | mRS | No follow-up | All |
| 15 mRS 3–6 | 8 (5–12) | 31.3 (24.6–34.8) | 81 (70–88) | ||||||||
| Qiao 2017 | Serum | Ischemic stroke | ELISA | On 1st day of stroke | 270 | 7 (4–12) | 22.1 (14.5–27.5) | 65 (56–73) | NA | No follow-up | 58 |
| Rodier 2015 | Serum | Ischemic stroke | ELISA | Day 0, 1, 7 and 90 | 14 non rtPA treated | 11.44 ± 2.25 | NA | 74.71 ± 3.55 | NA | 90 days | 24 |
| 24 rtPA treated | 11.20 ± 1.34 | 69.13 ± 3.01 | |||||||||
| Sobrino 2019 | Serum | Ischemic stroke | ELISA | Admission, 3rd months and 12 months | 351 good outcome | 8 (5, 13) | 66.9 ± 11.6 | mRS | 12 months | 198 | |
| 201 poor outcome | 18 (14, 20) | 69.6 ± 9.4 | |||||||||
| Stanne 2016 | Serum | Ischemic stroke | ELISA | Within 10 days after stroke | 491 | 3 (2, 7) | 15.4 ± 5.9 | 58 (51–63) | mRS | 3months, 2 and 7 years | NA |
| Wang 2016 | Serum | Ischemic stroke | ELISA | On 1st day of admission (until 48 h) | 204 | 6 (3–12) | 13.4 (9.2–16.9) | 64 (55–75) | mRS | 3 months | 41 |
| Wang 2019 | Serum | Ischemic stroke | ELISA | NA | 40 | 10 (5, 15) | 19.14 ± 4.87 | 63 (50–75) | NA | No follow-up | NA |
| Yang 2010 | Serum | Ischemic stroke | ELISA | 24–48 h after stroke | 37 PSD | 7 (4–9.5) | NA | 68.95 ± 9.28 | mBI | 14 days | None |
| 63 non-PSD | 3 (2–4) | 68.43 ± 11.18 | |||||||||
| Zhang 2016 | Serum | Ischemic stroke | ELISA | On the 1st day of stroke | 37 received statin | 7.87 ± 2.26 | 32.95 ± 6.14 | 65.11 ± 10.72 | mRS, BI | 6 weeks | NA |
| 38 not received statin | 8.36 ± 2.93 | 23.06 ± 5.13 | 63.34 ± 9.67 | ||||||||
| Zhou 2011 | Serum | Any type | ELISA | Within 7 days after stroke | 35 PSD | 7 (1, 24) | 29.1 ± 11.4 | 61.7 ± 8.5 | mRS, BI | 6 months | NA |
| 58 non-PSD | 5 (1, 13) | 28.1 ± 9.7 | 63.5 ± 12.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karantali, E.; Kazis, D.; Papavasileiou, V.; Prevezianou, A.; Chatzikonstantinou, S.; Petridis, F.; McKenna, J.; Luca, A.-C.; Trus, C.; Ciobica, A.; et al. Serum BDNF Levels in Acute Stroke: A Systematic Review and Meta-Analysis. Medicina 2021, 57, 297. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57030297
Karantali E, Kazis D, Papavasileiou V, Prevezianou A, Chatzikonstantinou S, Petridis F, McKenna J, Luca A-C, Trus C, Ciobica A, et al. Serum BDNF Levels in Acute Stroke: A Systematic Review and Meta-Analysis. Medicina. 2021; 57(3):297. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57030297
Chicago/Turabian StyleKarantali, Eleni, Dimitrios Kazis, Vasileios Papavasileiou, Angeliki Prevezianou, Symela Chatzikonstantinou, Foivos Petridis, Jack McKenna, Alina-Costina Luca, Constantin Trus, Alin Ciobica, and et al. 2021. "Serum BDNF Levels in Acute Stroke: A Systematic Review and Meta-Analysis" Medicina 57, no. 3: 297. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57030297