
Surgical Treatment in a High-Risk Pulmonary Embolism: Case Report


 ,
, {kind=link}
{kind=link}
Abstract
:1. Introduction
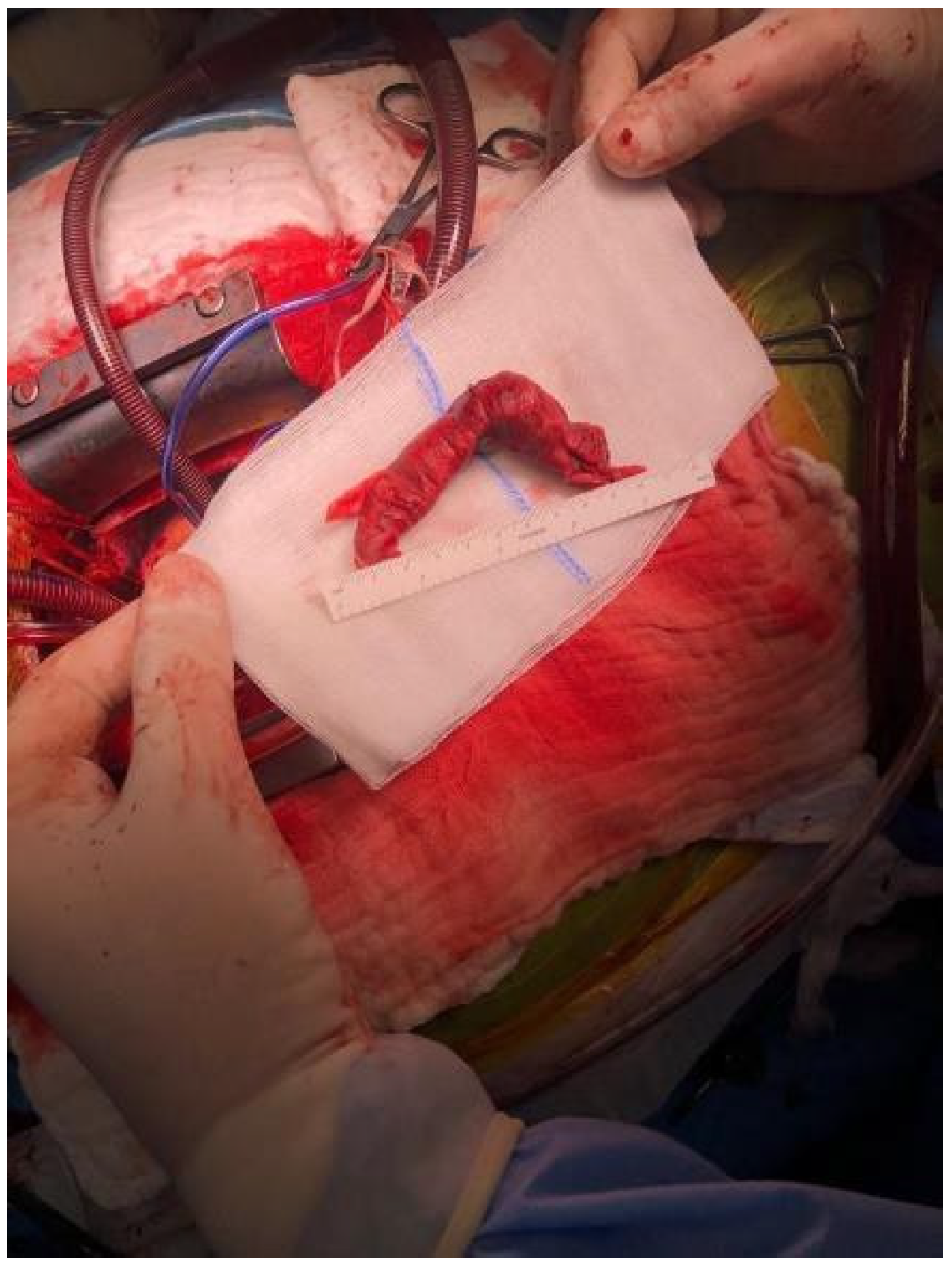
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bĕlohlávek, J.; Dytrych, V.; Linhart, A. Pulmonary embolism, part I: Epidemiology, risk factors and risk stratification, pathophysiology, clinical presentation, diagnosis and nonthrombotic pulmonary embolism. Exp. Clin. Cardiol. 2013, 18, 129–138. [Google Scholar] [PubMed]
- Konstantinides, S.V.; Guy Meyer, G.; Becattini, C.; Bueno, H.; Geersing, G.-J.; Harjola, V.-P.; Huisman, M.V.; Humbert, M.; Jennings, C.S.; Jiménez, D.; et al. ESC Scientific Document Group, 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS): The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC). Eur. Heart J. 2020, 41, 543–603. [Google Scholar]
- Saad, N. Aggressive management of pulmonary embolism. In Seminars in Interventional Radiology; Thieme Medical Publishers: New York, NY, USA, 2012; Volume 29, pp. 52–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamamoto, T. Management of patients with high-risk pulmonary embolism: A narrative review. J. Intensiv. Care 2018, 6, 16. [Google Scholar] [CrossRef] [Green Version]
- Pasrija, C.; Kronfli, A.; Rouse, M.; Raithel, M.; Bittle, G.J.; Pousatis, S.; Ghoreishi, M.; Gammie, J.S.; Griffith, B.P.; Sanchez, P.G.; et al. Outcomes after surgical pulmonary embolectomy for acute submassive and massive pulmonary embolism: A single-center experience. J. Thorac. Cardiovasc. Surg. 2018, 155, 1095–1106.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohteki, H.; Norita, H.; Sakai, M.; Narita, Y. Emergency pulmonary embolectomy with percutaneous cardiopulmonary bypass. Ann. Thorac. Surg. 1997, 63, 1584–1586. [Google Scholar] [CrossRef]
- Brevetti, G.R.; O’Brien, B.; Coomer, C.L.; Hall, T.S.; Brevetti, L.S.; Jablons, D.M. Emergent surgery for massive pulmonary embolism on the basis of clinical diagnosis. Tex. Heart Inst. J. 2003, 30, 149–151. [Google Scholar]
- Ferrari, E.; Imbert, A.; Chevalier, T.; Mihoubi, A.; Morand, P.; Baudouy, M. The ECG in pulmonary embolism: Predictive value of negative T waves in precordial leads-80 case reports. Chest 1997, 111, 537–543. [Google Scholar] [CrossRef]
- Moore, A.J.E.; Wachsmann, J.; Chamarthy, M.R.; Panjikaran, L.; Tanabe, Y.; Rajiah, P. Imaging of acute pulmonary embolism: An update. Cardiovasc. Diagn. Ther. 2018, 8, 225–243. [Google Scholar] [CrossRef]
- Miranda-Bacallado, J.; Izquierdo-Gómez, M.M.; García-Niebla, J.; Jiménez, J.J.; Iribarren, J.L.; Laynez-Cerdeña, I.; Lacalzada-Almeida, J. Role of echocardiography in a patient with suspected acute pulmonary embolism: A case report. J. Med. Case Rep. 2019, 13, 37. [Google Scholar] [CrossRef]
- Molnar, A.; Sacui, D.; Manole, S.; Radulescu, A.; Beyer, R. The value of transthoracic and transesophageal echocardiography for the diagnosis of the native aortic infective endocarditis valve complications: A case report and literature review. Med. Ultrason. 2016, 18, 253–256. [Google Scholar] [CrossRef] [Green Version]
- Moldovan, H.; Popescu, D.; Buliga, T.; Filip, A.; Antoniac, I.; Gheorghita, D.; Molnar, A. Gastric adenocarcinoma associated with acute endocarditis of the aortic valve and coronary artery disease in a 61-yearold male with multiple comorbidities—Combined surgical management—Case report. Medicina 2019, 55, 242. [Google Scholar] [CrossRef] [Green Version]
- Onisai, M.; Dumitru, A.; Iordan, I.; Alius, C.; Teodor, O.; Alexandru, A.; Gheorghita, D.; Antoniac, I.; Nica, A.; Mihailescu, A.A. Synchronous Multiple Breast Cancers-Do We Need to Reshape Staging? Medicina 2020, 56, 230. [Google Scholar] [CrossRef]
- Gradinaru, S.; Stoicea, M.C.; Mocanu, L.; Antoniac, I.; Gheorghita, D.; Grigore, A.G.M. Rare Breast Carcinoma with Paradoxical Plasma Cell Immunoprofile: A Case Report. Medicina 2020, 56, 62. [Google Scholar] [CrossRef] [Green Version]
- Antoniac, I.; Negrusoiu, M.; Mardare, M.; Socoliuc, C.; Zazgyva, A.; Niculescu, M. Adverse local tissue reaction after 2 revision hip replacements for ceramic liner fracture A case report. Medicine 2017, 96, e6687. [Google Scholar] [CrossRef] [PubMed]
- Jurcut, R.; Savu, O.; Popescu, B.A.; Florian, A.; Herlea, V.; Moldovan, H.; Ginghina, C. Primary Cardiac Leiomyosarcoma When Valvular Disease Becomes a Vascular Surgical Emergency. Circulation 2010, 121, E415–E418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rivera-Lebron, B.; McDaniel, M.; Ahrar, K.; Alrifai, A.; Dudzinski, D.M.; Fanola, C.; Blais, D.; Janicke, D.; Melamed, R.; Mohrien, K.; et al. Diagnosis, Treatment and Follow Up of Acute Pulmonary Embolism: Consensus Practice from the PERT Consortium. Clin. Appl. Thromb. 2019, 25, 1076029619853037. [Google Scholar] [CrossRef]
- Duffett, L.; Castellucci, L.A.; Forgie, M.A. Pulmonary embolism: Update on management and controversies. BMJ 2020, 370, m2177. [Google Scholar] [CrossRef] [PubMed]
- Gulba, D.C.; Schmid, C.; Borst, H.G.; Lichtlen, P.; Dietz, R.; Luft, F.C. Medical compared with surgical treatment for massive pulmonary embolism. Lancet 1994, 343, 576–577. [Google Scholar] [CrossRef]
- Azari, A.; Beheshti, A.T.; Moravvej, Z.; Bigdelu, L.; Salehi, M. Surgical embolectomy versus thrombolytic therapy in the management of acute massive pulmonary embolism: Short and long-term prognosis. Heart Lung 2015, 44, 335–339. [Google Scholar] [CrossRef]
- Ucar, E.Y. Update on Thrombolytic Therapy in Acute Pulmonary Thromboembolism. Eurasian J. Med. 2019, 51, 186–190. [Google Scholar] [CrossRef] [PubMed]
- Nasrin, S.; Cader, F.A.; Salahuddin, M.; Nazrin, T.; Shafi, M.J. Pulmonary embolism with floating right atrial thrombus successfully treated with streptokinase: A case report. BMC Res. Notes 2016, 9, 371. [Google Scholar] [CrossRef] [Green Version]
- Todoran, T.M.; Sobieszczyk, P. Catheter-based therapies for massive pulmonary embolism. Prog. Cardiovasc. Dis. 2010, 52, 429–437. [Google Scholar] [CrossRef] [PubMed]
- Loyalka, P.; Ansari, M.Z.; Cheema, F.H.; Miller, C.C., 3rd; Rajagopal, S.; Rajagopal, K. Surgical pulmonary embolectomy and catheter-based therapies for acute pulmonary embolism: A contemporary systematic review. J. Thorac. Cardiovasc. Surg. 2018, 156, 2155–2167. [Google Scholar] [CrossRef] [PubMed]
- Sareyyupoglu, B.; Greason, K.L.; Suri, R.M.; Keegan, M.T.; Dearani, J.A.; Sundt, T.M. A More Aggressive Approach to Emergency Embolectomy for Acute Pulmonary Embolism. Mayo Clin. Proc. 2010, 85, 785–790. [Google Scholar] [CrossRef] [Green Version]
- McFadden, P.M.; Ochsner, J.L. Aggressive Approach to Pulmonary Embolectomy for Massive Acute Pulmonary Embolism: A Historical and Contemporary Perspective. Mayo Clin. Proc. 2010, 85, 782–784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashrafian, H.; Kumar, P.; Athanasiou, T.; Stanbridge, R.D. Minimally invasive off-pump pulmonary embolectomy. Cardiovasc. Surg. 2003, 11, 471–473. [Google Scholar] [CrossRef]
- Kodani, N.; Ohashi, T.; Iida, H.; Kageyama, S.; Furui, M.; Uchino, G. Emergency pulmonary embolectomy using minimally invasive cardiac surgery. Ann. Thorac. Surg. 2016, 101, 1569–1571. [Google Scholar] [CrossRef] [Green Version]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moldovan, H.; Sibisan, A.-M.; Tiganasu, R.; Nechifor, E.; Gheorghita, D.; Zaharia, O.; Albu, M.; Popescu, D.; Molnar, A.; Craciun, M.; et al. Surgical Treatment in a High-Risk Pulmonary Embolism: Case Report. Medicina 2021, 57, 725. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57070725
Moldovan H, Sibisan A-M, Tiganasu R, Nechifor E, Gheorghita D, Zaharia O, Albu M, Popescu D, Molnar A, Craciun M, et al. Surgical Treatment in a High-Risk Pulmonary Embolism: Case Report. Medicina. 2021; 57(7):725. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57070725
Chicago/Turabian StyleMoldovan, Horatiu, Andra-Madalina Sibisan, Robert Tiganasu, Elena Nechifor, Daniela Gheorghita, Ondin Zaharia, Mihai Albu, Daniela Popescu, Adrian Molnar, Mihaela Craciun, and et al. 2021. "Surgical Treatment in a High-Risk Pulmonary Embolism: Case Report" Medicina 57, no. 7: 725. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57070725