
Analysis of the Impact of Comorbidities on Endometrial Lesions Using the Charlson Comorbidity Index in Western Romania

 , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Charlson Comorbidity Index in Endometrial Lesions
- Comorbidities are organized into 16 categories, but six of them cannot be established from the medical documents of the patients (myocardial infarction, COPD, collagenases, leukemia, lymphoma, and AIDS);
- It does not include obesity, hypertension (HT) (but only complications from myocardial infarction, chronic kidney disease, etc.), venous circulation disorders, asthma, and bronchopneumonia, nor locomotor, sensory, and cognitive deficiencies, which is why they have been analyzed separately.
2.3. Statistical Analysis
- Age, based on 5 age categories (0 = under 50, 1 = 50–59, 2 = 60–69, 3 = 70–79, 4 = over 80), where an additional point is assigned for each decade of life for the age over 50, maximum 4 points;
- The existence of myocardial infarction (MI) in the patient’s history, defined or probable, established as a result of an electrocardiogram (EKG) and/or enzymatic changes;
- Congestive heart failure: the existence of nocturnal paroxysmal dyspnea episodes that responded to digitalis, diuretics, etc.;
- Peripheral arterial disease (PAD) manifested by intermittent claudication, history of gangrene or arterial insufficiency, or the presence of an untreated abdominal or thoracic aneurysm (≥6 cm);
- Personal pathological history of stroke/including transient ischemic attack, chronic cognitive deficits, chronic obstructive pulmonary disease (COPD), collagenases, peptic ulcer disease, liver disease (severe—cirrhosis and portal HT with a history of rupture of esophageal varices, moderate—cirrhosis and portal HT without a history of rupture of esophageal varices, mild—chronic hepatitis or cirrhosis without portal HT), DM (without or controlled by diet, complicated or uncomplicated), hemiplegia, chronic kidney disease (moderate—creatinine below 3 mg/dL (0.27 mmol/L) or severe—on dialysis, posttransplant status, uremia), solid tumor (localized or metastatic), leukemia, lymphoma, acquired immunodeficiency syndrome (AIDS).
3. Results
- Between the average age in EC and that in the typical EH, with the main specification that at higher average age, there are malignant lesions, followed by benign ones, at a distance of at least a decade;
- Between the average age in EC and other diagnoses, with the main specification that malignant lesions are present at higher average age, while other diagnoses of benign endometrial diseases are of particular interest to women with average age of at least one decade less;
- Between the average age in atypical EH and that in typical EH with the main specification that at higher average age, there are premalignant lesions due to atypical EH, while other typical EH are of particular interest in women with an average age smaller by at least a decade;
- Between the mean age in typical EH and that in other diagnoses.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- International Agency for Research on Cancer. Available online: https://gco.iarc.fr/today/data/factsheets/populations/642-romania-fact-sheets.pdf (accessed on 27 February 2019).
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer Statistics, 2017. CA Cancer J. Clin. 2017, 67, 7–30. [Google Scholar] [CrossRef] [Green Version]
- World Health Statistics. Available online: https://www.who.int/data/gho/publications/world-health-statistics (accessed on 27 February 2019).
- Kang, S.; Kim, H.S.; Kim, W.; Kim, J.H.; Kang, S.H.; Han, I. Comorbidity is independently associated with poor outcome in extremity soft tissue sarcoma. Clin. Orthop. Surg. 2015, 7, 120–130. [Google Scholar] [CrossRef] [PubMed]
- Creasman, W.T.; Odicino, F.; Maisonneuve, P.; Quinn, M.A.; Beller, U.; Benedet, J.L.; Heintz, A.P.; Ngan, H.Y.; Pecorelli, S. Carcinoma of the corpus uteri. FIGO 26th annual report on the results of treatment in gynecological cancer. Int. J. Gynaecol. Obstet. 2006, 95, 105–143. [Google Scholar] [CrossRef]
- Ouldamer, L.; Duquesne, M.; Arbion, F.; Barillot, I.; Marret, H.; Body, G. The impact of therapeutic management on survival of elderly women with endometrial cancer. Gynecol. Obstet. Fertil. 2012, 40, 759–764. [Google Scholar] [CrossRef]
- Ward, K.K.; Shah, N.R.; Saenz, C.C.; McHale, M.T.; Alvarez, E.A.; Plaxe, S.C. Cardiovascular disease is the leading cause of death among endometrial cancer patients. Gynecol. Oncol. 2012, 126, 176–179. [Google Scholar] [CrossRef]
- Nicholas, Z.; Hu, N.; Ying, J.; Soisson, P.; Dodson, M.; Gaffney, D.K. Impact of comorbid conditions on survival in endometrial cancer. Am. J. Clin. Oncol. 2014, 37, 131–134. [Google Scholar] [CrossRef]
- Ni, J.; Zhu, T.; Zhao, L.; Che, F.; Chen, Y.; Shou, H.; Yu, A. Metabolic syndrome is an independent prognostic factor for endometrial adenocarcinoma. Clin. Transl. Oncol. 2015, 17, 835–839. [Google Scholar] [CrossRef] [PubMed]
- Babes, E.E.; Zaha, D.C.; Tit, D.M.; Nechifor, A.C.; Bungau, S.; Andronie-Cioara, F.L.; Behl, T.; Stoicescu, M.; Munteanu, M.A.; Rus, M.; et al. Value of Hematological and Coagulation Parameters as Prognostic Factors in Acute Coronary Syndromes. Diagnostics 2021, 11, 850. [Google Scholar] [CrossRef] [PubMed]
- Nagle, C.M.; Crosbie, E.J.; Brand, A.; Obermair, A.; Oehler, M.K.; Quinn, M.; Leung, Y.; Spurdle, A.B.; Webb, P.M. Australian National Endometrial Cancer Study Group. The association between diabetes; comorbidities; body mass index and all-cause and cause-specific mortality among women with endometrial cancer. Gynecol. Oncol. 2018, 150, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Kahl, A.; du Bois, A.; Harter, P.; Prader, S.; Schneider, S.; Heitz, F.; Traut, A.; Alesina, P.F.; Meier, B.; Walz, M.; et al. Prognostic value of the age-adjusted Charlson comorbidity index (ACCI) on short- and long-term outcome in patients with advanced primary epithelial ovarian cancer. Ann. Surg. Oncol. 2017, 24, 3692–3699. [Google Scholar] [CrossRef] [PubMed]
- Robbins, J.R.; Gayar, O.H.; Zaki, M.; Mahan, M.; Buekers, T.; Elshaikh, M.A. Impact of age-adjusted Charlson comorbidity score on outcomes for patients with early-stage endometrial cancer. Gynecol. Oncol. 2013, 131, 593–597. [Google Scholar] [CrossRef]
- Suidan, R.S.; Leitao, M.M.; Zivanovic, O.; Gardener, G.J.; Roche, K.C.L.; Levine, D.A.; Jewell, E.L.; Brown, C.L.; Abu-Rustum, N.R.; Charlson, M.E.; et al. Predictive value of the age-adjusted Charlson Comorbidity Index on perioperative complications and survival in patients undergoing primary debulking surgery for advanced epithelial ovarian cancer. Gynecol. Oncol. 2015, 138, 246–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tataru, A.L.; Furau, G.; Afilon, J.; Ionescu, C.; Dimitriu, M.; Bratu, O.G.; Tit, D.M.; Bungau, S.; Furau, C. The Situation of Cervical Cancers in the Context of Female Genital Cancer Clustering and Burden of Disease in Arad County, Romania. J. Clin. Med. 2019, 8, 96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charlson Comorbidity Index. Available online: https://www.mdcalc.com/charlson-comorbidity-index-cci#use-cases (accessed on 27 February 2019).
- Truong, P.T.; Kader, H.A.; Lacy, B.; Lesperance, M.; MacNeil, M.V.; Berthelet, E.; McMurtrie, E.; Alexander, S. The effects of age and comorbidity on treatment and outcomes in women with endometrial cancer. Am. J. Clin. Oncol. 2005, 28, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Vance, S.; Yechieli, R.; Cogan, C.; Hanna, R.; Munkarah, A.; Elshaikh, M.A. The prognostic significance of age in surgically staged patients with Type II endometrial carcinoma. Gynecol. Oncol. 2012, 126, 16–19. [Google Scholar] [CrossRef]
- Tian, W.Y.; Wang, Y.M.; Yan, Y.; Gao, J.P.; Sun, D.D.; Jiang, S.; Sheng, Y.; Teng, F.; Xue, F.X. Clinical application of adult comorbidity evaluation-27 in endometrial cancer. Zhonghua Fu Chan Ke Za Zhi 2016, 51, 810–817. [Google Scholar] [CrossRef] [PubMed]
- Al Feghali, K.A.; Robbins, J.R.; Mahan, M.; Burmeister, C.; Khan, N.T.; Rasool, N.; Munkarah, A.; Elshaikh, M.A. Predictive Capacity of 3 Comorbidity Indices in Estimating Survival Endpoints in Women with Early-Stage Endometrial Carcinoma. Int. J. Gynecol. Cancer 2016, 26, 1455–1460. [Google Scholar] [CrossRef]
- Furau, A.M.; Toma, M.M.; Ionescu, C.; Furau, C.; Bungau, S.; Dimitriu, M.; Tit, D.M.; Furau, G.; Petre, I.; Craina, M. The Correlation of the IETA Ultrasound Score with the Histopathology Results for Women with Abnormal Bleeding in Western Romania. Diagnostics 2021, 11, 1342. [Google Scholar] [CrossRef]
- Joung, K.H.; Jeong, J.W.; Ku, B.J. The association between type 2 diabetes mellitus and women cancer: The epidemiological evidences and putative mechanisms. Biomed. Res. Int. 2015, 2015, 920618. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.F.; Liu, M.D.; Chen, P.; Chen, L.H.; Chang, Y.H.; Wen, P.C.; Li, C.Y. Risks of Breast and Endometrial Cancer in Women with Diabetes: A Population-Based Cohort Study. PLoS ONE 2013, 8, e67420. [Google Scholar] [CrossRef] [Green Version]
- Reeves, G.K.; Pirie, K.; Beral, V.; Green, J.; Spencer, E.; Bull, D. Million Women Study Collaboration. Cancer incidence and mortality in relation to body mass index in the Million Women Study: Cohort study. BMJ 2007, 335, 1134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- von Gruenigen, V.E.; Tian, C.; Frasure, H.; Waggoner, S.; Keys, H.; Barakat, R.R. Treatment effects.; disease recurrence.; and survival in obese women with early endometrial carcinoma: A Gynecologic Oncology Group study. Cancer 2006, 107, 2786–2791. [Google Scholar] [CrossRef] [PubMed]
- Clark, L.H.; Ko, E.M.; Kernodle, A.; Harris, A.; Moore, D.T.; Gehrig, P.A.; Bae-Jump, V. Endometrial Cancer Survivors’ Perceptions of Provider Obesity Counseling and Attempted Behavior Change: Are We Seizing the Moment? Int. J. Gynecol. Cancer 2016, 26, 318–324. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Sen, A.; Vatten, L.J. Hypertension and the risk of endometrial cancer: A systematic review and meta-analysis of case-control and cohort studies. Sci. Rep. 2017, 7, 44808. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dependent Variable: Age | ||||||
|---|---|---|---|---|---|---|
| (I) Group | (J) Group | Difference (Average) (I-J) | SD | Sig. | Less or Equal to | Greater or Equal to |
| EC | Atypical EH | 6.099 | 3.038 | 0.186 | −1.73 | 13.93 |
| Typical EH | 14.277 * | 1.295 | 0.000 | 10.94 | 17.61 | |
| Other | 8.964 * | 1.083 | 0.000 | 6.17 | 11.75 | |
| Atypical EH | EC | −6.099 | 3.038 | 0.186 | −13.93 | 1.73 |
| Typical EH | 8.178 * | 3.059 | 0.039 | 0.30 | 16.06 | |
| Other | 2.865 | 2.976 | 0.771 | −4.80 | 10.53 | |
| Typical EH | EC | −14.277 * | 1.295 | 0.000 | −17.61 | −10.94 |
| Atypical EH | −8.178 * | 3.059 | 0.039 | −16.06 | −0.30 | |
| Other | −5.313 * | 1.142 | 0.000 | −8.25 | −2.37 | |
| Other | EC | −8.964 * | 1.083 | 0.000 | −11.75 | −6.17 |
| Atypical EH | −2.865 | 2.976 | 0.771 | −10.53 | 4.80 | |
| Typical EH | 5.313 * | 1.142 | 0.000 | 2.37 | 8.25 | |
| Diagnosis | Patients | |
|---|---|---|
| Number | % | |
| Diabetes | 133 | 22.39 |
| Obesity | 208 | 35.01 |
| High blood pressure | 370 | 62.28 |
| Dyslipidemia | 46 | 7.74 |
| Hepatitis B or C virus | 15 | 2.52 |
| Veins disorders | 59 | 9.93 |
| Cardiovascular | 110 | 18.51 |
| Renal insufficiency | 4 | 0.67 |
| Asthma, bronchopneumonia | 15 | 2.52 |
| Locomotor, sensory, and cognitive deficits | 30 | 5.05 |
| Comorbidity | Other | EC | Atypical EH | Typical EH | Total | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| No | % | No | % | No | % | No | % | No | % | |
| Uncomplicated diabetes | 41 | 39.42 | 35 | 33.65 | 2 | 1.92 | 26 | 25.00 | 104 | 17.51 |
| Localized solid tumor | 10 | 25.00 | 10 | 25.00 | 0 | 0.00 | 20 | 50.00 | 40 | 6.73 |
| Diabetes mellitus with organ failure | 10 | 34.48 | 14 | 48.28 | 1 | 3.45 | 4 | 13.79 | 29 | 4.88 |
| Congestive heart failure | 11 | 35.48 | 17 | 54.84 | 1 | 3.23 | 2 | 6.45 | 31 | 5.22 |
| Mild liver damage | 14 | 28.00 | 9 | 18.00 | 14 | 28.00 | 13 | 26.00 | 50 | 8.42 |
| Chronic moderate or severe kidney disease | 3 | 30.00 | 6 | 60.00 | 0 | 0.00 | 1 | 10.00 | 10 | 1.68 |
| Moderate to severe liver damage | 4 | 57.14 | 2 | 28.57 | 0 | 0.00 | 1 | 14.29 | 7 | 1.18 |
| Stroke or transient ischemic attack | 3 | 7.50 | 19 | 47.50 | 12 | 30.00 | 6 | 15.00 | 40 | 6.73 |
| Hemiplegia | 0 | 0.00 | 3 | 100.00 | 0 | 0.00 | 0 | 0.00 | 3 | 0.51 |
| Peripheral arterial disease | 1 | 25.00 | 2 | 50.00 | 1 | 25.00 | 0 | 0.00 | 4 | 0.67 |
| Metastatic solid tumor | 2 | 100.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 2 | 0.34 |
| Ulcerative peptic disease | 1 | 25.00 | 2 | 50.00 | 0 | 0.00 | 1 | 25.00 | 4 | 0.67 |
| Dementia | 1 | 11.11 | 4 | 44.44 | 3 | 33.33 | 1 | 11.11 | 9 | 1.52 |
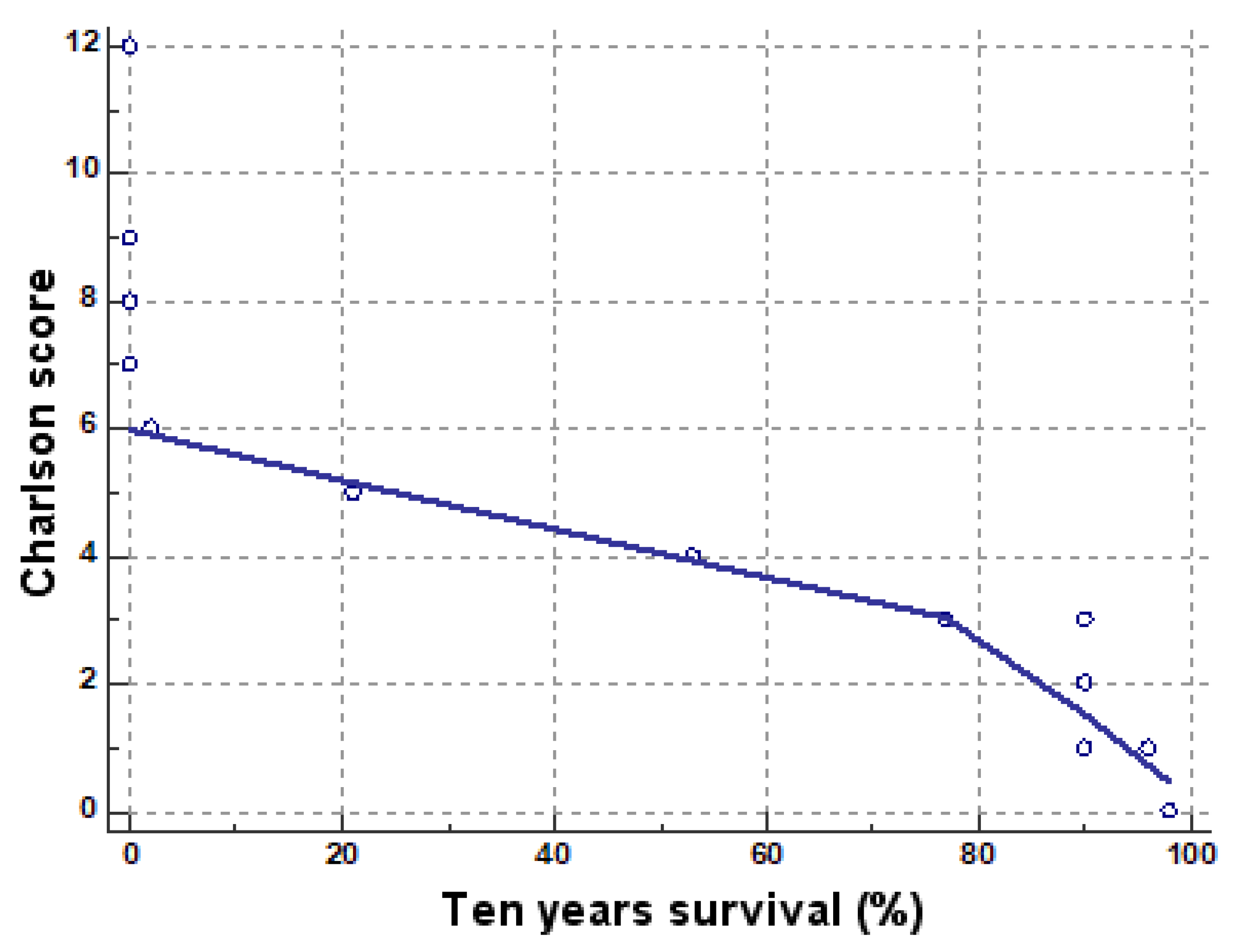
| Ten-Year Survival % | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Charlson Score | 0 | 2 | 21 | 53 | 77 | 90 | 96 | 98 | Total (no/%) |
| 0 | 00.0% RT | 00.0% RT | 00.0% RT | 00.0% RT | 00.0% RT | 00.0% RT | 00.0% RT | 130100.0% RT | 130/21.9 |
| 0.0% CT | 0.0% CT | 0.0% CT | 0.0% CT | 0.0% CT | 0.0% CT | 0.0% CT | 100.0% CT | ||
| 0.0% GT | 0.0% GT | 0.0% GT | 0.0% GT | 0.0% GT | 0.0% GT | 0.0% GT | 21.9% GT | ||
| 1 | 00.0% RT | 00.0% RT | 00.0% RT | 00.0% RT | 00.0% RT | 11.0% RT | 9699.0% RT | 00.0% RT | 97/16.3 |
| 0.0% CT | 0.0% CT | 0.0% CT | 0.0% CT | 0.0% CT | 0.8% CT | 100.0% CT | 0.0% CT | ||
| 0.0% GT | 0.0% GT | 0.0% GT | 0.0% GT | 0.0% GT | 0.2% GT | 16.2% GT | 0.0% GT | ||
| 2 | 00.0% RT | 00.0% RT | 00.0% RT | 00.0% RT | 00.0% RT | 116100.0% RT | 00.0% RT | 00.0% RT | 116/19.5 |
| 0.0% CT | 0.0% CT | 0.0% CT | 0.0% CT | 0.0% CT | 97.5% CT | 0.0% CT | 0.0% CT | ||
| 0.0% GT | 0.0% GT | 0.0% GT | 0.0% GT | 0.0% GT | 19.5% GT | 0.0% GT | 0.0% GT | ||
| 3 | 00.0% RT | 00.0% RT | 00.0% RT | 00.0% RT | 8297.6% RT | 22.4% RT | 00.0% RT | 00.0% RT | 84/14.1 |
| 0.0% CT | 0.0% CT | 0.0% CT | 0.0% CT | 100.0% CT | 1.7% CT | 0.0% CT | 0.0% CT | ||
| 0.0% GT | 0.0% GT | 0.0% GT | 0.0% GT | 13.8% GT | 0.3% GT | 0.0% GT | 0.0% GT | ||
| 4 | 00.0% RT | 00.0% RT | 00.0% RT | 79100.0% RT | 00.0% RT | 00.0% RT | 00.0% RT | 00.0% RT | 79/13.3 |
| 0.0% CT | 0.0% CT | 0.0% CT | 100.0% CT | 0.0% CT | 0.0% CT | 0.0% CT | 0.0% CT | ||
| 0.0% GT | 0.0% GT | 0.0% GT | 13.3% GT | 0.0% GT | 0.0% GT | 0.0% GT | 0.0% GT | ||
| 5 | 00.0% RT | 00.0% RT | 47100.0% RT | 00.0% RT | 00.0% RT | 00.0% RT | 00.0% RT | 00.0% RT | 47/7.9 |
| 0.0% CT | 0.0% CT | 100.0% CT | 0.0% CT | 0.0% CT | 0.0% CT | 0.0% CT | 0.0% CT | ||
| 0.0% GT | 0.0% GT | 7.9% GT | 0.0% GT | 0.0% GT | 0.0% GT | 0.0% GT | 0.0% GT | ||
| 6 | 00.0% RT | 25100.0% RT | 00.0% RT | 00.0% RT | 00.0% RT | 00.0% RT | 00.0% RT | 00.0% RT | 25/4.2 |
| 0.0% CT | 100.0% CT | 0.0% CT | 0.0% CT | 0.0% CT | 0.0% CT | 0.0% CT | 0.0% CT | ||
| 0.0% GT | 4.2% GT | 0.0% GT | 0.0% GT | 0.0% GT | 0.0% GT | 0.0% GT | 0.0% GT | ||
| 7 | 4100.0% RT | 00.0% RT | 00.0% RT | 00.0% RT | 00.0% RT | 00.0% RT | 00.0% RT | 00.0% RT | 4/0.7 |
| 25.0% CT | 0.0% CT | 0.0% CT | 0.0% CT | 0.0% CT | 0.0% CT | 0.0% CT | 0.0% CT | ||
| 0.7% GT | 0.0% GT | 0.0% GT | 0.0% GT | 0.0% GT | 0.0% GT | 0.0% GT | 0.0% GT | ||
| 8 | 9100.0% RT | 00.0% RT | 00.0% RT | 00.0% RT | 00.0% RT | 00.0% RT | 00.0% RT | 00.0% RT | 9/1.5 |
| 56.2% CT | 0.0% CT | 0.0% CT | 0.0% CT | 0.0% CT | 0.0% CT | 0.0% CT | 0.0% CT | ||
| 1.5% GT | 0.0% GT | 0.0% GT | 0.0% GT | 0.0% GT | 0.0% GT | 0.0% GT | 0.0% GT | ||
| 9 | 2100.0% RT | 00.0% RT | 00.0% RT | 00.0% RT | 00.0% RT | 00.0% RT | 00.0% RT | 00.0% RT | 2/0.3 |
| 12.5% CT | 0.0% CT | 0.0% CT | 0.0% CT | 0.0% CT | 0.0% CT | 0.0% CT | 0.0% CT | ||
| 0.3% GT | 0.0% GT | 0.0% GT | 0.0% GT | 0.0% GT | 0.0% GT | 0.0% GT | 0.0% GT | ||
| 12 | 1100.0% RT | 00.0% RT | 00.0% RT | 00.0% RT | 00.0% RT | 00.0% RT | 00.0% RT | 00.0% RT | 1/0.2 |
| 6.2% CT | 0.0% CT | 0.0% CT | 0.0% CT | 0.0% CT | 0.0% CT | 0.0% CT | 0.0% CT | ||
| 0.2% GT | 0.0% GT | 0.0% GT | 0.0% GT | 0.0% GT | 0.0% GT | 0.0% GT | 0.0% GT | ||
| Total no/% | 16/ 2.7 | 25/ 4.2 | 47/ 7.9 | 79/ 13.3 | 82/ 13.8 | 119/ 20 | 96/ 16.2 | 130/ 21.9 | 594/ 100 |
| Factor | N | Average | Standard Deviation | Different from Factor Number |
|---|---|---|---|---|
| (1) 0 | 130 | 98.0000 | 0.0000 | (2)(3)(4)(5)(6)(7)(8)(9)(10)(11) |
| (2) 1 | 97 | 95.9381 | 0.6092 | (1)(3)(4)(5)(6)(7)(8)(9)(10)(11) |
| (3) 2 | 116 | 90.0000 | 0.0000 | (1)(2)(4)(5)(6)(7)(8)(9)(10)(11) |
| (4) 3 | 84 | 77.3095 | 1.9938 | (1)(2)(3)(5)(6)(7)(8)(9)(10)(11) |
| (5) 4 | 79 | 53.0000 | 0.0000 | (1)(2)(3)(4)(6)(7)(8)(9)(10)(11) |
| (6) 5 | 47 | 21.0000 | 0.0000 | (1)(2)(3)(4)(5)(7)(8)(9)(10)(11) |
| (7) 6 | 25 | 2.0000 | 0.0000 | (1)(2)(3)(4)(5)(6)(8)(9)(10) |
| (8) 7 | 4 | 0.0000 | 0.0000 | (1)(2)(3)(4)(5)(6)(7) |
| (9) 8 | 9 | 0.0000 | 0.0000 | (1)(2)(3)(4)(5)(6)(7) |
| (10) 9 | 2 | 0.0000 | 0.0000 | (1)(2)(3)(4)(5)(6)(7) |
| (11) 12 | 1 | 0.0000 | 0.0000 | (1)(2)(3)(4)(5)(6) |
| Group | Arterial Hypertension | Percent % |
|---|---|---|
| Other | 166 | 56.46 |
| EC | 124 | 81.04 |
| Atypical EH | 9 | 64.28 |
| Typical EH | 71 | 53.38 |
| Total number/% | 370/100.0 | 62.28 |
| Association of DM + Diagnosis | Yes | No | % DM | Total |
|---|---|---|---|---|
| DM + EC | 49 | 104 | 32.02 | 153 |
| DM + Atypical EH | 3 | 11 | 21.42 | 14 |
| DM + Typical EH | 30 | 103 | 22.45 | 133 |
| DM + other | 51 | 243 | 17.34 | 294 |
| Total | 133 | 461 | 22.39 | 594 |
| Group | No. of Patients | % |
|---|---|---|
| Other | 69 | 23.46 |
| 100.0% RT | ||
| 33.2% CT | ||
| 33.2% GT | ||
| EC | 103 | 67.32 |
| 100.0% RT | ||
| 49.5% CT | ||
| 49.5% GT | ||
| Atypical EH | 5 | 35.71 |
| 100.0% RT | ||
| 2.4% CT | ||
| 2.4% GT | ||
| Typical EH | 31 | 23.3 |
| 100.0% RT | ||
| 14.9% CT | ||
| 14.9% GT | ||
| Total | 208 | 100 |
| Tukey HSD Dependent Variable Obesity | ||||||
|---|---|---|---|---|---|---|
| (I) Group | (J) Group | Av. Diff. (I-J) | SE | Sig. | 95% Confidence Interval | |
| ≤ | ≥ | |||||
| EC | Atypical EH | 0.316 * | 0.122 | 0.049 | 0 | 0.63 |
| Typical EH | 0.437 * | 0.052 | 0 | 0.3 | 0.57 | |
| other | 0.440 * | 0.044 | 0 | 0.33 | 0.55 | |
| Atypical EH | EC | −0.316 * | 0.122 | 0.049 | −0.63 | 0 |
| Typical EH | 0.121 | 0.123 | 0.762 | −0.2 | 0.44 | |
| Other | 0.124 | 0.12 | 0.729 | −0.18 | 0.43 | |
| Typical EH | EC | −0.437 * | 0.052 | 0 | −0.57 | −0.3 |
| Atypical EH | −0.121 | 0.123 | 0.762 | −0.44 | 0.2 | |
| Other | 0.004 | 0.046 | 1 | −0.12 | 0.12 | |
| Other | EC | −0.440 * | 0.044 | 0 | −0.55 | −0.33 |
| Atypical EH | −0.124 | 0.12 | 0.729 | −0.43 | 0.18 | |
| Typical EH | −0.004 | 0.046 | 1 | −0.12 | 0.12 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Furau, A.; Tit, D.M.; Furau, C.; Bungau, S.; Furau, G.; Toma, M.M.; Cirstoveanu, C.G.; Petre, I.; Todor, D.-S.; Romosan, R.S.; et al. Analysis of the Impact of Comorbidities on Endometrial Lesions Using the Charlson Comorbidity Index in Western Romania. Medicina 2021, 57, 945. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57090945
Furau A, Tit DM, Furau C, Bungau S, Furau G, Toma MM, Cirstoveanu CG, Petre I, Todor D-S, Romosan RS, et al. Analysis of the Impact of Comorbidities on Endometrial Lesions Using the Charlson Comorbidity Index in Western Romania. Medicina. 2021; 57(9):945. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57090945
Chicago/Turabian StyleFurau, Alexandru, Delia Mirela Tit, Cristian Furau, Simona Bungau, Gheorghe Furau, Mirela Marioara Toma, Catalin Gabriel Cirstoveanu, Izabella Petre, Denisia-Suzana Todor, Radu Stefan Romosan, and et al. 2021. "Analysis of the Impact of Comorbidities on Endometrial Lesions Using the Charlson Comorbidity Index in Western Romania" Medicina 57, no. 9: 945. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57090945