
Craniovertebral and Craniomandibular Changes in Patients with Temporomandibular Joint Disorders after Physiotherapy Combined with Occlusal Splint Therapy: A Prospective Case Control Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Intervention
2.4. Outcome Measures
2.5. Sample Size Calculation
2.6. Statistical Analysis
3. Results
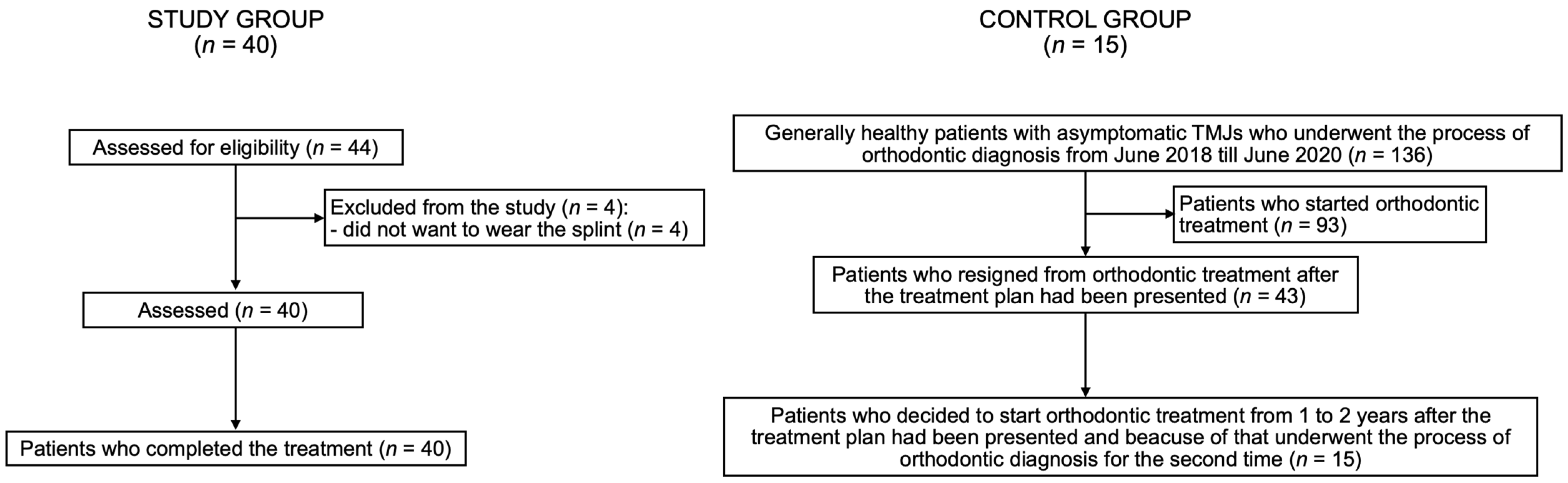
3.1. Flow of Participants
3.2. Research Question
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Look, J.; Anderson, G.; Goulet, J.P.; List, T.; Svensson, P.; Gonzalez, Y.; Lobbezoo, F.; et al. International RDC/TMD Consortium Network, International association for Dental Research; Orofacial Pain Special Interest Group, International Association for the Study of Pain. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: Recommendations of the International RDC/TMD Consortium Network and Orofacial Pain Special Interest Group. J. Oral Facial. Pain Headache 2014, 28, 6–27. [Google Scholar] [CrossRef]
- Michelotti, A.; Alstergren, P.; Goulet, J.P.; Lobbezoo, F.; Ohrbach, R.; Peck, C.; Schiffman, E.; List, T. Next steps in development of the diagnostic criteria for temporomandibular disorders (DC/TMD): Recommendations from the International RDC/TMD Consortium Network workshop. J. Oral Rehabil. 2016, 43, 453–467. [Google Scholar] [CrossRef] [PubMed]
- Gauer, R.L.; Semidey, M.J. Diagnosis and treatment of temporomandibular disorders. Am. Fam. Physician 2015, 91, 378–386. [Google Scholar]
- Liu, F.; Steinkeler, A. Epidemiology, diagnosis, and treatment of temporomandibular disorders. Dent. Clin. N. Am. 2013, 57, 465–479. [Google Scholar] [CrossRef]
- Valesan, L.F.; Da-Cas, C.D.; Réus, J.C.; Denardin, A.C.S.; Garanhani, R.R.; Bonotto, D.; Januzzi, E.; de Souza, B.D.M. Prevalence of temporomandibular joint disorders: A systematic review and meta-analysis. Clin. Oral Investig. 2021, 25, 441–453. [Google Scholar] [CrossRef]
- Robinson, J.L.; Johnson, P.M.; Kister, K.; Yin, M.T.; Chen, J.; Wadhwa, S. Estrogen signaling impacts temporomandibular joint and periodontal disease pathology. Odontology 2020, 108, 153–165. [Google Scholar] [CrossRef]
- Manfredini, D.; Guarda-Nardini, L.; Winocur, E.; Piccotti, F.; Ahlberg, J.; Lobbezoo, F. Research diagnostic criteria for temporomandibular disorders: A systematic review of axis I epidemiologic findings. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2011, 112, 453–462. [Google Scholar] [CrossRef]
- Manfredini, D.; Lombardo, L.; Siciliani, G. Temporomandibular disorders and dental occlusion. A systematic review of association studies: End of an era? J. Oral Rehabil. 2017, 44, 908–923. [Google Scholar] [CrossRef]
- Magnusson, T.; Egermarki, I.; Carlsson, G.E. A prospective investigation over two decades on signs and symptoms of temporomandibular disorders and associated variables. A final summary. Acta Odontol. Scand. 2005, 63, 99–109. [Google Scholar] [CrossRef]
- Michelotti, A.; Iodice, G. The role of orthodontics in temporomandibular disorders. J. Oral Rehabil. 2010, 37, 411–429. [Google Scholar] [CrossRef]
- Derwich, M.; Mitus-Kenig, M.; Pawlowska, E. Interdisciplinary Approach to the Temporomandibular Joint Osteoarthritis-Review of the Literature. Medicina 2020, 56, 225. [Google Scholar] [CrossRef] [PubMed]
- Bialosky, J.E.; Bishop, M.D.; Price, D.D.; Robinson, M.E.; George, S.Z. The mechanisms of manual therapy in the treatment of musculoskeletal pain: A comprehensive model. Man. Ther. 2009, 14, 531–538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gomes, C.A.; Politti, F.; Andrade, D.V.; de Sousa, D.F.; Herpich, C.M.; Dibai-Filho, A.V.; Gonzalez Tde, O.; Biasotto-Gonzalez, D.A. Effects of massage therapy and occlusal splint therapy on mandibular range of motion in individuals with temporomandibular disorder: A randomized clinical trial. J. Manip. Physiol. Ther. 2014, 37, 164–169. [Google Scholar] [CrossRef] [PubMed]
- Kuzmanovic Pficer, J.; Dodic, S.; Lazic, V.; Trajkovic, G.; Milic, N.; Milicic, B. Occlusal stabilization splint for patients with temporomandibular disorders: Meta-analysis of short and long term effects. PLoS ONE 2017, 12, e0171296. [Google Scholar] [CrossRef]
- Calixtre, L.B.; Moreira, R.F.; Franchini, G.H.; Alburquerque-Sendín, F.; Oliveira, A.B. Manual therapy for the management of pain and limited range of motion in subjects with signs and symptoms of temporomandibular disorder: A systematic review of randomised controlled trials. J. Oral Rehabil. 2015, 42, 847–861. [Google Scholar] [CrossRef]
- Lopez, A.J.; Scheer, J.K.; Leibl, K.E.; Smith, Z.A.; Dlouhy, B.J.; Dahdaleh, N.S. Anatomy and biomechanics of the craniovertebral junction. Neurosurg. Focus 2015, 38, E2. [Google Scholar] [CrossRef] [Green Version]
- Akita, K.; Sakaguchi-Kuma, T.; Fukino, K.; Ono, T. Masticatory Muscles and Branches of Mandibular Nerve: Positional Relationships Between Various Muscle Bundles and Their Innervating Branches. Anat. Rec. 2019, 302, 609–619. [Google Scholar] [CrossRef]
- Shaw, S.M.; Martino, R.; Mahdi, A.; Sawyer, F.K.; Mathur, S.; Hope, A.; Agur, A.M. Architecture of the Suprahyoid Muscles: A Volumetric Musculoaponeurotic Analysis. J. Speech Lang. Hear. Res. 2017, 60, 2808–2818. [Google Scholar] [CrossRef]
- Tsumori, N.; Abe, S.; Agematsu, H.; Hashimoto, M.; Ide, Y. Morphologic characteristics of the superior pharyngeal constrictor muscle in relation to the function during swallowing. Dysphagia 2007, 22, 122–129. [Google Scholar] [CrossRef]
- Derwich, M.; Pawlowska, E. Do the Mandibular Condyles Change Their Positions within Glenoid Fossae after Occlusal Splint Therapy Combined with Physiotherapy in Patients Diagnosed with Temporomandibular Joint Disorders? A Prospective Case Control Study. J. Pers. Med. 2022, 12, 254. [Google Scholar] [CrossRef]
- Rocabado, M.; Iglarsh, Z.A. Physical modalities and manual techniques used in the treatment of maxillofacial pain. In Musculoskeletal Approach to Maxillofacial Pain, 1st ed.; JB Lippincott: Philadelphia, PA, USA, 1991; pp. 187–192. [Google Scholar]
- Derwich, M.; Mitus-Kenig, M.; Pawlowska, E. Is the Temporomandibular Joints' Reciprocal Clicking Related to the Morphology and Position of the Mandible, as Well as to the Sagittal Position of Lower Incisors?-A Case-Control Study. Int. J. Environ. Res. Public Health 2021, 18, 4994. [Google Scholar] [CrossRef] [PubMed]
- Rocabado, M. Biomechanical relationship of the cranial, cervical, and hyoid regions. J. Craniomandib. Pract. 1983, 1, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Wieckiewicz, M.; Boening, K.; Wiland, P.; Shiau, Y.Y.; Paradowska-Stolarz, A. Reported concepts for the treatment modalities and pain management of temporomandibular disorders. J. Headache Pain. 2015, 16, 106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ismail, F.; Demling, A.; Hessling, K.; Fink, M.; Stiesch-Scholz, M. Short-term efficacy of physical therapy compared to splint therapy in treatment of arthrogenous TMD. J. Oral Rehabil. 2007, 34, 807–813. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Xu, L.; Wu, D.; Yu, C.; Fan, S.; Cai, B. Effectiveness of exercise therapy versus occlusal splint therapy for the treatment of painful temporomandibular disorders: A systematic review and meta-analysis. Ann. Palliat. Med. 2021, 10, 6122–6132. [Google Scholar] [CrossRef] [PubMed]
- Espí-López, G.V.; Arnal-Gómez, A.; Cuerda Del Pino, A.; Benavent-Corai, J.; Serra-Añó, P.; Inglés, M. Effect of Manual Therapy and Splint Therapy in People with Temporomandibular Disorders: A Preliminary Study. J. Clin. Med. 2020, 9, 2411. [Google Scholar] [CrossRef] [PubMed]
- Shankland, W.E., 2nd. Anterior throat pain syndromes: Causes for undiagnosed craniofacial pain. Cranio 2010, 28, 50–59. [Google Scholar] [CrossRef]
- Moya, H.; Miralles, R.; Zuñiga, C.; Carvajal, R.; Rocabado, M.; Santander, H. Influence of stabilization occlusal splint on craniocervical relationships. Part I: Cephalometric analysis. Cranio 1994, 12, 47–51. [Google Scholar] [CrossRef]
- Miralles, R.; Moya, H.; Ravera, M.J.; Santander, H.; Zúñiga, C.; Carvajal, R.; Yazigi, C. Increase of the vertical occlusal dimension by means of a removable orthodontic appliance and its effect on craniocervical relationships and position of the cervical spine in children. Cranio 1997, 15, 221–228. [Google Scholar] [CrossRef]
- Oliveira, S.S.I.; Pannuti, C.M.; Paranhos, K.S.; Tanganeli, J.P.C.; Laganá, D.C.; Sesma, N.; Duarte, M.; Frigerio, M.L.M.A.; Cho, S.C. Effect of occlusal splint and therapeutic exercises on postural balance of patients with signs and symptoms of temporomandibular disorder. Clin. Exp. Dent. Res. 2019, 5, 109–115. [Google Scholar] [CrossRef] [Green Version]
- Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia 2013, 33, 629–808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barmherzig, R.; Kingston, W. Occipital Neuralgia and Cervicogenic Headache: Diagnosis and Management. Curr. Neurol. Neurosci. Rep. 2019, 19, 20. [Google Scholar] [CrossRef] [PubMed]
- Bogduk, N. Cervicogenic headache: Anatomic basis and pathophysiologic mechanisms. Curr. Pain. Headache Rep. 2001, 5, 382–386. [Google Scholar] [CrossRef] [PubMed]
- Rocabado, M. The importance of soft tissue mechanics in stability and instability of the cervical spine: A functional diagnosis for treatment planning. Cranio 1987, 5, 130–138. [Google Scholar] [CrossRef]
- Been, E.; Shefi, S.; Soudack, M. Cervical lordosis: The effect of age and gender. Spine J. 2017, 17, 880–888. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Measurement | Point/Line/Angle | Description |
|---|---|---|
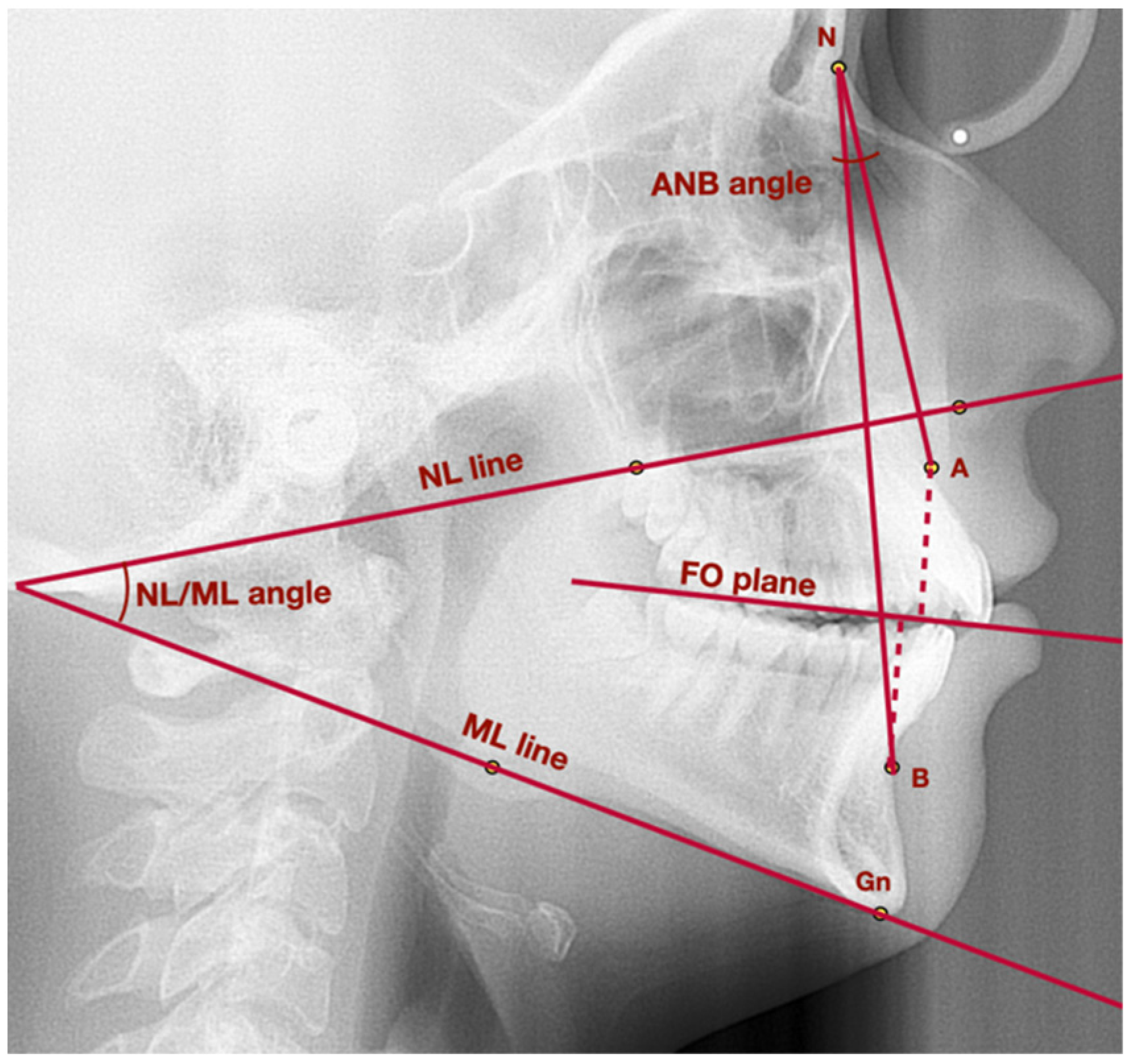
| General points and lines | Point A | Subspinale—point localized in the deepest area of the anterior outline of the maxilla, below the anterior nasal spine |
| Point B | Supramentale—point localized in the deepest area of the anterior outline of the mandible, above the pogonion | |
| Point S | Sella—geometrical center of Sella turcica | |
| Point Pg | Pogonion—the most prominent point localized in the mental tuberosity | |
| Point N | Nasion—the most anterior point localized in the frontonasal suture | |
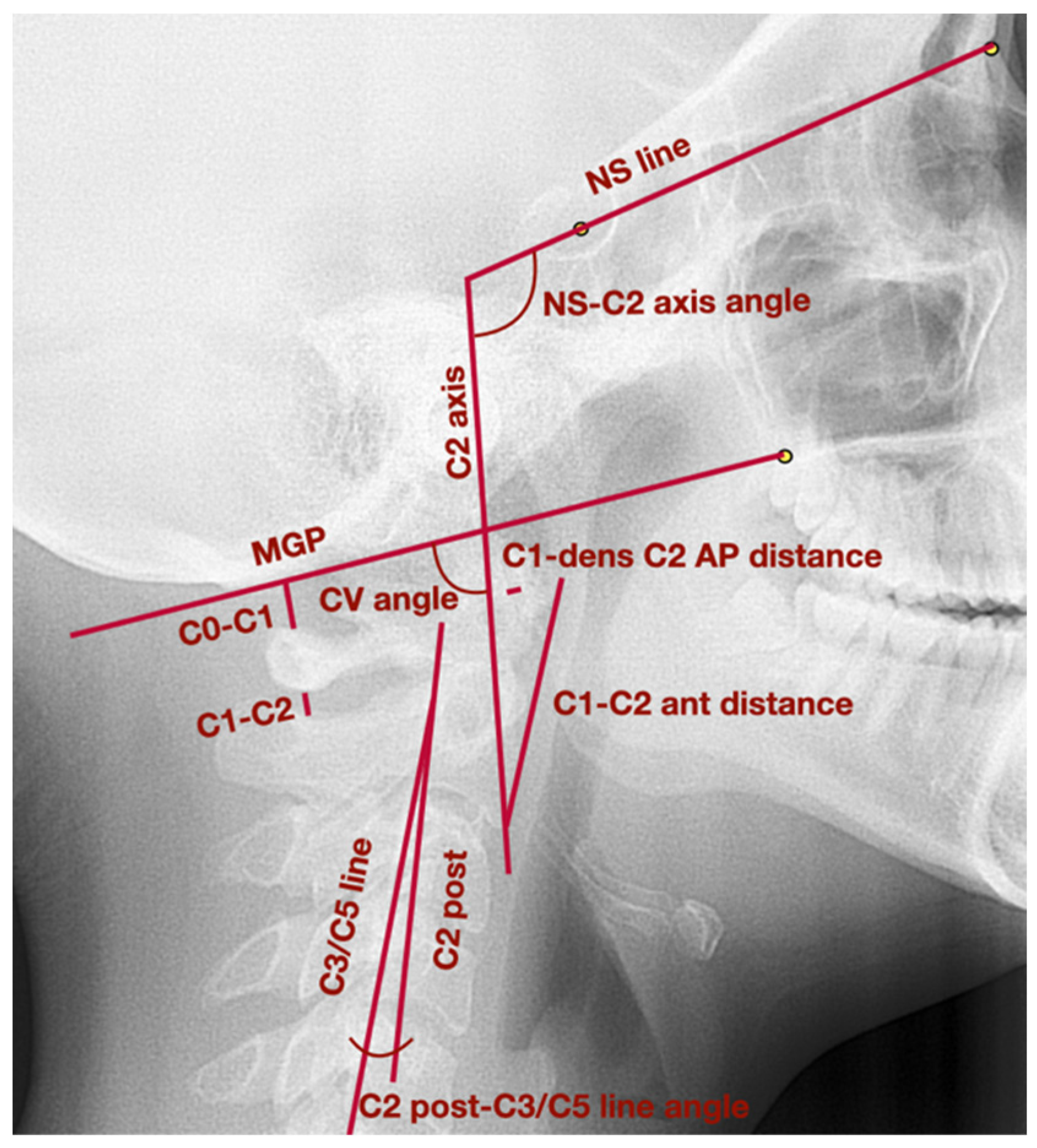
| C2 axis | Long axis of C2 vertebra, which crosses the apex of the odontoid process and the most inferior anterior angle of the body of the second cervical vertebra | |
| C2 post | Line tangent to the posterior wall of the odontoid process of the second cervical vertebra | |
| C3/C5 line | Line which links the most posterior superior angle of the body of the third cervical vertebra with the most posterior inferior angle of the body of the fifth cervical vertebra | |
| MGP | McGregor’s Plane—line which links posterior nasal spine with the basiocciput | |
| NS line | Line which crosses the points: nasion and sella | |
| NL line | Nasal line—line which crosses the points: anterior nasal spine and posterior nasal spine | |
| ML line | Mandibular line—line tangent to the lower border of the mandible, which crosses points: gnathion and the lowest point in the masseteric tuberosity | |
| NA line | Line which crosses points: nasion and point A | |
| NB line | Line which crosses points: nasion and point B | |
| Vertical position of mandible | NL-ML angle | The angle between NL line and ML line |
| Sagittal position of mandible | Wits | The distance between the perpendicular projection of points A and B onto the functional occlusal plane |
| ANB | The angle between the lines: NA line and NB line | |
| Head position and cervical vertebrae | CV angle | The posterior angle between the lines: C2 axis and MGP |
| C2 post-C3/C5 line angle | The angle between the lines: posterior wall of C2 odontoid process and C3/C5 line; the value of the angle is positive when the C2 axis is placed anteriorly to C3/C5 line; when the C2 axis is placed posteriorly to C3/C5 line, the value of the angle is negative | |
| C1-dens C2 AP distance | The anteroposterior distance between anterior surface of the odontoid process and posterior border of the atlas anterior arch | |
| C1-C2 ant distance | The distance between the most anterior point of the atlas anterior arch and the most inferior anterior angle of the body of the second cervical vertebra | |
| NS-C2 axis angle | The anterior angle between the lines: NS line and C2 axis | |
| Cervical vertebrae functional spaces | C0-C1 distance | The distance between basiocciput and superior part of the posterior arch of the atlas |
| C1-C2 distance | The distance between inferior part of the posterior arch of the atlas and superior part of the spinous process of the second cervical vertebra |
| Diagnosis on the Basis of DC/TMD | Number of Patients (%) |
|---|---|
| Myalgia | 29 (72.5%) |
| Arthralgia | 11 (27.5%) |
| Headache attributed to TMD | 13 (32.5%) |
| Disc displacement with reduction | 31 (77.5%) |
| Disc displacement with reduction with intermittent locking | 3 (7.5%) |
| Disc displacement without reduction with limited opening | 0 |
| Disc displacement without reduction without limited opening | 0 |
| Degenerative joint disease | 5 (12.5%) |
| Subluxation | 11 (27.5%) |
| Comparable Characteristic | Study Group av. ± SD (95% CI) | Control Group av. ± SD (95% CI) | p-Value | |
|---|---|---|---|---|
| Vertical position of mandible | NL-ML angle (°) | 25.5 ± 7.4 (23.2 to 27.6) | 21.1 ± 5.5 (18.0 to 24.1) | 0.0469 a |
| Sagittal position of mandible | Wits (mm) | 1.3 ± 2.9 (0.2 to 2.2) | 0.6 ± 2.8 (−0.9 to 2.2) | 0.5278 a |
| ANB (°) | 3.8 ± 2.8 (2.9 to 4.7) | 2.3 ± 2.7 (0.9 to 3.8) | 0.0932 a | |
| Head position and cervical vertebrae | CV angle (°) | 100.3 ± 8.3 (97.6 to 103.0) | 100.4 ± 7.1 (96.4 to 104.3) | 0.9478 a |
| C2 post-C3/C5 line angle (°) | 10.6 ± 7.9 (8.5 to 13.5) | 9.0 ± 7.7 (4.7 to 13.2) | 0.4845 a | |
| C1-dens C2 AP distance (mm) | 1.5 ± 0.3 (1.4 to 1.6) | 1.5 ± 0.2 (1.4 to 1.6) | 0.6638 b | |
| C1-C2 ant distance (mm) | 33.3 ± 3.5 (32.2 to 34.5) | 34.4 ± 2.6 (32.9 to 35.9) | 0.2964 a | |
| NS-C2 axis angle (°) | 87.6 ± 8.3 (85.2 to 90.7) | 87.3 ± 6.5 (83.7 to 90.9) | 0.8130 a | |
| Cervical vertebrae functional spaces | C0-C1 distance (mm) | 6.8 ± 3.2 (5.8 to 7.6) | 7.4 ± 1.6 (6.5 to 8.2) | 0.3443 a |
| C1-C2 distance (mm) | 5.9 ± 2.0 (5.4 to 6.3) | 5.5 ± 1.7 (4.6 to 6.5) | 0.4368 a | |
| Comparable Characteristic | First Examination av. ± SD (95% CI) | Second Examination (1–2 Years after the Initial One) av. ± SD (95% CI) | p-Value | |
|---|---|---|---|---|
| Vertical position of mandible | NL-ML angle (°) | 21.1 ± 5.5 (18.0 to 24.1) | 21.1 ± 5.5 (18.0 to 24.1) | 1.0000 a |
| Sagittal position of mandible | Wits (mm) | 0.6 ± 2.8 (−0.9 to 2.2) | 0.6 ± 2.8 (−0.9 to 2.2) | 1.0000 a |
| ANB (°) | 2.3 ± 2.7 (0.9 to 3.8) | 2.3 ± 2.7 (0.9 to 3.8) | 1.0000 b | |
| Head position and cervical vertebrae | CV angle (°) | 100.4 ± 7.1 (96.4 to 104.3) | 100.4 ± 7.0 (96.5 to 104.2) | 0.3003 b |
| C2 post-C3/C5 line angle (°) | 9.0 ± 7.7 (4.7 to 13.2) | 9.0 ± 7.6 (4.7 to 13.2) | 0.5563 b | |
| C1-dens C2 AP distance (mm) | 1.5 ± 0.2 (1.4 to 1.6) | 1.5 ± 0.2 (1.4 to 1.6) | 0.5930 b | |
| C1-C2 ant distance (mm) | 34.4 ± 2.6 (32.9 to 35.9) | 34.4 ± 2.6 (33.0 to 35.8) | 0.3505 b | |
| NS-C2 axis angle (°) | 87.3 ± 6.5 (83.7 to 90.9) | 87.3 ± 6.5 (83.7 to 90.9) | 0.9029 a | |
| Cervical vertebrae functional spaces | C0-C1 distance (mm) | 7.4 ± 1.6 (6.5 to 8.2) | 7.4 ± 1.6 (6.5 to 8.2) | 0.8494 a |
| C1-C2 distance (mm) | 5.5 ± 1.7 (4.6 to 6.5) | 5.5 ± 1.6 (4.6 to 6.4) | 0.8939 b | |
| Comparable Characteristic | Before Treatment av. ± SD (95% CI) | After Treatment av. ± SD (95% CI) | p-Value | |
|---|---|---|---|---|
| Vertical position of mandible | NL-ML angle (°) | 25.5 ± 7.4 (23.2 to 27.6) | 27.1 ± 7.8 (24.2 to 29.8) | <0.0001 a |
| Sagittal position of mandible | Wits (mm) | 1.3 ± 2.9 (0.2 to 2.2) | 1.9 ± 3.2 (0.8 to 3.0) | 0.0065 a |
| ANB (°) | 3.8 ± 2.8 (2.9 to 4.7) | 4.4 ± 3.2 (3.3 to 5.5) | 0.0092 b | |
| Head position and cervical vertebrae | CV angle (°) | 100.3 ± 8.3 (97.6 to 103.0) | 99.7 ± 9.4 (96.6 to 103.1) | 0.4735 a |
| C2 post-C3/C5 line angle (°) | 10.6 ± 7.9 (8.5 to 13.5) | 14.6 ± 9.1 (11.5 to 17.6) | <0.0001 a | |
| C1-dens C2 AP distance (mm) | 1.5 ± 0.3 (1.4 to 1.6) | 1.5 ± 0.3 (1.4 to 1.6) | 0.5255 b | |
| C1-C2 ant distance (mm) | 33.3 ± 3.5 (32.2 to 34.5) | 33.3 ± 3.32 (32.2 to 34.1) | 0.9406 b | |
| NS-C2 axis angle (°) | 87.6 ± 8.3 (85.2 to 90.7) | 88.0 ± 8.6 (85.2 to 90.8) | 0.8265 a | |
| Cervical vertebrae functional spaces | C0-C1 distance (mm) | 6.8 ± 3.2 (5.8 to 7.6) | 6.8 ± 3.1 (5.8 to 7.9) | 0.3245 b |
| C1-C2 distance (mm) | 5.9 ± 2.0 (5.4 to 6.3) | 5.3 ± 1.8 (4.7 to 6.1) | 0.0042 a | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Derwich, M.; Gottesman, L.; Urbanska, K.; Pawlowska, E. Craniovertebral and Craniomandibular Changes in Patients with Temporomandibular Joint Disorders after Physiotherapy Combined with Occlusal Splint Therapy: A Prospective Case Control Study. Medicina 2022, 58, 684. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58050684
Derwich M, Gottesman L, Urbanska K, Pawlowska E. Craniovertebral and Craniomandibular Changes in Patients with Temporomandibular Joint Disorders after Physiotherapy Combined with Occlusal Splint Therapy: A Prospective Case Control Study. Medicina. 2022; 58(5):684. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58050684
Chicago/Turabian StyleDerwich, Marcin, Lawrence Gottesman, Karolina Urbanska, and Elzbieta Pawlowska. 2022. "Craniovertebral and Craniomandibular Changes in Patients with Temporomandibular Joint Disorders after Physiotherapy Combined with Occlusal Splint Therapy: A Prospective Case Control Study" Medicina 58, no. 5: 684. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58050684