
The Use of near Infra-Red Radiation Imaging after Injection of Indocyanine Green (NIR–ICG) during Laparoscopic Treatment of Benign Gynecologic Conditions: Towards Minimalized Surgery. A Systematic Review of Literature

 , , , ,
, , , , 
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Protocol
2.2. Search Strategy and Study Selection
- −
- case reports;
- −
- literature reviews;
- −
- studies in languages other than English;
- −
- video articles;
- −
- studies which assessed the use of NIR–ICG in gynecologic malignancies or in non-gynecologic conditions.
2.3. Risk of Bias within Studies Assessment
2.4. Data Extraction
3. Results
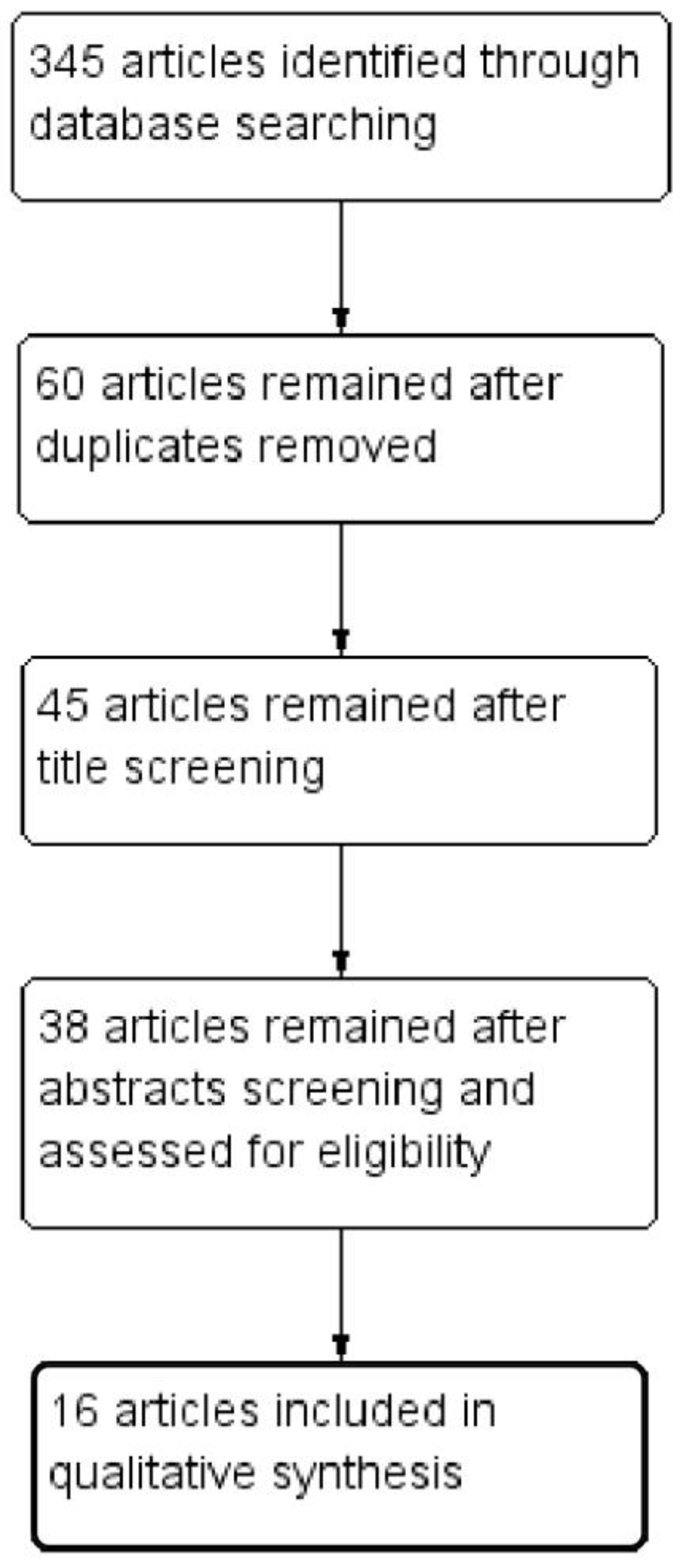
3.1. Study Selection
3.2. Studies and Patients’ Characteristics
- −
- −
3.3. NIR–ICG Performance
- −
- −
- supporting surgeons in surgical decision-making process with the assessment of ureteral perfusion after conservative surgery [1];
- −
- improving endometriosis identification, with particular help in (1) separating the healthy rectal tissue from the rectovaginal DIE nodules (RVDIEN) [22], (2) decision whether to enlarge the resection to the posterior vaginal fornix in case of RVDIEN [22], (3) in the resection of deep infiltrating nodules [22]; such improvement was not found in one study [19];
- −
- −
- evaluating vascular perfusion of the vaginal cuff during total laparoscopic hysterectomy (TLH) and robotic-assisted total laparoscopic hysterectomy (RATLH), with help in understanding causes for vaginal cuff dehiscence; however, an improving in methods for quantification of fluorescence might be needed to utilize it for clinical use [26,27];
- −
- intraoperative assessment of ovarian perfusion in adnexal torsion [16].
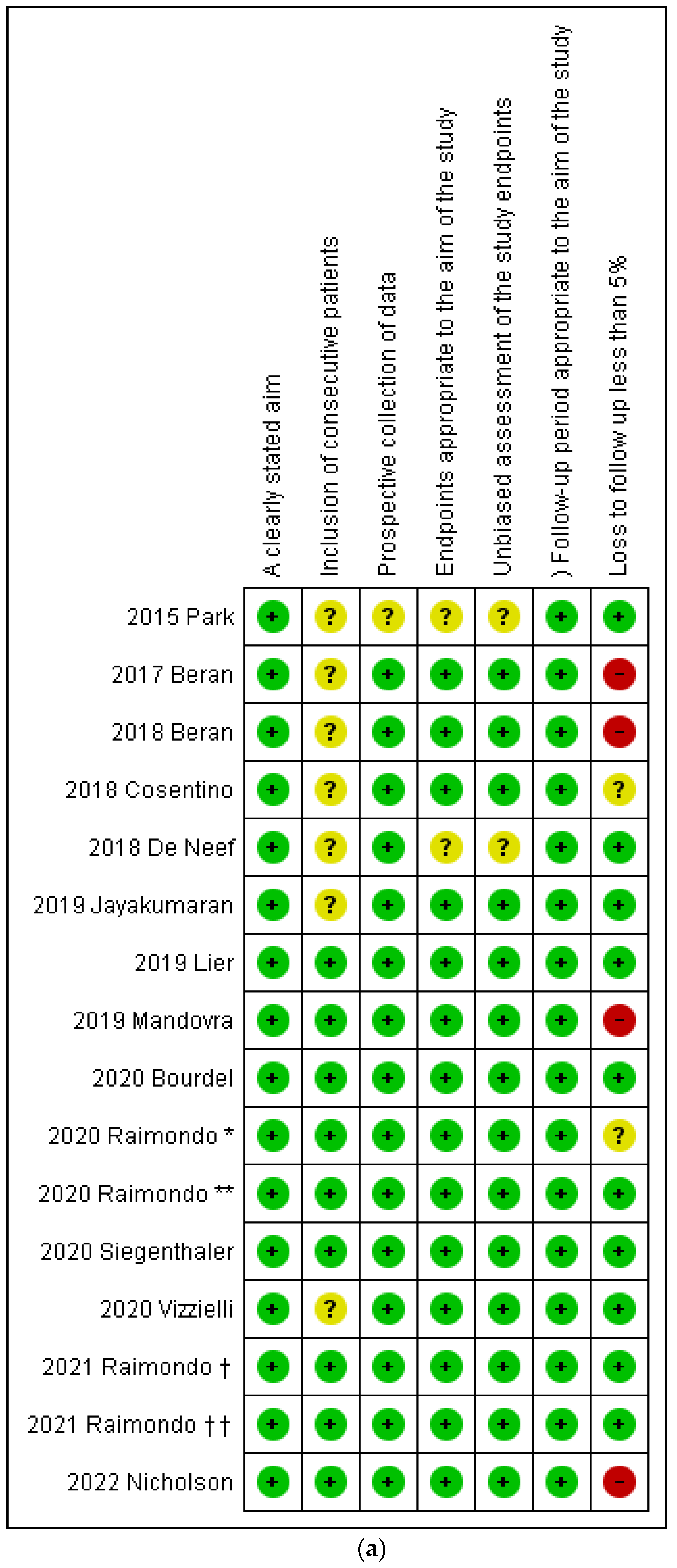
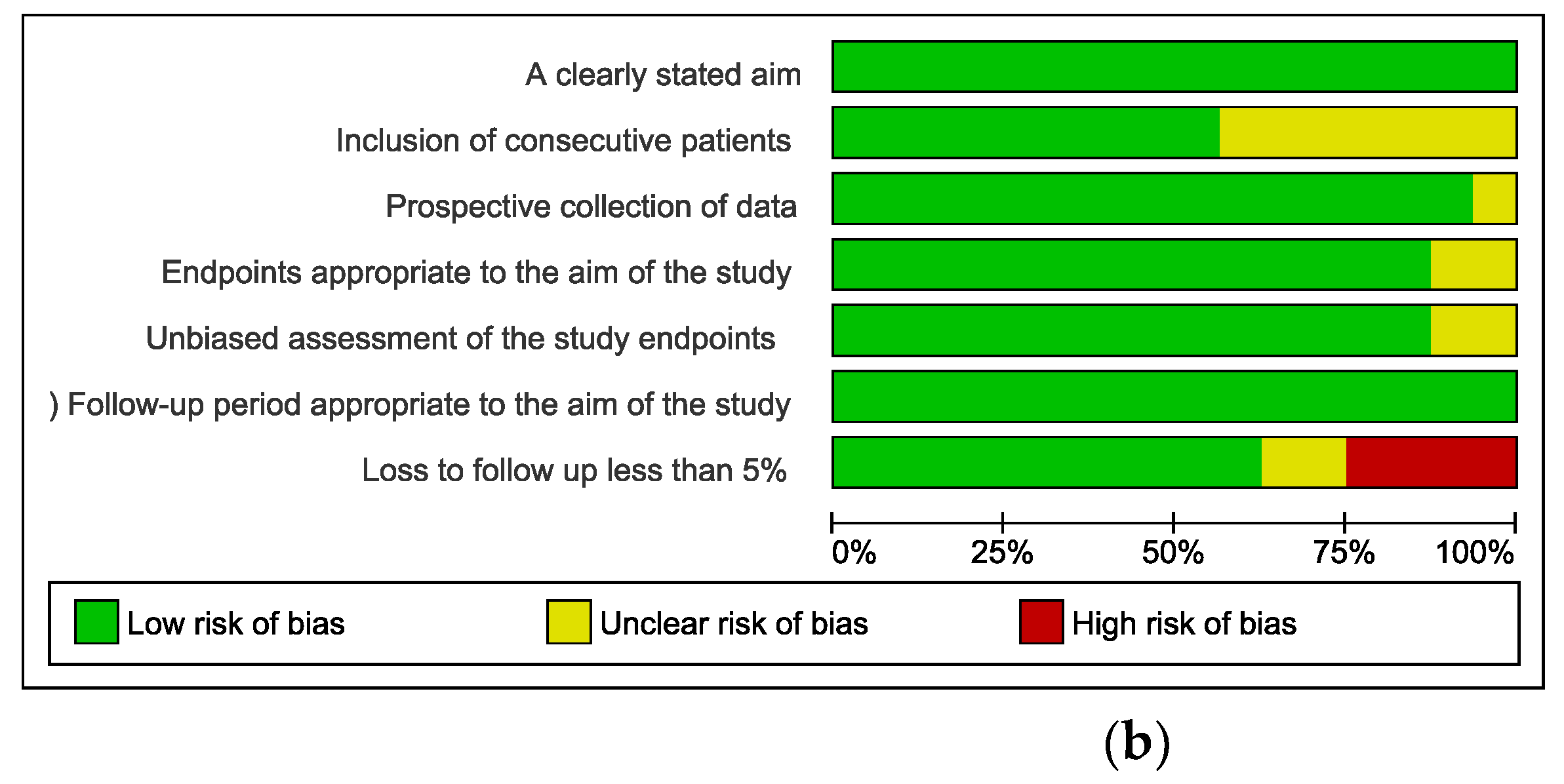
3.4. Risk of Bias within Studies Assessment
4. Discussion
4.1. Main Findings
4.2. NIR_ICG History
4.3. NIR–ICG Application in Gynecological Conditions
4.3.1. Endometriosis
Localization of Ureteral Course
Endometriosis Identification and DIE
4.3.2. Non-Endometriosis Conditions
Evaluation of the Vascular Perfusion of Vaginal Cuff
Evaluation of Ovarian Perfusion after Adnexal Detorsion
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Raimondo, D.; Borghese, G.; Mabrouk, M.; Arena, A.; Ambrosio, M.; Del Forno, S.; Degli Esposti, E.; Casadio, P.; Mattioli, G.; Mastronardi, M.; et al. Use of Indocyanine Green for Intraoperative Perfusion Assessment in Women with Ureteral Endometriosis: A Preliminary Study. J. Minim. Invasive Gynecol. 2021, 28, 42–49. [Google Scholar] [CrossRef]
- Raimondo, D.; Mastronardi, M.; Mabrouk, M.; Cafagna, G.; Salucci, P.; Arena, A.; Iodice, R.; Borghese, G.; Casadio, P.; Del Forno, S.; et al. Rectosigmoid Endometriosis Vascular Patterns at Intraoperative Indocyanine Green Angiography and their Correlation with Clinicopathological Data. Surg. Innov. 2020, 27, 474–480. [Google Scholar] [CrossRef]
- Lue, J.; Pyrzak, A.; Allen, J. Improving accuracy of intra-operative diagnosis of endometriosis: Role of firefly in minimal access robotic surgery. J. Minimal Access Surg. 2016, 12, 186–189. [Google Scholar] [CrossRef]
- Alander, J.T.; Kaartinen, I.; Laakso, A.; Pätilä, T.; Spillmann, T.; Tuchin, V.V.; Venermo, M.; Välisuo, P. A review of indocyanine greenfluorescent imaging in surgery. Int. J. Biomed. Imaging 2012, 2012, 940585. [Google Scholar] [CrossRef]
- Tajima, Y.; Murakami, M.; Yamazaki, K.; Masuda, Y.; Kato, M.; Sato, A.; Goto, S.; Otsuka, K.; Kato, T.; Kusano, M. Sentinel node mapping guided by indocyanine green fluorescence imaging during laparoscopic surgery in gastric cancer. Ann. Surg. Oncol. 2010, 17, 1787–1793. [Google Scholar] [CrossRef]
- Tanaka, E.; Choi, H.S.; Fujii, H.; Bawendi, M.G.; Frangioni, J.V. Image-guided oncologic surgery using invisible light: Completed pre-clinical development for sentinel lymph node mapping. Ann. Surg. Oncol. 2006, 13, 1671–1681. [Google Scholar] [CrossRef]
- Cosentino, F.; Vizzielli, G.; Turco, L.C.; Fagotti, A.; Cianci, S.; Vargiu, V.; Zannoni, G.F.; Ferrandina, G.; Scambia, G. Near-infrared imaging with indocyanine green for detection of endometriosis lesions (greendo trial): A pilot study. J. Minim. Invasive Gynecol. 2018, 25, 1249–1254. [Google Scholar] [CrossRef]
- Laios, A.; Volpi, D.; Tullis, I.D.; Woodward, M.; Kennedy, S.; Pathiraja, P.N.; Haldar, K.; Vojnovic, B.; Ahmed, A.A. A prospective pilot study of detection of sentinel lymph nodes in gynaecological cancers using a novel near infrared fluorescence imaging system. BMC Res. Notes 2015, 8, 608. [Google Scholar] [CrossRef]
- Manny, T.B.; Patel, M.; Hemal, A.K. Fluorescence-enhanced robotic radical prostatectomy using real-time lymphangiography and tissue marking with percutaneous injection of unconjugated indocyanine green: The initial clinical experience in 50 patients. Eur. Urol. 2014, 65, 1162–1168. [Google Scholar] [CrossRef]
- Rossi, E.C.; Jackson, A.; Ivanova, A.; Boggess, J.F. Detection of sentinel nodes for endometrial cancer with robotic assisted fluorescence imaging: Cervical versus hysteroscopic injection. Int. J. Gynecol. Cancer 2013, 23, 1704–1711. [Google Scholar] [CrossRef]
- Cahill, R.A.; Anderson, M.; Wang, L.M.; Lindsey, I.; Cunningham, C.; Mortensen, N.J. Near-infrared (NIR) laparoscopy for intraoperative lymphatic road-mapping and sentinel node identification during definitive surgical resection of early-stage colorectal neoplasia. Surg. Endosc. 2012, 26, 197–204. [Google Scholar] [CrossRef]
- Jayakumaran, J.; Pavlovic, Z.; Fuhrich, D.; Wiercinski, K.; Buffington, C.; Caceres, A. Robotic single-site endometriosis resection using near-infrared fluorescence imaging with indocyanine green: A prospective case series and review of literature. J. Robot. Surg. 2019, 14, 145–154. [Google Scholar] [CrossRef]
- Seracchioli, R.; Raimondo, D.; Arena, A.; Zanello, M.; Mabrouk, M. Clinical use of endovenous indocyanine green during rectosigmoid segmental resection for endometriosis. Fertil. Steril. 2018, 109, 1135. [Google Scholar] [CrossRef]
- Raimondo, D.; Maletta, M.; Malzoni, M.; Cosentino, F.; Scambia, G.; Falcone, F.; Coppola, M.; Turco, L.C.; Borghese, G.; Raffone, A.; et al. Indocyanine green fluorescence angiography after full-thickness bowel resection for rectosigmoid endometriosis: A multicentric experience with quantitative analysis. Int. J. Gynaecol. Obstet. 2021, 28, 1225–1230. [Google Scholar] [CrossRef]
- Raimondo, D.; Maletta, M.; Borghese, G.; Mastronardi, M.; Arena, A.; Del Forno, S.; Salucci, P.; Giaquinto, I.; Casadio, P.; Seracchioli, R. Indocyanine Green Fluorescence Angiography after Full-thickness Bowel Resection for Rectosigmoid Endometriosis-A Feasibility Study. J. Minim. Invasive Gynecol. 2021, 28, 1225–1230. [Google Scholar] [CrossRef]
- Nicholson, K.; Urh, A.; Demertzis, K.; Holubyeva, A.; LaPier, Z.; Cisneros-Camacho, A.; Goldberg, G.L.; Schwartz, B. Intraoperative Indocyanine Green Dye Use in Ovarian Torsion: A Feasibility Study. J. Minim. Invasive Gynecol. 2022, S1553-46. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef]
- Deeks, J.; Bossuyt, P.; Leeflang, M.; Takwoingi, Y.; Flemyng, E. Cochrane Handbook for Systematic Reviews of Diagnostic Test Accuracy. Cochrane Training; Cochrane: London, UK, 2022. [Google Scholar]
- Lier, M.C.I.; Vlek, S.L.; Ankersmit, M.; van de Ven, P.M.; Dekker, J.J.M.L.; Bleeker, M.C.G.; Mijatovic, V.; Tuynman, J.B. Comparison of enhanced laparoscopic imaging techniques in endometriosis surgery: A diagnostic accuracy study. Surg. Endosc. 2020, 34, 96–104. [Google Scholar] [CrossRef]
- Park, H.; Farnam, R.W. Novel Use of Indocyanine Green for Intraoperative, Real-time Localization of Ureter During Robot-Assisted Excision of Endometriosis. J. Minim. Invasive Gynecol. 2015, 22, S69. [Google Scholar] [CrossRef]
- Vizzielli, G.; Cosentino, F.; Raimondo, D.; Turco, L.C.; Vargiu, V.; Iodice, R.; Mastronardi, M.; Mabrouk, M.; Scambia, G.; Seracchioli, R. Real three-dimensional approach vs. two-dimensional camera with and without real-time near-infrared imaging with indocyanine green for detection of endometriosis: A case-control study. Acta Obstet. Gynecol. Scand. 2020, 99, 1330–1338. [Google Scholar] [CrossRef]
- De Neef, A.; Cadière, G.B.; Bourgeois, P.; Barbieux, R.; Dapri, G.; Fastrez, M. Fluorescence of deep infiltrating endometriosis during laparoscopic surgery: A preliminary report on 6 cases. Surg. Innov. 2018, 25, 450–454. [Google Scholar] [CrossRef]
- Mandovra, P.; Kalikar, V.; Patankar, R.V. Real-Time Visualization of Ureters Using Indocyanine Green During Laparoscopic Surgeries: Can We Make Surgery Safer? Surg. Innov. 2019, 26, 464–468. [Google Scholar] [CrossRef]
- Siegenthaler, F.; Knabben, L.; Mohr, S.; Nirgianakis, K.; Imboden, S.; Mueller, M.D. Visualization of endometriosis with laparoscopy and near-infrared optics with indocyanine green. Acta Obstet. Gynecol. Scand. 2020, 99, 591–597. [Google Scholar] [CrossRef]
- Bourdel, N.; Jaillet, L.; Bar-Shavit, Y.; Comptour, A.; Pereira, B.; Canis, M.; Chauvet, P. Indocyanine green in deep infiltrating endometriosis: A preliminary feasibility study to examine vascularization after rectal shaving. Fertil. Steril. 2020, 114, 367–373. [Google Scholar] [CrossRef]
- Beran, B.D.; Shockley, M.; Arnolds, K.; Escobar, P.; Zimberg, S.; Sprague, M.L. Laser Angiography with Indocyanine Green to Assess Vaginal Cuff Perfusion during Total Laparoscopic Hysterectomy: A Pilot Study. J. Minim. Invasive Gynecol. 2017, 24, 432–437. [Google Scholar] [CrossRef]
- Beran, B.D.; Shockley, M.; Padilla, P.F.; Farag, S.; Escobar, P.; Zimberg, S.; Sprague, M.L. Laser Angiography to Assess the Vaginal Cuff During Robotic Hysterectomy. JSLS 2018, 22, e2018.00001. [Google Scholar] [CrossRef]
- Bar-Shavit, Y.; Jaillet, L.; Chauvet, P.; Canis, M.; Bourdel, N. Use of indocyanine green in endometriosis surgery. Fertil. Steril. 2018, 109, 1136–1137. [Google Scholar] [CrossRef]
- Ianieri, M.M.; Della Corte, L.; Campolo, F.; Cosentino, F.; Catena, U.; Bifulco, G.; Scambia, G. Indocyanine green in the surgical management of endometriosis: A systematic review. Acta Obstet. Gynecol. Scand. 2021, 100, 189–199. [Google Scholar] [CrossRef]
- Son, G.M.; Kwon, M.S.; Kim, Y.; Kim, J.; Kim, S.H.; Lee, J.W. Quantitative analysis of colon perfusion pattern using indocyanine green (ICG) angiography in laparoscopic colorectal surgery. Surg. Endosc. 2019, 33, 1640–1649. [Google Scholar] [CrossRef]
- Spagnolo, E.; Hernández, A.; Pascual, I.; Cabanes, M.; López, A.; Zapardiel, I. Bowel and ureteral assessment by indocyanine green real-time visualization during deep infiltrating endometriosis surgery. Colorectal Dis. 2020, 22, 1464–1465. [Google Scholar] [CrossRef]
- Casals, G.; Carrera, M.; Domínguez, J.A.; Abrão, M.S.; Carmona, F. Impact of Surgery for Deep Infiltrative Endometriosis before In Vitro Fertilization: A Systematic Review and Meta-analysis. J. Minim. Invasive Gynecol. 2021, 28, 1303–1312.e5. [Google Scholar] [CrossRef] [PubMed]
- Duepree, H.J.; Senagore, A.J.; Delaney, C.P.; Marcello, P.W.; Brady, K.M.; Falcone, T. Laparoscopic resection of deep pelvic endometriosis with rectosigmoid involvement. J. Am. Coll. Surg. 2002, 195, 754–758. [Google Scholar] [CrossRef]
- Keckstein, J.; Wiesinger, H. Deep endometriosis, including intestinal involvement--the interdisciplinary approach. Minim. Invasive Ther. Allied Technol. 2005, 14, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Ruffo, G.; Scopelliti, F.; Scioscia, M.; Ceccaroni, M.; Mainardi, P.; Minelli, L. Laparoscopic colorectal resection for deep infiltrating endometriosis: Analysis of 436 cases. Surg. Endosc. 2010, 24, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Dubernard, G.; Piketty, M.; Rouzier, R.; Houry, S.; Bazot, M.; Darai, E. Quality of life after laparoscopic colorectal resection for endometriosis. Hum. Reprod. 2006, 21, 1243–1247. [Google Scholar] [CrossRef]
- Park, J.H.; Park, J.W.; Song, K.; Jo, M.K. Ureteral injury in gynecologic surgery: A 5-year review in a community hospital. Korean J. Urol. 2012, 53, 120–125. [Google Scholar] [CrossRef]
- Laschke, M.W.; Menger, M.D. Basic mechanisms of vascularization in endometriosis and their clinical implications. Hum. Reprod. Update 2018, 24, 207–222. [Google Scholar] [CrossRef]
- Potente, M.; Gerhardt, H.; Carmeliet, P. Basic and therapeutic aspects of angiogenesis. Cell 2011, 146, 873–887. [Google Scholar] [CrossRef]
- Asahara, T.; Kawamoto, A. Endothelial progenitor cells for postnatal vasculogenesis. Am. J. Physiol. Cell Physiol. 2004, 287, C572–C579. [Google Scholar] [CrossRef]
- Jafari, M.D.; Wexner, S.D.; Martz, J.E.; McLemore, E.C.; Margolin, D.A.; Sherwinter, D.A.; Lee, S.W.; Senagore, A.J.; Phelan, M.J.; Stamos, M.J. Perfusion assessment in laparoscopic left-sided/anterior resection (PILLAR II): A multi-institutional study. J. Am. Coll. Surg. 2015, 220, 82–92.e1. [Google Scholar] [CrossRef]
- Liu, D.; Liang, L.; Liu, L.; Zhu, Z. Does intraoperative indocyanine green fluorescence angiography decrease the incidence of anastomotic leakage in colorectal surgery? A systematic review and meta-analysis. Int. J. Colorectal Dis. 2021, 36, 57–66. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Field | ICG Application | Study | Country | Study Design | Sample Size | Study Period | Benign Gynecologic Condition Details | Study Outcomes |
|---|---|---|---|---|---|---|---|---|
| Endometriosis | To localize ureteral course | 2015 Park [20] | USA | Retrospective, observational, cohort study | 10 | 1 July 2014–30 March 2015 | DIE | Iatrogenic ureteral injury ICG complications Operative time Estimated blood loss Length of hospital stay |
| 2019 Mandovra [23] | India | Prospective, observational, cohort study | 30 | September 2017–December 2017 | DIE | Identification of ureters ICG complications Operative time ICG injection time | ||
| To assess ureteral perfusion after conservative surgery | 2020 Raimondo [1] | Italy | Prospective, observational case series | 36 | May 2018–January 2019 | DIE (Ureteral) | Ureteral perfusion grade NIR–ICG assessment time Inter-operator agreement regarding ureteral perfusion grade Changes to the surgical plan after NIR–ICG evaluation Perioperative complications Clinical-radiologic outcomes at early follow-up | |
| To improve endometriosis identification | 2018 Cosentino [7] | Italy | Prospective, observational, cohort, single center, single-arm, pilot study | 27 | January 2016–February 2017 | PE-DIE rARSM score -Stage I: 0 -Stage II: 3 -Stage III: 10 -Stage IV: 14 | Identified endometriosis lesions | |
| 2018 De Neef [22] | Belgium | Prospective, observational case series | 6 | - | RVDIE | Resection of RVDIEN Rectal perforations | ||
| 2019 Jayakumaran [12] | USA | Prospective, observational cohort study | 7 | July 2013–June 201 | DIE | Identified endometriosis lesions Quality of life | ||
| 2019 Lier [19] | The Netherlands | Prospective, single-center, randomized within subject clinical trial | 20 | February 2016–May 2017 | ASRM stage III–IV endometriosis | Detection of peritoneal endometriotic lesions | ||
| 2020 Siegenthaler [24] | Switzerland | Prospective, observational, cohort, single-center, single-arm pilot study | 63 | April 2017–December 2018 | PE-DIE No endometriosis: 9 (14.3) rARSM stage (%) -Stage I: 12 (19.0) -Stage II: 10 (15.9) -Stage III: 11 (17.5) -Stage IV: 20 (31.7) | Identified endometriosis lesions | ||
| 2020 Vizzielli [21] | Italy | Retrospective, observational, multicenter case-control study | 20 cases vs. 27 controls | January 2016–March 2018 | PE-DIE -Stage I: 0 -Stage II: 6 (13) -Stage III: 16 (34) -Stage IV: 25 (47) | Visual detection rate of endometriotic lesions | ||
| To evaluate the different RSE vascular patterns and the correlation with clinicopathological data | 2020 Raimondo [2] | Italy | Prospective, observational cohort pilot study | 30 | June 2019–September 2019 | DIE (RSE) | Perfusion grade of RSE Preoperative, intraoperative and pathological data | |
| To assess bowel vascularization after surgery to reduce the risk of fistula | 2020 Bourdel [25] | France | Prospective, observational, cohort, single-center, study | 23 | August 2017–October 2018 | Shaving technique for DIE infiltrating the rectovaginal septum | Fluorescence degree in the operated rectal area and in the vaginal Suture ICG adverse reactions Operative time Digestive fistula | |
| 2021 Raimondo [15] | Italy | Retrospective, observational, single-center, cohort, pilot study | 32 | May 2018–January 2020 | Full-thickness bowel resection for RSE | Fluorescence degree of the anastomotic lie ICG adverse reactions Operative time Anastomotic leakage | ||
| 2021 Raimondo [14] | Italy | Retrospective, multicentric, cohort, pilot study | 33 | November 2019–July 2020 | Full-thickness bowel resection for RSE | Accuracy of quantitative NIR–ICG evaluation in predicting bowel fistula Accuracy of qualitative NIR–ICG imaging in predicting bowel fistula Reproducibility of quantitative and qualitative NIR–ICG imaging | ||
| Non-endometriosis | To assess vascular perfusion of the vaginal cuff after total hysterectomy to decrease vaginal cuff dehiscence rate | 2017 Beran [26] | USA | Prospective, observational cohort, single-center, pilot study | 20 | 2 months | TLH for benign gynecologic condition | Vaginal cuff fluorescence rate Percent of cuff perimeter with adequate perfusion Length of vaginal cuff adequately perfused |
| 2018 Beran [27] | USA | Prospective, observational, cohort, single-center, study | 20 | February 2016–March 2017 | RATLH for benign gynecologic condition | Vaginal cuff perfusion | ||
| To intraoperatively evaluate ovarian perfusion after adnexal detorsion | 2022 Nicholson [16] | USA | Prospective, observational, cohort, multicenter, single-arm study | 12 | September 2018–December 2020 | Adnexal torsion | Feasibility of using ICG dye Intraoperative visualization of ICG perfusion to the detorsed adnexa Time to visualized perfusion Operative time Ovarian preservation Post operative follow-up measures |
| Field | ICG Application | Study | Age, Years [Median or Mean ± SD (Range)] | BMI, kg/m2 [Median or Mean ± SD (Range)] | Parity | Operative time, Minutes (min) [Median or Mean ± SD (Range)] | Follow up Time (Months) [Median or Mean ± SD (Range)] | Estimated Blood Loss (mL) [Median or Mean ± SD (Range)] | Indication for Surgery |
|---|---|---|---|---|---|---|---|---|---|
| Endometriosis | To localize ureteral course | 2015 Park [20] | 35 ± ns | 28 ± ns | 1.2 ± ns | 121 ± ns | 5.6 ± ns | 23 ± ns | Dysmenorrhea (9), dyspareunia (8), menorrhagia (7) pelvic pain (8), ovarian cysts (3), infertility (1) |
| 2019 Mandovra [23] | 46.7 (8–78) | 23.2 (21.6–32.1) | - | 138 (90–240) | - | - | - | ||
| To assess ureteral perfusion after conservative surgery | 2020 Raimondo [1] | 35.3 ± 6.8 | 24.9 ± 5.85 | 6 patients ≥ 1 | - | - | - | Pelvic pain (16), dysmenorrhea (12), dyspareunia (16), dyschezia (10) | |
| To improve endometriosis identification | 2018 Cosentino [7] | 37 (31.5–42.5) | 22 (21–24) | - | - | - | - | Dysmenorrhea (27), dyschezia (14), dysuria (5), dyspareunia (23), pelvic pain (22) | |
| 2018 De Neef [22] | - | - | - | - | 16 (2–23) | - | Symptomatic RVDIE | ||
| 2019 Jayakumaranet [12] | 33 ± 2.8 | 28.6 ± 3 | - | - | 1 | - | Endometriosis (3) | ||
| 2019 Lier [19] | 34.5 (29.3–39.5) | <25 (12 patients- 60%) 25–30 (8 patients 40%) | 0 (0–1) | 30 (30–37.5 min) | - | 50 (IQR: 27.5–100) | Dysmenorrhea (19), dyschezia (13), dysuria (1), dyspareunia (10) | ||
| 2020 Siegenthaler [24] | 33.7 ± 6.68 | 23.4 ± 4.19 | 4 patients ≥ 1 | 163.5 ± ns | - | 110.8 ± ns | Pelvic pain (45), infertility (4), both (13) | ||
| 2020 Vizzielli [21] | 37 (31–42) | 19 (19–24) | - | 150 (118–185) | 1 | 100 (50–250) | Dysmenorrhea (8), dyschezia (7), dysuria (8), dyspareunia (7), pelvic pain (7) | ||
| To evaluate the different RSE vascular patterns and the correlation with clinicopathological data | 2020 Raimondo [2] | 25 ± 5.8 | 35.4 ± 7.2 | 6 patients ≥ 1 | - | 3 | - | Dysmenorrhea (8), dyschezia (6) dyspareunia (6), pelvic pain (7), renal colic (2), hydroureter (6), hydroureteronephrosis (4) | |
| To assess bowel vascularization after surgery to reduce the risk of fistula | 2020 Bourdel [25] | 35 ± 6.7 | 25 (22.7–30.8) | - | 240 (180–254) | 3 | - | - | |
| 2021 Raimondo [15] | 36 ± 7 | 26 ± 6.4 | 8 patients ≥ 1 | 210 (95–300) | 3 | 125 (100–500) | Dysmenorrhea (8), dyschezia (6), dyspareunia (5), pelvic pain (7), rectorrhagia (1) | ||
| 2021 Raimondo [14] | 35.1 ± 6.2 | 22.8 ± 5.2 | 5 patients ≥ 1 | 180 (70–350) | 3 | 100 (10–150) | Dysmenorrhea (8), dyschezia (6), dyspareunia (6), pelvic pain (4) | ||
| Non-endometriosis | To assess vascular perfusion of the vaginal cuff after total hysterectomy to decrease vaginal cuff dehiscence rate | 2017 Beran [26] | 45.5 (32–68) | 30.4 (22.4–44.7) | 1.5 (0–4) | - | 3 | 150 (20–450) | Pelvic pain (4), AUB (17) |
| 2018 Beran [27] | 45 (31–64) | 28.0 (21.1–43.6) | 2 (0–3) | - | 3 | 65.5 (25–400) | AUB (10), Pelvic pain (5), cervical dysplasia (3), Lynch syndrome (1), postmenopausal bleeding (1) | ||
| To intraoperatively evaluate ovarian perfusion after adnexal detorsion | 2022 Nicholson [16] | 27 (25–31) | - | - | 73.4 (48–94) | 1 | - | Suspected adnexal torsion | |
| TOTAL | - | - | 25–36 (mean) | 22.8–35.4 (mean) | 14.9% patients ≥ 1 | 121–163.5 (mean) | 1–23 (n) | 50–150 (median) | 43.8% dysmenorrhea 27.6% dyschezia 14.9% dysuria 34.5% dyspareunia 39.3% pelvic pain 30.0% ovarian cysts 6.8% infertility 20.6% pelvic pain and infertility 6.7% renal colic 20.0% hydroureter 13.3% hydroureteronephrosis 3.1% rectorrhagia 42.5% AUB 15.0% cervical dysplasia 5.0% Lynch syndrome 5.0% postmenopausal bleeding 26.7% menorrhagia |
| Field | ICG Application | Study | Surgical Procedure and Detection System of Fluorescence | Indocyanine Dosage and Injection Method | Time to ICG Visualization in Minutes [Median or Mean ± SD (Range)] | Type of Surgery |
|---|---|---|---|---|---|---|
| Endometriosis | To localize ureteral course | 2015 Park [20] | Robotic-assisted laparoscopy | - intraurethral | - | Resection of deep infiltrating endometriosis, ureterolysis and bilateral ureteral stent placement and removal |
| 2019 Mandovra [23] | Laparoscopy | 5 mg ICG diluted in 2 mL of distilled water–cystoscopy and ureteric cannulation | 7 (6–9) | Ventral mesh rectopexy Rectopexy Sacrocolpopexy Anterior resection Sigmoid colectomy Right hemicolectomy Total colectomy Hysterectomy Endometriotic cyst excision | ||
| To assess ureteral perfusion after conservative surgery | 2020 Raimondo [1] | Laparoscopy | 0.25 mg/kg-intravenous | 5.4 ± 2.3 | Removal of deep endometriotic lesions of the posterior and anterior compartments | |
| To improve endometriosis identification | 2018 Cosentino [7] | Laparoscopy | 0.25 mg/kg-intravenous | 5–30 | - | |
| 2018 De Neef [22] | Laparoscopy | 0.25 mg/kg-intravenous | - | Laparoscopic shaving | ||
| 2019 Jayakumara [12] | Robotic-assisted laparoscopy | 0.25 mg/kg-intravenous | - | Robotic endometriosis resection | ||
| 2019 Lier [19] | Laparoscopy | Bolo of 1 mL-intravenous | 5 ± ns | - | ||
| 2020 Siegenthaler [24] | Laparoscopy | 0.3 mg/kg-intravenous 25 mg-intraurethral | 2–20 | - | ||
| 2020 Vizzielli [21] | Robotic-assisted laparoscopy and Laparoscopy | 0.25 mg/kg-intravenous | 15–30 | Ovarian cyst removal Peritoneal removal Retrocervical nodule removal Vaginal nodule removal Utero-sacral ligament nodule removal Rectal nodule shaving Resection and anastomosis of sigma-rectum Resection and anastomosis of sigma-rectum plus loop ileostomy Discoid resection of bowel Appendicectomy Salpingectomy Ureteral stent placement, bladder surgery | ||
| To evaluate the different RSE vascular patterns and the correlation with clinicopathological data | 2020 Raimondo [2] | Robotic-assisted laparoscopy and Laparoscopy | 0.25 mg/kg-intravenous | (5–50) s | RSE: Shaving, Discoid resection, Segmental resect | |
| To assess bowel vascularization after surgery to reduce the risk of fistula | 2020 Bourdel [25] | Laparoscopic | 0.2 mg/kg-intravenous | 60 (45–60) s | Rectal shaving | |
| 2021 Raimondo [15] | Laparoscopy | 0.25 mg/kg-intravenous | 33 (6−41) s | Discoid excision and segmental resection Hysterectomy Salpingectomy Ovariectomy Protective ileostomy | ||
| 2021 Raimondo [14] | Laparoscopy | 0.25 mg/kg-intravenous | 30 (9–43) s | Discoid excision and segmental resection Hysterectomy Salpingectomy | ||
| Non-endometriosis | To assess vascular perfusion of the vaginal cuff after total hysterectomy to decrease vaginal cuff dehiscence rate | 2017 Beran [26] | Laparoscopy | 25 mg + 2.5/5 mg-intravenous | 11 s | Total laparoscopic hysterectomy |
| 2018 Beran [27] | Robotic-assisted laparoscopy | 2.5–10.0 mg followed by a 10 mL saline flush-intravenous | 18.4 ± 7.3 s before cuff closure 19 ± 8.7 after cuff closure | Robot-assisted total laparoscopic hysterectomy | ||
| To intraoperatively evaluate ovarian perfusion after adnexal detorsion | 2022 Nicholson [16] | Laparoscopy | 8–20 cc-intravenous | 1 (1–2) | Adnexal detorsion-annessectomy |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raffone, A.; Raimondo, D.; Oliviero, A.; Raspollini, A.; Travaglino, A.; Torella, M.; Riemma, G.; La Verde, M.; De Franciscis, P.; Casadio, P.; et al. The Use of near Infra-Red Radiation Imaging after Injection of Indocyanine Green (NIR–ICG) during Laparoscopic Treatment of Benign Gynecologic Conditions: Towards Minimalized Surgery. A Systematic Review of Literature. Medicina 2022, 58, 792. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58060792
Raffone A, Raimondo D, Oliviero A, Raspollini A, Travaglino A, Torella M, Riemma G, La Verde M, De Franciscis P, Casadio P, et al. The Use of near Infra-Red Radiation Imaging after Injection of Indocyanine Green (NIR–ICG) during Laparoscopic Treatment of Benign Gynecologic Conditions: Towards Minimalized Surgery. A Systematic Review of Literature. Medicina. 2022; 58(6):792. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58060792
Chicago/Turabian StyleRaffone, Antonio, Diego Raimondo, Alessia Oliviero, Arianna Raspollini, Antonio Travaglino, Marco Torella, Gaetano Riemma, Marco La Verde, Pasquale De Franciscis, Paolo Casadio, and et al. 2022. "The Use of near Infra-Red Radiation Imaging after Injection of Indocyanine Green (NIR–ICG) during Laparoscopic Treatment of Benign Gynecologic Conditions: Towards Minimalized Surgery. A Systematic Review of Literature" Medicina 58, no. 6: 792. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58060792