
Differences between Very Highly Sensitized Kidney Transplant Recipients as Identified by Machine Learning Consensus Clustering
 , , , ,
, , , ,  , ,
, ,  ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
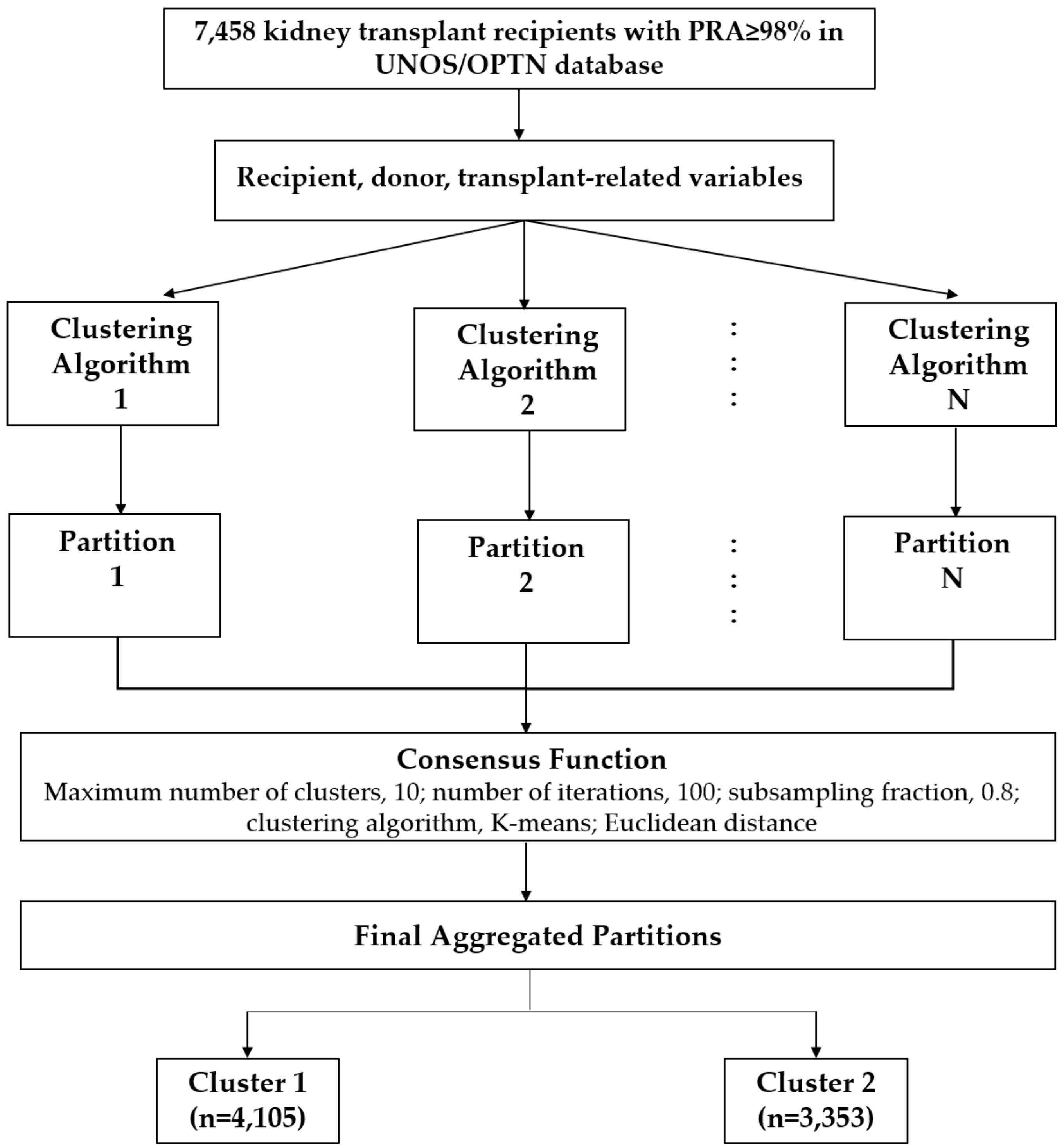
2.1. Data Source and Study Population
2.2. Data Collection
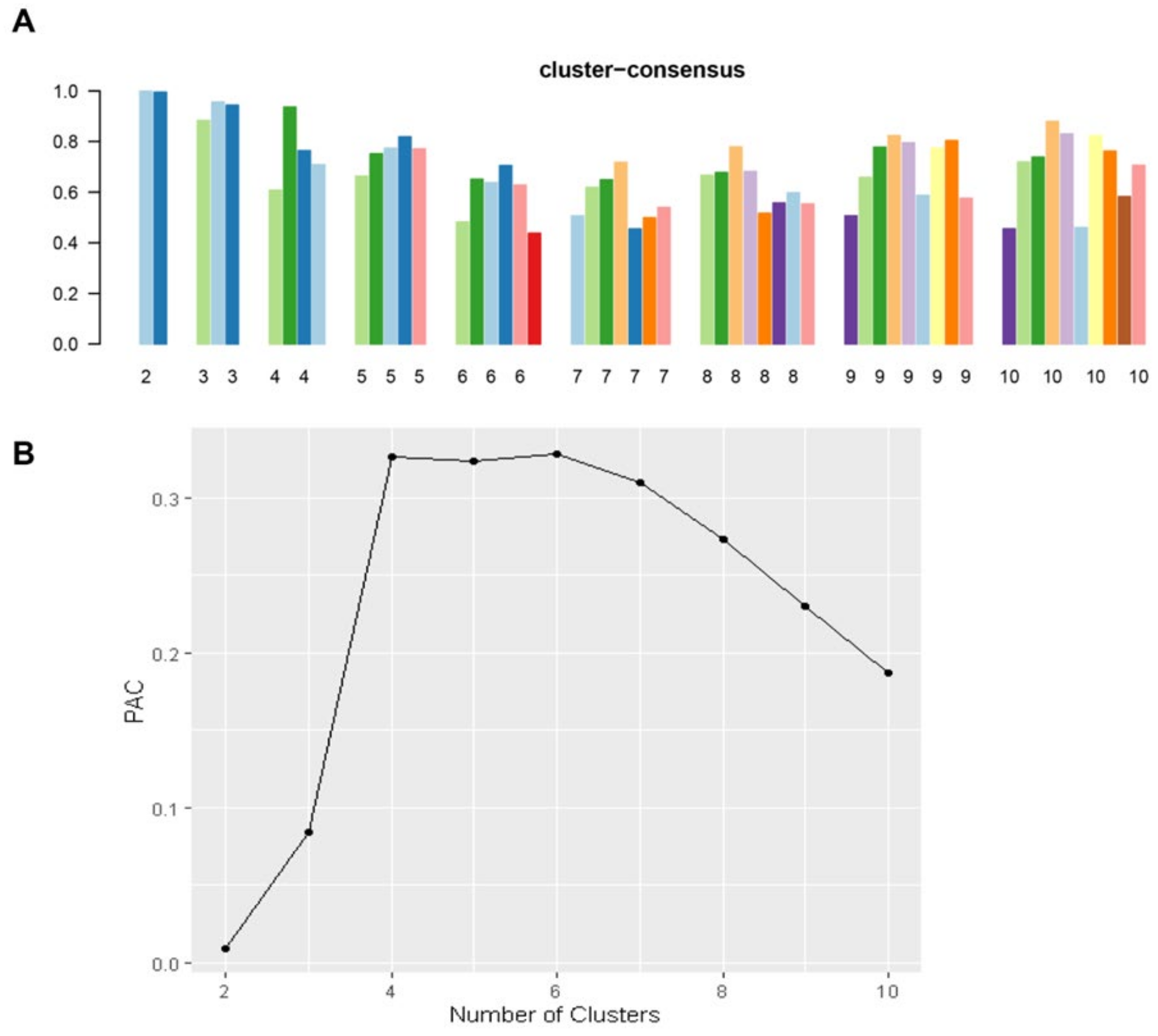
2.3. Clustering Analysis
2.4. Outcomes
2.5. Statistical Analysis
3. Results

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All (n = 7458) | Cluster 1 (n = 4105) | Cluster 2 (n = 3353) | p-Value | |
|---|---|---|---|---|
| Recipient age (year), median (IQR) | 49 (39–58) | 45 (35–54) | 54 (45–62) | <0.001 |
| Recipient male sex | 2697 (36) | 2409 (59) | 288 (9) | <0.001 |
Recipient race
| 2979 (40) 2321 (31) 1486 (20) 672 (9) | 1803 (44) 1249 (30) 736 (18) 317 (8) | 1176 (35) 1072 (32) 750 (22) 355 (11) | <0.001 |
| Body mass index (kg/m2), median (IQR) | 26.7 (23.0–31.2) | 25.7 (22.5–30.0) | 28.0 (24.0–32.4) | <0.001 |
| Retransplant | 4139 (56) | 4032 (98) | 107 (3) | <0.001 |
Dialysis duration
| 713 (10) 644 (9) 2037 (27) 4064 (54) | 240 (6) 299 (7) 1098 (27) 2468 (60) | 473 (14) 345 (10) 939 (28) 1596 (48) | <0.001 |
Cause of end-stage kidney disease
| 1095 (15) 1072 (14) 1452 (19) 456 (6) 3383 (45) | 130 (3) 338 (8) 690 (17) 105 (3) 2842 (69) | 965 (29) 734 (22) 762 (23) 351 (10) 541 (16) | <0.001 |
Comorbidity
| 1858 (25) 602 (8) 532 (7) | 686 (17) 342 (8) 232 (6) | 1172 (35) 260 (8) 300 (9) | <0.001 0.363 <0.001 |
PRA (%)
| 1081 (15) 2129 (29) 4248 (57) | 449 (11) 1010 (25) 2646 (65) | 632 (19) 1119 (33) 1602 (48) | <0.001 |
| Positive HCV serostatus | 344 (5) | 193 (5) | 151 (5) | 0.685 |
| Positive HBs antigen | 101 (1) | 62 (2) | 39 (1) | 0.197 |
| Positive HIV serostatus | 28 (0) | 20 (0) | 8 (0) | 0.081 |
Functional status
| 8 (0) 3374 (45) 4076 (55) | 4 (0) 1761 (43) 2340 (57) | 4 (0) 1613 (48) 1736 (52) | <0.001 |
| Working income | 2227 (30) | 1361 (33) | 866 (26) | <0.001 |
| Public insurance | 5730 (77) | 3313 (81) | 2417 (72) | <0.001 |
| U.S. resident | 7368 (99) | 4078 (99) | 3290 (98) | <0.001 |
| Undergraduate education or above | 4035 (54) | 2338 (57) | 1697 (51) | <0.001 |
| Serum albumin (g/dL), mean (SD) | 3.9 ± 0.6 | 3.9 ± 0.6 | 3.9 ± 0.6 | 0.483 |
Kidney donor status
| 6508 (87) 384 (5) 566 (8) | 3633 (89) 185 (5) 287 (7) | 2875 (86) 199 (6) 279 (8) | 0.001 |
| ABO incompatibility | 13 (0) | 9 (0) | 4 (0) | 0.303 |
| Donor age (year), median (IQR) | 35 (24–47) | 33 (23–45) | 36 (25–47) | <0.001 |
| Donor male sex | 4528 (61) | 2549 (62) | 1979 (59) | 0.007 |
Donor race
| 4676 (63) 1158 (16) 1279 (17) 345 (5) | 2605 (63) 617 (15) 694 (17) 189 (5) | 2071 (62) 541 (16) 585 (17) 156 (5) | 0.454 |
| History of hypertension in donor | 1409 (19) | 712 (17) | 697 (21) | <0.001 |
KDPI
| 566 (8) 6759 (91) 133 (2) | 287 (7) 3764 (92) 54 (1) | 279 (8) 2995 (89) 79 (2) | <0.001 |
| HLA mismatch, median (IQR) | 3 (2–4) | 3 (1–4) | 3 (2–4) | <0.001 |
| Cold ischemia time (hour), median (IQR) | 18.5 (13.2–23.8) | 19.0 (13.9–24.1) | 17.8 (12.3–23.2) | <0.001 |
| Kidney on pump | 2123 (28) | 1146 (28) | 977 (29) | 0.245 |
| Delay graft function | 1900 (25) | 1248 (30) | 652 (19) | <0.001 |
Allocation type
| 2211 (30) 1729 (23) 3518 (47) | 1070 (26) 886 (22) 2149 (52) | 1141 (34) 843 (25) 1369 (41) | <0.001 |
EBV status
| 48 (1) 6734 (90) 676 (9) | 26 (1) 3713 (90) 366 (9) | 22 (1) 3021 (90) 310 (9) | 0.878 |
CMV status
| 841 (11) 2135 (29) 1085 (15) 3397 (46) | 508 (12) 1192 (29) 663 (16) 1742 (42) | 333 (10) 943 (28) 422 (13) 1655 (49) | <0.001 |
Induction immunosuppression
| 2432 (73) 1125 (15) 468 (6) 91 (1) 490 (7) | 3035 (74) 633 (15) 221 (5) 60 (1) 258 (6) | 2432 (73) 492 (15) 247 (7) 31 (1) 232 (7) | 0.173 0.370 <0.001 0.036 0.272 |
Maintenance Immunosuppression
| 6937 (93) 84 (1) 6972 (93) 17 (0) 35 (0) 5995 (80) | 3789 (92) 62 (2) 3806 (93) 8 (0) 21 (1) 3345 (81) | 3148 (94) 22 (1) 3166 (94) 9 (0) 14 (0) 2650 (79) | 0.008 0.001 0.003 0.508 0.554 0.008 |
3.1. Clinical Characteristics Based on Clusters of Very Highly Sensitized Kidney Transplant Patients
3.2. Post-Transplant Outcomes Based on Clusters of Very Highly Sensitized Kidney Transplant Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- De Sousa-Amorim, E.; Revuelta, I.; Blasco, M.; Diekmann, F.; Cid, J.; Lozano, M.; Sanchez-Escuredo, A.; Martorell, J.; Palou, E.; Campistol, J.M.; et al. Desensitization Before Living Donor Kidney Transplantation in Highly HLA-Sensitized Patients: A Single-Center Study. Transplant. Proc. 2015, 47, 2332–2335. [Google Scholar] [CrossRef]
- Abecassis, M.; Bartlett, S.T.; Collins, A.J.; Davis, C.L.; Delmonico, F.L.; Friedewald, J.J.; Hays, R.; Howard, A.; Jones, E.; Leichtman, A.B.; et al. Kidney transplantation as primary therapy for end-stage renal disease: A National Kidney Foundation/Kidney Disease Outcomes Quality Initiative (NKF/KDOQITM) conference. Clin. J. Am. Soc. Nephrol. 2008, 3, 471–480. [Google Scholar] [CrossRef]
- Mamode, N.; Bestard, O.; Claas, F.; Furian, L.; Griffin, S.; Legendre, C.; Pengel, L.; Naesens, M. European Guideline for the Management of Kidney Transplant Patients with HLA Antibodies: By the European Society for Organ Transplantation Working Group. Transpl. Int. 2022, 35, 10511. [Google Scholar] [CrossRef] [PubMed]
- Dunn, T.B.; Noreen, H.; Gillingham, K.; Maurer, D.; Ozturk, O.G.; Pruett, T.L.; Bray, R.A.; Gebel, H.M.; Matas, A.J. Revisiting traditional risk factors for rejection and graft loss after kidney transplantation. Am. J. Transplant. 2011, 11, 2132–2143. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.; Ko, E.J.; Chung, B.H.; Yang, C.W. Kidney transplantation in highly sensitized recipients. Kidney Res. Clin. Pract. 2021, 40, 355–370. [Google Scholar] [CrossRef] [PubMed]
- Bray, R.A.; Gebel, H.M. The new kidney allocation system (KAS) and the highly sensitized patient: Expect the unexpected. Am. J. Transplant. 2014, 14, 2917. [Google Scholar] [CrossRef]
- Jordan, S.C.; Choi, J.; Vo, A. Kidney transplantation in highly sensitized patients. Br. Med. Bull. 2015, 114, 113–125. [Google Scholar] [CrossRef] [PubMed]
- Heidt, S.; Claas, F.H.J. Transplantation in highly sensitized patients: Challenges and recommendations. Expert. Rev. Clin. Immunol. 2018, 14, 673–679. [Google Scholar] [CrossRef] [PubMed]
- Thongprayoon, C.; Kattah, A.G.; Mao, M.A.; Keddis, M.T.; Pattharanitima, P.; Vallabhajosyula, S.; Nissaisorakarn, V.; Erickson, S.B.; Dillon, J.J.; Garovic, V.D.; et al. Distinct phenotypes of hospitalized patients with hyperkalemia by machine learning consensus clustering and associated mortality risks. Qjm Int. J. Med. 2022, 115, 442–449. [Google Scholar] [CrossRef]
- Zheng, Z.; Waikar, S.S.; Schmidt, I.M.; Landis, J.R.; Hsu, C.Y.; Shafi, T.; Feldman, H.I.; Anderson, A.H.; Wilson, F.P.; Chen, J.; et al. Subtyping CKD Patients by Consensus Clustering: The Chronic Renal Insufficiency Cohort (CRIC) Study. J. Am. Soc. Nephrol. 2021, 32, 639–653. [Google Scholar] [CrossRef]
- Thongprayoon, C.; Kaewput, W.; Kovvuru, K.; Hansrivijit, P.; Kanduri, S.R.; Bathini, T.; Chewcharat, A.; Leeaphorn, N.; Gonzalez-Suarez, M.L.; Cheungpasitporn, W. Promises of Big Data and Artificial Intelligence in Nephrology and Transplantation. J. Clin. Med. 2020, 9, 1107. [Google Scholar] [CrossRef] [PubMed]
- Wilkerson, M.D.; Hayes, D.N. ConsensusClusterPlus: A class discovery tool with confidence assessments and item tracking. Bioinformatics 2010, 26, 1572–1573. [Google Scholar] [CrossRef] [PubMed]
- MacEachern, S.J.; Forkert, N.D. Machine learning for precision medicine. Genome 2021, 64, 416–425. [Google Scholar] [CrossRef]
- Kampaktsis, P.N.; Tzani, A.; Doulamis, I.P.; Moustakidis, S.; Drosou, A.; Diakos, N.; Drakos, S.G.; Briasoulis, A. State-of-the-art machine learning algorithms for the prediction of outcomes after contemporary heart transplantation: Results from the UNOS database. Clin. Transplant. 2021, 35, e14388. [Google Scholar] [CrossRef] [PubMed]
- Killian, M.O.; Payrovnaziri, S.N.; Gupta, D.; Desai, D.; He, Z. Machine learning-based prediction of health outcomes in pediatric organ transplantation recipients. JAMIA Open 2021, 4, ooab008. [Google Scholar] [CrossRef] [PubMed]
- Ershoff, B.D.; Lee, C.K.; Wray, C.L.; Agopian, V.G.; Urban, G.; Baldi, P.; Cannesson, M. Training and Validation of Deep Neural Networks for the Prediction of 90-Day Post-Liver Transplant Mortality Using UNOS Registry Data. Transplant. Proc. 2020, 52, 246–258. [Google Scholar] [CrossRef]
- Wadhwani, S.I.; Hsu, E.K.; Shaffer, M.L.; Anand, R.; Ng, V.L.; Bucuvalas, J.C. Predicting ideal outcome after pediatric liver transplantation: An exploratory study using machine learning analyses to leverage Studies of Pediatric Liver Transplantation Data. Pediatr. Transplant. 2019, 23, e13554. [Google Scholar] [CrossRef] [PubMed]
- Schwantes, I.R.; Axelrod, D.A. Technology-Enabled Care and Artificial Intelligence in Kidney Transplantation. Curr. Transplant. Rep. 2021, 8, 235–240. [Google Scholar] [CrossRef]
- Thongprayoon, C.; Vaitla, P.; Jadlowiec, C.C.; Leeaphorn, N.; Mao, S.A.; Mao, M.A.; Pattharanitima, P.; Bruminhent, J.; Khoury, N.J.; Garovic, V.D.; et al. Use of Machine Learning Consensus Clustering to Identify Distinct Subtypes of Black Kidney Transplant Recipients and Associated Outcomes. JAMA Surg. 2022, 157, e221286. [Google Scholar] [CrossRef]
- van Buuren, S.; Groothuis-Oudshoorn, K. mice: Multivariate Imputation by Chained Equations in R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar] [CrossRef]
- Monti, S.; Tamayo, P.; Mesirov, J.; Golub, T. Consensus Clustering: A Resampling-Based Method for Class Discovery and Visualization of Gene Expression Microarray Data. Mach. Learn. 2003, 52, 91–118. [Google Scholar] [CrossRef]
- Șenbabaoğlu, Y.; Michailidis, G.; Li, J.Z. Critical limitations of consensus clustering in class discovery. Sci. Rep. 2014, 4, 6207. [Google Scholar] [CrossRef]
- Lee, C.Y.; Yang, C.Y.; Lin, W.C.; Chen, C.C.; Tsai, M.K. Prognostic factors for renal transplant graft survival in a retrospective cohort of 1000 cases: The role of desensitization therapy. J. Formos. Med. Assoc. 2020, 119, 829–837. [Google Scholar] [CrossRef]
- Grafals, M.; Chandraker, A. New approaches for desensitization strategies prior to kidney transplantation. Am. J. Kidney Dis. 2009, 53, 370–372. [Google Scholar] [CrossRef]
- Loupy, A.; Hill, G.S.; Jordan, S.C. The impact of donor-specific anti-HLA antibodies on late kidney allograft failure. Nat. Rev. Nephrol. 2012, 8, 348–357. [Google Scholar] [CrossRef]
- Stegall, M.D.; Gloor, J.; Winters, J.L.; Moore, S.B.; Degoey, S. A comparison of plasmapheresis versus high-dose IVIG desensitization in renal allograft recipients with high levels of donor specific alloantibody. Am. J. Transplant. 2006, 6, 346–351. [Google Scholar] [CrossRef]
- Lefaucheur, C.; Loupy, A.; Hill, G.S.; Andrade, J.; Nochy, D.; Antoine, C.; Gautreau, C.; Charron, D.; Glotz, D.; Suberbielle-Boissel, C. Preexisting donor-specific HLA antibodies predict outcome in kidney transplantation. J. Am. Soc. Nephrol. 2010, 21, 1398–1406. [Google Scholar] [CrossRef]
- Redfield, R.R.; Scalea, J.R.; Zens, T.J.; Mandelbrot, D.A.; Leverson, G.; Kaufman, D.B.; Djamali, A. The mode of sensitization and its influence on allograft outcomes in highly sensitized kidney transplant recipients. Nephrol. Dial. Transplant. 2016, 31, 1746–1753. [Google Scholar] [CrossRef]
- Aufhauser, D.D., Jr.; Peng, A.W.; Murken, D.R.; Concors, S.J.; Abt, P.L.; Sawinski, D.; Bloom, R.D.; Reese, P.P.; Levine, M.H. Impact of prolonged dialysis prior to renal transplantation. Clin. Transplant. 2018, 32, e13260. [Google Scholar] [CrossRef]
- Lum, E.L.; Homkrailas, P.; Abdalla, B.; Danovitch, G.M.; Bunnapradist, S. Cold Ischemia Time, Kidney Donor Profile Index, and Kidney Transplant Outcomes: A Cohort Study. Kidney Med. 2023, 5, 100570. [Google Scholar] [CrossRef]
- Jackson, K.R.; Motter, J.D.; Kernodle, A.; Desai, N.; Thomas, A.G.; Massie, A.B.; Garonzik-Wang, J.M.; Segev, D.L. How do highly sensitized patients get kidney transplants in the United States? Trends over the last decade. Am. J. Transplant. 2020, 20, 2101–2112. [Google Scholar] [CrossRef] [PubMed]
- Continuous Distribution—Kidney and Pancreas. Available online: https://optn.transplant.hrsa.gov/policies-bylaws/a-closer-look/continuous-distribution/continuous-distribution-kidney-and-pancreas/ (accessed on 19 February 2023).





| Cluster 1 | Cluster 2 | |
|---|---|---|
| 1-year survival | 97.3% | 97.1% |
| HR for 1-year death | 0.93 (0.69–1.24) | 1 (ref) |
| 5-year survival | 88.0% | 86.5% |
| HR for 5-year survival | 0.88 (0.73–1.06) | 1 (ref) |
| 1-year death-censored graft survival | 96.3% | 97.6% |
| HR for 1-year death-censored graft failure | 1.57 (1.18–2.09) | 1 (ref) |
| 5-year death-censored graft survival | 84.4% | 85.5% |
| HR for 5-year death-censored graft failure | 1.28 (1.07–1.54) | 1 (ref) |
| 1-year acute rejection | 9.2% | 5.4% |
| OR for 1-year acute rejection | 1.78 (1.48–2.14) | 1 (ref) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thongprayoon, C.; Miao, J.; Jadlowiec, C.C.; Mao, S.A.; Mao, M.A.; Vaitla, P.; Leeaphorn, N.; Kaewput, W.; Pattharanitima, P.; Tangpanithandee, S.; et al. Differences between Very Highly Sensitized Kidney Transplant Recipients as Identified by Machine Learning Consensus Clustering. Medicina 2023, 59, 977. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina59050977
Thongprayoon C, Miao J, Jadlowiec CC, Mao SA, Mao MA, Vaitla P, Leeaphorn N, Kaewput W, Pattharanitima P, Tangpanithandee S, et al. Differences between Very Highly Sensitized Kidney Transplant Recipients as Identified by Machine Learning Consensus Clustering. Medicina. 2023; 59(5):977. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina59050977
Chicago/Turabian StyleThongprayoon, Charat, Jing Miao, Caroline C. Jadlowiec, Shennen A. Mao, Michael A. Mao, Pradeep Vaitla, Napat Leeaphorn, Wisit Kaewput, Pattharawin Pattharanitima, Supawit Tangpanithandee, and et al. 2023. "Differences between Very Highly Sensitized Kidney Transplant Recipients as Identified by Machine Learning Consensus Clustering" Medicina 59, no. 5: 977. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina59050977