


Feasibility and Efficacy of Morning Light Therapy for Adults with Insomnia: A Pilot, Randomized, Open-Label, Two-Arm Study
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
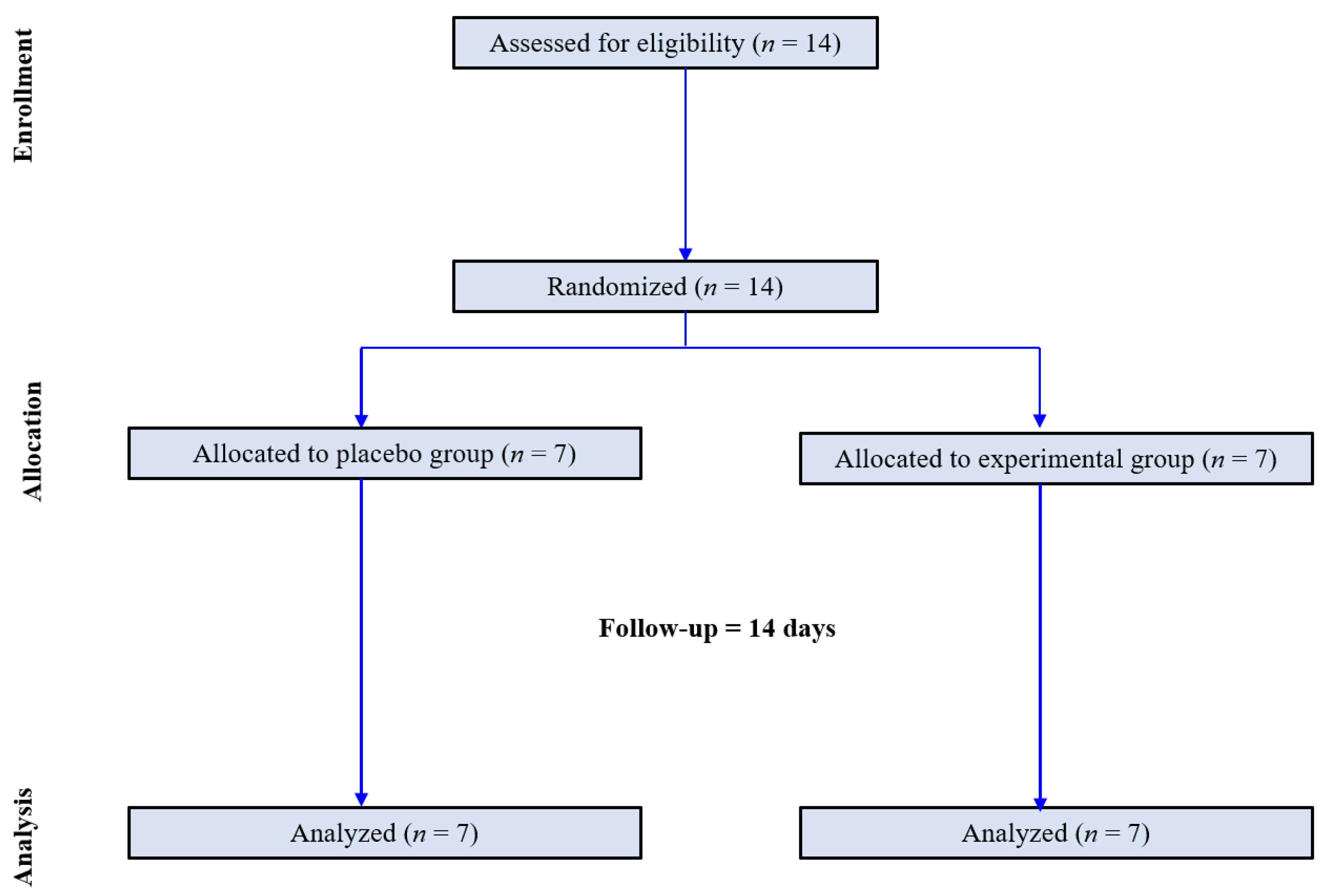
2.1. Study Design and Patients
2.2. Randomization and Study Protocol
2.3. Clinical and Biochemistry Analyses
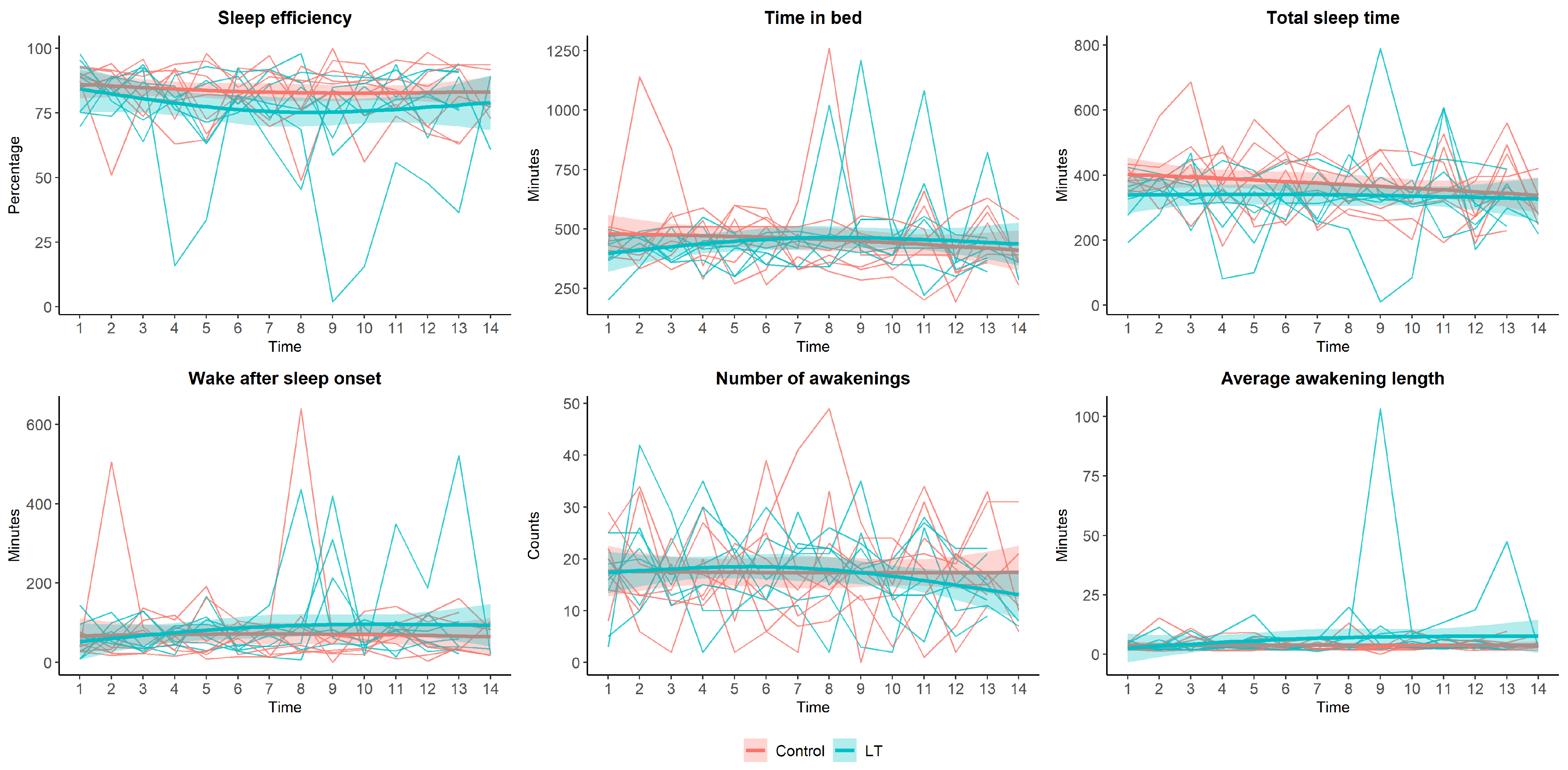
2.4. Actigraphy
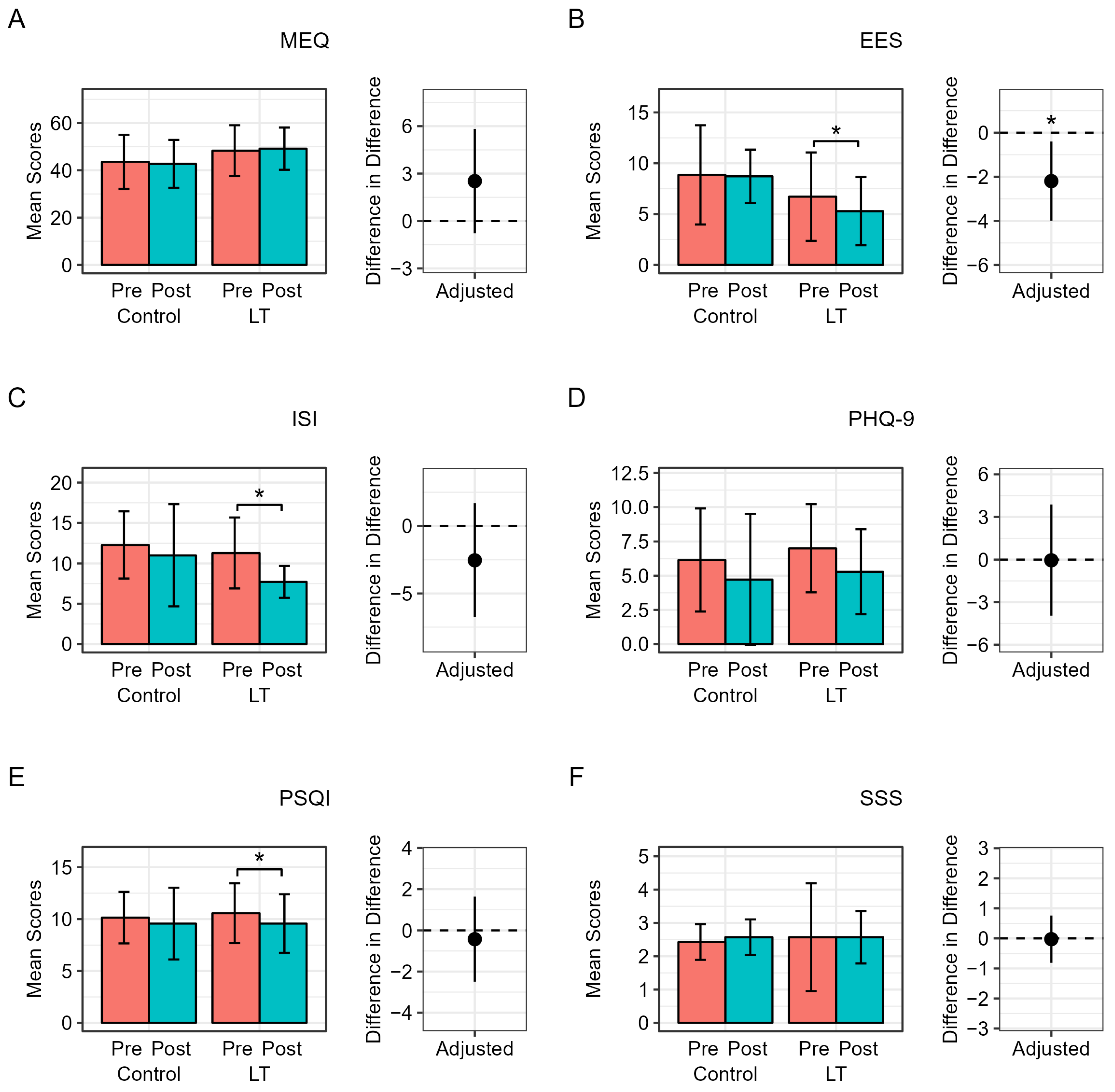
2.5. Sleep-Related Questionnaire
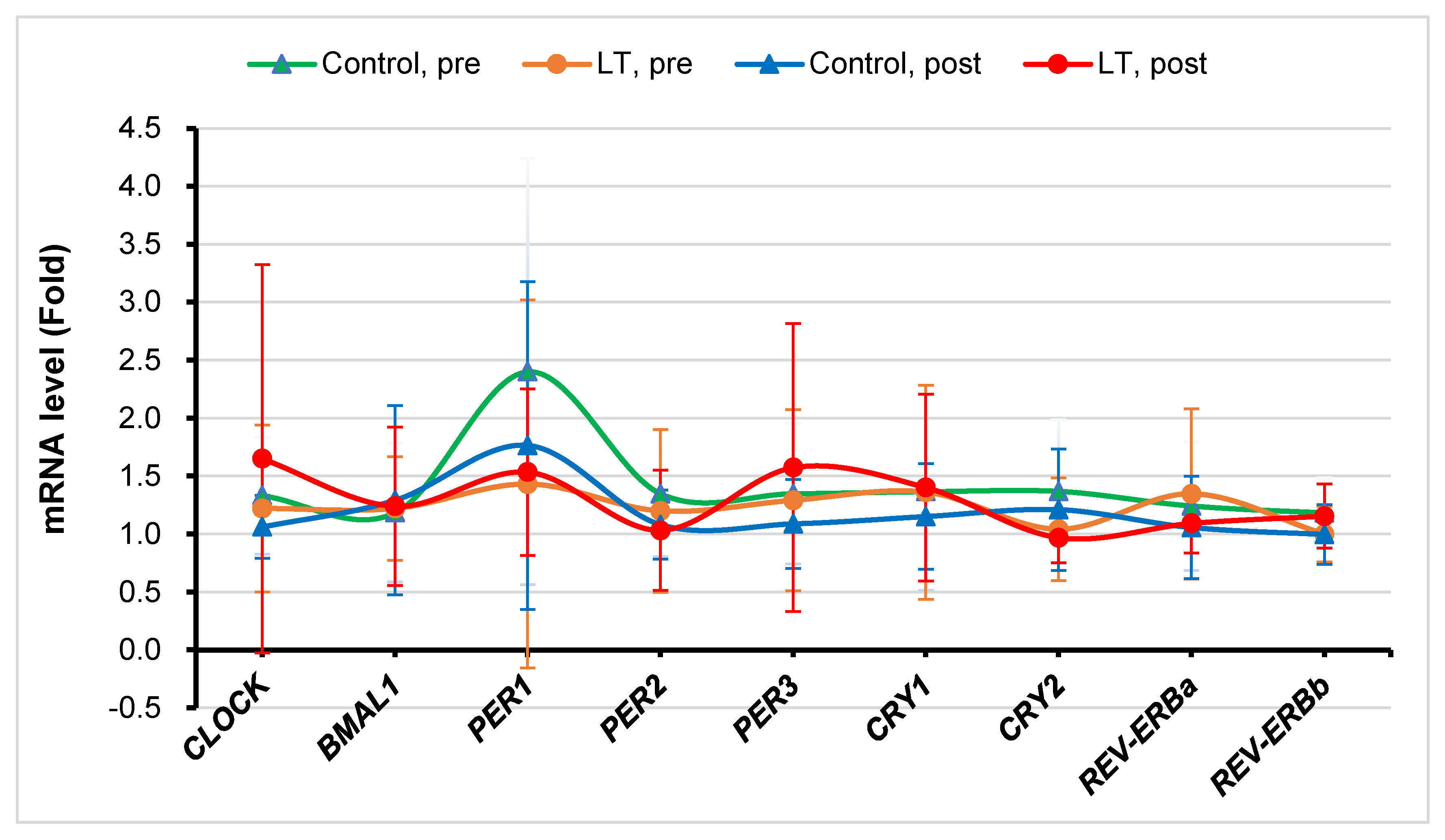
2.6. Real-Time Reverse Transcription Polymerase Chain Reaction (RT-PCR) Analysis of Clock Genes
2.7. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Changes in Biochemical and Physical Parameters
3.3. Changes in Sleep Patterns and Quality
3.4. Changes in Clock Genes’ Expression
3.5. Compliance and Safety
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Grandner, M.A.; Pack, A.I. Sleep disorders, public health, and public safety. JAMA 2011, 306, 2616–2617. [Google Scholar] [CrossRef] [PubMed]
- Silvestri, R.; Aricò, I. Sleep disorders in pregnancy. Sleep Sci. 2019, 12, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, A.N.; Walker, M.P. The role of sleep in emotional brain function. Annu. Rev. Clin. Psychol. 2014, 10, 679–708. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Berglund, P.A.; Coulouvrat, C.; Hajak, G.; Roth, T.; Shahly, V.; Shillington, A.C.; Stephenson, J.J.; Walsh, J.K. Insomnia and the performance of us workers: Results from the america insomnia survey. Sleep 2011, 34, 1161–1171. [Google Scholar] [CrossRef]
- Vgontzas, A.N.; Liao, D.; Bixler, E.O.; Chrousos, G.P.; Vela-Bueno, A. Insomnia with objective short sleep duration is associated with a high risk for hypertension. Sleep 2009, 32, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Nagai, M.; Hoshide, S.; Kario, K. Sleep duration as a risk factor for cardiovascular disease—A review of the recent literature. Curr. Cardiol. Rev. 2010, 6, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Cappuccio, F.P.; D’Elia, L.; Strazzullo, P.; Miller, M.A. Quantity and quality of sleep and incidence of type 2 diabetes: A systematic review and meta-analysis. Diabetes Care 2010, 33, 414–420. [Google Scholar] [CrossRef] [PubMed]
- Ayas, N.T.; White, D.P.; Al-Delaimy, W.K.; Manson, J.E.; Stampfer, M.J.; Speizer, F.E.; Patel, S.; Hu, F.B. A prospective study of self-reported sleep duration and incident diabetes in women. Diabetes Care 2003, 26, 380–384. [Google Scholar] [CrossRef]
- Gottlieb, D.J.; Punjabi, N.M.; Newman, A.B.; Resnick, H.E.; Redline, S.; Baldwin, C.M.; Nieto, F.J. Association of sleep time with diabetes mellitus and impaired glucose tolerance. Arch. Intern. Med. 2005, 165, 863–867. [Google Scholar] [CrossRef]
- Jiao, L.; Duan, Z.; Sangi-Haghpeykar, H.; Hale, L.; White, D.L.; El-Serag, H.B. Sleep duration and incidence of colorectal cancer in postmenopausal women. Br. J. Cancer 2013, 108, 213–221. [Google Scholar] [CrossRef]
- Spira, A.P.; Chen-Edinboro, L.P.; Wu, M.N.; Yaffe, K. Impact of sleep on the risk of cognitive decline and dementia. Curr. Opin. Psychiatry 2014, 27, 478–483. [Google Scholar] [CrossRef]
- Sabia, S.; Fayosse, A.; Dumurgier, J.; van Hees, V.T.; Paquet, C.; Sommerlad, A.; Kivimäki, M.; Dugravot, A.; Singh-Manoux, A. Association of sleep duration in middle and old age with incidence of dementia. Nat. Commun. 2021, 12, 2289. [Google Scholar] [CrossRef]
- Lapierre, S.; Boyer, R.; Desjardins, S.; Dubé, M.; Lorrain, D.; Préville, M.; Brassard, J. Daily hassles, physical illness, and sleep problems in older adults with wishes to die. Int. Psychogeriatr. 2012, 24, 243–252. [Google Scholar] [CrossRef] [PubMed]
- Morin, C.M.; LeBlanc, M.; Bélanger, L.; Ivers, H.; Mérette, C.; Savard, J. Prevalence of insomnia and its treatment in canada. Can. J. Psychiatry 2011, 56, 540–548. [Google Scholar] [CrossRef] [PubMed]
- Roth, T.; Coulouvrat, C.; Hajak, G.; Lakoma, M.D.; Sampson, N.A.; Shahly, V.; Shillington, A.C.; Stephenson, J.J.; Walsh, J.K.; Kessler, R.C. Prevalence and perceived health associated with insomnia based on dsm-iv-tr; international statistical classification of diseases and related health problems, tenth revision; and research diagnostic criteria/international classification of sleep disorders, second edition criteria: Results from the america insomnia survey. Biol. Psychiatry 2011, 69, 592–600. [Google Scholar] [PubMed]
- Ohayon, M.M.; Hong, S.C. Prevalence of insomnia and associated factors in South Korea. J. Psychosom. Res. 2002, 53, 593–600. [Google Scholar] [CrossRef] [PubMed]
- Serin, Y.; Acar Tek, N. Effect of circadian rhythm on metabolic processes and the regulation of energy balance. Ann. Nutr. Metab. 2019, 74, 322–330. [Google Scholar] [CrossRef]
- Duffy, J.F.; Wright, K.P., Jr. Entrainment of the human circadian system by light. J. Biol. Rhythms 2005, 20, 326–338. [Google Scholar] [CrossRef] [PubMed]
- van Maanen, A.; Meijer, A.M.; van der Heijden, K.B.; Oort, F.J. The effects of light therapy on sleep problems: A systematic review and meta-analysis. Sleep Med. Rev. 2016, 29, 52–62. [Google Scholar] [CrossRef]
- Aulsebrook, A.E.; Jones, T.M.; Mulder, R.A.; Lesku, J.A. Impacts of artificial light at night on sleep: A review and prospectus. J. Exp. Zool. A Ecol. Integr. Physiol. 2018, 329, 409–418. [Google Scholar] [CrossRef]
- Chambe, J.; Reynaud, E.; Maruani, J.; Fraih, E.; Geoffroy, P.A.; Bourgin, P. Light therapy in insomnia disorder: A systematic review and meta-analysis. J. Sleep Res. 2023, e13895. [Google Scholar] [CrossRef]
- Morin, C.M.; Benca, R. Chronic insomnia. Lancet 2012, 379, 1129–1141. [Google Scholar] [CrossRef] [PubMed]
- Geiger-Brown, J.M.; Rogers, V.E.; Liu, W.; Ludeman, E.M.; Downton, K.D.; Diaz-Abad, M. Cognitive behavioral therapy in persons with comorbid insomnia: A meta-analysis. Sleep Med. Rev. 2015, 23, 54–67. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The phq-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Horne, J.A.; Ostberg, O. A self-assessment questionnaire to determine morningness-eveningness in human circadian rhythms. Int. J. Chronobiol. 1976, 4, 97–110. [Google Scholar]
- Yu, J.H.; Yun, C.H.; Ahn, J.H.; Suh, S.; Cho, H.J.; Lee, S.K.; Yoo, H.J.; Seo, J.A.; Kim, S.G.; Choi, K.M.; et al. Evening chronotype is associated with metabolic disorders and body composition in middle-aged adults. J. Clin. Endocrinol. Metab. 2015, 100, 1494–1502. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F., 3rd; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef] [PubMed]
- Bastien, C.H.; Vallières, A.; Morin, C.M. Validation of the insomnia severity index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef]
- MacLean, A.W.; Fekken, G.C.; Saskin, P.; Knowles, J.B. Psychometric evaluation of the stanford sleepiness scale. J. Sleep Res. 1992, 1, 35–39. [Google Scholar] [CrossRef]
- Lapin, B.R.; Bena, J.F.; Walia, H.K.; Moul, D.E. The epworth sleepiness scale: Validation of one-dimensional factor structure in a large clinical sample. J. Clin. Sleep Med. 2018, 14, 1293–1301. [Google Scholar] [CrossRef]
- Münch, M.; Nowozin, C.; Regente, J.; Bes, F.; De Zeeuw, J.; Hädel, S.; Wahnschaffe, A.; Kunz, D. Blue-enriched morning light as a countermeasure to light at the wrong time: Effects on cognition, sleepiness, sleep, and circadian phase. Neuropsychobiology 2016, 74, 207–218. [Google Scholar] [CrossRef] [PubMed]
- Hatori, M.; Panda, S. The emerging roles of melanopsin in behavioral adaptation to light. Trends Mol. Med. 2010, 16, 435–446. [Google Scholar] [CrossRef] [PubMed]
- Yeung, V.; Sharpe, L.; Glozier, N.; Hackett, M.L.; Colagiuri, B. A systematic review and meta-analysis of placebo versus no treatment for insomnia symptoms. Sleep Med. Rev. 2018, 38, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Jung, C.M.; Khalsa, S.B.; Scheer, F.A.; Cajochen, C.; Lockley, S.W.; Czeisler, C.A.; Wright, K.P., Jr. Acute effects of bright light exposure on cortisol levels. J. Biol. Rhythm. 2010, 25, 208–216. [Google Scholar] [CrossRef]
- Gabel, V.; Maire, M.; Reichert, C.F.; Chellappa, S.L.; Schmidt, C.; Hommes, V.; Viola, A.U.; Cajochen, C. Effects of artificial dawn and morning blue light on daytime cognitive performance, well-being, cortisol and melatonin levels. Chronobiol. Int. 2013, 30, 988–997. [Google Scholar] [CrossRef]
- Scheer, F.A.; Buijs, R.M. Light affects morning salivary cortisol in humans. J. Clin. Endocrinol. Metab. 1999, 84, 3395–3398. [Google Scholar] [CrossRef]
- Cajochen, C.; Münch, M.; Kobialka, S.; Kräuchi, K.; Steiner, R.; Oelhafen, P.; Orgül, S.; Wirz-Justice, A. High sensitivity of human melatonin, alertness, thermoregulation, and heart rate to short wavelength light. J. Clin. Endocrinol. Metab. 2005, 90, 1311–1316. [Google Scholar] [CrossRef]
- Emeklİ, R.; İsmaİloğullari, S.; Bayram, A.; Akalin, H.; Tuncel, G.; Dündar, M. Comparing expression levels of period genes per1, per2 and per3 in chronic insomnia patients and medical staff working in the night shift. Sleep Med. 2020, 73, 101–105. [Google Scholar] [CrossRef]
- James, F.O.; Boivin, D.B.; Charbonneau, S.; Bélanger, V.; Cermakian, N. Expression of clock genes in human peripheral blood mononuclear cells throughout the sleep/wake and circadian cycles. Chronobiol. Int. 2007, 24, 1009–1034. [Google Scholar] [CrossRef]
- Archer, S.N.; Viola, A.U.; Kyriakopoulou, V.; von Schantz, M.; Dijk, D.J. Inter-individual differences in habitual sleep timing and entrained phase of endogenous circadian rhythms of bmal1, per2 and per3 mrna in human leukocytes. Sleep 2008, 31, 608–617. [Google Scholar] [CrossRef]
- Roenneberg, T.; Wirz-Justice, A.; Merrow, M. Life between clocks: Daily temporal patterns of human chronotypes. J. Biol. Rhythm. 2003, 18, 80–90. [Google Scholar] [CrossRef] [PubMed]
- Shechter, A.; Kim, E.W.; St-Onge, M.P.; Westwood, A.J. Blocking nocturnal blue light for insomnia: A randomized controlled trial. J. Psychiatr. Res. 2018, 96, 196–202. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Overall (n = 14) | Control Group (n = 7) | Experimental Group (n = 7) | p-Value |
|---|---|---|---|---|
| Age, years | 42.2 ± 10.2 | 37.0 ± 10.8 | 47.4 ± 6.7 | 0.054 |
| Gender, n (%) | >0.999 | |||
| Women | 13 (92.9) | 6 (85.7) | 7 (100.0) | |
| Men | 1 (7.1) | 1 (14.3) | 0 (0.0) | |
| Weight, kg | 62.1 ± 12.2 | 60.0 ± 13.1 | 64.3 ± 11.7 | 0.533 |
| Height, m | 161.9 ± 8.7 | 162.4 ± 10.5 | 161.5 ± 7.4 | 0.863 |
| Body mass index, kg/m2 | 23.5 ± 3.1 | 22.5 ± 2.2 | 24.6 ± 3.7 | 0.217 |
| SBP, mmHg | 121.9 ± 9.4 | 119.4 ± 6.7 | 124.3 ± 11.6 | 0.360 |
| DBP, mmHg | 74.3 ± 7.1 | 71.1 ± 7.2 | 77.4 ± 5.9 | 0.102 |
| Diabetes, n (%) | >0.999 | |||
| Yes | 1 (7.1) | 0 (0.0) | 1 (14.3) | |
| No | 13 (92.9) | 7 (100.0) | 6 (85.7) | |
| Hypertension, n (%) | ||||
| Yes | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| No | 14 (100.0) | 7 (100.0) | 7 (100.0) | |
| Dyslipidemia, n (%) | 0.445 | |||
| Yes | 2 (14.3) | 0 (0.0) | 2 (28.6) | |
| No | 12 (85.7) | 7 (100.0) | 5 (71.4) | |
| Smoking, n (%) | >0.999 | |||
| Yes | 1 (7.1) | 1 (14.3) | 0 (0.0) | |
| No | 13 (92.9) | 6 (85.7) | 7 (100.0) | |
| Drinking, n (%) | >0.999 | |||
| Yes | 9 (64.3) | 4 (57.1) | 5 (71.4) | |
| No | 5 (35.7) | 3 (42.9) | 2 (28.6) | |
| Exercise, n (%) | >0.999 | |||
| Yes | 9 (64.3) | 4 (57.1) | 5 (71.4) | |
| No | 5 (35.7) | 3 (42.9) | 2 (28.6) |
| Variable | Control Group | Experimental Group (LT) | p-Value † | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Diff | p-Value * | Pre | Post | Diff | p-Value * | ||
| WBC | 6.8 ± 2.4 | 6.0 ± 1.1 | −0.8 ± 1.8 | 0.284 | 7.1 ± 1.7 | 7.1 ± 1.4 | −0.1 ± 0.6 | 0.810 | 0.059 |
| Glucose, mg/dL | 98.0 ± 5.3 | 91.1 ± 8.1 | −6.9 ± 6.5 | 0.031 | 109.0 ± 15.0 | 101.6 ± 10.4 | −7.4 ± 8.6 | 0.062 | 0.369 |
| TC, mg/dL | 170.1 ± 27.5 | 168.3 ± 16.0 | −1.9 ± 23.3 | 0.840 | 186.3 ± 30.9 | 185.9 ± 29.5 | −0.4 ± 4.0 | 0.784 | 0.404 |
| TG, mg/dL | 188.4 ± 252.9 | 103.1 ± 41.2 | −85.3 ± 227.9 | 0.360 | 168.3 ± 133.4 | 120.0 ± 31.9 | −48.3 ± 131.5 | 0.369 | 0.313 |
| HDL-C, mg/dL | 57.6 ± 10.5 | 61.4 ± 8.3 | 3.0 ± 9.2 | 0.308 | 65.3 ± 10.7 | 64.7 ± 12.7 | −0.6 ± 7.5 | 0.847 | 0.658 |
| LDL-C, mg/dL | 94.7 ± 24.8 | 99.7 ± 15.5 | 5.0 ± 17.8 | 0.484 | 109.9 ± 34.3 | 113.0 ± 31.5 | 3.1 ± 11.7 | 0.505 | 0.743 |
| Insulin, IU/L | 16.2 ± 16.6 | 12.7 ± 11.0 | −3.5 ± 6.8 | 0.225 | 14.9 ± 11.2 | 7.2 ± 3.5 | −7.7 ± 11.9 | 0.138 | 0.132 |
| HOMA IR | 4.0 ± 4.0 | 2.8 ± 2.3 | −1.6 ± 2.1 | 0.198 | 4.2 ± 3.4 | 1.8 ± 1.0 | −2.4 ± 3.5 | 0.120 | 0.187 |
| HsCRP, mg/dL | 0.6 ± 0.5 | 0.5 ± 0.5 | −0.1 ± 0.5 | 0.700 | 0.8 ± 1.5 | 1.1 ± 1.7 | 0.4 ± 1.6 | 0.577 | 0.409 |
| Cortisol, μg/dL | 11.0 ± 4.5 | 10.8± 3.7 | −0.2 ± 2.2 | 0.792 | 9.7± 3.6 | 7.6 ± 3.1 | −2.1 ± 2.7 | 0.085 | 0.073 |
| ACTH | 24.2 ± 17.4 | 22.0 ± 10.5 | −2.2 ± 9.7 | 0.575 | 27.5 ± 14.4 | 24.5 ± 9.7 | −3.0 ± 12.0 | 0.526 | 0.818 |
| Serotonin | 165.0 ± 73.5 | 168.2 ± 97.9 | 3.2 ± 71.6 | 0.909 | 136.6 ± 132.5 | 146.0 ± 115.0 | 9.4 ± 39.6 | 0.551 | 0.950 |
| MHR (bpm) | 86.9 ± 16.1 | 89.6 ± 8.4 | 2.6 ± 8.4 | 0.436 | 75.4 ± 7.8 | 77.3 ± 8.8 | 1.9 ± 6.9 | 0.488 | 0.089 |
| SDNN (ms) | 27.1 ± 16.6 | 25.3 ± 7.5 | −1.8 ± 14.0 | 0.749 | 29.0 ± 11.4 | 28.4 ± 13.0 | −0.6 ± 5.2 | 0.762 | 0.639 |
| TP (m/s2) | 761.7 ± 842.5 | 438.6 ± 275.6 | −323.0 ± 830.5 | 0.343 | 805.1 ± 634.4 | 870.9 ± 984.9 | 65.7 ± 685.1 | 0.808 | 0.273 |
| LFNorm | 60.6 ± 16.9 | 36.8 ± 11.7 | −23.8 ± 16.8 | 0.009 | 56.1 ± 27.7 | 51.1 ± 19.6 | −5.1 ± 30.5 | 0.674 | 0.115 |
| HFNorm | 39.4 ± 16.9 | 63.2 ± 11.7 | 23.8 ± 16.8 | 0.009 | 43.9 ± 27.7 | 49.0 ± 19.6 | 5.1 ± 30.5 | 0.674 | 0.115 |
| LF/HF Ratio | 2.4 ± 2.5 | 0.6± 0.4 | −1.7 ± 2.5 | 0.118 | 2.7 ± 3.3 | 1.5 ± 1.3 | −1.2 ± 3.6 | 0.402 | 0.147 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoon, J.; Heo, S.; Lee, H.; Sul, E.; Han, T.; Kwon, Y.-J. Feasibility and Efficacy of Morning Light Therapy for Adults with Insomnia: A Pilot, Randomized, Open-Label, Two-Arm Study. Medicina 2023, 59, 1066. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina59061066
Yoon J, Heo S, Lee H, Sul E, Han T, Kwon Y-J. Feasibility and Efficacy of Morning Light Therapy for Adults with Insomnia: A Pilot, Randomized, Open-Label, Two-Arm Study. Medicina. 2023; 59(6):1066. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina59061066
Chicago/Turabian StyleYoon, Jihyun, Seokjae Heo, Hyangkyu Lee, Eungyeong Sul, Taehwa Han, and Yu-Jin Kwon. 2023. "Feasibility and Efficacy of Morning Light Therapy for Adults with Insomnia: A Pilot, Randomized, Open-Label, Two-Arm Study" Medicina 59, no. 6: 1066. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina59061066