
High Birth Weight Increases the Risk for Bone Tumor: A Systematic Review and Meta-Analysis

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
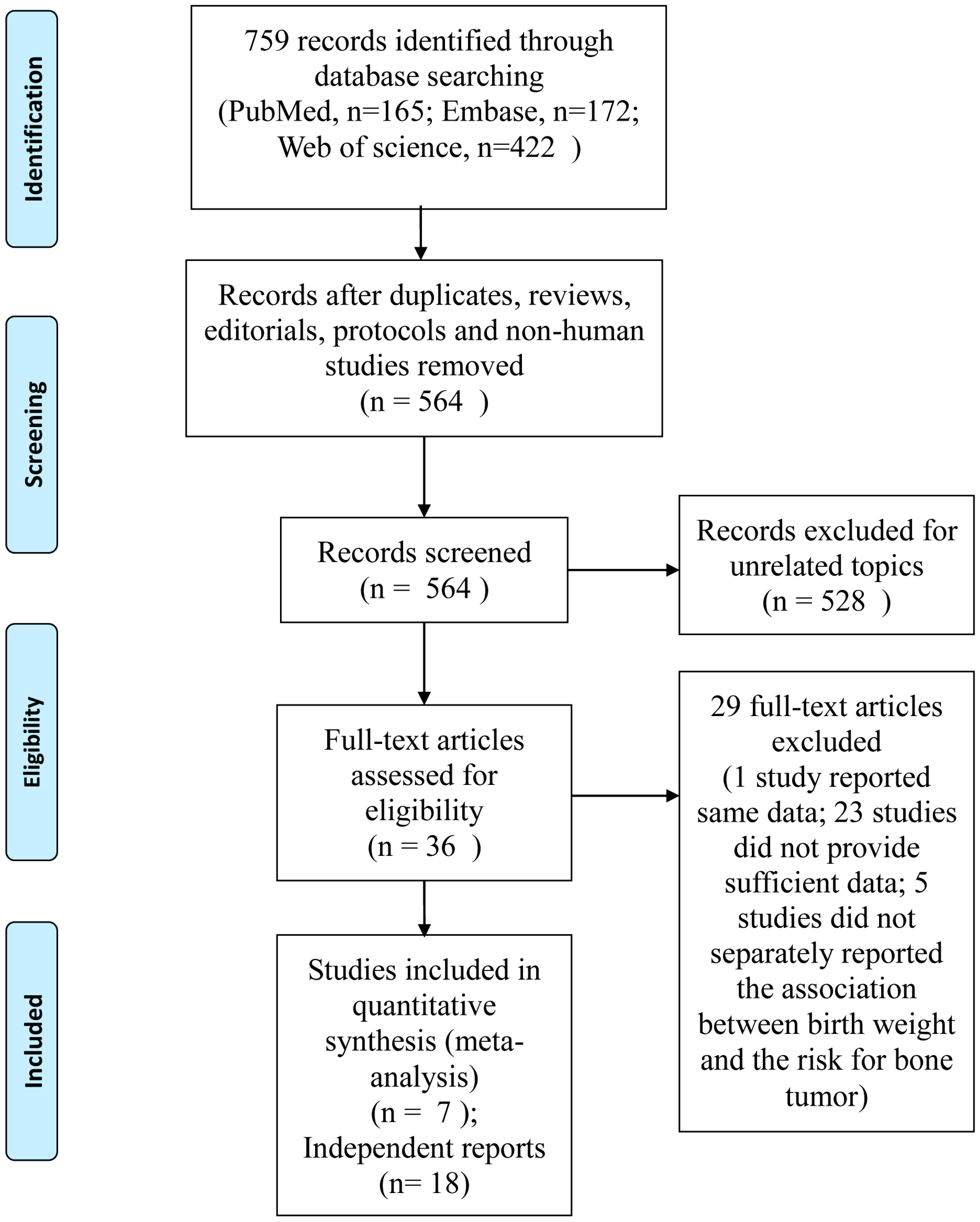
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Included Studies

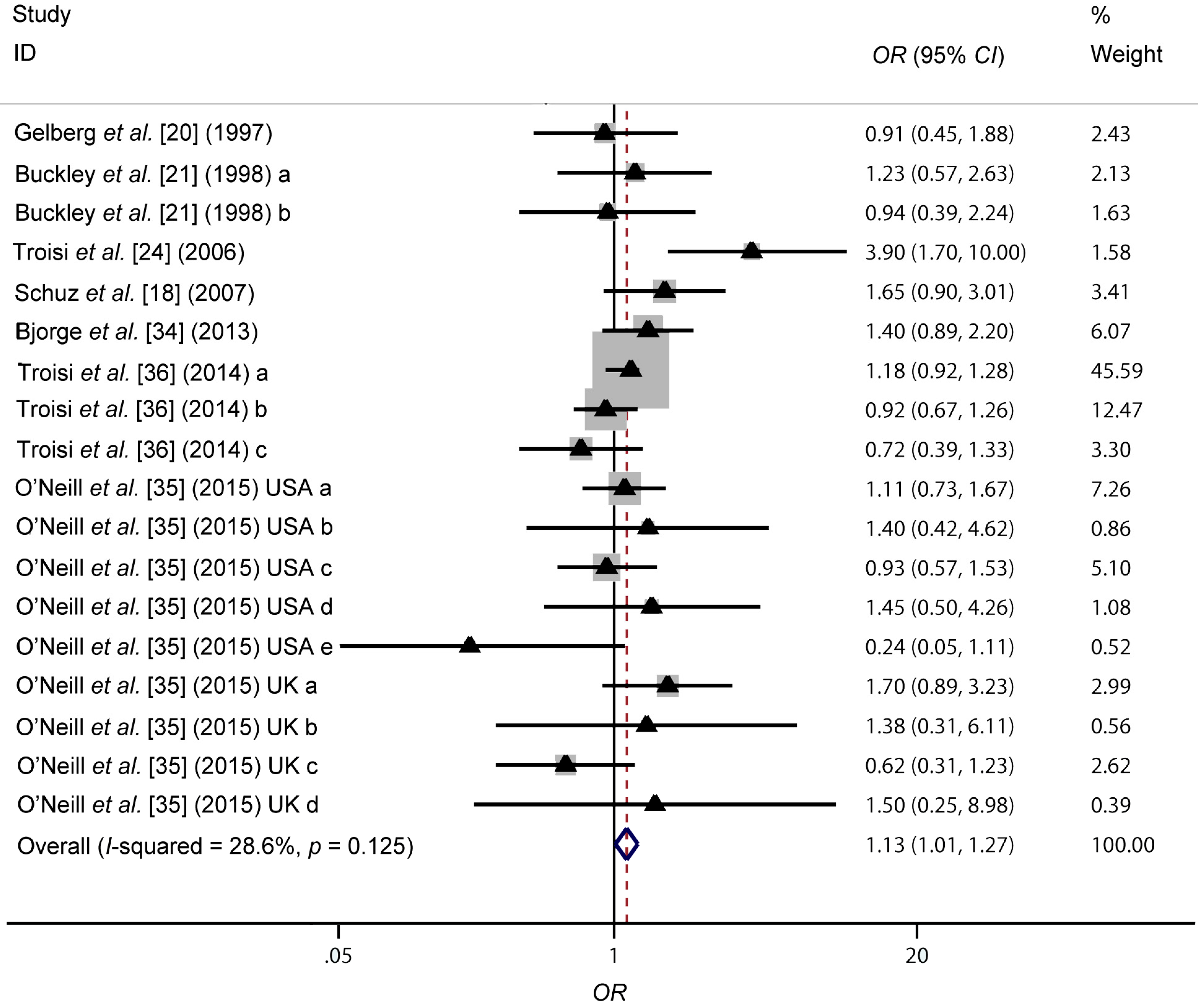
3.2. Association between High Birth Weight and Bone Tumor Risk

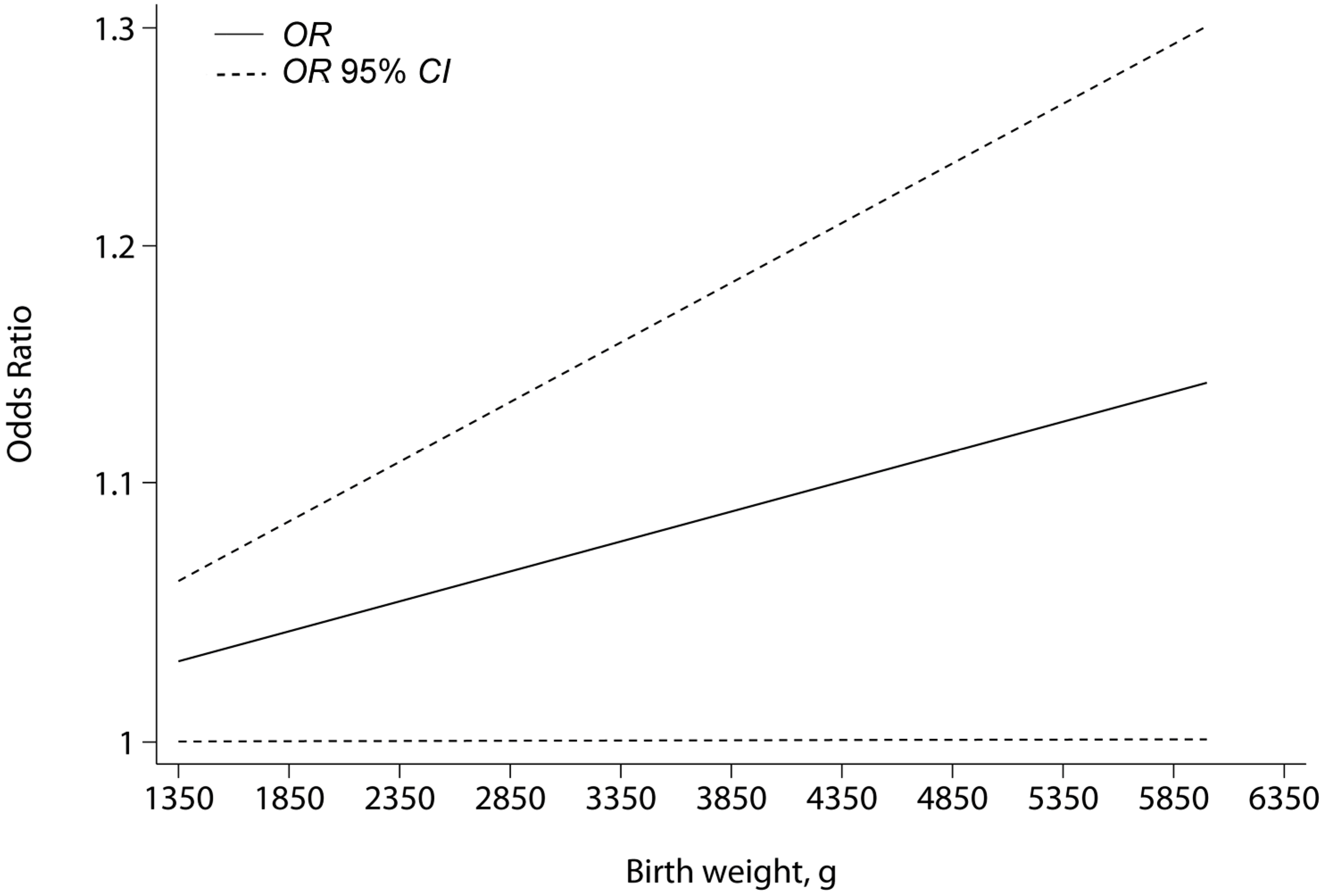
3.3. Dose-Response Analysis

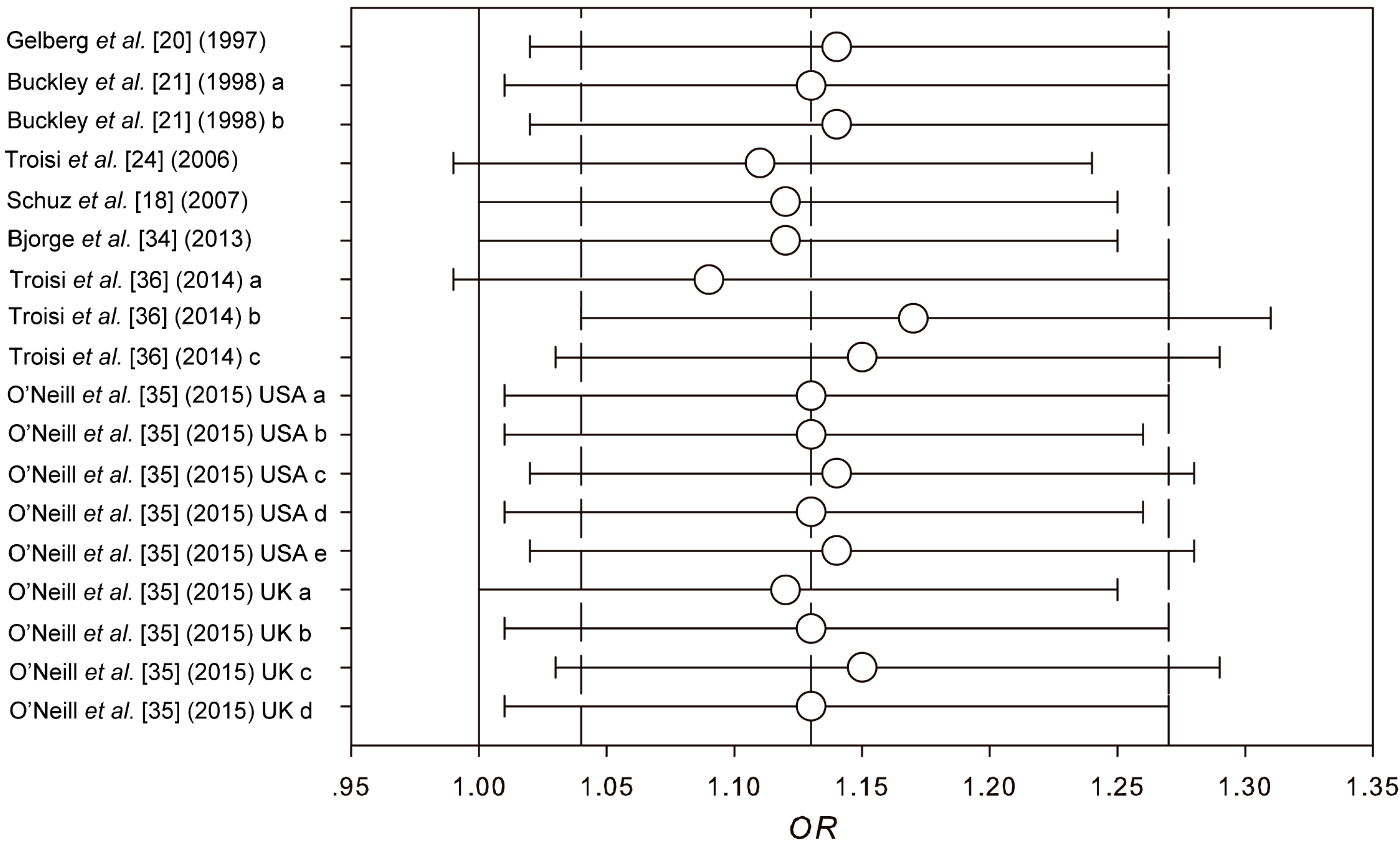
3.4. Sensitivity Analyses

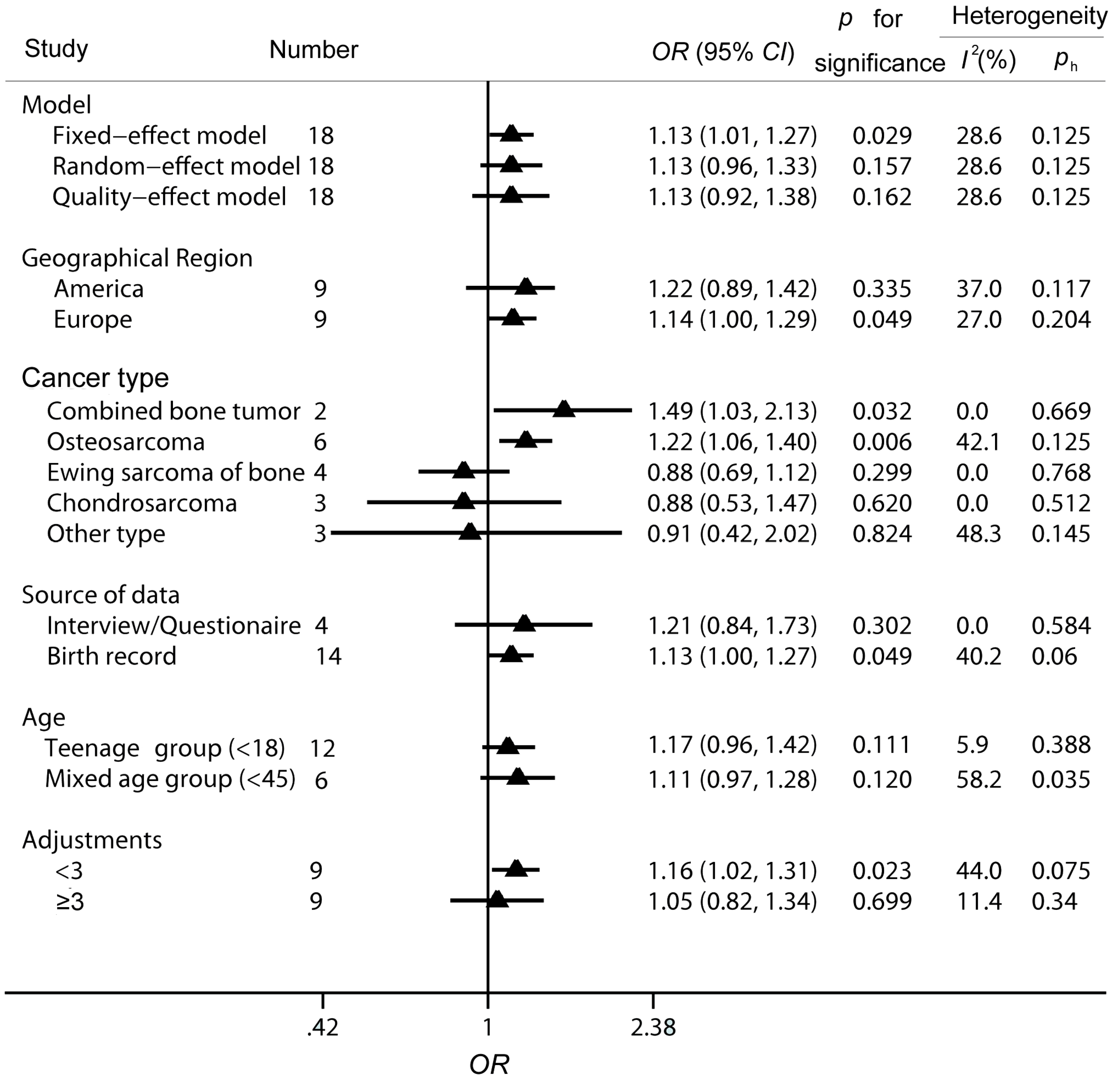
3.5. Subgroup Analyses

3.6. Analysis on the Relationship between High Birth Weight and the Risks for the Three Main Subtypes of Bone Tumor in Age-Related Groups

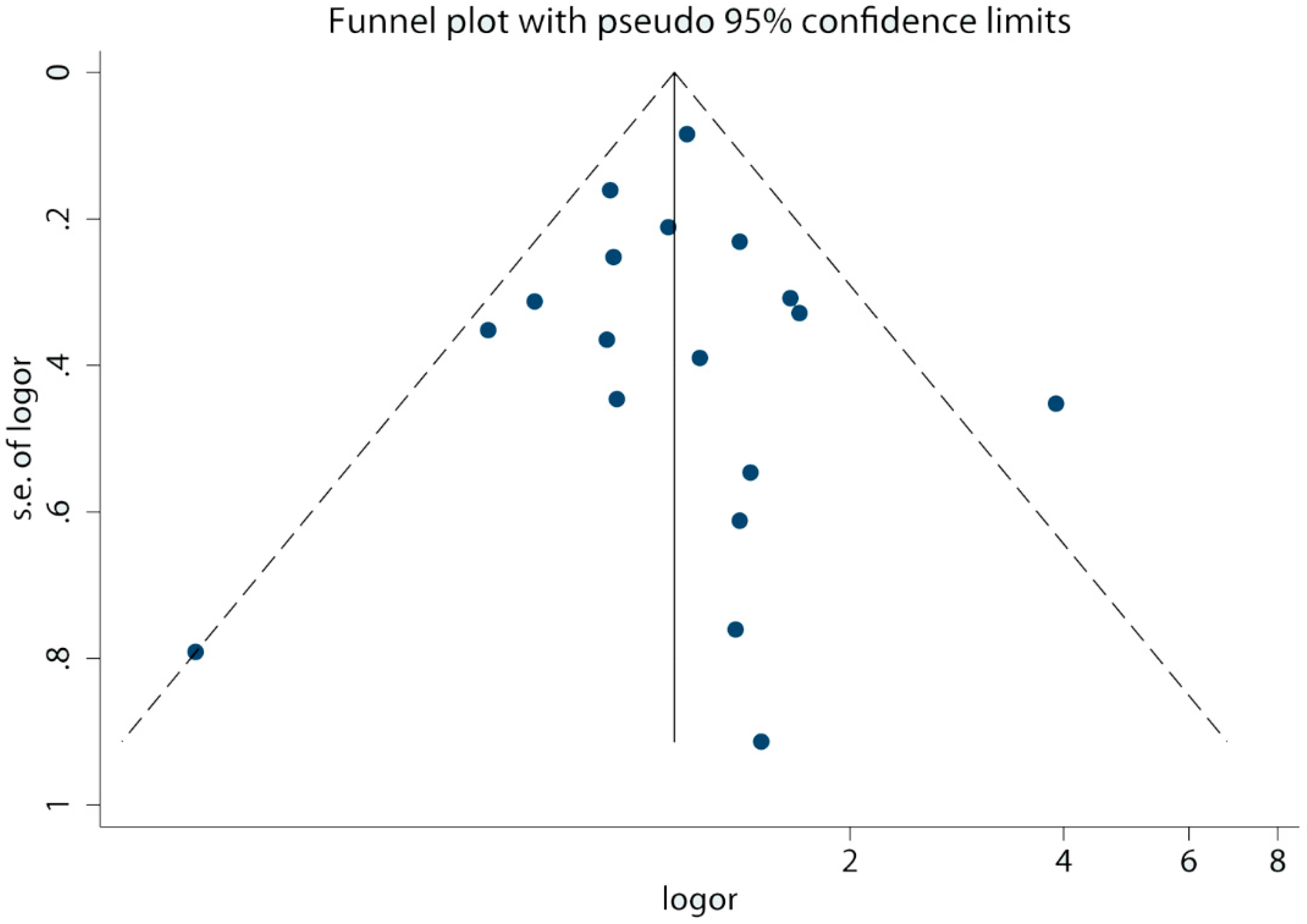
3.7. Publication Bias

4. Discussion
5. Conclusions
Supplementary Files
Supplementary File 1Acknowledgments
Author Contributions
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2015. CA Cancer J. Clin. 2015, 65, 5–29. [Google Scholar] [CrossRef] [PubMed]
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [PubMed]
- Gatta, G.; Botta, L.; Rossi, S.; Aareleid, T.; Bielska-Lasota, M.; Clavel, J.; Dimitrova, N.; Jakab, Z.; Kaatsch, P.; Lacour, B. Childhood cancer survival in europe 1999–2007: Results of eurocare-5—A population-based study. Lancet Oncol. 2014, 15, 35–47. [Google Scholar] [CrossRef]
- Gatta, G.; Zigon, G.; Capocaccia, R.; Coebergh, J.W.; Desandes, E.; Kaatsch, P.; Pastore, G.; Peris-Bonet, R.; Stiller, C.A.; Group, E.W. Survival of european children and young adults with cancer diagnosed 1995–2002. Eur. J. Cancer 2009, 45, 992–1005. [Google Scholar] [CrossRef] [PubMed]
- van den Berg, H.; Slaar, A.; Kroon, H.M.; Taminiau, A.H.; Hogendoorn, P. Results of diagnostic review in pediatric bone tumors and tumorlike lesions. J. Pediatr. Orthopaed. 2008, 28, 561–564. [Google Scholar] [CrossRef] [PubMed]
- Eyre, R.; Feltbower, R.G.; Mubwandarikwa, E.; Eden, T.O.; McNally, R.J. Epidemiology of bone tumours in children and young adults. Pediatr. Blood Cancer 2009, 53, 941–952. [Google Scholar] [CrossRef] [PubMed]
- Steer, C.D.; Sayers, A.; Kemp, J.; Fraser, W.D.; Tobias, J.H. Birth weight is positively related to bone size in adolescents but inversely related to cortical bone mineral density: Findings from a large prospective cohort study. Bone 2014, 65, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Mesa, J.; Restrepo-Méndez, M.; González, D.; Wehrmeister, F.; Horta, B.; Domingues, M.; Menezes, A. Life-course evidence of birth weight effects on bone mass: Systematic review and meta-analysis. Osteoporosis Int. 2013, 24, 7–18. [Google Scholar] [CrossRef] [PubMed]
- Kuh, D.; Wills, A.K.; Shah, I.; Prentice, A.; Hardy, R.; Adams, J.E.; Ward, K.; Cooper, C. Growth from birth to adulthood and bone phenotype in early old age: A british birth cohort study. Bone Miner. Res. 2014, 29, 123–133. [Google Scholar] [CrossRef] [PubMed]
- Lagiou, P.; Hsieh, C.; Lipworth, L.; Samoli, E.; Okulicz, W.; Troisi, R.; Xu, B.; Hall, P.; Ekbom, A.; Adami, H. Insulin-like growth factor levels in cord blood, birth weight and breast cancer risk. Br. J. Cancer 2009, 100, 1794–1798. [Google Scholar] [CrossRef] [PubMed]
- Macaulay, V. Insulin-like growth factors and cancer. Br. J. Cancer 1992, 65, 311. [Google Scholar] [CrossRef] [PubMed]
- Charalambous, M.; da Rocha, S.T.; Ferguson-Smith, A.C. Genomic imprinting, growth control and the allocation of nutritional resources: Consequences for postnatal life. Curr. Opin. Endocrinol. 2007, 14, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Michels, K.B.; Xue, F. Role of birthweight in the etiology of breast cancer. Int. J. Cancer 2006, 119, 2007–2025. [Google Scholar] [CrossRef] [PubMed]
- Schüz, J.; Forman, M.R. Birthweight by gestational age and childhood cancer. Cancer Cause. Control 2007, 18, 655–663. [Google Scholar] [CrossRef] [PubMed]
- Hjalgrim, L.L.; Westergaard, T.; Rostgaard, K.; Schmiegelow, K.; Melbye, M.; Hjalgrim, H.; Engels, E.A. Birth weight as a risk factor for childhood leukemia: A meta-analysis of 18 epidemiologic studies. Am. J. Epidemiol. 2003, 158, 724–735. [Google Scholar] [CrossRef] [PubMed]
- Harder, T.; Plagemann, A.; Harder, A. Birth weight and subsequent risk of childhood primary brain tumors: A meta-analysis. Am. J. Epidemiol. 2008, 168, 366–373. [Google Scholar] [CrossRef] [PubMed]
- Ognjanovic, S.; Carozza, S.; Chow, E.; Fox, E.; Horel, S.; McLaughlin, C.; Mueller, B.; Puumala, S.; Reynolds, P.; von Behren, J. Birth characteristics and the risk of childhood rhabdomyosarcoma based on histological subtype. Br. J. Cancer 2010, 102, 227–231. [Google Scholar] [CrossRef] [PubMed]
- Schüz, J.; Schmidt, L.S.; Kogner, P.; Lähteenmäki, P.M.; Pal, N.; Stokland, T.; Schmiegelow, K. Birth characteristics and wilms tumors in children in the nordic countries: A register-based case–control study. Int. J. Cancer 2011, 128, 2166–2173. [Google Scholar] [CrossRef] [PubMed]
- Holly, E.A.; Aston, D.A.; Ahn, D.K.; Kristiansen, J.J. Ewing’s bone sarcoma, paternal occupational exposure, and other factors. Am. J. Epidemiol. 1992, 135, 122–129. [Google Scholar] [PubMed]
- Gelberg, K.H.; Fitzgerald, E.F.; Hwang, S.; Dubrow, R. Growth and development and other risk factors for osteosarcoma in children and young adults. Int. J. Epidemiol. 1997, 26, 272–278. [Google Scholar] [CrossRef] [PubMed]
- Buckley, J.D.; Pendergrass, T.W.; Buckley, C.M.; Pritchard, D.J.; Nesbit, M.E.; Provisor, A.J.; Robison, L.L. Epidemiology of osteosarcoma and ewing’s sarcoma in childhood. Cancer 1998, 83, 1440–1448. [Google Scholar] [CrossRef]
- Hartley, A.L.; Birch, J.M.; McKinney, P.; Teare, M.D.; Blair, V.; Carrette, J.; Mann, J.; Draper, G.; Stiller, C.; Johnston, H. The Inter-Regional Epidemiological Study of Childhood Cancer (IRESCC): Case control study of children with bone and soft tissue sarcomas. Br. J. Cancer 1988, 58, 838–842. [Google Scholar] [CrossRef] [PubMed]
- Valery, P.C.; McWhirter, W.; Sleigh, A.; Williams, G.; Bain, C. A national case-control study of ewing’s sarcoma family of tumours in Australia. Int. J. Cancer 2003, 105, 825–830. [Google Scholar] [CrossRef] [PubMed]
- Troisi, R.; Masters, M.; Joshipura, K.; Douglass, C.; Cole, B.; Hoover, R. Perinatal factors, growth and development, and osteosarcoma risk. Br. J. Cancer 2006, 95, 1603–1607. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The prisma statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Stang, A. Critical evaluation of the newcastle-ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Doi, S.A.; Thalib, L. A quality-effects model for meta-analysis. Epidemiology 2008, 19, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.; Tong, Y.; Wei, X.; Zhao, Q.; Pan, X.; Yu, G.; Lu, Q. Association between int7g24a rs334354 polymorphism and cancer risk: A meta-analysis of case-control studies. Sci. Rep. 2015, 5, 11350. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.; Tong, Y.; Zhao, Q.; Yu, G.; Wei, X.; Lu, Q. Coffee consumption and bladder cancer: A meta-analysis of observational studies. Sci. Rep. 2015, 5. [Google Scholar] [CrossRef] [PubMed]
- Lau, J.; Ioannidis, J.P.; Schmid, C.H. Quantitative synthesis in systematic reviews. Ann. Inter. Med. 1997, 127, 820–826. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Bjørge, T.; Sørensen, H.T.; Grotmol, T.; Engeland, A.; Stephansson, O.; Gissler, M.; Tretli, S.; Troisi, R. Fetal growth and childhood cancer: A population-based study. Pediatrics 2013, 132, e1265–e1275. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, K.A.; Murphy, M.F.; Bunch, K.J.; Puumala, S.E.; Carozza, S.E.; Chow, E.J.; Mueller, B.A.; McLaughlin, C.C.; Reynolds, P.; Vincent, T.J. Infant birthweight and risk of childhood cancer: International population-based case control studies of 40,000 cases. Int. J. Epidemiol. 2015, 44, 153–168. [Google Scholar] [CrossRef] [PubMed]
- Troisi, R.; Stephansson, O.; Jacobsen, J.; Tretli, S.; Sørensen, H.T.; Gissler, M.; Kaaja, R.; Ekbom, A.; Hoover, R.N.; Grotmol, T. Perinatal characteristics and bone cancer risk in offspring—A scandinavian population-based study. Acta Oncol. 2014, 53, 830–838. [Google Scholar] [CrossRef] [PubMed]
- Jayanthiny, P.; Tennekoon, K.; Karunanayake, E.; Kumarasiri, J.; Wijesundera, A. Di-nucleotide repeat polymorphisms of the insulin-like growth factor-1 gene and their association with IGF-1, insulin-like growth factor-binding protein-1 and birth size in a Sri-Lankan cohort. Neonatology 2010, 100, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Javaid, M.K.; Lekamwasam, S.; Clark, J.; Dennison, E.M.; Syddall, H.E.; Loveridge, N.; Reeve, J.; Beck, T.J.; Cooper, C. Infant growth influences proximal femoral geometry in adulthood. J. Bone Miner. Res. 2006, 21, 508–512. [Google Scholar] [CrossRef] [PubMed]
- Ru, G.; Terracini, B.; Glickman, L. Host related risk factors for canine osteosarcoma. Vet. J. 1998, 156, 31–39. [Google Scholar] [CrossRef]
- Selvarajah, G.T.; Kirpensteijn, J. Prognostic and predictive biomarkers of canine osteosarcoma. Vet. J. 2010, 185, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Cerutti, P. Oxidant stress and carcinogenesis. Eur. J. Clin. Investig. 1991, 21, 1–5. [Google Scholar] [CrossRef]
- Sandberg, A.A.; Bridge, J.A. Updates on the cytogenetics and molecular genetics of bone and soft tissue tumors: Osteosarcoma and related tumors. Cancer Genet. Cytogen. 2003, 145, 1–30. [Google Scholar] [CrossRef]
- Al-Romaih, K.; Bayani, J.; Vorobyova, J.; Karaskova, J.; Park, P.; Zielenska, M.; Squire, J. Chromosomal instability in osteosarcoma and its association with centrosome abnormalities. Cancer Genet. Cytogen. 2003, 144, 91–99. [Google Scholar] [CrossRef]
- Ross, J.A.; Perentesis, J.P.; Robison, L.L.; Davies, S.M. Big babies and infant leukemia: A role for insulin-like growth factor-1? Cancer Cause. Control 1996, 7, 553–559. [Google Scholar] [CrossRef]
- Fürstenberger, G.; Senn, H.-J. Insulin-like growth factors and cancer. Lancet Oncol. 2002, 3, 298–302. [Google Scholar] [CrossRef]
- Operskalski, E.A.; Preston-Martin, S.; Henderson, B.E.; Visscher, B.R. A case-control study of osteosarcoma in young persons. Am. J. Epidemiol. 1987, 126, 118–126. [Google Scholar] [PubMed]
- Franchi, A. Epidemiology and classification of bone tumors. Clin. Cases Miner. Bone Metab. 2012, 9, 92. [Google Scholar] [PubMed]
- Stiller, C.; Bielack, S.; Jundt, G.; Steliarova-Foucher, E. Bone tumours in european children and adolescents, 1978–1997. Report from the automated childhood cancer information system project. Eur. J. Cancer 2006, 42, 2124–2135. [Google Scholar] [CrossRef] [PubMed]
- Ritter, J.; Bielack, S.S. Osteosarcoma. Ann. Oncol. 2010, 21, vii320–vii325. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, R.S.; Westgate, J.A.; Beattie, J.; Pattison, N.S.; Gamble, G.; Mildenhall, L.F.J.; Johnstone, F.D. Inverse changes in fetal insulin-like growth factor (IGF)-1 and IGF binding protein-1 in association with higher birth weight in maternal diabetes. Clin. Endocrinol. 2007, 66, 322–328. [Google Scholar] [CrossRef] [PubMed]
- Ong, K.; Kratzsch, J.; Kiess, W.; Costello, M.; Scott, C.; Dunger, D. Size at Birth and Cord Blood Levels of Insulin, Insulin-Like Growth Factor I (IGF-I), IGF-II, IGF-Binding Protein-1 (IGFBP-1), IGFBP-3, and the Soluble IGF-II/Mannose-6-Phosphate Receptor in Term Human Infants 1. J. Clin. Endocr. Metab. 2000, 85, 4266–4269. [Google Scholar] [CrossRef] [PubMed]
- Kappel, C.C.; Velez-Yanguas, M.C.; Hirschfeld, S.; Helman, L.J. Human osteosarcoma cell lines are dependent on insulin-like growth factor I for in vitro growth. Cancer Res. 1994, 54, 2803–2807. [Google Scholar] [PubMed]
- Bell, R.S. Expression of insulin-like growth factor receptor, IGF-1, and IGF-2 in primary and metastatic osteosarcoma. J. Sur. Oncol. 1998, 69, 21–27. [Google Scholar]
- Mirabello, L.; Pfeiffer, R.; Murphy, G.; Daw, N.C.; Patiño-Garcia, A.; Troisi, R.J.; Hoover, R.N.; Douglass, C.; Schüz, J.; Craft, A.W. Height at diagnosis and birth-weight as risk factors for osteosarcoma. Cancer Cause. Control 2011, 22, 899–908. [Google Scholar] [CrossRef] [PubMed]
- Savage, S.A.; Burdett, L.; Troisi, R.; Douglass, C.; Hoover, R.N.; Chanock, S.J. Germ-line genetic variation of tp53 in osteosarcoma. Pediatr. Blood Cancer 2007, 49, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Jensen, R.; Drake, R. Rarity of ewing’s tumour in Negroes. Lancet 1970, 295, 777. [Google Scholar] [CrossRef]
- Li, F.; Tu, J.-T.; Liu, F.-S.; Shiang, E. Rarity of Ewing’s Sarcoma in China. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/6104072 (accessed on 31 July 2015).
- Fraumeni, J.; Glass, A. Rarity of ewing’s sarcoma among us Negro children. Lancet 1970, 295, 366–367. [Google Scholar] [CrossRef]
- Ozaki, T.; Schaefer, K.-L.; Wai, D.; Yokoyama, R.; Ahrens, S.; Diallo, R.; Hasegawa, T.; Shimoda, T.; Hirohashi, S.; Kawai, A. Population-based genetic alterations in ewing’s tumors from Japanese and European caucasian patients. Ann. Oncol. 2002, 13, 1656–1664. [Google Scholar] [CrossRef] [PubMed]
- Bennett, K.; Howell, A.; Evans, D.G.R.; Birch, J.M. A follow-up study of breast and other cancers in families of an unselected series of breast cancer patients. Br. J. Cancer 2002, 86, 718–722. [Google Scholar] [CrossRef] [PubMed]
- Ji, J.; Hemminki, K. Familial risk for histology-specific bone cancers: An updated study in Sweden. Eur. J. Cancer 2006, 42, 2343–2349. [Google Scholar] [CrossRef] [PubMed]
- Polednak, A.P. Primary bone cancer incidence in black and white residents of New York state. Cancer 1985, 55, 2883–2888. [Google Scholar] [CrossRef]
- Martin, J.A.; Hamilton, B.E.; Ventura, S.J.; Osterman, M.J.; Wilson, E.C.; Mathews, T.J. Births: Final data for 2010. Natl. Vital Stat. Rep. 2012, 61, 1–72. [Google Scholar] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, S.; Yang, L.; Pu, F.; Lin, H.; Wang, B.; Liu, J.; Shao, Z. High Birth Weight Increases the Risk for Bone Tumor: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2015, 12, 11178-11195. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph120911178
Chen S, Yang L, Pu F, Lin H, Wang B, Liu J, Shao Z. High Birth Weight Increases the Risk for Bone Tumor: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2015; 12(9):11178-11195. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph120911178
Chicago/Turabian StyleChen, Songfeng, Lin Yang, Feifei Pu, Hui Lin, Baichuan Wang, Jianxiang Liu, and Zengwu Shao. 2015. "High Birth Weight Increases the Risk for Bone Tumor: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 12, no. 9: 11178-11195. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph120911178