
Beta-Arrestin1 Levels in Mononuclear Leukocytes Support Depression Scores for Women with Premenstrual Dysphoric Disorder

Abstract
:1. Introduction
2. Methods
2.1. Participants
HAM-D
2.2. Isolation of Mononuclear Leukocytes
2.3. ELISA
2.4. Statistical Analyses
3. Results



{kind=link}
{kind=link}
{kind=link}
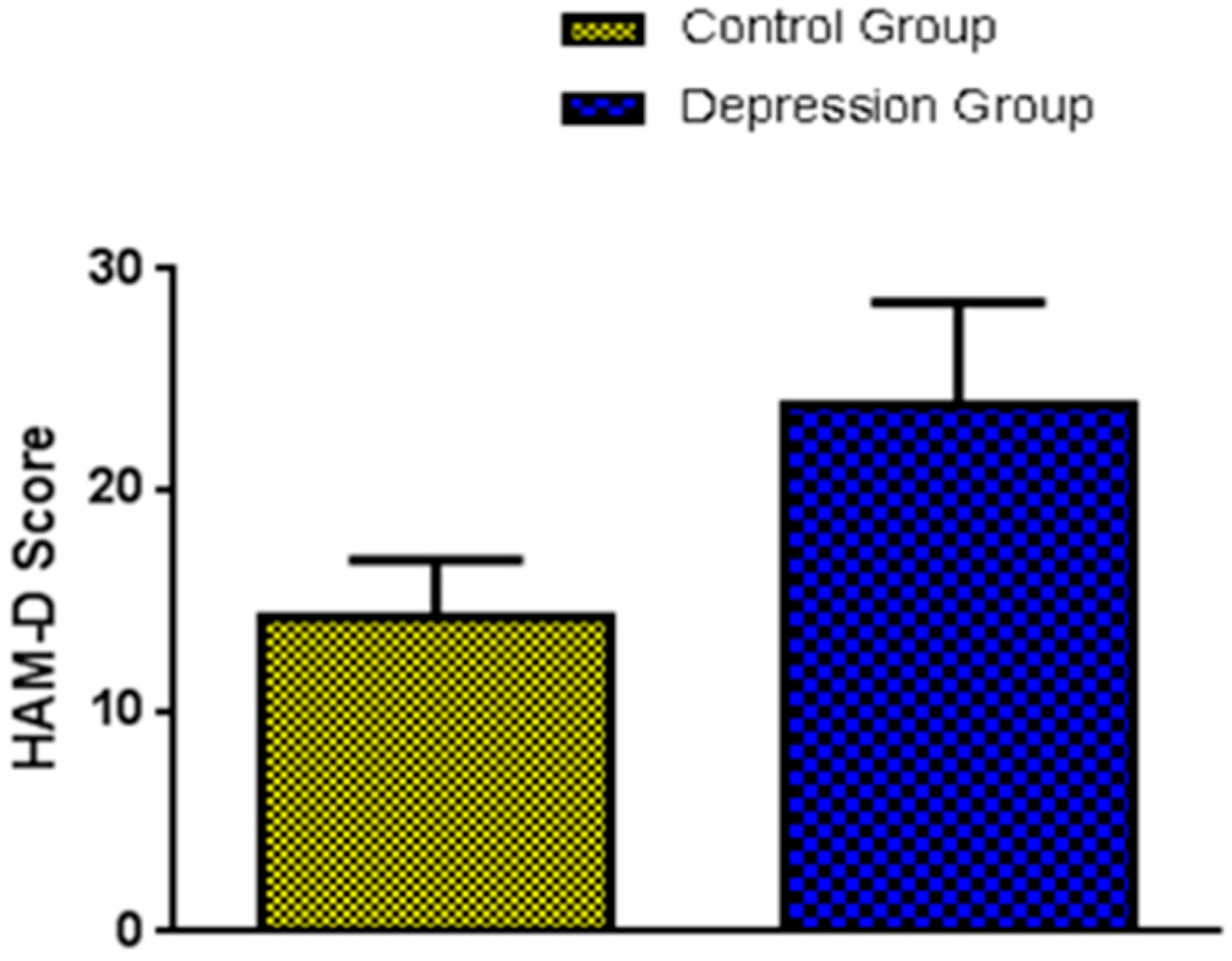
| Participants HAM-D Score Beta-arrestin1 (pg/mg Protein) | ||
|---|---|---|
| Control group | 14.31 ± 0.71 | 106.7 ± 2.14 |
| Depression Group | 23.83 ± 1.35 * | 96.12 ± 2.45 * |

4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Singh, B.B.; Berman, B.M.; Simpson, R.L.; Annechild, A. Incidence of premenstrual syndrome and remedy usage: A national probability sample study. Altern. Ther. Health Med. 1998, 4, 75–79. [Google Scholar] [PubMed]
- Halbreich, U.; Borenstein, J.; Pearlstein, T.; Kahn, L.S. The prevalence, impairment, impact, and burden of premenstrual dysphoric disorder (PMS/PMDD). Psychoneuroendocrinology 2003, 28, 1–23. [Google Scholar] [CrossRef]
- Kim, D.R.; Gyulai, L.; Freeman, E.W.; Morrison, M.F.; Baldassano, C.; Dube, B. Premenstrual dysphoric disorder and psychiatric co-morbidity. Arch. Womens Ment. Health 2004, 7, 37–47. [Google Scholar] [CrossRef] [PubMed]
- Rapkin, A. A review of treatment of premenstrual syndrome and premenstrual dysphoric disorder. Psychoneuroendocrinology 2003, 28, 39–53. [Google Scholar] [CrossRef]
- Seedat, S.; Scott, K.; Angermeyer, M.; Berglund, P.; Bromet, E.; Brugha, T.; Demyttenaere, K.; Girolamo, G.; Haro, J.; Jin, R.; et al. Cross-national associations between gender and mental disorders in the World Health Organization World Mental Health Surveys. Arch. Gen. Psychiatry 2009, 66, 785–795. [Google Scholar] [CrossRef] [PubMed]
- Avissar, S.; Schreiber, G. Toward molecular diagnostics of mood disorders in psychiatry. Trends Mol. Med. 2002, 8, 294–300. [Google Scholar] [CrossRef]
- Schreiber, G.; Avissar, S. Application of G-proteins in the molecular diagnosis of psychiatric disorders. Expert Rev. Mol. Diagn. 2003, 3, 69–80. [Google Scholar] [CrossRef] [PubMed]
- Avissar, S.; Matuzany-Ruban, A.; Tzukert, K.; Schreiber, G. Beta-arrestin-1 levels: Reduced in leukocytes of patients with depression and elevated by antidepressants in rat brain. Am. J. Psychiatry 2004, 161, 2066–2072. [Google Scholar] [CrossRef] [PubMed]
- Perry, S.J.; Lefkowitz, R.J. Arresting developments in heptahelical receptor signaling and regulation. Trends Cell Biol. 2002, 12, 130–138. [Google Scholar] [CrossRef]
- Gainetdinov, R.R.; Premont, R.T.; Bohn, L.M.; Lefkowitz, R.J.; Caron, M.G. Desensitization of G protein-coupled receptors and neuronal functions. Annu. Rev. Neurosci. 2004, 27, 107–144. [Google Scholar] [CrossRef] [PubMed]
- Lefkowitz, R.J. Historical review: A brief history and personal retrospective of seven-transmembrane receptors. Trends Pharmacol. Sci. 2004, 25, 413–422. [Google Scholar] [CrossRef] [PubMed]
- Pierce, K.L.; Lefkowitz, R.J. Classical and new roles of beta-arrestins in the regulation of G-protein-coupled receptors. Nat. Rev. Neurosci. 2001, 2, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Luttrell, L.M.; Lefkowitz, R.J. The role of beta-arrestins in the termination and transduction of G-protein-coupled receptor signals. J. Cell Sci. 2002, 115, 455–465. [Google Scholar] [PubMed]
- Goodman, O.B.; Krupnick, J.G., Jr.; Santini, F.; Gurevich, V.V.; Penn, R.B.; Gagnon, A.W.; Keen, J.H.; Benovic, J.L. Beta-arrestin acts as a clathrin adaptor in endocytosis of the beta2-adrenergic receptor. Nature 1996, 383, 447–450. [Google Scholar] [CrossRef] [PubMed]
- Laporte, S.A.; Oakley, R.H.; Zhang, J.; Holt, J.A.; Ferguson, S.S.; Caron, M.G.; Barak, L.S. The beta2-adrenergic receptor/betaarrestin complex recruits the clathrin adaptor AP-2 during endocytosis. Proc. Natl. Acad. Sci. USA 1999, 96, 3712–3717. [Google Scholar] [CrossRef] [PubMed]
- Gagnon, A.W.; Kallal, L.; Benovic, J.L. Role of clathrin-mediated endocytosis in agonist-induced down-regulation of the beta2-adrenergic receptor. J. Biol. Chem. 1998, 273, 6976–6981. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Barak, L.S.; Winkler, K.E.; Caron, M.G.; Ferguson, S.S. A central role for beta-arrestins and clathrin-coated vesicle-mediated endocytosis in beta2-adrenergic receptor resensitization. Differential regulation of receptor resensitization in two distinct cell types. J. Biol. Chem. 1997, 272, 27005–27014. [Google Scholar] [CrossRef] [PubMed]
- Oakley, R.H.; Laporte, S.A.; Holt, J.A.; Barak, L.S.; Caron, M.G. Association of beta-arrestin with G protein-coupled receptors during clathrin-mediated endocytosis dictates the profile of receptor resensitization. J. Biol. Chem. 1999, 274, 32248–32257. [Google Scholar] [CrossRef] [PubMed]
- Steiner, M.; Pearlstein, T.; Cohen, L.; Endicott, J.; Kornstein, S.; Roberts, C.; Roberts, D.; Yonkers, K. Expert guidelines for the treatment of severe PMS, PMDD, and comorbidities: The role of SSRIs. J. Womens Health (Larchmt.) 2006, 15, 57–69. [Google Scholar] [CrossRef] [PubMed]
- Cox, J.L.; Murray, D.; Chapman, G. A controlled study of the onset, duration and prevalence of postnatal depression. Br. J. Psychiatry 1993, 163, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Dominguez, R.; Hu, E.; Zhou, M.; Baudry, M. 17beta-estradiol-mediated neuroprotection and ERK activation require a pertussis toxin-sensitive mechanism involving GRK2 and beta-arrestin-1. J. Neurosci. 2009, 29, 4228–4238. [Google Scholar] [CrossRef] [PubMed]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Baker, R.; Dunbar, G.C. The Mini-International Neuropsychiatric Interview: The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J. Clin. Psychiatry 1998, 59, 22–33. [Google Scholar] [PubMed]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Matuzany-Ruban, A.; Avissar, S.; Schreiber, G. Dynamics of beta-arrestin1 protein and mRNA levels elevation by antidepressants in mononuclear leukocytes of patients with depression. J. Affect. Disord. 2005, 88, 307–312. [Google Scholar] [CrossRef] [PubMed]
- Kaur, G.; Gonsalves, L.; Thacker, H.L. Premenstrual dysphoric disorder: A review for the treating practitioner. Clevel. Clin. J. Med. 2004, 71, 303–305. [Google Scholar] [CrossRef]
- Eriksson, E.; Hedberg, M.A.; Andersch, B.; Sundblad, C. The serotonin reuptake inhibitor paroxetin is superior to the noradrenaline reuptake inhibitor maprotiline in the treatment of premenstrual syndrome. Neuropsychopharmacology 1995, 12, 167–176. [Google Scholar] [CrossRef]
- Steiner, M.; Steinberg, S.; Stewart, D.; Carter, D.; Berger, C.; Reid, R.; Grover, D.; Streiner, D. Fluoxetine in the treatment of premenstrual dysphoria. Canadian Fluoxetine/Premenstrual Dysphoria Collaborative Study Group. N. Engl. J. Med. 1995, 332, 1529–1534. [Google Scholar] [CrossRef] [PubMed]
- Yonkers, K.A.; Halbreich, U.; Freeman, E.; Brown, C.; Endicott, J.; Frank, E.; Parry, B.; Pearlstein, T.; Severino, S.; Stout, A.; Sertraline Premenstrual Dysphoric Collaborative Study Group. Symptomatic improvement of premenstrual dysphoric disorder with sertraline treatment. A randomized controlled trial. JAMA 1997, 278, 983–988. [Google Scholar] [CrossRef] [PubMed]
- Miner, C.; Brown, E.; McCray, S.; Gonzales, J.; Wohlreich, M. Weekly luteal-phase dosing with enteric-coated fluoxetine 90 mg in premenstrual dysphoric disorder: A randomized, double-blind, placebo-controlled clinical trial. Clin. Ther. 2002, 24, 417–433. [Google Scholar] [CrossRef]
- Bethea, C.L.; Lu, N.Z.; Gundlah, C.; Streicher, J.M. Diverse actions of ovarian steroids in the serotonin neural system. Front. Neuroendocrinol. 2002, 23, 41–100. [Google Scholar] [CrossRef] [PubMed]
- Lu, N.Z.; Eshleman, A.J.; Janowsky, A.; Bethea, C.L. Ovarian steroid regulation of serotonin reuptake transporter (SERT) binding, distribution, and function in female macaques. Mol. Psychiatry 2003, 8, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.J.; Henderson, J.A.; Abell, C.W.; Bethea, C.L. Effects of ovarian steroids and raloxifene on proteins that synthesize, transport, and degrade serotonin in the raphe region of macaques. Neuropsychopharmacology 2004, 29, 2035–2045. [Google Scholar] [CrossRef] [PubMed]
- Millan, M.J.; Marin, P.; Bockaert, J.; Mannoury la Cour, C. Signaling at G-protein-coupled serotonin receptors: Recent advances and future research directions. Trends Pharmacol. Sci. 2008, 29, 454–464. [Google Scholar] [CrossRef] [PubMed]
- Schreiber, G.; Golan, M.; Avissar, S. Beta-arrestin signaling complex as a target for antidepressants and as a depression marker. Drug News Perspect. 2009, 22, 467–480. [Google Scholar] [PubMed]
- Golan, M.; Schreiber, G.; Avissar, S. Antidepressantsincrease beta-arrestin2 ubiquitinylation and degradation by the proteasomal pathway in C6 rat glioma cells. J. Pharmacol. Exp. Ther. 2010, 332, 970–976. [Google Scholar] [CrossRef] [PubMed]
- Golan, M.; Schreiber, G.; Avissar, S. Antidepressant-induced differential ubiquitination of beta-arrestins1 and 2 in mononuclear leucocytes of patients with depression. Int. J. Neuropsychopharmacol. 2013, 16, 1745–1754. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alam, F.; Nayyar, S.; Richie, W.; Archibong, A.; Nayyar, T. Beta-Arrestin1 Levels in Mononuclear Leukocytes Support Depression Scores for Women with Premenstrual Dysphoric Disorder. Int. J. Environ. Res. Public Health 2016, 13, 43. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13010043
Alam F, Nayyar S, Richie W, Archibong A, Nayyar T. Beta-Arrestin1 Levels in Mononuclear Leukocytes Support Depression Scores for Women with Premenstrual Dysphoric Disorder. International Journal of Environmental Research and Public Health. 2016; 13(1):43. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13010043
Chicago/Turabian StyleAlam, Farzana, Sanket Nayyar, William Richie, Anthony Archibong, and Tultul Nayyar. 2016. "Beta-Arrestin1 Levels in Mononuclear Leukocytes Support Depression Scores for Women with Premenstrual Dysphoric Disorder" International Journal of Environmental Research and Public Health 13, no. 1: 43. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13010043