
Color It Real: A Program to Increase Condom Use and Reduce Substance Abuse and Perceived Stress

 and
and
Abstract
:1. Introduction
The Intervention
2. Experimental Section
2.1. Design
2.2. Participants and Procedures
2.3. Instruments
2.4. Analysis
3. Results
3.1. Substance Abuse

{kind=link}
| Characteristic | Total n = 192 | Intervention Group n = 122 | Comparison Group n = 70 | Group Difference p-Value | |
|---|---|---|---|---|---|
| Age | Mean age | 20.4 | 20.4 | 20.3 | 0.3516 |
| n (%) | n (%) | n (%) | |||
| Gender | Male | 49 (25.7%) | 22 (18.0%) | 27 (38.6%) | 0.0019 * |
| Female | 142 (74.4%) | 99 (81.1%) | 43 (61.4%) | ||
| Race | Black/African American | 181 (94.3%) | 118 (96.7%) | 63 (90.0%) | 0.1936 |
| White | 4 (2.1%) | 1 (0.8%) | 3 (4.3%) | ||
| Hispanic/Latino | 4 (2.1%) | 1 (0.8%) | 3 (4.3%) | ||
| Asian | 1 (0.52%) | 1 (0.8%) | 0 (0.0%) | ||
| Other | 2 (1.04%) | 1 (0.8%) | 1 (1.4%) | ||
| Education | Did not complete high school | 63 (32.8) | 48 (39.3%) | 15 (21.4%) | 0.0004 * |
| Completed high school | 59 (30.7) | 42 (34.4%) | 17 (24.3%) | ||
| Some college and higher | 70 (36.5) | 32 (26.2%) | 38 (54.3%) | ||
| Question In the Next 6 Months, How Likely Are You to…? | Group | Pre-Test Mean (SD) | Post-Test Mean (SD) | Intervention Group vs. Comparison Group | |
|---|---|---|---|---|---|
| F-Statistic | p-Value ** | ||||
| To drink five or more alcoholic drinks in one sitting? | Intervention | 1.59 (0.95) | 1.49 (0.94) | 5.10 | 0.0245 * |
| Comparison | 1.84 (1.17) | 2.14 (1.29) | |||
| To use any illegal drugs (including prescription drugs) to get high? | Intervention | 1.33 (0.83) | 1.40 (0.93) | 1.77 | 0.1836 |
| Comparison | 1.72 (1.15) | 1.36 (0.72) | |||
| To use injection drugs without a doctor’s orders, just to feel good or to get high? | Intervention | 1.06 (0.35) | 1.10 (0.54) | 1.16 | 0.2820 |
| Comparison | 1.30 (0.87) | 1.10 (0.51) | |||
| To use clean needles when injecting drugs? | Intervention | 2.20 (1.64) | 3.00 (1.73) | 36.99 | 0.0001 * |
| Comparison | 2.75 (1.54) | 3.00 (1.41) | |||
3.2. Sexual Behavior and Condom Use Intention
| Question | Group | Pre-test Mean (SD) | Post-test Mean (SD) | Intervention Group vs. Comparison Group | |
|---|---|---|---|---|---|
| F-Statistic | p-Value ** | ||||
| The last time you had sex did you use a condom? | Intervention | 0.63(0.49) | 0.75(0.44) | 4.43 | 0.0360 * |
| Comparison | 0.61(0.49) | 0.60(0.49) | |||
| The next time do you plan to use a condom? | Intervention | 0.86(0.34) | 0.90(0.31) | 0.11 | 0.7398 |
| Comparison | 0.85(0.36) | 0.88(0.33) | |||
| In the next 3 months do you plan to use a condom when you have sex? | Intervention | 0.86(0.34) | 0.90(0.30) | 0.13 | 0.7223 |
| Comparison | 0.86(0.35) | 0.87(0.34) | |||
| In the next 3 months do you plan to use a female condom? | Intervention | 0.30(0.46) | 0.37(0.48) | 8.66 | 0.0035 * |
| Comparison | 0.13(0.33) | 0.17(0.38) | |||
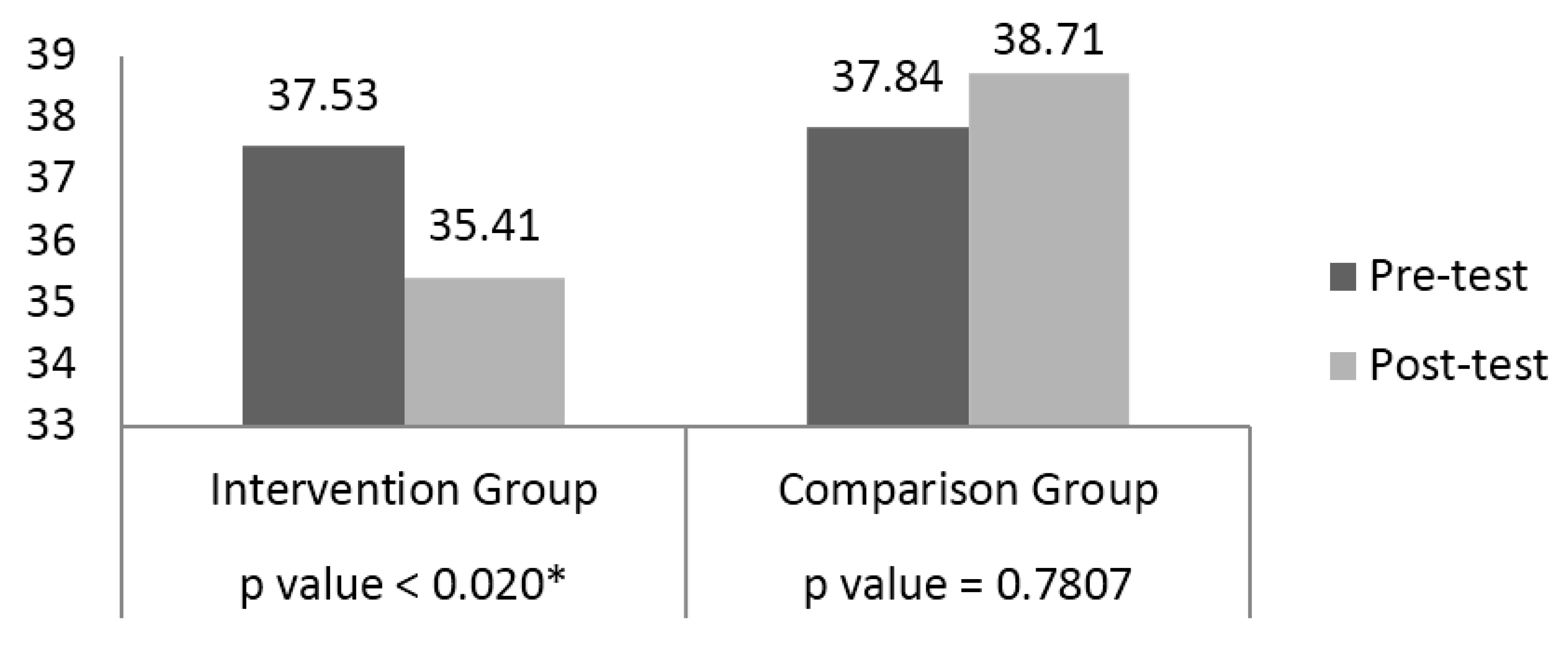
3.3. Perceived Stress

| Question In the Last Month, How Often Have You… | Group | Pre-Test Mean (SD) | Post-Test Mean (SD) | Intervention vs. Comparison Group | |
|---|---|---|---|---|---|
| F-Statistic | p-Value ** | ||||
| Been upset because of something that happened unexpectedly? | Intervention | 3.2 (1.1) | 3.0 (1.1) | 0.03 | 0.8726 |
| Comparison | 3.0 (1.3) | 2.9 (1.1) | |||
| Felt that you were unable to control the important things in your life? | Intervention | 2.9 (1.2) | 2.5 (1.3) | 0.03 | 0.8638 |
| Comparison | 2.7 (1.2) | 2.8 (1.1) | |||
| Felt nervous and stressed? | Intervention | 3.3 (1.2) | 3.0 (1.2) | 0.89 | 0.3456 |
| Comparison | 3.3 (1.2) | 2.9 (1.1) | |||
| Felt confident about your ability to handle your personal problems? | Intervention | 2.1 (1.1) | 2.0 (1.1) | 11.98 | 0.0006 * |
| Comparison | 2.4 (1.2) | 2.6 (1.2) | |||
| Felt that things were going your way? | Intervention | 2.7 (1.0) | 2.4 (1.1) | 2.30 | 0.1306 |
| Comparison | 2.7 (1.0) | 2.8 (1.1) | |||
| Found that you could not cope with all the things that you had to do? | Intervention | 2.9 (1.1) | 2.5 (1.1) | 1.62 | 0.2042 |
| Comparison | 2.8 (1.1) | 2.8 (1.2) | |||
| Been able to control irritations in your life? | Intervention | 2.5 (1.1) | 2.3 (1.1) | 5.15 | 0.0240 * |
| Comparison | 2.5 (1.1) | 3.0 (1.1) | |||
| Felt that you were on top of things? | Intervention | 2.3 (1.0) | 2.1 (1.0) | 8.06 | 0.0049 |
| Comparison | 2.4 (1.0) | 2.8 (1.1) | |||
| In the last month, how often have you been angered because of things that happened that were outside of your control? | Intervention | 3.0 (1.2) | 2.7 (1.1) | 0.88 | 0.3483 |
| Comparison | 2.9 (1.3) | 2.8 (1.0) | |||
| Felt difficulties were piling up so high that you could not overcome them? | Intervention | 2.6 (1.2) | 2.5 (1.3) | 3.24 | 0.0728 |
| Comparison | 2.8 (1.2) | 2.7 (1.1) | |||
| Been able to overcome being upset to handle something unexpectedly? | Intervention | 2.6 (1.2) | 2.5 (1.2) | 2.80 | 0.0956 |
| Comparison | 2.8 (1.1) | 2.8 (1.1) | |||
| Felt calm and grounded? | Intervention | 2.2 (1.0) | 2.2 (1.2) | 8.87 | 0.0032 * |
| Comparison | 2.4 (1.1) | 2.6 (1.1) | |||
| Found that you were coping well with all the things that you had to do? | Intervention | 2.4 (1.0) | 2.2 (1.1) | 2.90 | 0.0894 |
| Comparison | 2.4 (1.2) | 2.7 (1.1) | |||
| Had challenges that were piling up so high and that you were able to overcome them? | Intervention | 3.0 (1.2) | 3.3 (1.2) | 0.01 | 0.9426 |
| Comparison | 3.1 (1.2) | 2.9 (1.2) | |||
4. Discussion
4.1. Strengths
4.2. Limitations
4.3. Implications for Future Research
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- CDC. HIV Among Youth Fact Sheet; 2013. Available online: http://www.cdc.gov/hiv/group/age/youth/index.html (accessed on 2 December 2015).
- CDC. HIV/AIDS Fact Sheet: HIV among African Americans; 2011. Available online: http://www.cdc.gov/hiv/group/racialethnic/africanamericans/ (accessed on 2 December 2015).
- DCH. Georgia HIV/AIDS Surveillance Summary: Data through 31 December 2009; 2010. Available online: http://www.georgiaaids.org/files/GA-HIV-AIDS_Surveillance-Summary.pdf (accessed on 2 December 2015).
- Carter, M.W.; Kraft, J.M.; Hatfield-Timajchy, K.; Hock-Long, L.; Hogben, M. STD and HIV Testing Behaviors Among Black And Puerto Rican Young Adults. Perspect. Sex. Reprod. Health 2011, 43, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, B.L.; Roberts, S.T. Truths and Myths That Influence the Sexual Decision-Making Process Among Young Multiethnic College Women. Arch. Psychiatr. Nurs. 2009, 23, 366–375. [Google Scholar] [CrossRef] [PubMed]
- Kogan, S.M.; Brody, G.H.; Chen, Y.F.; Grange, C.M.; Slater, L.M.; di Clemente, R.J. Risk and Protective Factors for Unprotected Intercourse Among Rural African American Young Adults. Public Health Rep. 2010, 125, 709–717. [Google Scholar] [PubMed]
- Randolph, M.E.; Torres, H.; Gore-Felton, C.; Lloyd, B.; McGarvey, E.L. Alcohol Use and Sexual Risk Behavior among College Students: Understanding Gender and Ethnic Differences. Am. J. Drug Alcohol Abus. 2009, 35, 80–84. [Google Scholar] [CrossRef] [PubMed]
- Enoch, M.A. The role of early life stress as a predictor for alcohol and drug dependence. Psychopharmacology 2011, 214, 17–31. [Google Scholar] [CrossRef] [PubMed]
- Bluthenthal, R.; Do, D.P.; Finch, B.; Martinez, A.; Edlin, B.R.; Kral, A.H. Community Characteristics Associated with HIV Risk among Injection Drug Users in the San Francisco Bay Area: A Multilevel Analysis. J. Urban Health 2007, 84, 653–666. [Google Scholar] [CrossRef] [PubMed]
- Lampinen, T.M.; Joo, E.; Seweryn, S.; Hershow, R.C.; Wiebel, W. HIV seropositivity in community-recruited and drug treatment samples of injecting drug users. AIDS 1992, 6, 123–126. [Google Scholar] [CrossRef] [PubMed]
- Anthenelli, R.M. Overview: Stress and alcohol use disorders revisited. Alcohol Res. Curr. Rev. 2012, 34, 386. [Google Scholar]
- Keyes, K.M.; Hatzenbuehler, M.L.; Grant, B.F.; Hasin, D.S. Stress and Alcohol: Epidemiologic Evidence. Alcohol Res. Curr. Rev. 2012, 34, 391–400. [Google Scholar]
- Gee, G.C. A Multilevel Analysis of the Relationship Between Institutional and Individual Racial Discrimination and Health Status. Am. J. Public Health 2002, 92, 615–623. [Google Scholar] [CrossRef] [PubMed]
- Adimora, A.A.; Schoenbach, V.J. Social Context, Sexual Networks, and Racial Disparities in Rates of Sexually Transmitted Infections. J. Infect. Dis. 2005, 191 (Suppl. S1), S115–S122. [Google Scholar] [CrossRef] [PubMed]
- Barrow, R.Y.; Berkel, C.; Brooks, L.C.; Groseclose, S.L.; Johnson, D.B.; Valentine, J.A. Traditional Sexually Transmitted Disease Prevention and Control Strategies: Tailoring for African American Communities. Sex. Transm. Dis. 2008, 35 (Suppl. S12), S30–S39. [Google Scholar] [CrossRef] [PubMed]
- Freeman, C. The missing element: Incorporating culturally-specific clinical practices in HIV prevention programs for African-American females. J. Cult. Divers. 2010, 17, 51–55. [Google Scholar] [PubMed]
- Mongkuo, M.Y.; Mushi, R.J.; Thomas, R. Perception of HIV/AIDS and socio-cognitive determinants of safe sex practices among college students attending a historically black college and university in the United States of America. J. AIDS HIV Res. 2010, 2, 32–47. [Google Scholar]
- Peterson, J.L.; Jones, K.T. HIV Prevention for Black Men Who Have Sex With Men in the United States. Am. J. Public Health 2009, 99, 976–980. [Google Scholar] [CrossRef] [PubMed]
- Wyatt, G.E. Enhancing Cultural and Contextual Intervention Strategies to Reduce HIV/AIDS Among African Americans. Am. J. Public Health 2009, 99, 1941–1945. [Google Scholar] [CrossRef] [PubMed]
- Baker, J.L.; Brawner, B.; Cederbaum, J.A.; White, S.; Davis, Z.M.; Brawner, W.; Jemmott, L.S. Barbershops as venues to assess and intervene in HIV/STI risk among young, heterosexual African American men. Am. J. Men’s Health 2012, 6, 368–382. [Google Scholar] [CrossRef] [PubMed]
- Fisher, H.H.; Patel-Larson, A.; Green, K.; Shapatava, E.; Uhl, G.; Kalayil, E.J.; Moore, A.; Williams, W.; Chen, B. Evaluation of an HIV prevention intervention for African Americans and Hispanics: Findings from the VOICES/VOCES community-based organization behavioral outcomes project. AIDS Behav. 2011, 15, 1691–1706. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, S.B.; Nolen, S.; Pan, Z.; Smith, B.; Applewhite, J.; Vanderhoff, K.J. Effectiveness of a brief condom promotion program in reducing risky sexual behaviours among African American men. J. Eval. Clin. Pract. 2013, 19, 408–413. [Google Scholar] [CrossRef] [PubMed]
- Latkin, C.A.; Sherman, S.; Knowlton, A. HIV prevention among drug users: Outcome of a network-oriented peer outreach intervention. Health Psychol. 2003, 22, 332. [Google Scholar] [CrossRef] [PubMed]
- Hou, S.I. HIV-related behaviors among black students attending Historically Black Colleges and Universities (HBCUs) versus white students attending a traditionally white institution (TWI). AIDS Care 2009, 21, 1050–1057. [Google Scholar] [CrossRef] [PubMed]
- Rose, M.S. African American college freshman students’ knowledge, attitudes, beliefs, and behaviors related to HIV: A preliminary investigation. Int. J. Allied Health Sci. Pract. 2008, 6, 9. [Google Scholar]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84, 191. [Google Scholar] [CrossRef] [PubMed]
- Bandura, E.A. Self-Efficacy: The Exercise of Control. Available online: http://0-search-proquest-com.brum.beds.ac.uk/openview/55c56d1a75f8440c4bea93781b0dc952/1?pq-origsite=gscholar#top (accessed on 2 December 2015).
- Becker, M.H. The Health Belief Model and Preventive Health Behavior. Health Educ. Monogr. 1974, 2, 354–386. [Google Scholar] [CrossRef]
- Carpenter, C.J. A meta-analysis of the effectiveness of health belief model variables in predicting behavior. Health Commun. 2010, 25, 661–669. [Google Scholar] [CrossRef] [PubMed]
- Brest, P. The power of theories of change. Stanf. Soc. Innov. Rev. 2010, 8, 47–51. [Google Scholar]
- SAMHSA. National Minority SA/HIV Prevention Initiative, Cohort 6 Adult Questionnaire; 2008. Available online: http://www.samhsa.gov/grants/gpra-measurement-tools/csap-gpra (accessed on 2 December 2015).
- CDC. Street Smart Evaluation Field Guide; 2008. Available online: https://effectiveinterventions.cdc.gov/Files/Street_Smart_Eval_Field_Guide_09-1023.pdf (accessed on 2 December 2015).
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Ickovics, J.R.; Beren, S.E.; Grigorenko, E.L.; Morrill, A.C.; Druley, J.A.; Rodin, J. Pathways of risk: Race, social class, stress, and coping as factors predicting heterosexual risk behaviors for HIV among women. AIDS Behav. 2002, 6, 339–350. [Google Scholar] [CrossRef]
- El-Bassel, N.; Caldeira, N.A.; Ruglass, L.M.; Gilbert, L. Addressing the unique needs of African American women in HIV prevention. Am. J. Public Health 2009, 99, 996. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zellner, T.; Trotter, J.; Lenoir, S.; Walston, K.; Men-Na’a, L.; Henry-Akintobi, T.; Miller, A. Color It Real: A Program to Increase Condom Use and Reduce Substance Abuse and Perceived Stress. Int. J. Environ. Res. Public Health 2016, 13, 51. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13010051
Zellner T, Trotter J, Lenoir S, Walston K, Men-Na’a L, Henry-Akintobi T, Miller A. Color It Real: A Program to Increase Condom Use and Reduce Substance Abuse and Perceived Stress. International Journal of Environmental Research and Public Health. 2016; 13(1):51. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13010051
Chicago/Turabian StyleZellner, Tiffany, Jennie Trotter, Shelia Lenoir, Kelvin Walston, L’dia Men-Na’a, Tabia Henry-Akintobi, and Assia Miller. 2016. "Color It Real: A Program to Increase Condom Use and Reduce Substance Abuse and Perceived Stress" International Journal of Environmental Research and Public Health 13, no. 1: 51. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13010051