How Well Do Health-Mediation Programs Address the Determinants of the Poor Health Status of Roma? A Longitudinal Case Study

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting and Sample
2.2. Measures and Procedure
2.3. Analyses and Reporting
2.4. Ethics Approval
3. Results
3.1. The HMP Agenda
3.1.1. Intermediary SDH
3.1.2. Structural SDH
3.1.3. Socio-Political Context
3.2. The HMP Everyday Implementation
3.2.1. Intermediary SDH
3.2.2. Structural SDH
3.2.3. Socio-Political Context
4. Discussion
Strengths and Limitations
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix A
| Descriptions of the program agenda and practice Project Healthy Communities—Description of the Healthy Communities project [Projekt Zdravé komunity-Popis projektu Zdravé komunity] (2013) Healthy Communities—Final report [Zdravé komunity Záverečná správa] (2014) The statute of the association of legal entities Platform for promotion of the health of disadvantaged groups [Stanovy občianskeho združenia Platforma pre podporu zdravia znevýhodnených skupín] (2014) National project ‘Healthy Communities’ proposal [Zámer národného projektu Zdravé komunity] (2014, 2015) Project Healthy Communities Application Appendix 1—Project description [Žiadosť o poskytnutie nenávratného finančného príspevku Príloha 1—Opis projektu] (2014, 2015) Job specification for the Health edification assistant role [Pracovná náplň Asistenta osvety zdravia] (2014) Job specification for the Coordinator of the Health edification assistants role [Pracovná náplň Koordinátora asistentov zdravotnej osvety] (2014) Health edification assistant role activity sheets [Pracovné výkazy asistentov osvety zdravia] (2014, 2015) Recruitment forms Health edification assistant questionnaire [Dotazník pre asistentov/ky osvety zdravia] (2014) Coordinator of the Health edification assistants questionnaire [Dotazník pre koordinátorov asistentov osvety zdravia] (2014) Curriculum form [Formulár Životopis] (2014) Training documentation and materials The health edification assistant role [Úloha asistenta zdravotnej osvety] (2014) Care for pregnant women and new-borns [Starostlivosť o tehotné ženy a novorodencov] (2014) Human biology basics [Základy biológie človeka] (2014) Epidemiology [Epidemiológia] (2014) Basic communication skills for work within the Roma communities [Základné komunikačné zručnosti v práci s rómskymi komunitami] (2014) Specialized social counselling with respect to health care [Špecializované sociálne poradenstvo v oblasti zdravotníctva] (2014) |
Appendix B
| The program participation in the context of the participant’s life How did your life change after you took up your position within the program (explain the positives and negatives)? What do you like/don’t like about your current job? Personal account of segregated Roma health status Do you think there are differences in health between the Roma and the non-Roma? Based on what? If so, where do you think these differences come from? Based on what? What do you think could be done in order to alleviate these differences? Based on what? Personal account of the program agenda Why did the program start and who started it? Using what money? Where do you know this from? What does the program management claim it wants to achieve? What do you think the program management wants to achieve in reality? Where do you know these things from? How do you think the management wants to achieve these things? Where do you know this from? Do you think the program should focus on and should be doing something else as well? Why? Do you think enough attention is paid in the program set-up to whatever damages people’s health directly (e.g., material conditions, circumstances causing stress, risky health behaviours, specific bodily characteristics, and access to healthcare)? How? Do you think enough attention is paid in the program set-up to whatever else might be contributing to the worse health in the segregated communities (e.g., education, occupation, income, gender roles, and incidents of racism)? How? Do you think the program is well set-up to positively influence whatever might be affecting the health in the segregated communities at the country level (e.g., how these issues are governed centrally, particular related policies, the wide-spread anti-Roma racism) How? Personal account of the program practice Which of its goals is the program successful at achieving? How come? Based on what do you think that? Which of its goals is the program unsuccessful at achieving? How come? Based on what do you think that? Do you think the program is successful at dealing with whatever damages people’s health directly (e.g., material conditions, circumstances causing stress, risky health behaviours, specific bodily characteristics, and access to healthcare)? In what in particular? Based on what do you think that? What else should be done in this area and what should be done differently? Why? Do you think the program is successful at dealing with whatever else might be contributing to the worse health in the segregated communities (e.g., education, occupation, income, gender roles, and incidents of racism)? In what in particular? Based on what do you think that? What else should be done in this area and what should be done differently? Why? Do you think the program is successful at positively influencing whatever might be affecting the health in the segregated communities at the country level (e.g., how these issues are governed centrally, particular related policies, the wide-spread anti-Roma racism)? Based on what do you think that? What else should be done in this area and what should be done differently? Why? |
References
- Crowe, D. A History of the Gypsies of Eastern Europe and Russia, 2nd ed.; Palgrave/Macmilan: New York, NY, USA, 2007; 391p. [Google Scholar]
- Stewart, M. The Gypsy Menace: Populism and the New Anti-Gypsy Politics; Hurst & Company: London, UK, 2012. [Google Scholar]
- Stewart, M. Roma and Gypsy “ethnicity” as a subject of anthropological inquiry. Annu. Rev. Anthropol. 2013, 42, 415–432. [Google Scholar] [CrossRef]
- Barany, Z.D. The East European Gypsies: Regime Change, Marginality, and Ethnopolitics; Cambridge University Press: Cambridge, UK; New York, NY, USA, 2002; 408p. [Google Scholar]
- Vermeersch, P. Reframing the Roma: EU initiatives and the politics of reinterpretation. J. Ethn. Migr. Stud. 2012, 38, 1195–1212. [Google Scholar] [CrossRef]
- FSG. Health and the Roma Community: Analysis of the Situation in Europe. Bulgaria, Czech Republic, Greece, Portugal, Romania, Slovakia, Spain; FSG: Madrid, Spain, 2009. [Google Scholar]
- EUC. The Situation of Roma in an Enlarged European Union; European Commission—Directorate-General for Employment and Social Affairs: Luxembourg, 2004. [Google Scholar]
- EUC. Roma Health Report. Health Status of the Roma Population. Data Collection in the Member States of the European Union; EUC: Luxembourg, 2014; p. 153. [Google Scholar]
- Cook, B.; Wayne, G.F.; Valentine, A.; Lessios, A.; Yeh, E. Revisiting the evidence on health and health care disparities among the Roma: A systematic review 2003–2012. Int. J. Public Health 2013, 58, 885–911. [Google Scholar] [CrossRef] [PubMed]
- Hajioff, S.; McKee, M. The health of the Roma people: A review of the published literature. J. Epidemiol. Community Health 2000, 54, 864–869. [Google Scholar] [CrossRef] [PubMed]
- Open Society Foundations (OSF). Roma Health Mediators: Successes and Challenges; Open Society Foundations: New York, NY, USA, 2011; p. 84. [Google Scholar]
- World Health Organization (WHO). Roma Health Mediation in Romania; World Health Organization Europe: Copenhagen, Denmark, 2013. [Google Scholar]
- Open Society Institute (OSI). Mediating Romani Health: Policy and Program Opportunities; Open Society Institute Network Public Health Program New York: New York, NY, USA, 2005. [Google Scholar]
- Koller, T. (Ed.) Poverty and Social Exclusion in the WHO European Region: Health Systems Respond; World Health Organization: Copenhagen, Denmark, 2010. [Google Scholar]
- Fésüs, G.; Östlin, P.; McKee, M.; Ádány, R. Policies to improve the health and well-being of Roma people: The European experience. Health Policy 2012, 105, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Krieger, N. Epidemiology and the People’s Health: Theory and Context; Oxford University Press: New York, NY, USA, 2011; 381p. [Google Scholar]
- Berkman, L.F.; Kawachi, I.; Glymour, M.M. Social Epidemiology; Oxford University Press: Oxford, UK, 2014. [Google Scholar]
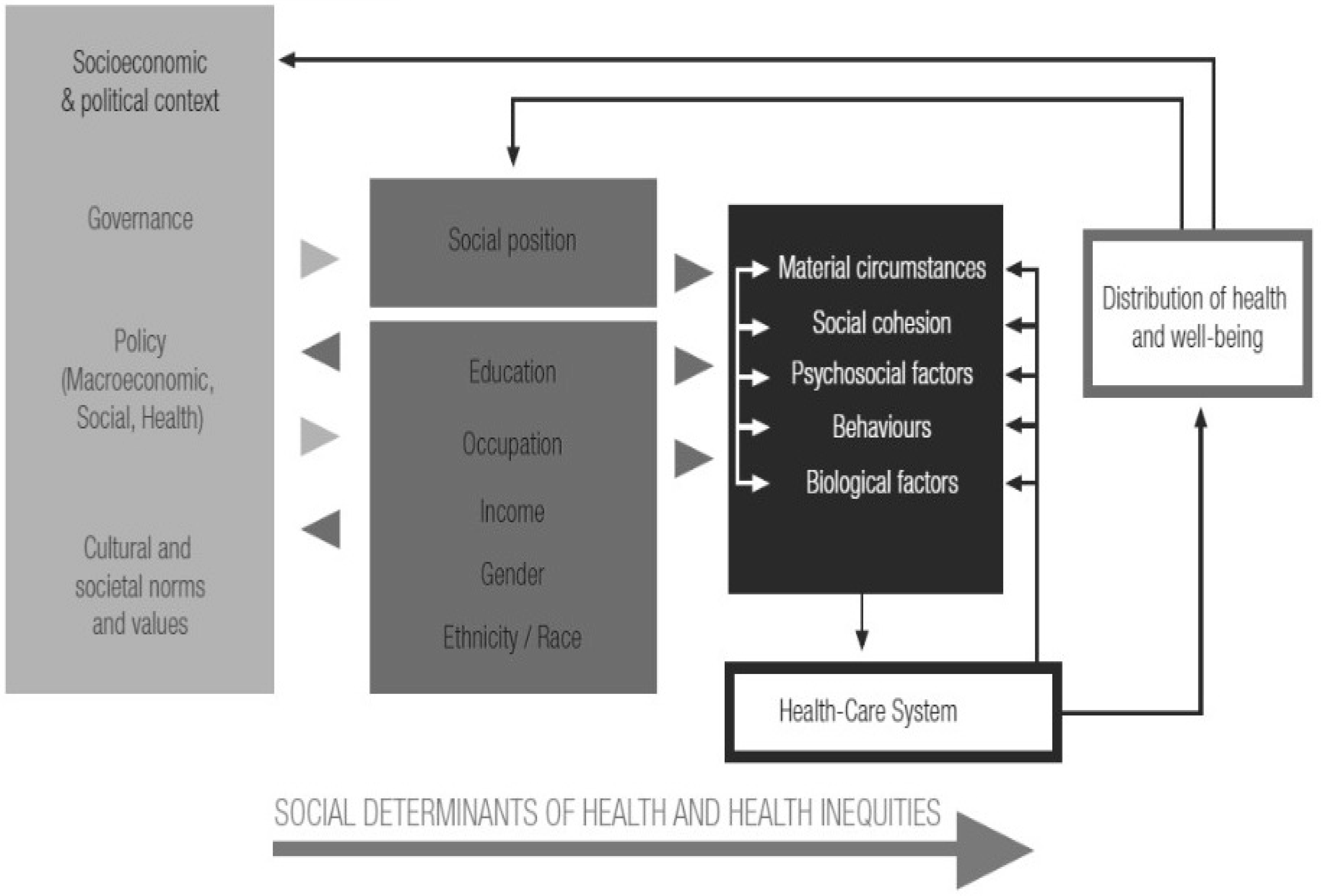
- WHO. A Conceptual Framework for Action on the Social Determinants of Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Kaplan, G.A. What’s wrong with social epidemiology, and how can we make it better? Epidemiol. Rev. 2004, 26, 124–135. [Google Scholar] [CrossRef] [PubMed]
- JSI. Research-Evaluation of the Helath Mediatiors Program within Roma Communities in Romania; JSI: Bucharest, Romania, 2006. [Google Scholar]
- Schneeweis, A. Empowered leaders and alone in community: Stories of Romanian Roma health mediators. Women’s Stud. Commun. 2013, 36, 167–188. [Google Scholar] [CrossRef]
- Slusna, L. Slovakia: Healthy communities. In Poverty and Social Exclusion in the WHO European Region: Health Systems Respond; Koller, T., Ed.; WHO Regional Office for Europe: Copenhagen, Denmark, 2010. [Google Scholar]
- Musinka, A.; Skobla, D.; Hurrle, J.; Matlovicova, K.; Kling, J. Atlas of Roma Communities in Slovakia 2013 [Atlas Rómskych Komunít na Slovensku 2013]; UNDP: Bratislava, Slovakia, 2014; p. 120. [Google Scholar]
- Belak, A.; Geckova, A.M.; van Dijk, J.P.; Reijneveld, S.A. Health-endangering everyday settings and practices in a rural segregated Roma settlement in Slovakia: A descriptive summary from an exploratory longitudinal case study. BMC Public Health 2017, 17, 128. [Google Scholar] [CrossRef] [PubMed]
- Goodyear, L.; Barela, E.; Jewiss, J.; Usinger, J. Qualitative Inquiry in Evaluation: From Theory to Practice; John Wiley & Sons: Hoboken, NJ, USA, 2014. [Google Scholar]
- Reeves, S.; Kuper, A.; Hodges, B.D. Qualitative research methodologies: Ethnography. BMJ 2008, 337, a1020. [Google Scholar] [CrossRef] [PubMed]
- Hammersley, M.; Atkinson, P. Ethnography: Principles in Practice, 3rd ed.; Routledge: London, UK; New York, NY, USA, 2007; 275p. [Google Scholar]
- WHO. Review of Social Determinants and the Health Divide in the WHO European Region: Final Report; WHO Regional Office for Europe: Copenhagen, Denmark, 2013; p. 188. [Google Scholar]
- Brown, C.; Harrison, D. Governance for Health Equity in the WHO European Region; WHO: Copenhagen, Denmark, 2013; p. 63. [Google Scholar]
- Garthwaite, K.; Smith, K.E.; Bambra, C.; Pearce, J. Desperately seeking reductions in health inequalities: Perspectives of UK researchers on past, present and future directions in health inequalities research. Sociol. Health Illn. 2016, 38, 459–478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsieh, H.-F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef] [PubMed]
- LeCompte, M.D.; Schensul, J.J. Analysis and Interpretation of Ethnographic Data: A Mixed Methods Approach, 2nd ed.; Ethnographer’s Toolkit; AltaMira Press: Lanham, MD, USA, 2013; 338p. [Google Scholar]
- Conrad, P. The Medicalization of Society: On the Transformation of Human Conditions into Treatable Disorders; Johns Hopkins University Press: Baltimore, MD, USA, 2007; 204p. [Google Scholar]
- McQueen, D.V.; Kickbusch, I.; Potvin, L.; Pelikan, J.M.; Balbo, L.; Abel, T. Health and Modernity: The Role of Theory in Health Promotion; Springer: Berlin/Heidelberg, Germany, 2007. [Google Scholar]
- Kreuter, M.W.; Lukwago, S.N.; Bucholtz, D.C.; Clark, E.M.; Sanders-Thompson, V. Achieving cultural appropriateness in health promotion programs: Targeted and tailored approaches. Health Educ. Behav. 2003, 30, 133–146. [Google Scholar] [CrossRef] [PubMed]
- Kringos, D.S.; Boerma, W.G.; van der Zee, J.; Groenewegen, P.P. Political, cultural and economic foundations of primary care in Europe. Soc. Sci. Med. 2013, 99, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Úrad Predsedníctva Zboru Povereníkov (ÚPZP). Work among the Gypsy Population. Handbook for National Committees [Praca Medzi Ciganskym Obyvatelstvom. Prirucka pre Narodne Vybory]; Úrad Predsedníctva Zboru Povereníkov: Bratislava, Slovakia, 1959. [Google Scholar]
- Belak, A. Segregated Roma and health policies: Ethical and practical contradictions [Segregovani Romovia a zdravotne politiky: Eticke a prakticke rozpory]. In Cierno-Biele Svety. Romovia v Majoritnej Spoločnosti na Slovensku; Podolinska, T., Hrustic, T., Eds.; VEDA Ustav Etnologie Slovenskej Akademie Vied: Bratislava, Slovakia, 2015. [Google Scholar]
- Ivasiuc, A. Empowering the Roma. Lessons from the Development Practice. Ph.D. Thesis, Unversity of Bucharest, Bucharest, Romania, 2014. [Google Scholar]
- Hickey, S.; Mohan, G. Participation—From Tyranny to Transformation: Exploring New Approaches to Participation in Development; Zed Books: London, UK, 2004. [Google Scholar]
- Merzel, C.; D’afflitti, J. Reconsidering community-based health promotion: Promise, performance, and potential. Am. J. Public Health 2003, 93, 557–574. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, U.; Sanders, D. Community health workers: What do we know about them. In The State of the Evidence on Programmes, Activities, Costs and Impact on Health Outcomes of Using Community Health Workers; World Health Organization: Geneva, Switzerland, 2007; pp. 1–42. [Google Scholar]
- Labonte, R.N.; Laverack, G. Health Promotion in Action: From Local to Global Empowerment; Palgrave Macmillan: Basingstoke, UK, 2008. [Google Scholar]
- Singer, M.K.; Dressler, W.; George, S.; Panel, T.N.E. Culture: The missing link in health research. Soc. Sci. Med. 2016, 170, 237–246. [Google Scholar] [CrossRef] [PubMed]
- Napier, A.D.; Ancarno, C.; Butler, B.; Calabrese, J.; Chater, A.; Chatterjee, H.; Guesnet, F.; Horne, R.; Jacyna, S.; Jadhav, S. Culture and health. Lancet 2014, 384, 1607–1639. [Google Scholar] [CrossRef]


{kind=link}
| HMP Organizational Structure 1 | HMP Recipients | ||||
|---|---|---|---|---|---|
| Fieldworkers | Central Management | ||||
| Assistants | Coordinators | Management | Executive Board | ||
| No. of persons | 200 | 20 | 6 | 4 | Approx. 60,000 |
| Main duties | Community-based health education and facilitation of healthcare access | Support and supervision of the HM assistants | HMP operational management and public relations | Strategic decision-making, fund-raising and lobbying | N/A |
| Criteria for hiring | Completed elementary education; residency in the community of service & personal motivation (brief questionnaire) | completed secondary education; proficiency in Romani language; related previous experience and personal motivation (interview) | Previous related experience and personal motivation (interview) | N/A | N/A |
| Roma/non-Roma Ethnicity | Self-declared Roma, with few exceptions | Self-declared Roma, with one exception | Self-declared non-Roma, with one exception | Self-declared Non-Roma | Self-declared Roma |
| Approx. female: male ratio | 3:1 | 1:1 | 2:1 | 1:1 | 1:1 |
| Location of participants’ practice/target communities | Community-based, 1 per segregated settlement | Rotating visits of 10 assistants working in 1 area | In Bratislava | In Bratislava | Across the country, in 23 counties |
| Final Sample Structure | |||||
| Number of job-shadowed or long-term observed respondents/Study phase(s); Observation length per person | 9 Phase 1; 1–3 weeks | 1 Phase 1; 3 months | 4 Phases 1 + 2; 3 to 14 days | 0 N/A | 18 Phase 1; 1–4 weeks |
| Number of occasionally observed and informally elicited respondents/Study phases | 61 Phases 1 + 2 | 6 Phases 1 + 2 | 7 Phases 1 + 2 | 3 Phases 1 + 2 | 39 Phases 1 + 2 |
| Number of persons who attended both structured and follow-up interviews/Study Phase | 5 Phase 2 | 4 Phase 2 | 3 Phase 2 | 1 Phase 2 | 0 N/A |
| Final Sample Size | 116 2 | ||||
| SDH to Be Addressed According to the WHO SDH Framework | How Well Did the HMP Address the Recommended SDH? | |
|---|---|---|
| In Its Agenda | In Its Everyday Implementation | |
| Intermediary determinants |
|
|
 |  | |
| Structural determinants | Social positions of the program recipients were not supposed to be addressed systematically |
|
 | | |
| Socio-political context | Socio-political context was not supposed to be addressed |
|
| | | |
designates ‘partially’, designates ‘well’, and designates ‘poorly’; we use the symbols to summarize how well the HMP addressed each main category of SDH according to the listed main findings.© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Belak, A.; Veselska, Z.D.; Geckova, A.M.; Dijk, J.P.v.; Reijneveld, S.A. How Well Do Health-Mediation Programs Address the Determinants of the Poor Health Status of Roma? A Longitudinal Case Study. Int. J. Environ. Res. Public Health 2017, 14, 1569. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph14121569
Belak A, Veselska ZD, Geckova AM, Dijk JPv, Reijneveld SA. How Well Do Health-Mediation Programs Address the Determinants of the Poor Health Status of Roma? A Longitudinal Case Study. International Journal of Environmental Research and Public Health. 2017; 14(12):1569. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph14121569
Chicago/Turabian StyleBelak, Andrej, Zuzana Dankulincova Veselska, Andrea Madarasova Geckova, Jitse P. van Dijk, and Sijmen A. Reijneveld. 2017. "How Well Do Health-Mediation Programs Address the Determinants of the Poor Health Status of Roma? A Longitudinal Case Study" International Journal of Environmental Research and Public Health 14, no. 12: 1569. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph14121569