Evaluation of Fitness and the Balance Levels of Children with a Diagnosis of Juvenile Idiopathic Arthritis: A Pilot Study

 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Context
2.2. Method of Testing
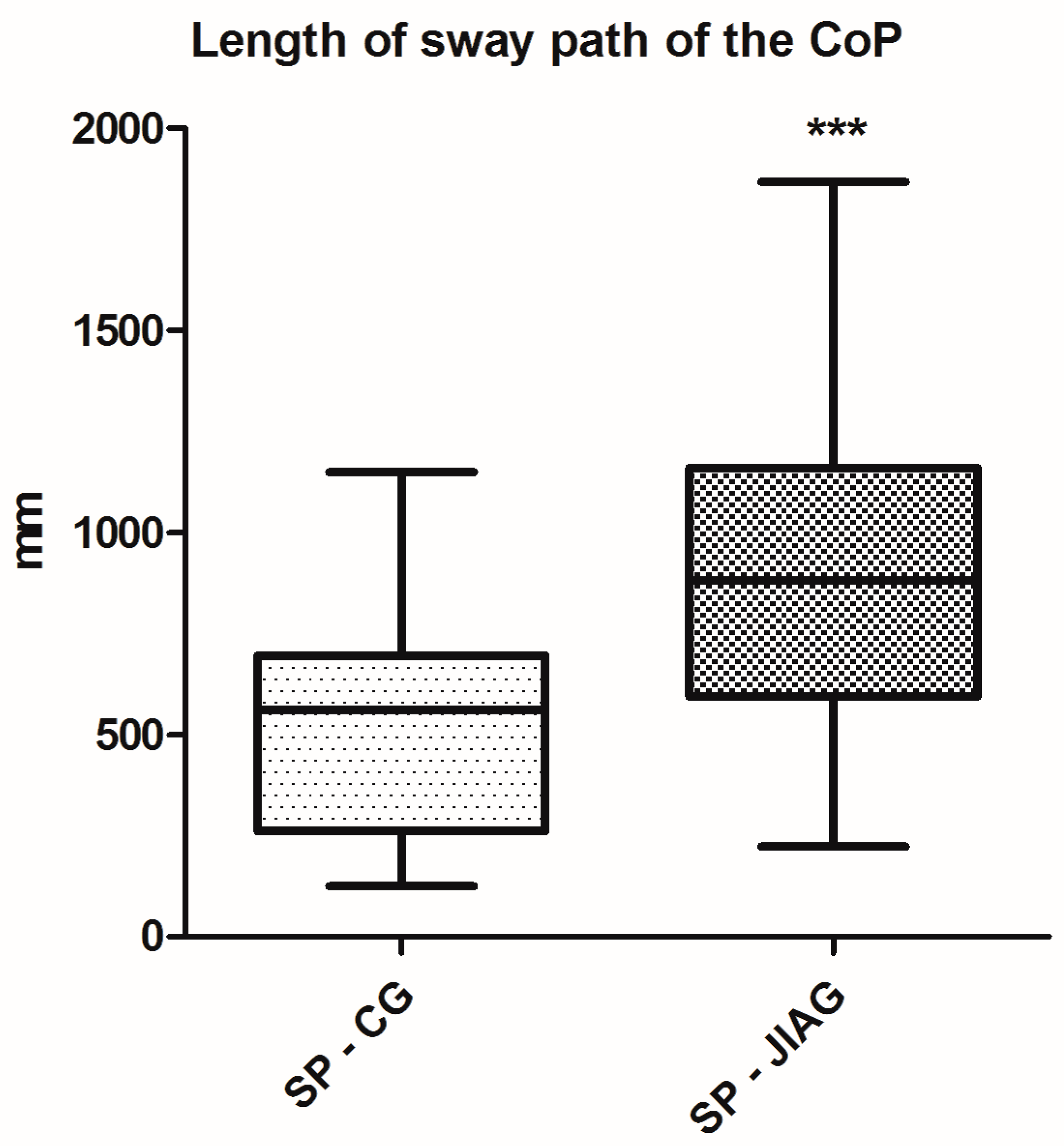
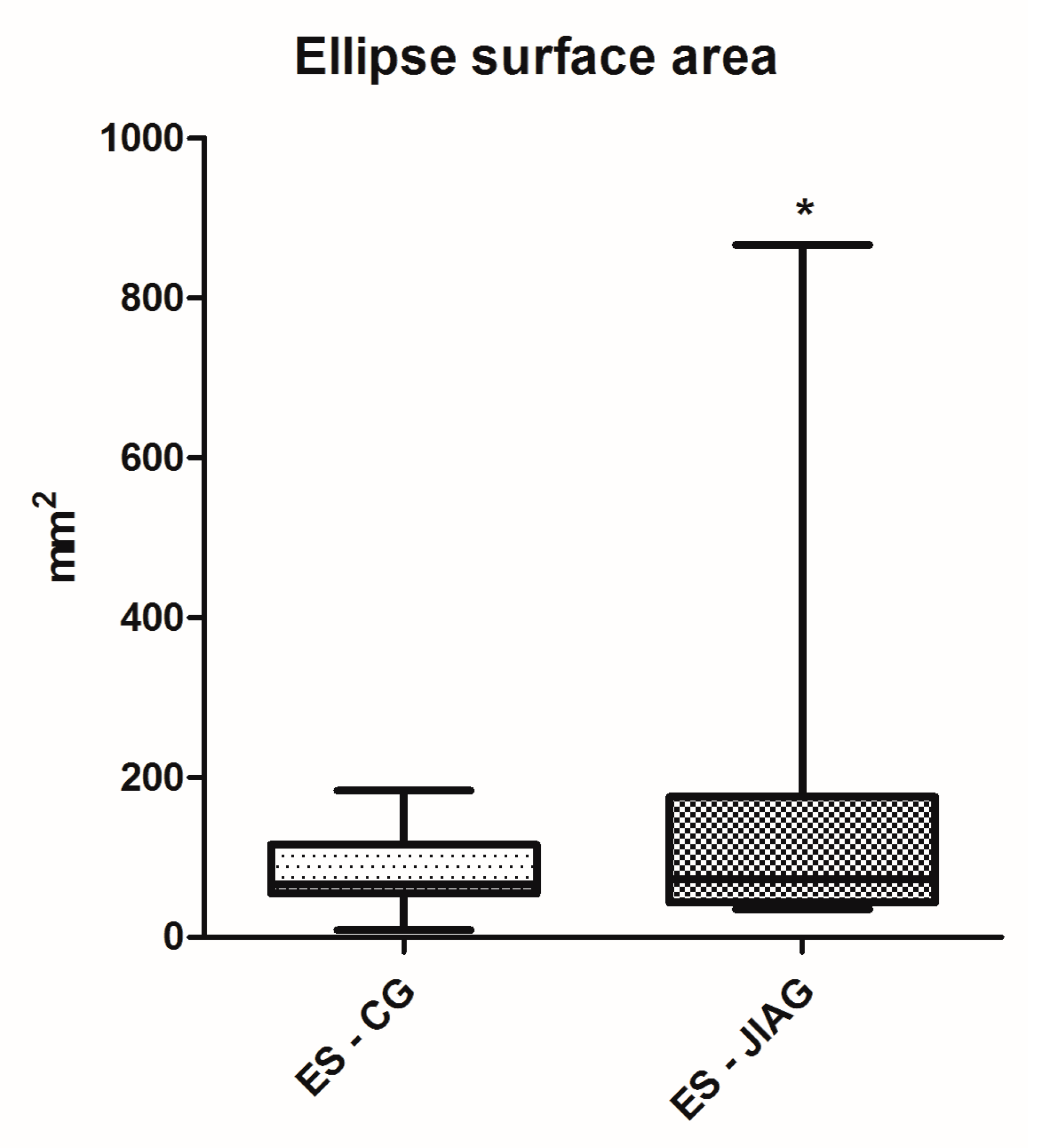
2.2.1. The Posturography Analysis
2.2.2. Fitness Test Battery
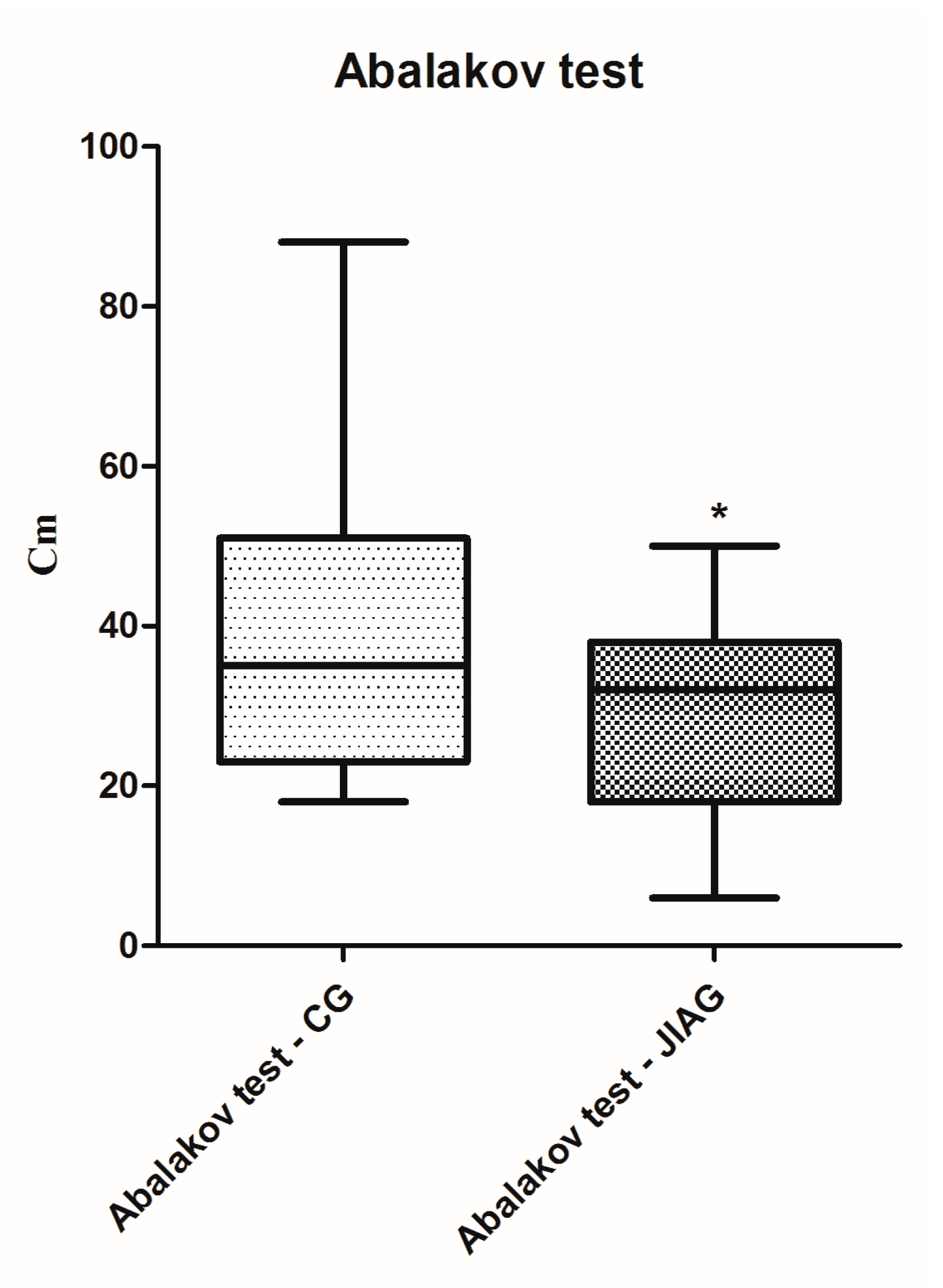
- Abalakov test [36]: when ready, the subject squats down until the knees are bent at a 90° angle while swinging the arms back behind the body; the arms move forward and the participants jumps as high as possible. The Abalakov jump is specific for maximal strength, and it is expressed on a vertical plane [31];
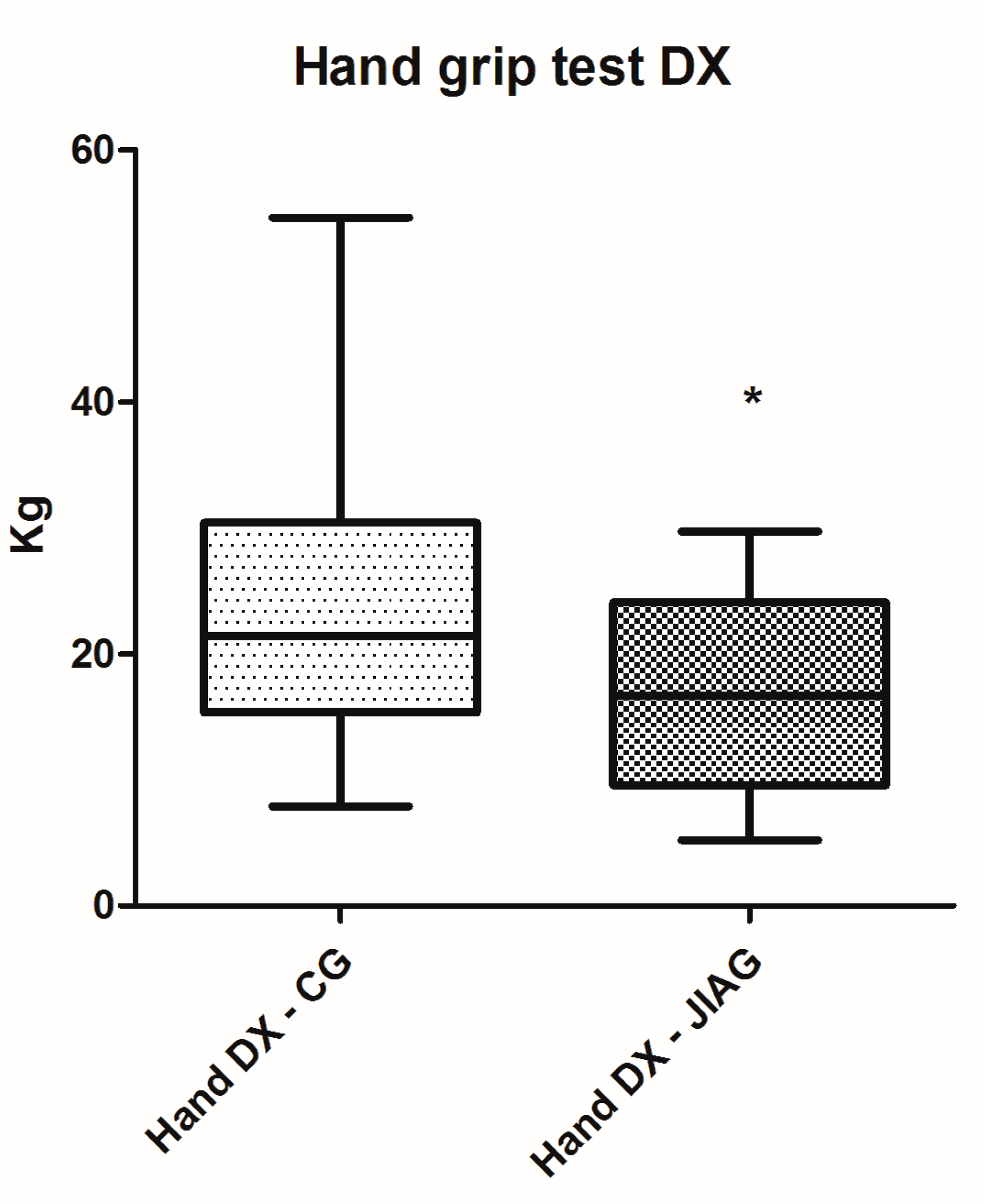
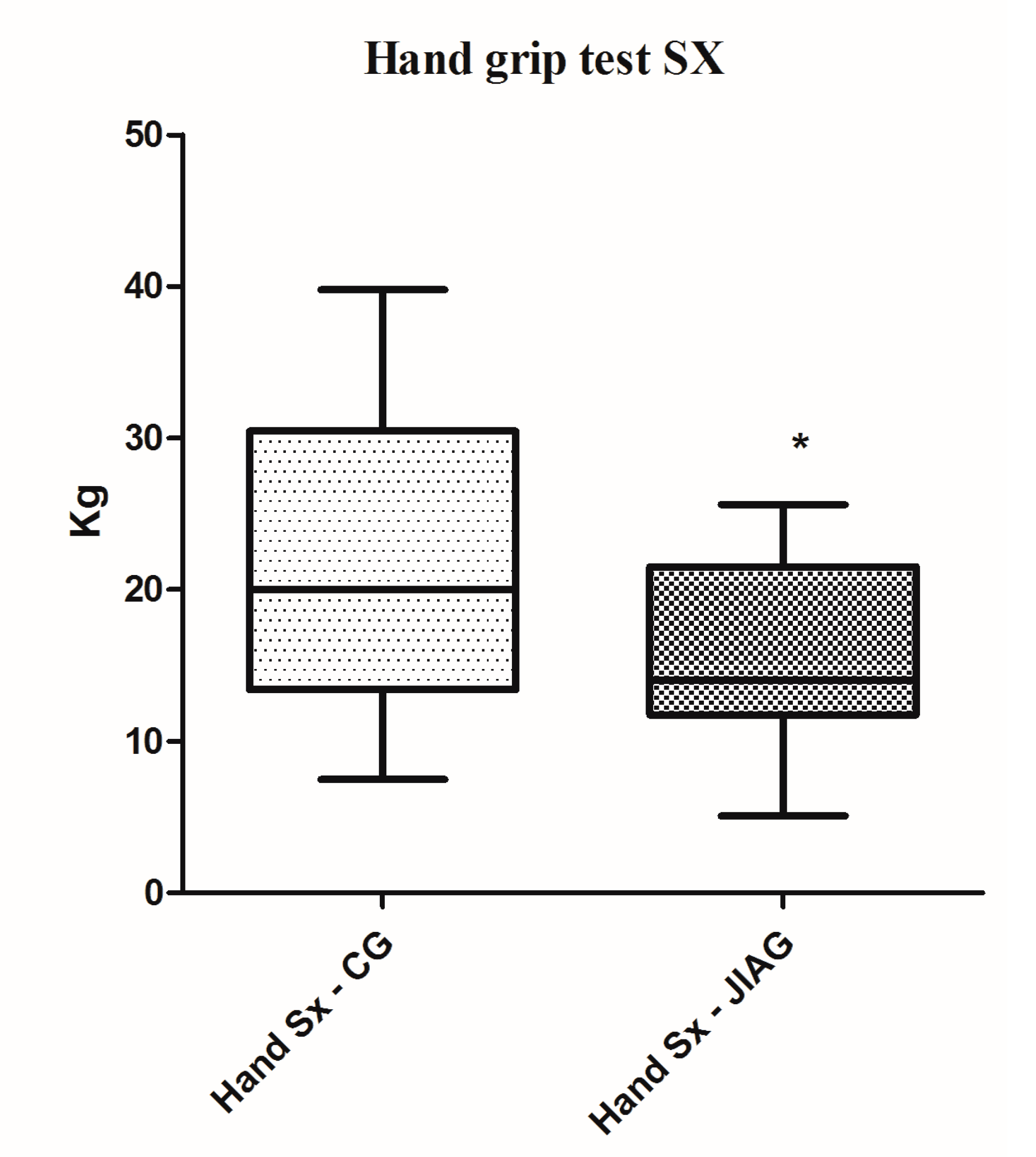
- The sit-up test and hand grip test [37,38]: in the first test, the subjects were instructed to bend the knees at an angle of 100°, with both arms on his hips while the ankles were held down. The subject performed the concentric movement of lifting the trunk, followed by the eccentric movement of lowering the trunk. The maximum number of executions was taken into account. The second test was an isometric grip strength for both hands, and was determined using an electronic dynamometer (KERN-MAP). The subject was standing with the shoulder adducted and neutrally rotated. The forearm was along the hips and in a neutral position. The children were told to make their best squeezing effort onto the dynamometer, one repetition with each hand, three times. The best performance for each hand was taken into account;
- Backsaver sit and reach [39,40,41,42]: the subjects sit on the floor with both legs out straight. The feet were placed flush against the measurement box. The arms were placed parallel to the floor, with the hands facing down, and the subject reached forward along the measuring line as far as possible; and
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Helmick, C.G.; Felson, D.T.; Lawrence, R.C.; Gabriel, S.; Hirsch, R.; Kwoh, C.K.; Liang, M.H.; Kremers, H.M.; Mayes, M.D.; Merkel, P.A.; et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States. Part I. Arthritis Rheum. 2008, 58, 15–25. [Google Scholar] [CrossRef] [PubMed]
- Schaller, J.G. The history of pediatric rheumatology. Pediatr. Res. 2005, 58, 997–1007. [Google Scholar] [CrossRef] [PubMed]
- Angelis, A.; Kanavos, P.; Lopez-Bastida, J.; Linertova, R.; Serrano-Aguilar, P.; Network, B.-R.R. Socioeconomic costs and health-related quality of life in juvenile idiopathic arthritis: A cost-of-illness study in the United Kingdom. BMC Musculoskelet. Disord. 2016, 17, 321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cassidy, J.T.; Petty, R.E. Chronic arthritis in childhood. In Textbook of Pediatric Rheumatology, 5th ed.; Elsevier Saunders: Philadelphia, PA, USA, 2005; pp. 206–260. [Google Scholar]
- Allaire, S.H.; Anderson, J.J.; Meenan, R.F. Reducing work disability associated with rheumatoid arthritis: Identification of additional risk factors and persons likely to benefit from intervention. Arthritis Care Res. 1996, 9, 349–357. [Google Scholar] [CrossRef]
- Breda, L.; Di Marzio, D.; Giannini, C.; Gaspari, S.; Nozzi, M.; Scarinci, A.; Chiarelli, F.; Mohn, A. Relationship between inflammatory markers, oxidant-antioxidant status and intima-media thickness in prepubertal children with juvenile idiopathic arthritis. Clin. Res. Cardiol. 2013, 102, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Vlahos, A.P.; Theocharis, P.; Bechlioulis, A.; Naka, K.K.; Vakalis, K.; Papamichael, N.D.; Alfantaki, S.; Gartzonika, K.; Mavridis, A.; Michalis, L.K.; et al. Changes in vascular function and structure in juvenile idiopathic arthritis. Arthritis Care Res. 2011, 63, 1736–1744. [Google Scholar] [CrossRef] [PubMed]
- Andersen, L.B.; Harro, M.; Sardinha, L.B.; Froberg, K.; Ekelund, U.; Brage, S.; Anderssen, S.A. Physical activity and clustered cardiovascular risk in children: A cross-sectional study (The European Youth Heart Study). Lancet 2006, 368, 299–304. [Google Scholar] [CrossRef]
- Bohr, A.H.; Nielsen, S.; Muller, K.; Karup Pedersen, F.; Andersen, L.B. Reduced physical activity in children and adolescents with Juvenile Idiopathic Arthritis despite satisfactory control of inflammation. Pediatr. Rheumatol. Online J. 2015, 13, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aasland, A.; Flato, B.; Vandvik, I.H. Psychosocial outcome in juvenile chronic arthritis: A nine-year follow-up. Clin. Exp. Rheumatol. 1997, 15, 561–568. [Google Scholar] [PubMed]
- Ding, T.; Hall, A.; Jacobs, K.; David, J. Psychological functioning of children and adolescents with juvenile idiopathic arthritis is related to physical disability but not to disease status. Rheumatology 2008, 47, 660–664. [Google Scholar] [CrossRef] [PubMed]
- Bromberg, M.H.; Connelly, M.; Anthony, K.K.; Gil, K.M.; Schanberg, L.E. Self-reported pain and disease symptoms persist in juvenile idiopathic arthritis despite treatment advances: An electronic diary study. Arthritis Rheumatol. 2014, 66, 462–469. [Google Scholar] [CrossRef] [PubMed]
- Stanley, L.C.; Ward-Smith, P. The diagnosis and management of juvenile idiopathic arthritis. J. Pediatr. Health Care 2011, 25, 191–194. [Google Scholar] [CrossRef] [PubMed]
- Philips, C.A. Rehabilitation of the patient with rheumatoid hand involvement. Phys. Ther. 1989, 69, 1091–1098. [Google Scholar] [CrossRef] [PubMed]
- Colditz, J.C. Plaster of Paris: The forgotten hand splinting material. J. Hand Ther. 2002, 15, 144–157. [Google Scholar] [CrossRef] [PubMed]
- Li-Tsang, C.W.; Hung, L.K.; Mak, A.F. The effect of corrective splinting on flexion contracture of rheumatoid fingers. J. Hand Ther. 2002, 15, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Philpott, J.F.; Houghton, K.; Luke, A. Physical activity recommendations for children with specific chronic health conditions: Juvenile idiopathic arthritis, hemophilia, asthma, and cystic fibrosis. Clin. J. Sport Med. 2010, 20, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Takken, T.; van der Net, J.; Kuis, W.; Helders, P.J. Physical activity and health related physical fitness in children with juvenile idiopathic arthritis. Ann. Rheum. Dis. 2003, 62, 885–889. [Google Scholar] [CrossRef] [PubMed]
- Cavallo, S.; Brosseau, L.; Toupin-April, K.; Wells, G.A.; Smith, C.A.; Pugh, A.G.; Stinson, J.; Thomas, R.; Ahmed, S.; Duffy, C.M.; et al. Ottawa Panel Evidence-Based Clinical Practice Guidelines for Structured Physical Activity in the Management of Juvenile Idiopathic Arthritis. Arch. Phys. Med. Rehabil. 2017, 98, 1018–1041. [Google Scholar] [CrossRef] [PubMed]
- Lelieveld, O.T.; Armbrust, W.; Geertzen, J.H.; de Graaf, I.; van Leeuwen, M.A.; Sauer, P.J.; van Weert, E.; Bouma, J. Promoting physical activity in children with juvenile idiopathic arthritis through an internet-based program: Results of a pilot randomized controlled trial. Arthritis Care Res. 2010, 62, 697–703. [Google Scholar] [CrossRef] [PubMed]
- Ekdahl, C.; Andersson, S.I. Standing balance in rheumatoid arthritis. A comparative study with healthy subjects. Scand. J. Rheumatol. 1989, 18, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Winter, D.A. Human balance and posture control during standing and walking. Gait Posture 1995, 3, 193–214. [Google Scholar] [CrossRef]
- Noren, A.M.; Bogren, U.; Bolin, J.; Stenstrom, C. Balance assessment in patients with peripheral arthritis: Applicability and reliability of some clinical assessments. Physiother. Res. Int. 2001, 6, 193–204. [Google Scholar] [CrossRef] [PubMed]
- Hilberg, T.; Herbsleb, M.; Gabriel, H.H.; Jeschke, D.; Schramm, W. Proprioception and isometric muscular strength in haemophilic subjects. Haemophilia 2001, 7, 582–588. [Google Scholar] [CrossRef] [PubMed]
- Houghton, K.M.; Guzman, J. Evaluation of static and dynamic postural balance in children with juvenile idiopathic arthritis. Pediatr. Phys. Ther. 2013, 25, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Warner, J.T. Body composition, exercise and energy expenditure in survivors of acute lymphoblastic leukaemia. Pediatr. Blood Cancer 2008, 50, 456–461. [Google Scholar] [CrossRef] [PubMed]
- Bianco, A.; Patti, A.; Thomas, E.; Palma, R.; Maggio, M.C.; Paoli, A.; Palma, A. Evaluation of fitness levels of children with a diagnosis of acute leukemia and lymphoma after completion of chemotherapy and autologous hematopoietic stem cell transplantation. Cancer Med. 2014, 3, 385–389. [Google Scholar] [CrossRef] [PubMed]
- Bianco, A.; Mammina, C.; Jemni, M.; Filippi, A.R.; Patti, A.; Thomas, E.; Paoli, A.; Palma, A.; Tabacchi, G. A fitness index model for Italian adolescents living in Southern Italy. The ASSO project. J. Sports Med. Phys. Fit. 2016, 56, 1279–1288. [Google Scholar]
- Ruiz, J.R.; Espana Romero, V.; Castro Pinero, J.; Artero, E.G.; Ortega, F.B.; Cuenca Garcia, M.; Jimenez Pavon, D.; Chillon, P.; Girela Rejon, M.J.; Mora, J.; et al. ALPHA-fitness test battery: Health-related field-based fitness tests assessment in children and adolescents. Nutr. Hosp. 2011, 26, 1210–1214. [Google Scholar] [PubMed]
- Yurdalan, S.U.; Kondu, S.; Malkoc, M. Assessment of health-related fitness in the patients with end-stage renal disease on hemodialysis: Using Eurofit Test Battery. Ren. Fail. 2007, 29, 955–960. [Google Scholar] [CrossRef] [PubMed]
- Bianco, A.; Jemni, M.; Thomas, E.; Patti, A.; Paoli, A.; Ramos Roque, J.; Palma, A.; Mammina, C.; Tabacchi, G. A systematic review to determine reliability and usefulness of the field-based test batteries for the assessment of physical fitness in adolescents—The ASSO Project. Int. J. Occup. Med. Environ. Health 2015, 28, 445–478. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, Y.; Carey, J.P.; Hoffman, H.J.; Sklare, D.A.; Schubert, M.C. The modified Romberg Balance Test: Normative data in U.S. adults. Otol. Neurotol. 2011, 32, 1309–1311. [Google Scholar] [CrossRef] [PubMed]
- Scoppa, F.; Capra, R.; Gallamini, M.; Shiffer, R. Clinical stabilometry standardization: Basic definitions-acquisition interval-sampling frequency. Gait Posture 2013, 37, 290–292. [Google Scholar] [CrossRef] [PubMed]
- Gagey, P.M.; Weber, B. Study of intra-subject random variations of stabilometric parameters. Med. Biol. Eng. Comput. 2010, 48, 833–835. [Google Scholar] [CrossRef] [PubMed]
- Kapteyn, T.S.; Bles, W.; Njiokiktjien, C.J.; Kodde, L.; Massen, C.H.; Mol, J.M. Standardization in platform stabilometry being a part of posturography. Agressologie 1983, 24, 321–326. [Google Scholar] [PubMed]
- Fernandez-Santos, J.R.; Ruiz, J.R.; Cohen, D.D.; Gonzalez-Montesinos, J.L.; Castro-Pinero, J. Reliability and Validity of Tests to Assess Lower-Body Muscular Power in Children. J. Strength Cond. Res. 2015, 29, 2277–2285. [Google Scholar] [CrossRef] [PubMed]
- Ortega, F.B.; Artero, E.G.; Ruiz, J.R.; Vicente-Rodriguez, G.; Bergman, P.; Hagstromer, M.; Ottevaere, C.; Nagy, E.; Konsta, O.; Rey-Lopez, J.P.; et al. Reliability of health-related physical fitness tests in European adolescents. The HELENA Study. Int. J. Obes. 2008, 32, S49–S57. [Google Scholar] [CrossRef] [PubMed]
- Esmaeilzadeh, S.; Ebadollahzadeh, K. Physical fitness, physical activity and sedentary activities of 7 to 11 year old boys with different body mass indexes. Asian J. Sports Med. 2012, 3, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Castro-Pinero, J.; Chillon, P.; Ortega, F.B.; Montesinos, J.L.; Sjostrom, M.; Ruiz, J.R. Criterion-related validity of sit-and-reach and modified sit-and-reach test for estimating hamstring flexibility in children and adolescents aged 6–17 years. Int. J. Sports Med. 2009, 30, 658–662. [Google Scholar] [CrossRef] [PubMed]
- Cornbleet, S.L.; Woolsey, N.B. Assessment of hamstring muscle length in school-aged children using the sit-and-reach test and the inclinometer measure of hip joint angle. Phys. Ther. 1996, 76, 850–855. [Google Scholar] [CrossRef] [PubMed]
- Chillon, P.; Castro-Pinero, J.; Ruiz, J.R.; Soto, V.M.; Carbonell-Baeza, A.; Dafos, J.; Vicente-Rodriguez, G.; Castillo, M.J.; Ortega, F.B. Hip flexibility is the main determinant of the back-saver sit-and-reach test in adolescents. J. Sports Sci. 2010, 28, 641–648. [Google Scholar] [CrossRef] [PubMed]
- Ayala, F.; Sainz de Baranda, P.; De Ste Croix, M.; Santonja, F. Reproducibility and criterion-related validity of the sit and reach test and toe touch test for estimating hamstring flexibility in recreationally active young adults. Phys. Ther. Sport 2012, 13, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Kippers, V.; Parker, A.W. Toe-touch test. A measure of its validity. Phys. Ther. 1987, 67, 1680–1684. [Google Scholar] [CrossRef] [PubMed]
- Bos, G.J.; Lelieveld, O.T.; Armbrust, W.; Sauer, P.J.; Geertzen, J.H.; Dijkstra, P.U. Physical activity in children with Juvenile Idiopathic Arthritis compared to controls. Pediatr. Rheumatol. Online J. 2016, 14, 42. [Google Scholar] [CrossRef] [PubMed]
- Gueddari, S.; Amine, B.; Rostom, S.; Badri, D.; Mawani, N.; Ezzahri, M.; Moussa, F.; Shyen, S.; Abouqal, R.; Chkirat, B.; et al. Physical activity, functional ability, and disease activity in children and adolescents with juvenile idiopathic arthritis. Clin. Rheumatol. 2014, 33, 1289–1294. [Google Scholar] [CrossRef] [PubMed]
- Stapley, P.J.; Pozzo, T.; Cheron, G.; Grishin, A. Does the coordination between posture and movement during human whole-body reaching ensure center of mass stabilization? Exp. Brain Res. 1999, 129, 134–146. [Google Scholar] [CrossRef] [PubMed]
- Klepper, S.E. Exercise and fitness in children with arthritis: Evidence of benefits for exercise and physical activity. Arthritis Rheum. 2003, 49, 435–443. [Google Scholar] [CrossRef] [PubMed]
- Aydog, E.; Bal, A.; Aydog, S.T.; Cakci, A. Evaluation of dynamic postural balance using the Biodex Stability System in rheumatoid arthritis patients. Clin. Rheumatol. 2006, 25, 462–467. [Google Scholar] [CrossRef] [PubMed]
- Faigenbaum, A.D.; MacDonald, J.P. Dynapenia: It’s not just for grown-ups anymore. Acta Paediatr. 2017, 106, 696–697. [Google Scholar] [CrossRef] [PubMed]
- Maggio, A.B.; Hofer, M.F.; Martin, X.E.; Marchand, L.M.; Beghetti, M.; Farpour-Lambert, N.J. Reduced physical activity level and cardiorespiratory fitness in children with chronic diseases. Eur. J. Pediatr. 2010, 169, 1187–1193. [Google Scholar] [CrossRef] [PubMed]
- Burnham, J.M.; Shults, J.; Dubner, S.E.; Sembhi, H.; Zemel, B.S.; Leonard, M.B. Bone density, structure, and strength in juvenile idiopathic arthritis: Importance of disease severity and muscle deficits. Arthritis Rheum. 2008, 58, 2518–2527. [Google Scholar] [CrossRef] [PubMed]
- Haberfehlner, H.; Visser, B.; Daffertshofer, A.; van Rossum, M.A.; Roorda, L.D.; van der Leeden, M.; Dekker, J.; Hoeksma, A.F. Handwriting difficulties in juvenile idiopathic arthritis: A pilot study. Clin. Exp. Rheumatol. 2011, 29, 887–893. [Google Scholar] [PubMed]
- Lindehammar, H. Hand strength in juvenile chronic arthritis: A two-year follow-up. Acta Paediatr. 2003, 92, 1291–1296. [Google Scholar] [CrossRef] [PubMed]
- Houghton, K. Physical activity, physical fitness, and exercise therapy in children with juvenile idiopathic arthritis. Phys. Sportsmed. 2012, 40, 77–82. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | CG n = 39 (Mean ± SD) | JIAG n = 17 (Mean ± SD) | p |
|---|---|---|---|
| Age (years) | 12.87 ± 3.04 | 12.23 ± 4.46 | ns |
| Weight (kg) | 45.18 ± 18.32 | 42.82 ± 11.75 | ns |
| Height (cm) | 151.46 ± 18.94 | 145.88 ± 15.83 | ns |
| Variables | Correlations JIAG Group; n = 17 | |||||
|---|---|---|---|---|---|---|
| Y Mean | Abalakov Test | Backsaver Sit and Reach | Toe Touch Test | Hand Grip DX | Hand Grip SX | |
| ES, mm2 | −0.74 | −0.54 | −0.54 | −0.67 | −0.59 | |
| SP, mm | −0.7 | |||||
| X mean | 0.49 | |||||
| Y mean | ||||||
| Abalakov test | 0.6 | 0.6 | 0.76 | 0.76 | ||
| Backsaver Sit and Reach | 0.94 | |||||
| The Toe Touch Test | ||||||
| Hand grip DX | 0.96 | |||||
| Variables | Correlations CG; n = 39 | ||||
|---|---|---|---|---|---|
| Abalakov Test | Backsaver Sit and Reach | Toe Touch Test | Hand Grip DX | Hand Grip SX | |
| ES, mm2 | −0.75 | −0.64 | −0.73 | ||
| SP, mm | |||||
| X mean | −0.64 | −0.57 | |||
| Y mean | |||||
| Abalakov test | 0.64 | 0.72 | |||
| Sit up test | −0.40 | ||||
| Backsaver Sit and Reach | 0.88 | ||||
| The Toe Touch Test | |||||
| Hand grip DX | 0.91 | ||||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patti, A.; Maggio, M.C.; Corsello, G.; Messina, G.; Iovane, A.; Palma, A. Evaluation of Fitness and the Balance Levels of Children with a Diagnosis of Juvenile Idiopathic Arthritis: A Pilot Study. Int. J. Environ. Res. Public Health 2017, 14, 806. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph14070806
Patti A, Maggio MC, Corsello G, Messina G, Iovane A, Palma A. Evaluation of Fitness and the Balance Levels of Children with a Diagnosis of Juvenile Idiopathic Arthritis: A Pilot Study. International Journal of Environmental Research and Public Health. 2017; 14(7):806. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph14070806
Chicago/Turabian StylePatti, Antonino, Maria Cristina Maggio, Giovanni Corsello, Giuseppe Messina, Angelo Iovane, and Antonio Palma. 2017. "Evaluation of Fitness and the Balance Levels of Children with a Diagnosis of Juvenile Idiopathic Arthritis: A Pilot Study" International Journal of Environmental Research and Public Health 14, no. 7: 806. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph14070806