Syncope and Collapse Are Associated with an Increased Risk of Cardiovascular Disease and Mortality in Patients Undergoing Dialysis

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Study Design and Participants
2.3. Outcomes and Relevant Variables
2.4. Statistical Analysis
3. Results
3.1. Incidence and Prevalence of Syncope in the Dialysis Population
3.2. Patient Characteristics
3.3. Risk Factors for Primary Outcomes
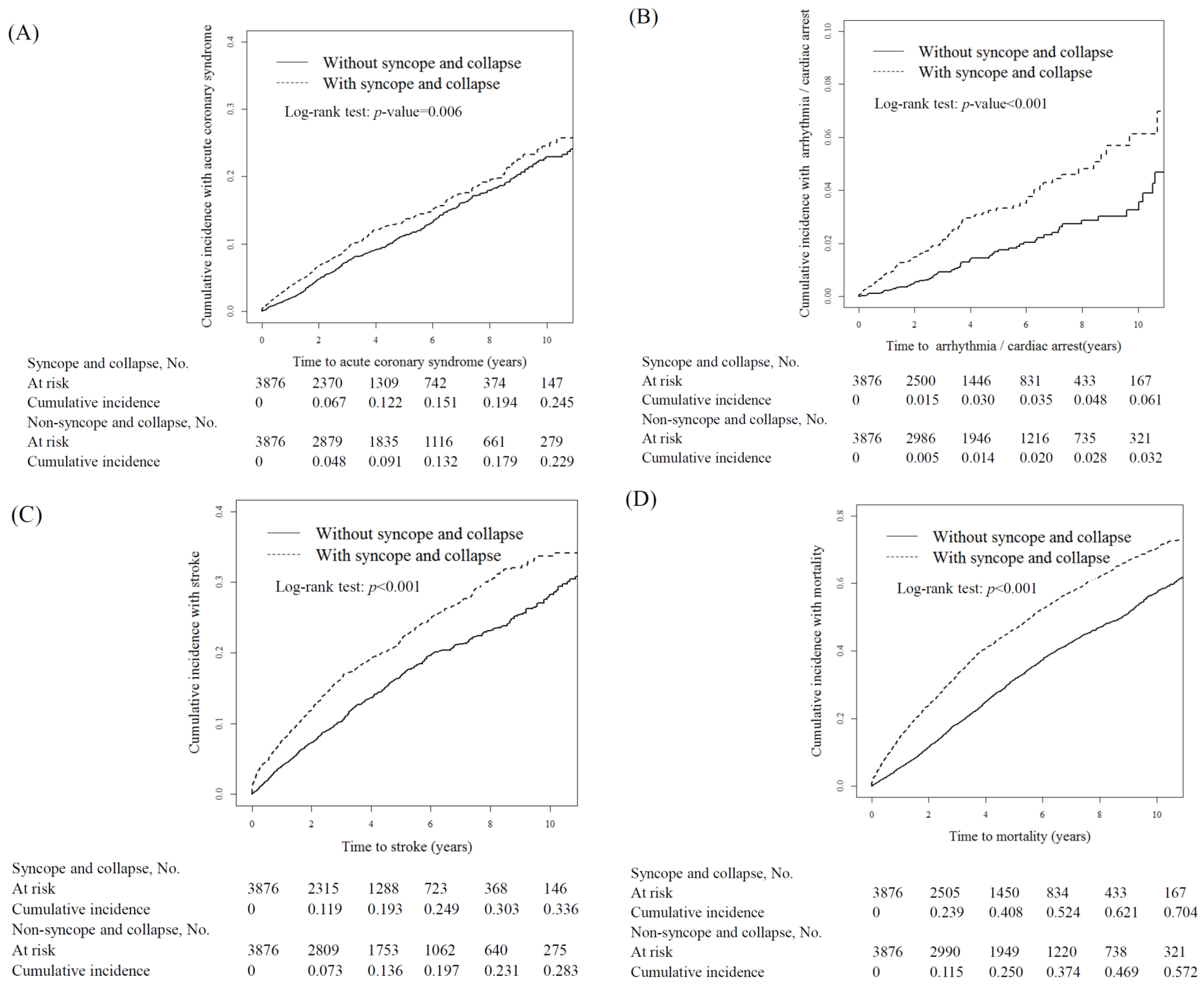
3.4. Primary Outcomes and Risk Stratification
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
Abbreviations
References
- United States Renal Data System. USRDS 2013 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States; National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2013. [Google Scholar]
- US Renal Data System: USRDS 2011 Annual Data Report; National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2011.
- Go, A.S.; Chertow, G.M.; Fan, D.; McCulloch, C.E.; Hsu, C.Y. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N. Engl. J. Med. 2004, 351, 1296–1305. [Google Scholar] [CrossRef] [PubMed]
- Chronic Kidney Disease Prognosis Consortium. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: A collaborative meta-analysis. Lancet 2010, 375, 2073–2081. [Google Scholar] [CrossRef]
- Foley, R.N.; Murray, A.M.; Li, S.; Herzog, C.A.; McBean, A.M.; Eggers, P.W.; Collins, A.J. Chronic kidney disease and the risk for cardiovascular disease, renal replacement, and death in the United States Medicare population, 1998 to 1999. J. Am. Soc. Nephrol. 2005, 16, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Saran, R.; Li, Y.; Robinson, B.; Abbott, K.C.; Agodoa, L.Y.; Ayanian, J. US Renal Data System 2015 Annual Data Report: Epidemiology of Kidney Disease in the United States. Am. J. Kidney Dis. 2016, 67, S1–S305. [Google Scholar] [CrossRef] [PubMed]
- KDIGO. Chapter 1: Definition and Classification of CKD. Kidney Int. Suppl. 2013, 3, 19. Available online: http://www.kdigo.org/clinical_practice_guidelines/pdf/CKD/KDIGO_2012_CKD_GL.pdf (accessed on 20 August 2018).
- Palmer, S.C.; Craig, J.C.; Navaneethan, S.D.; Tonelli, M.; Pellegrini, F.; Strippoli, G.F. Benefits and harms of statin therapy for persons with chronic kidney disease: A systematic review and meta-analysis. Ann. Intern. Med. 2012, 157, 263–275. [Google Scholar] [CrossRef] [PubMed]
- Palmer, S.C.; Di Micco, L.; Razavian, M.; Craig, J.C.; Perkovic, V.; Pellegrini, F.; Jardine, M.J.; Webster, A.C.; Zoungas, S.; Strippoli, G.F. Antiplatelet agents for chronic kidney disease. Cochrane Database Syst. Rev. 2013, CD008834. [Google Scholar] [CrossRef]
- Jadoul, M.; Thumma, J.; Fuller, D.S.; Tentori, F.; Li, Y.; Morgenstern, H. Modifiable practices associated with sudden death among hemodialysis patients in the Dialysis Outcomes and Practice Patterns Study. Clin. J. Am. Soc. Nephrol. 2012, 7, 765–774. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, A.; Takase, H.; Toriyama, T.; Sugiura, T.; Kurita, Y.; Ueda, R.; Dohi, Y. Candesartan, an angiotensin II type-1 receptor blocker, reduces cardiovascular events in patients on chronic haemodialysis—A randomized study. Nephrol. Dial. Transplant. 2006, 21, 2507–2512. [Google Scholar] [CrossRef] [PubMed]
- Shen, W.K.; Sheldon, R.S.; Benditt, D.G.; Cohen, M.I.; Forman, D.E.; Goldberger, Z.D. 2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients with Syncope: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J. Am. Coll. Cardiol. 2017, 70, 620–663. [Google Scholar] [CrossRef] [PubMed]
- Ruwald, M.H.; Hansen, M.L.; Lamberts, M.; Hansen, C.M.; Højgaard, M.V.; Køber, L. The relation between age, sex, comorbidity, and pharmacotherapy and the risk of syncope: A Danish nationwide study. Europace 2012, 14, 1506–1514. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, Y.; Bellamy, M.F.; Baker, C.S.R. Aortic Stenosis in Dialysis Patients. Semin. Dial. 2017, 30, 224–231. [Google Scholar] [CrossRef] [PubMed]
- Freeman, K.; Feldman, J.A.; Mitchell, P.; Donovan, J.; Dyer, K.S.; Eliseo, L. Effects of presentation and electrocardiogram on time to treatment of hyperkalemia. Acad. Emerg. Med. 2008, 15, 239–249. [Google Scholar] [CrossRef] [PubMed]
- Hentges, M.J.; Gunderson, B.W.; Lewis, M.J. Retrospective analysis of cisapride-induced QT changes in end-stage renal disease patients. Nephrol. Dial. Transplant. 2000, 15, 1814–1818. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, M.; Tokoro, T.; Yamazaki, S.; Hashimoto, T.; Kobayashi, H.; Ono, T. Idiopathic pre-capillary pulmonary hypertension in patients with end-stage kidney disease: Effect of endothelin receptor antagonists. Clin. Exp. Nephrol. 2017, 21, 1088–1096. [Google Scholar] [CrossRef] [PubMed]
- Roberts, R.G.; Kenny, R.A.; Brierley, E.J. Are elderly haemodialysis patients at risk of falls and postural hypotension? Int. Urol. Nephrol. 2003, 35, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Roberts, R.; Jeffrey, C.; Carlisle, G.; Brierley, E. Prospective investigation of the incidence of falls, dizziness and syncope in haemodialysis patients. Int. Urol. Nephrol. 2007, 39, 275–279. [Google Scholar] [CrossRef] [PubMed]
- Database NHIR. Taiwan. Available online: http://nhird.nhri.org.tw/en/index.html (accessed on 20 August 2018).
- Peng, Y.C.; Lin, C.L.; Hsu, W.Y.; Chang, C.S.; Yeh, H.Z.; Tung, C.F.; Wu, Y.L.; Sung, F.C.; Kao, C.H. Statins are associated with a reduced risk of cholangiocarcinoma: A population-based case-control study. Br. J. Clin. Pharmacol. 2015, 80, 755–761. [Google Scholar] [CrossRef] [PubMed]
- Huang, K.W.; Kuan, Y.C.; Luo, J.C.; Lin, C.L.; Liang, J.A.; Kao, C.H. Impact of long-term gastric acid suppression on spontaneous bacterial peritonitis in patients with advanced decompensated liver cirrhosis. Eur. J. Intern. Med. 2016, 32, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Charytan, D.; Kuntz, R.E.; Mauri, L.; DeFilippi, C. Distribution of coronary artery disease and relation to mortality in asymptomatic hemodialysis patients. Am. J. Kidney Dis. 2007, 49, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Ohtake, T.; Kobayashi, S.; Moriya, H.; Negishi, K.; Okamoto, K.; Maesato, K.; Saito, S. High prevalence of occult coronary artery stenosis in patients with chronic kidney disease at the initiation of renal replacement therapy: An angiographic examination. J. Am. Soc. Nephrol. 2005, 16, 1141–1148. [Google Scholar] [CrossRef] [PubMed]
- Multiple Risk Factor Intervention Trial Research Group. Exercise electrocardiogram and coronary heart disease mortality in the Multiple Risk Factor Intervention Trial. Am. J. Cardiol. 1985, 55, 16–24. [Google Scholar] [CrossRef]
- Herzog, C.A. How to manage the renal patient with coronary heart disease: The agony and the ecstasy of opinion-based medicine. J. Am. Soc. Nephrol. 2003, 14, 2556–2572. [Google Scholar] [CrossRef] [PubMed]
- K/DOQI Workgroup. K/DOQI clinical practice guidelines for cardiovascular disease in dialysis patients. Am. J. Kidney Dis. 2005, 45, S1–S153. [Google Scholar]
- De Vriese, A.S.; Vandecasteele, S.J.; Van den Bergh, B.; De Geeter, F.W. Should we screen for coronary artery disease in asymptomatic chronic dialysis patients? Kidney Int. 2012, 81, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.H.; Hung, S.Y.; Sung, J.M.; Hung, K.Y.; Wang, J.D. Risk of stroke in long-term dialysis patients compared with the general population. Am. J. Kidney Dis. 2014, 63, 604–611. [Google Scholar] [CrossRef] [PubMed]
- Molnar, A.O.; Sood, M.M. Predicting in a predicament: Stroke and hemorrhage risk prediction in dialysis patients with atrial fibrillation. Semin. Dial. 2017. [Google Scholar] [CrossRef] [PubMed]
- Harel, Z.; Chertow, G.M.; Shah, P.S.; Harel, S.; Dorian, P.; Yan, A.T. Warfarin and the Risk of Stroke and Bleeding in Patients with Atrial Fibrillation Receiving Dialysis: A Systematic Review and Meta-analysis. Can. J. Cardiol. 2017, 33, 737–746. [Google Scholar] [CrossRef] [PubMed]
- Herzog, C.A.; Strief, J.W.; Collins, A.J.; Gilbertson, D.T. Cause-specific mortality of dialysis patients after coronary revascularization: Why don’t dialysis patients have better survival after coronary intervention? Nephrol. Dial. Transplant. 2008, 23, 2629–2633. [Google Scholar] [CrossRef] [PubMed]
- Herzog, C.A.; Li, S.; Weinhandl, E.D.; Strief, J.W.; Collins, A.J.; Gilbertson, D.T. Survival of dialysis patients after cardiac arrest and the impact of implantable cardioverter defibrillators. Kidney Int. 2005, 68, 818–825. [Google Scholar] [CrossRef] [Green Version]
- Soteriades, E.S.; Evans, J.C.; Larson, M.G.; Chen, M.H.; Chen, L.; Benjamin, E.J.; Levy, D. Incidence and prognosis of syncope. N. Engl. J. Med. 2002, 347, 878–885. [Google Scholar] [CrossRef] [PubMed]
- Kapoor, W.N.; Hanusa, B.H. Is syncope a risk factor for poor outcomes? Comparison of patients with and without syncope. Am. J. Med. 1996, 100, 646–655. [Google Scholar] [CrossRef]
- Li, M.; Tomlinson, G.; Naglie, G.; Cook, W.L.; Jassal, S.V. Geriatric comorbidities, such as falls, confer an independent mortality risk to elderly dialysis patients. Nephrol. Dial. Transplant. 2008, 23, 1396–1400. [Google Scholar] [CrossRef] [PubMed]
- Desmet, C.; Beguin, C.; Swine, C.; Jadoul, M.; Université Catholique de Louvain Collaborative Group. Falls in hemodialysis patients: Prospective study of incidence, risk factors, and complications. Am. J. Kidney Dis. 2005, 45, 148–153. [Google Scholar] [CrossRef] [PubMed]
- Liem, Y.S.; Wong, J.B.; Hunink, M.G.; de Charro, F.T.; Winkelmayer, W.C. Comparison of hemodialysis and peritoneal dialysis survival in The Netherlands. Kidney Int. 2007, 71, 153–158. [Google Scholar] [CrossRef] [PubMed]
- McDonald, S.P.; Marshall, M.R.; Johnson, D.W.; Polkinghorne, K.R. Relationship between dialysis modality and mortality. J. Am. Soc. Nephrol. 2009, 20, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Polinder-Bos, H.A.; Emmelot-Vonk, M.H.; Gansevoort, R.T.; Diepenbroek, A.; Gaillard, C.A. High fall incidence and fracture rate in elderly dialysis patients. Neth. J. Med. 2014, 72, 509–515. [Google Scholar] [PubMed]


{kind=link}
| Syncope and Collapse | |||
|---|---|---|---|
| Characteristics | No (n = 3876) | Yes (n = 3876) | p-Value |
| n (%) | n (%) | ||
| Age, years | 0.89 | ||
| ≤49 | 585 (15.1) | 599 (15.5) | |
| 50–64 | 1300 (33.5) | 1301 (33.6) | |
| ≥65 | 1991 (51.4) | 1976 (51.0) | |
| Mean (SD) # | 63.6 (13.2) | 63.7 (13.3) | 0.91 |
| Dialysis modality | 0.003 | ||
| Peritoneal dialysis | 310 (8.00) | 384 (9.91) | |
| Hemodialysis | 3566 (92.0) | 3492 (90.1) | |
| Gender | 0.86 | ||
| Female | 2039 (52.6) | 2031 (52.4) | |
| Male | 1837 (47.4) | 1845 (47.6) | |
| Comorbidity | |||
| Deep vein thrombosis | 228 (5.88) | 228 (5.88) | 0.99 |
| Pulmonary embolism | 5 (0.13) | 5 (0.13) | 0.99 |
| Valvular heart disease | 534 (13.8) | 542 (14.0) | 0.79 |
| Atrial fibrillation | 260 (6.71) | 260 (6.71) | 0.99 |
| Diabetes | 1581 (40.8) | 1547 (39.9) | 0.43 |
| Hypertension | 3432 (88.5) | 3417 (88.2) | 0.60 |
| Hyperlipidemia | 1559 (40.2) | 1553 (40.1) | 0.89 |
| Variable | ACS | Arrhythmia/Cardiac Arrest | Stroke | Mortality | ||||
|---|---|---|---|---|---|---|---|---|
| Crude HR (95% CI) | Adjusted HR † (95% CI) | Crude HR (95% CI) | Adjusted HR † (95% CI) | Crude HR (95% CI) | Adjusted HR † (95% CI) | Crude HR (95% CI) | Adjusted HR † (95% CI) | |
| Syncope and collapse | 1.21 (1.06, 1.39) ** | 1.28 (1.11, 1.46) *** | 1.93 (1.41, 2.65) *** | 2.05 (1.50, 2.82) *** | 1.40 (1.26, 1.56) *** | 1.48 (1.33, 1.66) *** | 1.65 (1.54, 1.77) *** | 1.79 (1.67, 1.92) *** |
| Gender (Men vs. women) | 1.21 (1.05, 1.38) ** | 1.24 (1.08, 1.42) ** | 1.24 (0.91, 1.68) | - | 1.23 (1.11, 1.38) *** | 1.20 (1.08, 1.34) *** | 1.18 (1.11, 1.27) *** | 1.19 (1.11, 1.27) *** |
| Age, years | 1.03 (1.02, 1.03) *** | 1.02 (1.02, 1.03) *** | 1.03 (1.01, 1.04) *** | 1.03 (1.01, 1.04) *** | 1.03 (1.03, 1.04) *** | 1.03 (1.03, 1.04) *** | 1.05 (1.04, 1.05) *** | 1.05 (1.04, 1.05) *** |
| Dialysis modality | ||||||||
| Peritoneal dialysis | 1 (Reference) | 1 (Reference) | 1 (Reference) | 1 (Reference) | 1 (Reference) | 1 (Reference) | 1 (Reference) | 1 (Reference) |
| Hemodialysis | 1.32 (1.01–1.73) * | 1.09 (0.83, 1.44) | 1.43 (0.75, 2.71) | - | 1.46 (1.16, 1.83) ** | 1.14 (0.91, 1.44) | 1.23 (1.08, 1.41) ** | 0.86 (0.75, 0.98) * |
| Baseline comorbidities (yes vs. no) | ||||||||
| Deep vein thrombosis | 1.25 (0.96, 1.63) | - | 0.97 (0.49, 1.89) | - | 0.78 (0.60, 1.01) | - | 1.10 (0.95, 1.26) | - |
| Pulmonary embolism | 2.46 (0.61, 9.86) | - | - | - | 1.43 (0.36, 5.71) | - | 1.02 (0.38, 2.71) | - |
| Valvular heart disease | 1.39 (1.16, 1.68) *** | 1.30 (1.08, 1.58) ** | 1.37 (0.90, 2.09) | - | 1.17 (1.00, 1.37) * | - | 1.33 (1.21, 1.46) *** | 1.15 (1.05, 1.27) ** |
| Atrial fibrillation | 1.54 (1.18, 2.01) ** | 1.25 (0.95, 1.64) | 2.59 (1.58, 4.24) *** | 2.23 (1.35, 3.67) ** | 1.51 (1.23, 1.87) *** | 1.26 (1.02, 1.56) * | 2.13 (1.89, 2.40) *** | 1.65 (1.46, 1.86) *** |
| Diabetes | 1.88 (1.64, 2.16) *** | 1.62 (1.40, 1.87) *** | 1.84 (1.35, 2.51) *** | 1.76 (1.28, 2.41) *** | 1.90 (1.71, 2.13) *** | 1.77 (1.58, 1.99) *** | 1.52 (1.42, 1.63) *** | 1.51 (1.41, 1.62) *** |
| Hypertension | 1.99 (1.55, 2.57) *** | 1.44 (1.11, 1.87) ** | 2.06 (1.14, 3.71) * | 1.57 (0.86, 2.87) | 1.98 (1.61, 2.44) *** | 1.55 (1.25, 1.91) *** | 1.28 (1.15, 1.43) *** | 0.98 (0.88, 1.09) |
| Hyperlipidemia | 1.62 (1.42, 1.86) *** | 1.38 (1.19, 1.59) *** | 1.29 (0.95, 1.77) | 1.18 (1.06, 1.32) ** | 0.97 (0.86, 1.09) | 1.00 (0.93, 1.07) | - | |
| Variables | Syncope and Collapse | Compared to Control | ||||||
|---|---|---|---|---|---|---|---|---|
| No | Yes | |||||||
| Events n | PY | Rate # | Events n | PY | Rate # | Crude HR (95% CI) | Adjusted HR † (95% CI) | |
| ACS | ||||||||
| All | 435 | 17,613 | 24.7 | 409 | 13,611 | 30.1 | 1.21 (1.06, 1.39) ** | 1.28 (1.11, 1.46) *** |
| Gender | ||||||||
| Female | 217 | 9601 | 22.6 | 204 | 7450 | 27.4 | 1.20 (0.99, 1.46) | 1.26 (1.04, 1.53) * |
| Male | 218 | 8011 | 27.2 | 205 | 6161 | 33.3 | 1.22 (1.01, 1.48) * | 1.29 (1.06, 1.56) * |
| p-value for interaction | 0.97 | |||||||
| Age, years | ||||||||
| ≤49 | 32 | 3421 | 9.36 | 56 | 2930 | 19.1 | 2.16 (1.39, 3.36) *** | 2.30 (1.48, 3.57) *** |
| 50–64 | 155 | 6205 | 25.0 | 146 | 5030 | 29.0 | 1.16 (0.92, 1.45) | 1.23 (0.98, 1.54) |
| ≥65 | 248 | 7987 | 31.1 | 207 | 5650 | 36.6 | 1.19 (0.99, 1.43) | 1.17 (0.97, 1.41) |
| p-value for interaction | 0.16 | |||||||
| Dialysis modality | ||||||||
| Peritoneal dialysis | 26 | 1413 | 18.4 | 31 | 1319 | 23.5 | 1.28 (0.76, 2.16) | 1.30 (0.76, 2.21) |
| Hemodialysis | 409 | 16,200 | 25.3 | 378 | 12,292 | 30.8 | 1.21 (1.05, 1.39) ** | 1.24 (1.08, 1.43) ** |
| p-value for interaction | 0.86 | |||||||
| Comorbidity § | ||||||||
| No | 21 | 1746 | 12.0 | 14 | 1282 | 10.9 | 0.91 (0.46, 1.79) | 1.02 (0.51, 2.01) |
| Yes | 414 | 15,867 | 26.1 | 395 | 12,329 | 32.0 | 1.23 (1.07, 1.41) ** | 1.27 (1.10, 1.46) *** |
| p-value for interaction | 0.41 | |||||||
| Arrhythmia/cardiac arrest | ||||||||
| All | 65 | 18,542 | 3.51 | 98 | 14,527 | 6.75 | 1.93 (1.41, 2.65) *** | 2.05 (1.50, 2.82) *** |
| Gender | ||||||||
| Female | 31 | 10,067 | 3.08 | 49 | 7900 | 6.20 | 2.01 (1.28, 3.16) ** | 2.08 (1.32, 3.27) ** |
| Male | 34 | 8475 | 4.01 | 49 | 6627 | 7.39 | 1.85 (1.19, 2.87) ** | 2.03 (1.30, 3.16) ** |
| p-value for interaction | 0.76 | |||||||
| Age, years | ||||||||
| ≤49 | 5 | 3526 | 1.42 | 5 | 3089 | 1.62 | 1.16 (0.33, 4.02) | 1.13 (0.32, 3.92) |
| 50–64 | 25 | 6561 | 3.81 | 38 | 5375 | 7.07 | 1.87 (1.13, 3.11) * | 1.99 (1.20, 3.31) ** |
| ≥65 | 35 | 8456 | 4.14 | 25 | 6063 | 9.07 | 2.23 (1.45, 3.42) *** | 2.24 (1.46, 3.43) *** |
| p-value for interaction | 0.49 | |||||||
| Dialysis modality | ||||||||
| Peritoneal dialysis | 4 | 1457 | 2.74 | 6 | 1381 | 4.35 | 1.71 (0.48, 6.14) | 1.73 (0.48, 6.29) |
| Hemodialysis | 61 | 17,085 | 3.57 | 92 | 13,146 | 7.00 | 1.96 (1.42, 2.71) *** | 2.01 (1.45, 2.78) *** |
| p-value for interaction | 0.75 | |||||||
| Comorbidity § | ||||||||
| No | 5 | 1783 | 2.80 | 4 | 1322 | 3.03 | 1.07 (0.29, 3.99) | 1.16 (0.31, 4.38) |
| Yes | 60 | 16,760 | 3.58 | 94 | 13,205 | 7.12 | 2.00 (1.45, 2.77) *** | 2.08 (1.50, 2.88) *** |
| p-value for interaction | 0.37 | |||||||
| Stroke | ||||||||
| All | 611 | 17,114 | 35.7 | 686 | 13,304 | 51.6 | 1.40 (1.26, 1.56) *** | 1.48 (1.33, 1.66) *** |
| Gender | ||||||||
| Female | 298 | 9341 | 31.9 | 338 | 7294 | 46.3 | 1.42 (1.21, 1.66) *** | 1.49 (1.28, 1.75) *** |
| Male | 313 | 7773 | 40.3 | 348 | 6010 | 57.9 | 1.39 (1.19, 1.62) *** | 1.46 (1.25, 1.71) *** |
| p-value for interaction | 0.92 | |||||||
| Age, years | ||||||||
| ≤49 | 55 | 3384 | 16.3 | 71 | 2935 | 24.2 | 1.50 (1.05, 2.13) * | 1.56 (1.10, 2.22) * |
| 50–64 | 176 | 6104 | 28.8 | 226 | 4871 | 46.4 | 1.59 (1.30, 1.93) *** | 1.70 (1.40, 2.08) *** |
| ≥65 | 380 | 7627 | 49.8 | 389 | 5498 | 70.8 | 1.36 (1.18, 1.56) *** | 1.37 (1.19, 1.58) *** |
| p-value for interaction | 0.52 | |||||||
| Dialysis modality | ||||||||
| Peritoneal dialysis | 23 | 1376 | 16.7 | 57 | 1279 | 44.6 | 2.44 (1.50, 3.96) *** | 2.46 (1.51, 4.00) *** |
| Hemodialysis | 588 | 15,738 | 37.4 | 629 | 12,025 | 52.3 | 1.36 (1.22, 1.53) *** | 1.40 (1.25, 1.57) *** |
| p-value for interaction | 0.01 | |||||||
| Comorbidity § | ||||||||
| No | 36 | 1686 | 21.4 | 25 | 1265 | 19.8 | 0.89 (0.54, 1.49) | 0.98 (0.58, 1.64) |
| Yes | 575 | 15,428 | 37.3 | 661 | 12,039 | 54.9 | 1.43 (1.28, 1.60) *** | 1.48 (1.32, 1.66) *** |
| p-value for interaction | 0.09 | |||||||
| Mortality | ||||||||
| All | 1447 | 18,569 | 77.9 | 1859 | 14,555 | 127.7 | 1.65 (1.54, 1.77) *** | 1.79 (1.67, 1.92) *** |
| Gender | ||||||||
| Female | 715 | 10,078 | 71.0 | 942 | 7910 | 119.1 | 1.70 (1.54, 1.87) *** | 1.82 (1.65, 2.01) *** |
| Male | 732 | 8491 | 86.2 | 917 | 6645 | 138.0 | 1.60 (1.46, 1.77) *** | 1.78 (1.61, 1.96) *** |
| p-value for interaction | 0.45 | |||||||
| Age, years | ||||||||
| ≤49 | 99 | 3527 | 28.1 | 160 | 3093 | 51.7 | 1.86 (1.45, 2.40) *** | 1.93 (1.50, 2.48) *** |
| 50–64 | 367 | 6572 | 55.8 | 543 | 5390 | 100.7 | 1.82 (1.60, 2.08) *** | 1.90 (1.66, 2.17) *** |
| ≥65 | 981 | 8470 | 115.8 | 1156 | 6072 | 190.4 | 1.70 (1.56, 1.85) *** | 1.71 (1.57, 1.86) *** |
| p-value for interaction | 0.19 | |||||||
| Dialysis modality | ||||||||
| Peritoneal dialysis | 79 | 1459 | 54.2 | 155 | 1385 | 111.9 | 2.02 (1.54, 2.65) *** | 2.17 (1.65, 2.86) *** |
| Hemodialysis | 1368 | 17,110 | 80.0 | 1704 | 13,170 | 129.4 | 1.63 (1.52, 1.75) *** | 1.66 (1.55, 1.78) *** |
| p-value for interaction | 0.09 | |||||||
| Comorbidity § | ||||||||
| No | 101 | 1783 | 56.7 | 134 | 1321 | 101.4 | 1.75 (1.35, 2.26) *** | 2.07 (1.59, 2.69) *** |
| Yes | 1346 | 16,786 | 80.2 | 1725 | 13,233 | 130.4 | 1.64 (1.53, 1.76) *** | 1.75 (1.63, 1.88) *** |
| p-value for interaction | 0.48 | |||||||
| Frequency for Medical Visit, Per Year | Event | PY | Rate # | Crude HR (95% CI) | Adjusted HR † (95% CI) |
|---|---|---|---|---|---|
| ACS | |||||
| Without syncope and collapse | 435 | 17,613 | 24.7 | 1.00 | 1.00 |
| With syncope and collapse | |||||
| 0–1 | 218 | 11,461 | 19.0 | 0.78 (0.66, 0.91) ** | 0.83 (0.71, 0.98) * |
| 1–2 | 61 | 1049 | 58.2 | 2.41 (1.84, 3.17) *** | 2.26 (1.72, 2.97) *** |
| ≥3 | 130 | 1101 | 118.0 | 4.85 (3.97, 5.93) *** | 4.57 (3.74, 5.60) *** |
| p-value for trend | <0.001 | ||||
| Arrhythmia/cardiac arrest | |||||
| Without syncope and collapse | 65 | 18,542 | 3.51 | 1.00 | 1.00 |
| With syncope and collapse | |||||
| 0–1 | 51 | 11,926 | 4.28 | 1.23 (1.86, 1.78) | 1.35 (0.93, 1.95) |
| 1–2 | 16 | 1191 | 13.4 | 4.03 (2.32, 7.02) *** | 3.83 (2.19, 6.67) *** |
| ≥3 | 31 | 1409 | 22.0 | 6.55 (4.23, 10.1) *** | 6.08 (3.92, 9.42) *** |
| p-value for trend | |||||
| Stroke | |||||
| Without syncope and collapse | 611 | 17,114 | 35.7 | 1.00 | 1.00 |
| With syncope and collapse | |||||
| 0–1 | 332 | 11,379 | 29.2 | 0.82 (0.71, 0.93) ** | 0.88 (0.77, 1.01) |
| 1–2 | 112 | 977 | 114.6 | 2.99 (2.43, 3.66) *** | 2.82 (2.30, 3.47) *** |
| ≥3 | 242 | 948 | 255.3 | 6.47 (5.55, 7.54) *** | 6.26 (5.36, 7.30) *** |
| p-value for trend | <0.001 | ||||
| Mortality | |||||
| Without syncope and collapse | 1447 | 18,569 | 77.9 | 1.00 | 1.00 |
| With syncope and collapse | |||||
| 0–1 | 1000 | 11,944 | 83.7 | 1.09 (1.00, 1.18) * | 1.22 (1.13, 1.33) *** |
| 1–2 | 307 | 1193 | 257.4 | 3.48 (3.07, 3.94) *** | 3.24 (2.86, 3.67) *** |
| ≥3 | 552 | 1418 | 389.3 | 5.22 (4.72, 5.76) *** | 4.86 (4.40, 5.38) *** |
| p-value for trend | <0.001 | ||||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, S.-T.; Yu, T.-M.; Ke, T.-Y.; Wu, M.-J.; Chuang, Y.-W.; Li, C.-Y.; Chiu, C.-W.; Lin, C.-L.; Liang, W.-M.; Chou, T.-C.; et al. Syncope and Collapse Are Associated with an Increased Risk of Cardiovascular Disease and Mortality in Patients Undergoing Dialysis. Int. J. Environ. Res. Public Health 2018, 15, 2082. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15102082
Huang S-T, Yu T-M, Ke T-Y, Wu M-J, Chuang Y-W, Li C-Y, Chiu C-W, Lin C-L, Liang W-M, Chou T-C, et al. Syncope and Collapse Are Associated with an Increased Risk of Cardiovascular Disease and Mortality in Patients Undergoing Dialysis. International Journal of Environmental Research and Public Health. 2018; 15(10):2082. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15102082
Chicago/Turabian StyleHuang, Shih-Ting, Tung-Min Yu, Tai-Yuan Ke, Ming-Ju Wu, Ya-Wen Chuang, Chi-Yuan Li, Chih-Wei Chiu, Cheng-Li Lin, Wen-Miin Liang, Tzu-Chieh Chou, and et al. 2018. "Syncope and Collapse Are Associated with an Increased Risk of Cardiovascular Disease and Mortality in Patients Undergoing Dialysis" International Journal of Environmental Research and Public Health 15, no. 10: 2082. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15102082