Depression Negatively Impacts Survival of Patients with Metastatic Prostate Cancer

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Database
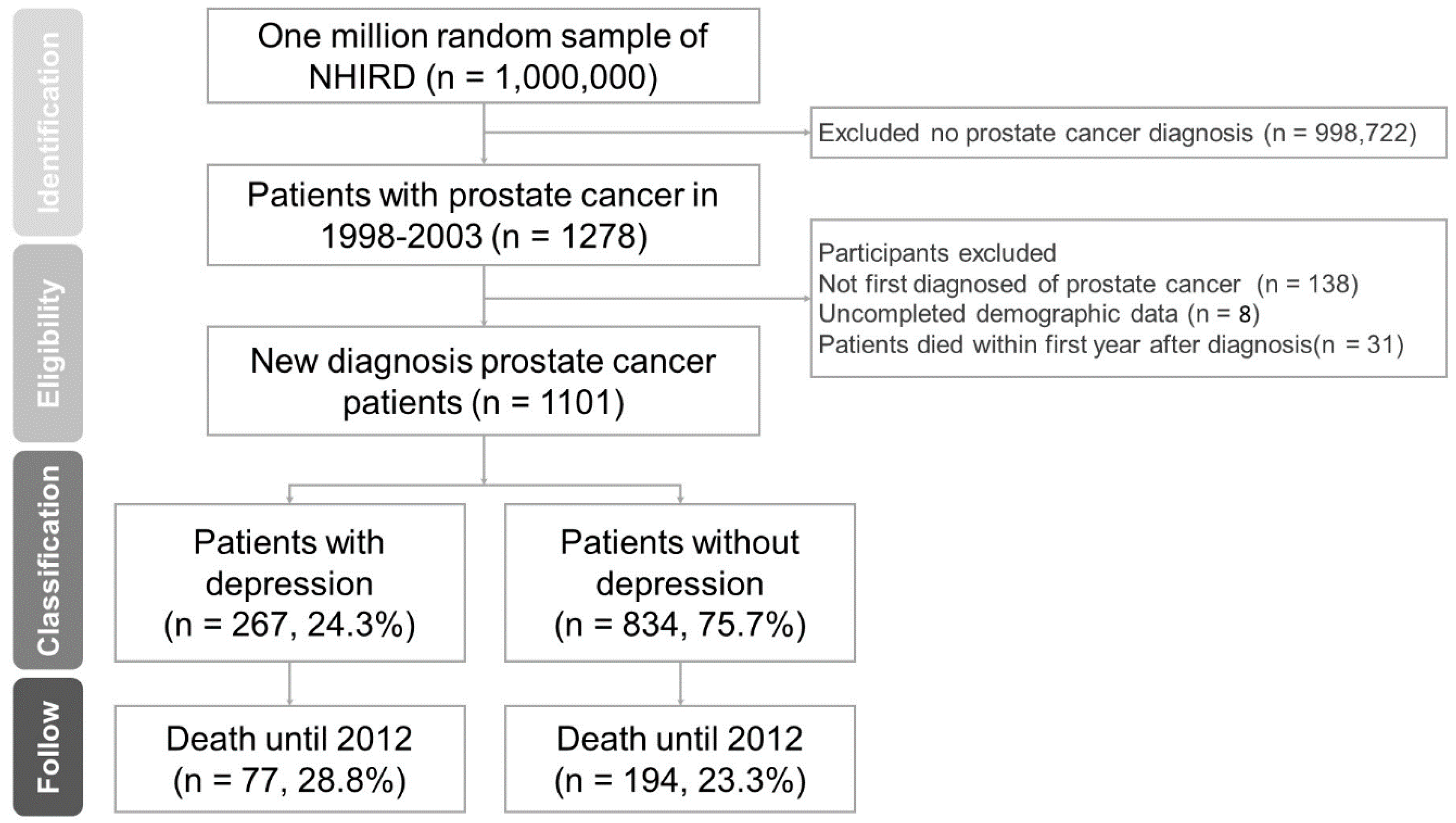
2.2. Study Participants
2.3. Study Outcomes
2.4. Adjustment of Covariates
2.5. Statistical Methods
3. Results
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Canoui-Poitrine, F.; Reinald, N.; Laurent, M.; Guery, E.; Caillet, P.; David, J.P.; Tournigand, C.; Lagrange, J.L.; Bastuji-Garin, S.; Lemogne, C.; et al. Geriatric assessment findings independently associated with clinical depression in 1092 older patients with cancer, the ELCAPA cohort study. Psychooncology 2016, 25, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Meyer, F.; Fletcher, K.; Prigerson, H.G.; Braun, I.M.; Maciejewski, P.K. Advanced cancer as a risk for major depressive episodes. Psychooncology 2015, 24, 1080–1087. [Google Scholar] [CrossRef] [PubMed]
- Raison, C.L.; Miller, A.H. Depression in cancer, new developments regarding diagnosis and treatment. Biol. Psychiatry 2003, 54, 283–294. [Google Scholar] [CrossRef]
- Giese-Davis, J.; Collie, K.; Rancourt, K.M.; Neri, E.; Kraemer, H.C.; Spiegel, D. Decrease in depression symptoms is associated with longer survival in patients with metastatic breast cancer: A secondary analysis. J. Clin. Oncol. 2011, 29, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Steel, J.L.; Geller, D.A.; Gamblin, T.C.; Olek, M.C.; Carr, B.I. Depression, immunity, and survival in patients with hepatobiliary carcinoma. J. Clin. Oncol. 2007, 25, 2397–2405. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.C.; Chen, S.J.; Liu, C.Y. Risk of developing depressive disorders following hepatocellular carcinoma: A nationwide population-based study. PLoS ONE 2016, 10, e0135417. [Google Scholar] [CrossRef] [PubMed]
- Pirl, W.F.; Greer, J.A.; Traeger, L.; Jackson, V.; Lennes, I.T.; Gallagher, E.R.; Perez-Cruz, P.; Heist, R.S.; Temel, J.S. Depression and survival in metastatic non-small-cell lung cancer: Effects of early palliative care. J. Clin. Oncol. 2012, 30, 1310–1315. [Google Scholar] [CrossRef] [PubMed]
- Taiwanese Health Promotion Administration, Ministry of Health and Welfare. Available online: https://cris.hpa.gov.tw/pagepub/Home.aspx (accessed on 15 July 2018).
- Lin, S.K.; Liu, J.M.; Chang, Y.H.; Ting, Y.T.; Pang, S.T.; Hsu, R.J.; Lin, P.H. Increased risk of endotracheal intubation and heart failure following acute myocardial infarction in patients with urolithiasis, a nationwide population-based study. Ther. Clin. Risk Manag. 2017, 13, 245–253. [Google Scholar] [CrossRef] [PubMed]
- National Center for Health Statistics. The International Classification of Diseases, 9th Revision, Clinical Modification, ICD-9-CM; US Department of Health and Human Services, Public Health Service, Health Care Financing Administration: Atlanta, GA, USA, 1989.
- Lin, S.K.; Lin, P.H.; Hsu, R.J.; Chuang, H.C.; Liu, J.M. Traditional Chinese medicine therapy reduces the catheter indwelling risk in dementia patients with difficult voiding symptoms. J. Ethnopharmacol. 2017, 203, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.M.; Lin, P.H.; Hsu, R.J.; Chang, Y.H.; Cheng, K.C.; Pang, S.T.; Lin, S.K. Complementary traditional Chinese medicine therapy improves survival in patients with metastatic prostate cancer. Medicine 2016, 95, e4475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krebber, A.M.; Buffart, L.M.; Kleijn, G.; Riepma, I.C.; De Bree, R.; Leemans, C.R.; Becker, A.; Brug, J.; Van Straten, A.; Cuijpers, P.; et al. Prevalence of depression in cancer patients: A meta-analysis of diagnostic interviews and self-report instruments. Psychooncology 2014, 23, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Schneider, S.; Moyer, A. Depression as a predictor of disease progression and mortality in cancer patients: A meta-analysis. Cancer 2010, 116, 3304. [Google Scholar] [CrossRef] [PubMed]
- Huggins, C.; Hodges, C.V. Studies on prostatic cancer, I. The effect of castration, of estrogen and of androgen injection on serum phosphatases in metastatic carcinoma of the prostate. J. Urol. 2002, 168, 9–12. [Google Scholar] [CrossRef]
- European Association of Urology. Available online: http://uroweb.org/guideline/prostate-cancer (accessed on 1 March 2018).
- Gilbert, S.M.; Kuo, Y.F.; Shahinian, V.B. Prevalent and incident use of androgen deprivation therapy among men with prostate cancer in the United States. Urol. Oncol. 2011, 29, 647–653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shahinian, V.B.; Kuo, Y.F.; Freeman, J.L.; Orihuela, E.; Goodwin, J.S. Increasing use of gonadotropin-releasing hormone agonists for the treatment of localized prostate carcinoma. Cancer 2005, 103, 1615–1624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saini, A.; Berruti, A.; Cracco, C.; Sguazzotti, E.; Porpiglia, F.; Russo, L.; Bertaglia, V.; Picci, R.L.; Negro, M.; Tosco, A.; et al. Psychological distress in men with prostate cancer receiving adjuvant androgen-deprivation therapy. Urol. Oncol. 2013, 31, 352–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dinh, K.T.; Reznor, G.; Muralidhar, V.; Mahal, B.A.; Nezolosky, M.D.; Choueiri, T.K.; Hoffman, K.E.; Hu, J.C.; Sweeney, C.J.; Trinh, Q.D.; et al. Association of androgen deprivation therapy with depression in localized prostate cancer. J. Clin. Oncol. 2016, 34, 1905–1912. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Jim, H.S.; Fishman, M.; Zachariah, B.; Heysek, R.; Biagioli, M.; Jacobsen, P.B. Depressive symptomatology in men receiving androgen deprivation therapy for prostate cancer, a controlled comparison. Psychooncology 2015, 24, 472–477. [Google Scholar] [CrossRef] [PubMed]
- Prasad, S.M.; Eggener, S.E.; Lipsitz, S.R.; Irwin, M.R.; Ganz, P.A.; Hu, J.C. Effect of depression on diagnosis, treatment, and mortality of men with clinically localized prostate cancer. J. Clin. Oncol. 2014, 32, 2471–2478. [Google Scholar] [CrossRef] [PubMed]
- Ng, A.; Tam, W.W.; Zhang, M.W.; Ho, C.S.; Husain, S.F.; McIntyre, R.S.; Ho, R.C. IL-1β, IL-6, TNF- α and CRP in elderly patients with depression or Alzheimer’s disease: Systematic review and meta-analysis. Sci. Rep. 2018, 8, 12050. [Google Scholar] [CrossRef] [PubMed]
- Aldea, M.; Craciun, L.; Tomuleasa, C.; Crivii, C. The role of depression and neuroimmune axis in the prognosis of cancer patients. J. BUON 2014, 19, 5–14. [Google Scholar] [PubMed]
- Lu, Y.; Ho, C.S.; Liu, X.; Chua, A.N.; Wang, W.; McIntyre, R.S.; Ho, R.C. Chronic administration of fluoxetine and pro-inflammatory cytokine change in a rat model of depression. PLoS ONE 2017, 12, e0186700. [Google Scholar] [CrossRef] [PubMed]
- Minsun, L.; Yuan, S.; Lin, Z.; Grace, X.M. Coping strategies and benefit-finding in the relationship between non-disclosure and depressive symptoms among breast cancer survivors in China. Am. J. Health Behav. 2017, 41, 368–377. [Google Scholar]
- Romanzini, A.E.; Pereira, M.D.G.; Guilherme, C.; Cologna, A.J.; Carvalho, E.C. Predictors of well-being and quality of life in men who underwent radical prostatectomy: Longitudinal study. Rev. Lat.-Am. Enferm. 2018, 26, e3031. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.M.; Tsai, C.M.; Wu, Y.C.; Lin, K.C.; Lin, C.C. Randomised controlled trial on the effectiveness of home-based walking exercise on anxiety, depression and cancer-related symptoms in patients with lung cancer. Br. J. Cancer 2015, 112, 438–445. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Patients with Depression No. (%) | Patients without Depression No. (%) | Chi-Square Test p-Value |
|---|---|---|---|
| Total | 267 (100%) | 834 (100%) | |
| Age at diagnosis | 0.58 | ||
| <60 | 14 (5.24%) | 60 (7.19%) | |
| 60–70 | 34 (12.73%) | 142 (17.03%) | |
| 70–80 | 78 (29.21%) | 242 (29.02%) | |
| ≥80 | 141 (52.81%) | 390 (46.76% | |
| Urbanization | 0.58 | ||
| Very high | 143 (53.56%) | 473 (56.71%) | |
| High | 57 (21.35%) | 177 (21.22%) | |
| Moderate | 47 (17.60%) | 138 (16.55%) | |
| Low | 20 (7.49%) | 46 (5.52%) | |
| Insured amount (NT$) a | 0.43 | ||
| Dependent | 59 (22.10%) | 216 (25.90%) | |
| 1–199,99 | 114 (42.70%) | 314 (37.65%) | |
| 20,000–39,999 | 61 (22.85%) | 165 (19.78%) | |
| ≥40,000 | 33 (12.36%) | 139 (16.67%) | |
| Comorbidity | |||
| Diabetes mellitus | 134 (50.19%) | 348 (41.73%) | 0.04 |
| Chronic kidney disease | 74 (27.72%) | 224 (26.86%) | 0.06 |
| Cerebrovascular accident | 152 (56.93%) | 355 (42.57%) | 0.66 |
| Coronary heart disease | 170 (63.67%) | 433 (51.92%) | 0.04 |
| Heart failure | 90 (33.71%) | 184 (22.06%) | <0.001 |
| Liver cirrhosis | 139 (52.06%) | 295 (35.37%) | 0.02 |
| Hypertension | 232 (86.89%) | 619 (74.22%) | 0.03 |
| Prostate cancer type | 0.04 | ||
| Localize or Locally Advance | 73 (27.3%) | 320 (38.4%) | |
| Metastatic | 194 (72.7%) | 51 4 (61.7%) |
| Variables | Adjust Hazard Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Depression | |||
| Non depression | [Reference] | [Reference] | [Reference] |
| 1.37 | 1.04-1.80 | 0.01 | 1.37 |
| Age at diagnosis | |||
| <60 | [Reference] | [Reference] | [Reference] |
| 60–70 | 0.95 | 0.38–2.37 | 0.91 |
| 70–80 | 1.24 | 0.55–2.81 | 0.61 |
| ≥80 | 1.63 | 0.73–3.64 | 0.23 |
| Urbanization | |||
| Very high | [Reference] | [Reference] | [Reference] |
| High | 1.29 | 0.95–1.75 | 0.11 |
| Moderate | 1.73 | 1.26–2.38 | 0.02 |
| Low | 1.61 | 0.95–2.73 | 0.08 |
| Insured amount (NT$) b | |||
| Dependent | [Reference] | [Reference] | [Reference] |
| 1–19,999 | 1.25 | 0.93–1.68 | 0.13 |
| 20,000–39,999 | 0.83 | 0.62–0.95 | 0.03 |
| ≥40,000 | 0.57 | 0.39–0.71 | 0.02 |
| Comorbidity | |||
| Diabetes mellitus | 1.19 | 0.93–1.52 | 0.18 |
| Chronic kidney disease | 1.08 | 0.80–1.46 | 0.61 |
| Cerebrovascular accident | 1.09 | 0.84–1.42 | 0.50 |
| Coronary heart disease | 1.15 | 0.77–1.70 | 0.50 |
| Liver cirrhosis | 1.30 | 1.00–1.69 | 0.05 |
| Hypertension | 1.61 | 1.23–2.10 | 0.01 |
| Prostate Cancer Type | Adjust Hazard Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Localize or Locally Advance Prostate Cancer | 1.20 | 0.83–2.34 | 0.07 |
| Metastatic Prostate Cancer | 1.52 | 1.04–2.10 | 0.02 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, P.-H.; Liu, J.-M.; Hsu, R.-J.; Chuang, H.-C.; Chang, S.-W.; Pang, S.-T.; Chang, Y.-H.; Chuang, C.-K.; Lin, S.-K. Depression Negatively Impacts Survival of Patients with Metastatic Prostate Cancer. Int. J. Environ. Res. Public Health 2018, 15, 2148. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15102148
Lin P-H, Liu J-M, Hsu R-J, Chuang H-C, Chang S-W, Pang S-T, Chang Y-H, Chuang C-K, Lin S-K. Depression Negatively Impacts Survival of Patients with Metastatic Prostate Cancer. International Journal of Environmental Research and Public Health. 2018; 15(10):2148. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15102148
Chicago/Turabian StyleLin, Po-Hung, Jui-Ming Liu, Ren-Jun Hsu, Heng-Chang Chuang, Su-Wei Chang, See-Tong Pang, Ying-Hsu Chang, Cheng-Keng Chuang, and Shun-Ku Lin. 2018. "Depression Negatively Impacts Survival of Patients with Metastatic Prostate Cancer" International Journal of Environmental Research and Public Health 15, no. 10: 2148. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15102148