Protected Natural Areas: In Sickness and in Health



Abstract
:1. Introduction
1.1. Natural Environment and Health: The Evidence
1.2. Protected Natural Areas in Relation to Health and Well-Being
2. Methodology
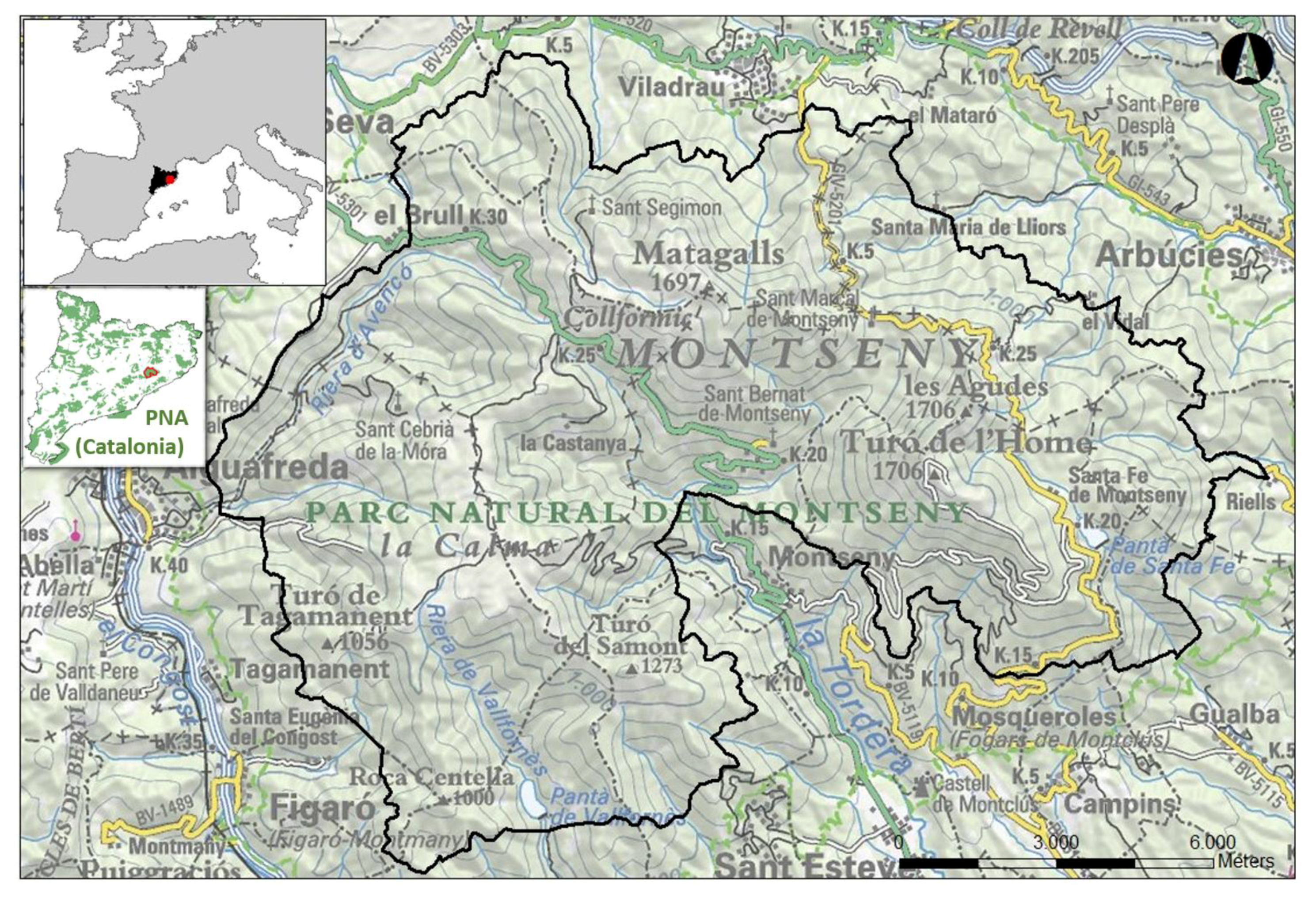
2.1. Study Area
2.2. Participants and Data Collection
2.3. Questionnaire Design
2.4. Data Analysis
3. Results
3.1. Frequency of Visiting Montseny NP-BR
3.2. Beliefs in the Benefits of Nature in Relation to Health
3.3. Reasons for Visiting Montseny NP-BR
3.4. Health-Related Activities in Montseny NP-BR
3.4.1. Exercise
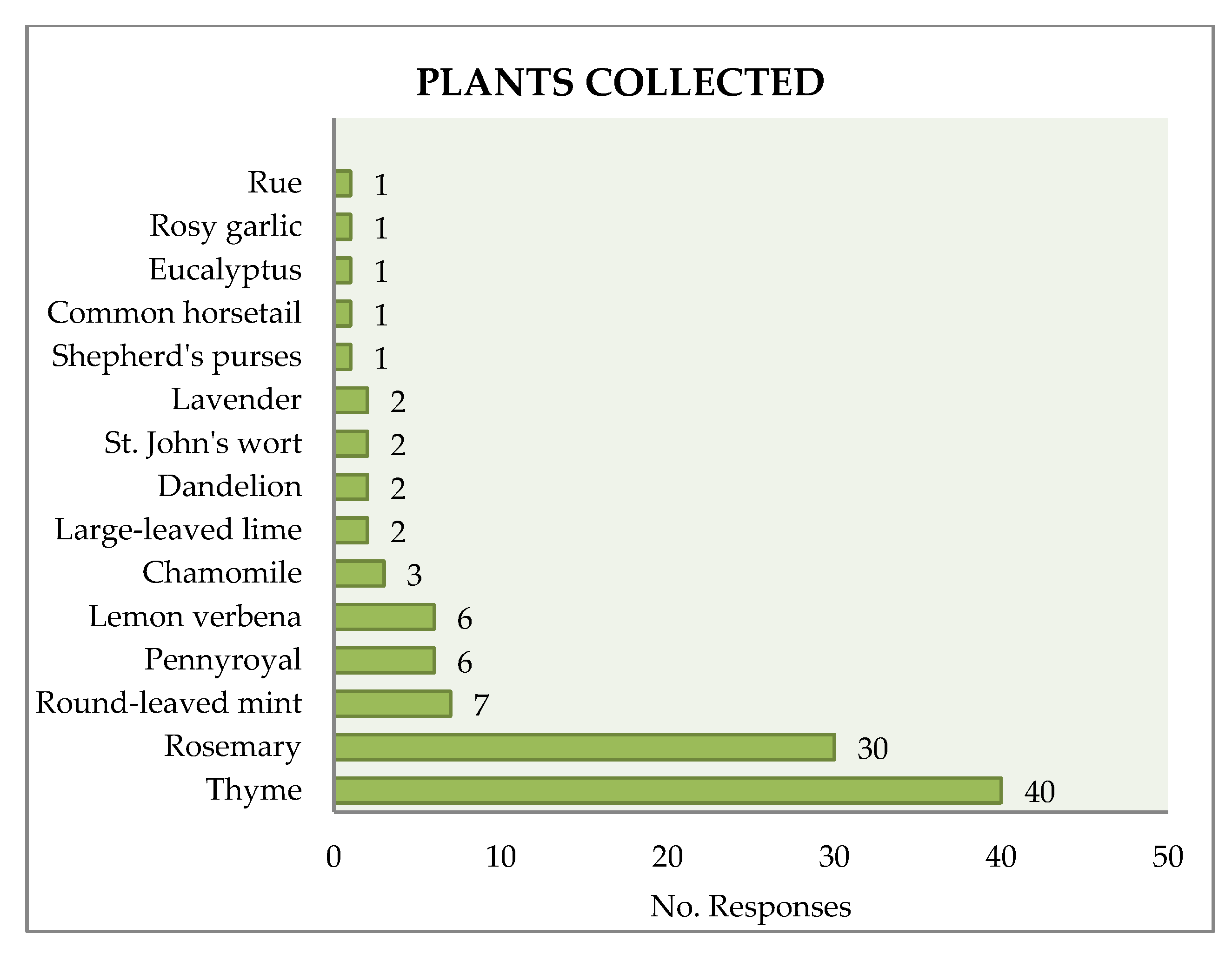
3.4.2. Plant-Picking
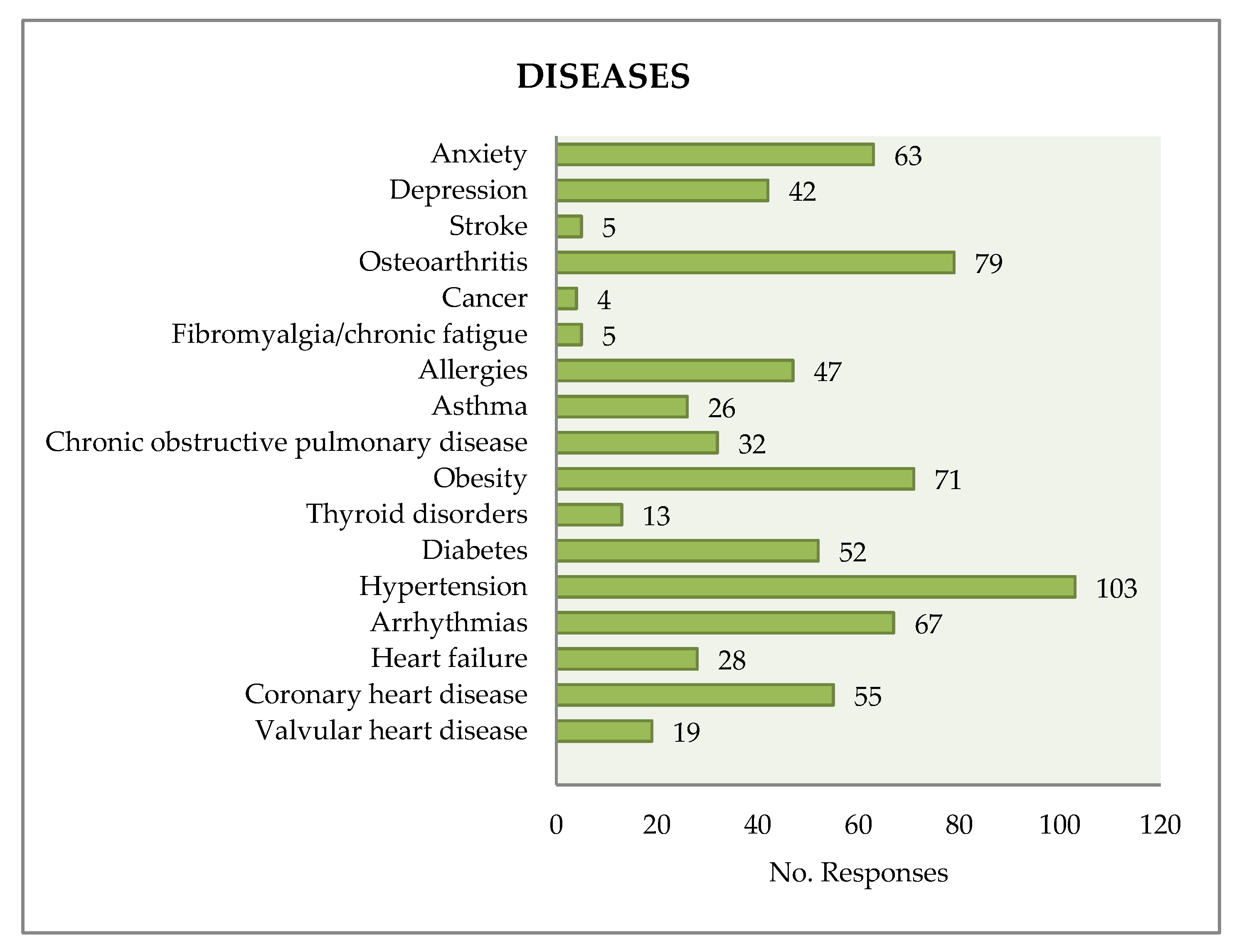
3.5. Beliefs, Motivations, and Activities in Relation to the Diseases Suffered
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interests
References
- Keniger, L.E.; Gaston, K.J.; Irvine, K.N.; Fuller, R.A. What are the benefits of interacting with nature? Int. J. Environ. Res. Public Health 2013, 10, 913–935. [Google Scholar] [CrossRef] [PubMed]
- Hartig, T.; Mitchell, R.; de Vries, S.; Frumkin, H. Nature and health. Annu. Rev. Public Health 2014, 35, 207–228. [Google Scholar] [CrossRef] [PubMed]
- Fong, K.C.; Hart, J.E.; James, P. A review of epidemiologic studies on greenness and health: Updated literature through 2017. Curr. Environ. Health Rep. 2018, 2, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Kassebaum, N.J.; Arora, M.; Barber, R.M.; Bhutta, Z.A.; Brown, J.; Carter, A.; Casey, D.C.; Charlson, F.J.; Coates, M.M.; Coggeshall, M.; et al. Global, regional, and national disability-adjusted life-years (DALYs) for 315 diseases and injuries and healthy life expectancy (HALE), 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1603–1658. [Google Scholar] [CrossRef] [Green Version]
- Wagner, K.H.; Brath, H. A global view on the development of non-communicable diseases. Prev. Med. 2012, 54, S38–S41. [Google Scholar] [CrossRef] [PubMed]
- Mokdad, A.H.; Ford, E.S.; Bowman, B.A.; Dietz, W.H.; Vinicor, F.; Bales, V.S.; Marks, J.S. Prevalence of obesity, diabetes, and obesity-related health risk factors, 2001. JAMA 2003, 289, 76–79. [Google Scholar] [CrossRef] [PubMed]
- Goodwin, R.D. Association between physical activity and mental disorders among adults in the United States. Prev. Med. 2003, 36, 698–703. [Google Scholar] [CrossRef]
- Calle, E.E.; Thun, M. Obesity and cancer. Oncogene 2004, 23, 6365. [Google Scholar] [CrossRef] [PubMed]
- Kelishadi, R.; Poursafa, P. A review on the genetic, environmental, and lifestyle aspects of the early-life origins of cardiovascular disease. Curr. Probl. Pediatr. Adolesc. Health Care 2014, 44, 54–72. [Google Scholar] [CrossRef] [PubMed]
- Lear, S.A.; Hu, W.; Rangarajan, S.; Gasevic, D.; Leong, D.; Iqbal, R.; Rosengren, A. The effect of physical activity on mortality and cardiovascular disease in 130,000 people from 17 high-income, middle-income, and low-income countries: The PURE study. Lancet 2017, 390, 2643–2654. [Google Scholar] [CrossRef]
- Bowler, D.E.; Buyung-Ali, L.M.; Knight, T.M.; Pullin, A.S. A systematic review of evidence for the added benefits to health of exposure to natural environments. BMC Public Health 2010, 10, 456. [Google Scholar] [CrossRef] [PubMed]
- James, P.; Banay, R.F.; Hart, J.E.; Laden, F. A Review of the Health Benefits of Greenness. Curr. Epid. Rep. 2015, 2, 131. [Google Scholar] [CrossRef] [PubMed]
- Pretty, J.; Rogerson, M.; Barton, J. Green Mind Theory: How brain-body-behaviour links into natural and social environments for healthy habits. Int. J. Environ. Res. Public Health 2017, 14, 706. [Google Scholar] [CrossRef] [PubMed]
- Marcus, C.C.; Barnes, M. Healing Gardens: Therapeutic Benefits and Design Recommendations; John Wiley & Sons: New York, NY, USA, 1999; ISBN 0-471-19203-1. [Google Scholar]
- Daniel, T.M. The history of tuberculosis. Respir. Med. 2006, 100, 1862–1870. [Google Scholar] [CrossRef] [PubMed]
- Maas, J.; Verheij, R.; Groenewegen, P.P.; de Vries, S.; Spreeuwenberg, P. Green space, urbanity, and health: How strong is the relation? J. Epid. Comm. Health 2006, 60, 587–592. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.C.K.; Maheswaran, R. The health benefits of urban green spaces: A review of the evidence. J. Public Health 2011, 33, 212–222. [Google Scholar] [CrossRef] [PubMed]
- Kondo, M.C.; Fluehr, J.M.; McKeon, T.; Branas, C.C. Urban green space and its impact on human health. Int. J. Environ. Res. Public Health 2018, 15, 445. [Google Scholar] [CrossRef] [PubMed]
- Healthy Outside-Healthy Inside: The human health and well-being benefits of Alberta’s protected areas—Towards a benefits-based management agenda. Available online: www.ccea.org (accessed on 17 March 2018).
- Romagosa, F.; Eagles, P.F.; Lemieux, C.J. From the inside out to the outside in: Exploring the role of parks and protected areas as providers of human health and well-being. J. Outdoor Recreat. Tour. 2015, 10, 70–77. [Google Scholar] [CrossRef]
- Jiang, Y.; Yuan, Y.; Neale, A.; Jackson, L.; Mehaffey, M. Association between natural resources for outdoor activities and physical inactivity: results from the contiguous United States. Int. J. Environ. Res. Public Health 2016, 13, 830. [Google Scholar] [CrossRef] [PubMed]
- Guidelines for Applying Protected Area Management Categories 2008. Available online: https://portals.iucn.org/library/sites/library/files/documents/PAG-021.pdf (accessed on 25 March 2018).
- Ulrich, R.S. View through a window may influence recovery from surgery. Am. Assoc. Adv. Sci. 1984, 224, 420–421. [Google Scholar] [CrossRef] [Green Version]
- James, P.; Banay, R.F.; Hart, J.E.; Laden, F. A review of the health benefits of greenness. Curr. Epidemiol. Rep. 2015, 2, 131–142. [Google Scholar] [CrossRef] [PubMed]
- Van den Berg, M.; Wendel-Vos, W.; Van Poppel, M.; Kemper, H.; Van Mechelen, W.; Maas, J. Health benefits of green spaces in the living environment: A systematic review of epidemiological studies. Urban For. Urban Green. 2015, 14, 806–816. [Google Scholar] [CrossRef]
- Van den Bosch, M.; Ode Sang, Å. Urban natural environments as nature-based solutions for improved public health—A systematic review of reviews. Environ. Res. 2017, 158, 373–384. [Google Scholar] [CrossRef] [PubMed]
- Gascon, M.; Triguero-Mas, M.; Martínez, D.; Dadvand, P.; Rojas-Rueda, D.; Plasència, A.; Nieuwenhuijsen, M.J. Residential green spaces and mortality: A systematic review. Environ. Int. 2016, 86, 60–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, J.; Rappazzo, K.M.; Simpson, R.J.; Joodi, G.; Pursell, I.W.; Mounsey, J.P.; Cascio, W.E.; Jackson, L.E. Exploring links between greenspace and sudden unexpected death—A spatial analysis. Environ. Int. 2018, 113, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Vienneau, D.; de Hoogh, K.; Faeh, D.; Kaufmann, M.; Wunderli, J.M.; Roosli, M. More than clean air and tranquillity: Residential green is independently associated with decreasing mortality. Environ. Int. 2017, 108, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Takano, T.; Nakamura, K.; Watanabe, M. Urban residential environments and senior citizens’ longevity in megacity areas: The importance of walkable green spaces. J. Epidemiol. Community Health 2002, 56, 913–918. [Google Scholar] [CrossRef]
- Mitchell, R.; Astell-Burt, T.; Richardson, E. A comparison of green space indicators for epidemiological research. J. Epidemiol. Community Health 2011, 65, 853–858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jonker, M.F.; van Lenthe, F.J.; Donkers, B.; Mackenbach, J.P; Burdorf, A. The effect of urban green on small-area (healthy) life expectancy. J. Epidemiol. Community Health 2014, 68, 999–1002. [Google Scholar] [CrossRef] [PubMed]
- Pereira, G.; Foster, S.; Martin, K.; Christian, H.; Boruff, B.J.; Knuiman, M.; Giles-Corti, B. The association between neighborhood greenness and cardiovascular disease: An observational study. BMC Public Health 2012, 12, 466. [Google Scholar] [CrossRef] [PubMed]
- Tamosiunas, A.; Grazuleviciene, R.; Luksiene, D.; Dedele, A.; Reklaitiene, R.; Baceviciene, M.; Vencloviene, J.; Bernotiene, G.; Radisauskas, R.; Malinauskiene, V. Accessibility and use of urban green spaces, and cardiovascular health: findings from a Kaunas cohort study. Environ. Health 2014, 13, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, Y.S.; Lung, S.C. Can green structure reduces the mortality of cardiovascular diseases? Sci. Total Environ. 2016, 566, 1159–1167. [Google Scholar] [CrossRef] [PubMed]
- Prince, S.A.; Kristjansson, E.A.; Russell, K.; Billette, J.M.; Sawada, M.; Ali, A.; Tremblay, M.S.; Prud’homme, D. A multilevel analysis of neighbourhood built and social environments and adult self-reported physical activity and body mass index in Ottawa, Canada. Int. J. Environ. Res. Public Health 2011, 8, 3953–3978. [Google Scholar] [CrossRef] [PubMed]
- Boncinelli, F.; Riccioli, F.; Marone, E. Do forests help to keep my body mass index low? For. Policy Econ. 2015, 54, 11–17. [Google Scholar] [CrossRef] [Green Version]
- Ghimire, R.; Ferreira, S.; Green, G.T.; Poudyal, N.C.; Cordell, H.K.; Thapa, J.R. Green Space and Adult Obesity in the United States. Ecol. Econ. 2017, 136, 201–212. [Google Scholar] [CrossRef]
- Li, Q.; Kobayashi, M.; Kawada, T. Relationships between Percentage of Forest Coverage and Standardized Mortality Ratios (SMR) in All Prefectures in Japan. Open Public Health J. 2008, 1, 1–7. [Google Scholar] [CrossRef]
- Donovan, G.H.; Michael, Y.L.; Butry, D.T.; Sullivan, A.D.; Chase, J.M. Urban trees and the risk of poor birth outcomes. Health Place 2011, 17, 390–393. [Google Scholar] [CrossRef] [PubMed]
- Dadvand, P.; Villanueva, C.M.; Font-Ribera, L.; Martinez, D.; Basagaña, X.; Belmonte, J.; Vrijheid, M.; Gražulevičienė, R.; Kogevinas, M.; Nieuwenhuijsen, M.J. Risks and benefits of green spaces for children: A cross-sectional study of associations with sedentary behavior, obesity, asthma, and allergy. Environ. Health Perspect. 2014, 122, 1329–1335. [Google Scholar] [CrossRef] [PubMed]
- Markevych, I.; Tiesler, C.M.; Fuertes, E.; Romanos, M.; Dadvand, P.; Nieuwenhuijsen, M.J.; Berdel, D.; Koletzko, S.; Heinrich, J. Access to urban green spaces and behavioural problems in children: Results from the GINIplus and LISAplus studies. Environ. Int. 2014, 71, 29–35. [Google Scholar] [CrossRef] [PubMed]
- de Vries, S.; van Dillen, S.M.E.; Groenewegen, P.P.; Spreeuwenberg, P. Streetscape greenery and health: Stress, social cohesion and physical activity as mediators. Soc. Sci. Med. 2013, 94, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Strum, R.; Cohen, D. Proximity to urban parks and mental health. J. Ment. Health Policy Econ. 2014, 17, 19–24. [Google Scholar]
- Beyer, K.M.M.; Kaltenbach, A.; Szabo, A.; Bogar, S.; Nieto, F.J.; Malecki, K.M. Exposure to neighborhood green space and mental health: Evidence from the survey of the health of Wisconsin. Int. J. Environ. Res. Public Health 2014, 11, 3453–3472. [Google Scholar] [CrossRef] [PubMed]
- Gascon, M.; Sánchez-Benavides, G.; Dadvand, P.; Martínez, D.; Gramunt, N.; Gotsens, X.; Cirach, M.; Vert, C.; Molinuevo, J.L.; Crous-Bou, M.; Nieuwenhuijsen, M.; et al. Long-term exposure to residential green and blue spaces and anxiety and depression in adults—A cross-sectional study. Environ. Res. 2018, 162, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Das, K.V.; Chen, Q. Neighborhood green, social support, physical activity, and stress: Assessing the cumulative impact. Health Place 2011, 17, 1202–1211. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, T.; Leslie, E.; Giles-Corti, B.; Owen, N. Associations of neighbourhood greenness with physical and mental health: Do walking, social coherence and local social interaction explains the relationships? J. Epidemiol. Community Health 2008, 62, e9. [Google Scholar] [CrossRef]
- Richardson, E.A.; Pearce, J.; Mitchell, R.; Kingham, S. Role of physical activity in the relationship between urban green space and health. Public Health 2013, 127, 318–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gascon, M.; Triguero-Mas, M.; Martínez, D.; Dadvand, P.; Forns, J.; Plasència, A.; Nieuwenhuijsen, M.J. Mental health benefits of long term exposure to residential green and blue spaces: A systematic review. Int. J. Environ. Res. Public Health 2015, 12, 4354–4379. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, R. The nature of the view from home psychological benefits. Environ. Behav. 2001, 33, 507–542. [Google Scholar] [CrossRef]
- Triguero-Masa, M.; Dadvand, P.; Ciracha, M.; Martínez, D.; Medinad, A.; Momparte, A.; Basagaña, X.; Gražulevičienėf, R.; Nieuwenhuijsen, M.J. Natural outdoor environments and mental and physical health: Relationships and mechanisms. Environ. Int. 2015, 77, 35–41. [Google Scholar] [CrossRef] [PubMed]
- DeVries, S.; Verheij, R.A.; Groenewegen, P.P.; Spreeuwenberg, P. Natural environments—Healthy environments? An exploratory analysis of the relationship between green space and health. Environ. Plan. A 2003, 35, 1717–1731. [Google Scholar] [CrossRef]
- Ulrich, R.S.; Lundén, O.; Eltinge, J.L. Effects of exposure to nature and abstract pictures on patients recovering from heart surgery. J. Soc. Psy. Res. 1993, 30, 204–221. [Google Scholar]
- Shen, Y.S.; Lung, S.C.C. Mediation pathways ans effects of green structures on respiratory mortality via reducing air pollution. Sci. Rep. 2017, 7, 42854. [Google Scholar] [CrossRef] [PubMed]
- Coombes, E.; Jones, A.P.; Hillsdon, M. The relationship of physical activity and overweight to objectively measured green space accessibility and use. Soc. Sci. Med. 2010, 70, 816–822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dadvand, P.; Bartoll, X.; Basagaña, X.; Dalmau-Bueno, A.; Martinez, D.; Ambros, A.; Cirach, M.; Triguero-Mas, M.; Gascon, M.; Borrell, C.; Nieuwenhuijsen, M.J. Green spaces and General Health: Roles of mental health status, social support, and physical activity. Environ. Int. 2016, 91, 161–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson Coon, J.; Boddy, K.; Stein, K.; Whear, R.; Barton, J.; Depledge, M.H. Does participating in physical activity in outdoor natural environments have a greater effect on physical and mental wellbeing than physical activity indoors? A systematic review. Environ. Sci. Technol. 2011, 45, 1761–1772. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, S. The restorative benefits of nature: Toward an integrative framework. J. Environ. Psychol. 1995, 15, 169–183. [Google Scholar] [CrossRef]
- Mayer, F.S.; Frantz, C.M. The connectedness to nature scale: A measure of individuals’ feeling in community with nature. J. Environ. Psychol. 2004, 24, 503–515. [Google Scholar] [CrossRef]
- Capaldi, C.A.; Dopko, R.L.; Zelenski, J.M. The relationship between nature connectedness and happiness: A meta-analysis. Front. Psychol. 2104, 5, 76. [Google Scholar] [CrossRef] [PubMed]
- Bedimo-Rung, A.L.; Mowen, A.J.; Cohen, D.A. The significance of parks to physical activity and public health: A conceptual model. Am. J. Prev. Med. 2005, 28, 159–168. [Google Scholar] [CrossRef] [PubMed]
- Jansen, F.M.; Ettema, D.F.; Kamphuis, C.B.M.; Pierik, F.H.; Dijst, M.J. How do type and size of natural environments relate to physical activity behavior? Health Place 2017, 46, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Nordh, H.; Hartig, T.; Hagerhal, C.M.; Fry, G. Components of small urban parks that predict the possibility for restoration. Urban For. Urban Green. 2009, 8, 225–235. [Google Scholar] [CrossRef]
- Akpinar, A. How is quality of urban green spaces associated with physical activity and health? Urban For. Urban Green. 2016, 16, 76–83. [Google Scholar] [CrossRef]
- Foo, C.H. Linking forest naturalness and human wellbeing—A study on public’s experiential connection to remnant forests within a highly urbanized region in Malaysia. Urban For. Urban Green. 2016, 16, 13–24. [Google Scholar] [CrossRef]
- Laumann, K.; Garling, T.; Stormark, K. Rating scale measures of restorative components of environments. J. Environ. Psychol. 2001, 21, 31–44. [Google Scholar] [CrossRef]
- Van Dillen, S.M.; de Vries, S.; Groenewegen, P.P.; Spreeuwenberg, P. Greenspace in urban neighbourhoods and residents’ health: Adding quality to quantity. J. Epidemiol. Commun. Health 2012, 66, e8. [Google Scholar] [CrossRef] [PubMed]
- Dallimer, M.; Irvine, K.N.; Skinner, A.M.; Davies, Z.G.; Rouquette, J.R.; Maltby, L.L.; Warren, H.; Armasworth, R.P.; Gaston, K.J. Biodiversity and the feel-good factor: Understanding associations between self-reported human well-being and species richness. BioScience 2012, 62, 47–55. [Google Scholar] [CrossRef] [Green Version]
- Wheeler, B.W.; Lovell, R.; Higgins, S.L.; White, M.P.; Alcock, I.; Osborne, N.J.; Depledge, M.H. Beyond greenspace: An ecological study of population general health and indicators of natural environment type and quality. Int. J. Health Geogr. 2015, 14, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shanahan, D.F.; Fuller, R.A.; Bush, R.; Lin, B.B.; Gaston, K.J. The health benefits of urban nature: How much do we need? BioScience 2015, 65, 476–485. [Google Scholar] [CrossRef]
- Sandifer, P.A.; Sutton-Grier, A.E.; Ward, B.P. Exploring connections among nature, biodiversity, ecosystem services, and human health and well-being: Opportunities to enhance health and biodiversity conservation. Ecosyst. Serv. 2015, 12, 1–15. [Google Scholar] [CrossRef]
- Carrus, G.; Scopelliti, M.; Lafortezza, R.; Colangelo, G.; Ferrini, F.; Salbitano, F.; Sanesi, G. Go greener, feel better? The positive effects of biodiversity on the well-being of individuals visiting urban and peri-urban green areas. Landsc. Urban Plan. 2015, 134, 221–228. [Google Scholar] [CrossRef]
- Rook, G.A. Regulation of the immune system by biodiversity from the natural environment: An ecosystem service essential to health. PNAS 2013, 110, 18360–18367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strachan, D.P. Hay fever, hygiene, and household size. BMJ 1989, 229, 1259–1260. [Google Scholar] [CrossRef]
- Von Hertzen, L.; Hanski, I.; Haahtela, T. Natural immunity: Biodiversity loss and inflammatory diseases are two global megatrends that might be related. EMBO Rep. 2011, 12, 1089–1093. [Google Scholar] [CrossRef] [PubMed]
- Maas, J.; Verheij, R.A.; De Vries, S.; Spreeuwenberg, P.; Schellevis, F.G.; Groenewegen, P.P. Morbidity is related to a green living environment. J. Epidemiol. Commun. H. 2009, 63, 967–973. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Browning, M.; Lee, K. Within what distance does “greenness” best predict physical health? A systematic review of articles with GIS buffer analyses across the lifespan. Int. J. Environ. Res. Public Health 2017, 14, 675. [Google Scholar] [CrossRef] [PubMed]
- Vital Sites: The Contribution of Protected Areas to Human Health: A Research Report by WWF and Equilibrium Research. Available online: https://www.iucn.org/content/vital-sites-contribution-protected-areas-human-health (accessed on 27 March 2018).
- European Environment Agency. Protected Areas in Europe: An Overview. Available online: https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&ved=2ahUKEwj5gtje-_DdAhVD_ywKHc9oBnAQFjAAegQICRAC&url=http%3A%2F%2Fahpne.fr%2FIMG%2Fpdf%2FEEA_05-2012_Protected_areas_in_Europe-an_overview.pdf&usg=AOvVaw1Y4nkLnBLnltnjSOlvD1fQ (accessed on 27 March 2018).
- Balmford, A.; Green, J.M.; Anderson, M.; Beresford, J.; Huang, C.; Naidoo, R.; Wallpole, M.; Manica, A. Walk on the Wild Side: Estimating the Global Magnitude of Visits to Protected Areas. PLoS Biol. 2015, 13, e1002074. [Google Scholar] [CrossRef] [PubMed]
- Protected areas and biodiversity: An Overview of Key Issues. CBD Secretariat and UNEP-WCMC, Montreal, Canada and Cambridge, UK. 2004. Available online: http://www.dolomitipark.it/doc_pdf/parchi.sola.terra/07.ProtectedAreas_Biodiversity.pdf (accessed on 27 March 2018).
- Daniel, T.C.; Muhar, A.; Arnberger, A.; Aznar, O.; Boyd, J.W.; Chan, K.M.; Costanza, R.; Elmqvist, T.; Flint, C.G.; Gobster, P.H.; et al. Contributions of cultural services to the ecosystem services agenda. Proc. Nat. Acad. Sci. USA 2012, 109, 8812–8819. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gesler, W.M. Therapeutic landscapes: Medical issues in light of the new cultural geography. Soc. Sci. Med. 1992, 34, 735–746. [Google Scholar] [CrossRef]
- Mace, B.L.; Bell, P.A.; Loomis, R.J. Visibility and natural quiet in national parks and wilderness areas: Psychological considerations. Environ. Behav. 2004, 36, 5–31. [Google Scholar] [CrossRef]
- Kingsley, J.Y.; Townsend, M. “Dig In” to social capital: Community gardens as mechanisms for growing urban social connectedness. Urban Policy Res. 2006, 24, 525–537. [Google Scholar] [CrossRef]
- Rowe, D.B. Green roofs as a means of pollution abatement. Environ. Pollut. 2011, 159, 2100–2110. [Google Scholar] [CrossRef] [PubMed]
- Baró, F.; Chaparro, L.; Gómez-Baggethun, E.; Langemeyer, J.; Nowak, D.J.; Terradas, J. Contribution of ecosystem services to air quality and climate change mitigation policies: The case of urban forests in Barcelona, Spain. Ambio 2014, 43, 466–479. [Google Scholar] [CrossRef] [PubMed]
- Salkeld, D.J.; Padgett, K.A.; Jones, J.H. A meta-analysis suggesting that the relationship between biodiversity and risk of zoonotic pathogen transmission is idiosyncratic. Ecol. Lett. 2013, 16, 679–686. [Google Scholar] [CrossRef] [PubMed]
- Lemieux, C.J.; Eagles, P.F.; Slocombe, D.S.; Doherty, S.T.; Elliott, S.J.; Mock, S.E. Human health and well-being motivations and benefits associated with protected area experiences: An opportunity for transforming policy and management in Canada. Parks 2012, 18, 71–85. [Google Scholar]
- Jones, K.R.; Wills, J. The Invention of the Park: From the Garden of Eden to Disney’s Magic Kingdom; Polity: Cambridge, UK, 2005; p. 216. ISBN 074563138X. 05. [Google Scholar]
- El Parc Natural del Montseny y el turismo sostenible. Available online: http://www.redeuroparc.org/system/files/shared/CETS-MONTSENY3b85.pdf (accessed on 27 March 2018).
- Boada, M.; i Juncá, M.B. El Montseny. Cinquanta anys d’evolució dels paisatges; Publicacions de l’Abadia de Montserrat: Barcelona, Spain, 2002; ISBN 84-8415-393-2. [Google Scholar]
- Santos, A.; Pinho, P.; Munzi, S.; Botelho, M.J.; Palma-Oliveira, J.M.; Branquinho, C. The role of forest in mitigating the impact of atmospheric dust pollution in a mixed landscape. Environ. Sci. Poll. Res. 2017, 24, 12038–12048. [Google Scholar] [CrossRef] [PubMed]
- Torbidoni, E.I.F. El Aprovechamiento recreativo, deportivo y turístico de los espacios naturales protegidos: modelos de frecuentación, el caso del Parc Nacional d’Aigüestortes i Estany de Sant Maurici-Espanya. Ph.D. Thesis, Universitat de Lleida, Lleida, Spain, 2003. [Google Scholar]
- Torbidoni, E.I.F. Managing for recreational experience opportunities: The case of hikers in protected areas in Catalonia, Spain. Environ. Manag. 2011, 47, 482–496. [Google Scholar] [CrossRef] [PubMed]
- Fuentes, M.C. Análisis de la demanda de uso público en tres parques naturales de Galicia. Boletín de la Asociación de Geógrafos Españoles 2013, 61, 261–284. [Google Scholar]
- La percepció dels visitants de la Xarxa de Parcs com a espais de salut. Available online: https://parcs.diba.cat/documents/10534/74749675/11-30-Francesc+Romagosa.pdf/59090f6c-44cc-4907-8355-292de35a25e5 (accessed on 27 March 2018).
- Stigsdotter, U.K.; Ekholm, O.; Schipperijn, J.; Toftager, M.; Kamper-Jørgensen, F.; Randrup, T.B. Health promoting outdoor environments—Associations between green space, and health, health-related quality of life and stress based on a Danish national representative survey. Scand. J. Public Health 2010, 38, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Forestry Commision. Public Opinion of Forestry 2017, UK and England. Available online: https://www.forestry.gov.uk/pdf/pof2017ukeng.pdf/$FILE/pof2017ukeng.pdf (accessed on 17 March 2018).
- Healthy Outside-Healthy Inside: The Human Health & Well-being Benefits of Alberta’s Protected Areas—Towards a benefits-based management agenda. Available online: http://www.ccea.org/wp-content/uploads/2015/10/P20_Healthy-Outside-Healthy-Inside.pdf (accessed on 25 March 2018).
- Bell, S. Design for Outdoor Recreation, 2nd ed.; Taylor and Francis: Abingdon, UK, 2008; ISBN 0-203-92811-3. [Google Scholar]
- Kendal, D.; Ford, R.M.; Anderson, N.M.; Farrar, A. The VALS: A new tool to measure people’s general valued attributes of landscapes. J. Environ. Manag. 2015, 163, 224–233. [Google Scholar] [CrossRef] [PubMed]
- Richardson, E.A.; Mitchell, R. Gender differences in relationships between urban green space and health in the United Kingdom. Soc. Sci. Med. 2010, 71, 568–575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soroka, A.; Mazurek-Kusiak, A.; Wojciechowska-Solis, J.; Hawlena, J. Importance of forest resources in health tourism—Wigierski National Park case study. Sylwan 2016, 160, 64–70. [Google Scholar]
- Puhakka, R.; Pitkänen, K.; Siikamäki, P. The health and well-being impacts of protected areas in Finland. J. Sus. Tour. 2017, 25, 1830–1847. [Google Scholar] [CrossRef]
- Romagosa, F. Physical health in green spaces: Visitors’ perceptions and activities in protected areas around Barcelona. J. Outdoor Recreat. Tour. 2018, 23, 26–32. [Google Scholar] [CrossRef]
- Marselle, M.R.; Irvine, K.N.; Lorenzo-Arribas, A.; Warber, S.L. Moving beyond green: Exploring the relationship of environment type and indicators of perceived environmental quality on emotional well-being following group walks. Int. J. Environ. Res. Public Health 2014, 12, 106–130. [Google Scholar] [CrossRef] [PubMed]
- Weiler, B.; Moyle, B.D.; Wolf, I.D.; de Bie, K.; Torland, M. Assessing the efficacy of communication interventions for shifting public perceptions of park benefits. J. Travel Res. 2017, 56, 468–481. [Google Scholar] [CrossRef]
- Simon, J.G.; De Boer, J.B.; Joung, I.M.A.; Bosma, H.; Mackenback, J.P. How is your health in general? A qualitative study on self-assessed health. Eur. J. Public Health 2005, 15, 200–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willaert, L. El Sanatori del Montseny. Monogr. Montseny 2008, 23, 135–141. [Google Scholar]
- Agència de Salut Pública de Barcelona. La salut a Barcelona 2016. Available online: http://www.aspb.cat (accessed on 15 January 2018).
- EUROSTAT. Time spent on health-enhancing (non-work-related) aerobic physical activity by sex, age and educational attainment level. 2017. Available online: http://ec.europa.eu/eurostat/web/products-eurostat-news/-/DDN-20170302-1 (accessed on 30 March 2018).
- Clarke, T.C.; Norris, T.; Schiller, J.S. Early release of selected estimates based on data from 2016 National Health Interview Survey. Available online: https://www.cdc.gov/nchs/data/nhis/earlyrelease/earlyrelease201705.pdf (accessed on 10 April 2018).
- WHO. Available online: http://www.who.int/mediacentre/factsheets/fs385/es/ (accessed on 30 March 2018).
- Go, A.S.; Mozaffarian, D.; Roger, V.L.; Benjamin, E.J.; Berry, J.D.; Blaha, M.J.; Dai, S.; Ford, E.S.; Fox, C.S.; Franco, S. Heart disease and stroke statistics—2013 update: A report from the American heart association. Circulation 2013, 127, e6–e245. [Google Scholar] [CrossRef] [PubMed]
- Stewart, R.A.; Held, C.; Hadziosmanovic, N.; Armstrong, P.W.; Cannon, C.P.; Granger, C.B.; Nicolau, J.C. Physical activity and mortality in patients with stable coronary heart disease. J. Am. Coll. Cardiol. 2017, 70, 1689–1700. [Google Scholar] [CrossRef] [PubMed]
- European Guidelines on cardiovascular disease prevention in clinical practice. Available online: https://0-doi-org.brum.beds.ac.uk/10.1016/j.atherosclerosis.2016.05.037 (accessed on 27 March 2018).
- Kahn, E.B.; Ramsey, L.T.; Brownson, R.C.; Heath, G.W.; Howze, E.H.; Powell, K.E.; Stone, E.J.; Rajab, M.W.; Corso, P. The effectiveness of interventions to increase physical activity: A systematic review. Am. J. Prev. Med. 2002, 22, 73–107. [Google Scholar] [CrossRef]
- The world health report 2006: Working together for health. Available online: http://apps.who.int/iris/bitstream/handle/10665/43432/9241563176_eng.pdf;jsessionid=A20DBA9C7AABAFBB2687F772F34EBA38?sequence=1 (accessed on 10 April 2018).
- Björk, J.; Albin, M.; Grahn, P.; Jacobsson, H.; Ardo, J.; Wadbro, J.; Östergren, P.-O.; Skärbäck, E. Recreational values of the natural environment in relation to neighbourhood satisfaction, physical activity, obesity and wellbeing. J. Epidemiol. Community Health 2008, 62, e2. [Google Scholar] [CrossRef]
- Guthold, R.; Ono, T.; Strong, K.L.; Chatterji, S.; Morabia, A. Worldwide variability in physical inactivity a 51-country survey. Am. J. Prev. Med. 2008, 34, 486–494. [Google Scholar] [CrossRef] [PubMed]
- Reis, J.P.; Bowles, H.R.; Ainsworth, B.E.; Dubose, K.D.; Smith, S.; Laditka, J.N. Non-occupational physical activity by degree of urbanization and US geographic region. Med. Sci. Sports Exerc. 2004, 36, 2093–2098. [Google Scholar] [CrossRef] [PubMed]
- Patterson, P.D.; Moore, C.G.; Probst, J.C.; Shinogle, J.A. Obesity and physical inactivity in rural America. J. Rural Health 2004, 20, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Flores, J.C.M. Tourism in the Spanish protected areas, something more than a new trend. Boletín de la Asociación de Geógrafos Españoles 2008, 46, 291–304. [Google Scholar]
- Lee, C.; Moudon, A.V. Physical Activity and Environment Research in the Health Field: Implications for Urban and Transportation Planning Practice and Research. J. Plan. Liter. 2004, 19, 147–181. [Google Scholar] [CrossRef]
- Brownson, R.C.; Baker, E.A.; Housemann, R.A.; Brennan, L.K.; Bacak, S.J. Environmental and policy determinants of physical activity in the United States. Am. J. Public Health 2001, 91, 1995–2003. [Google Scholar] [CrossRef] [PubMed]
- Troped, P.J.; Saunders, R.P.; Pate, R.R.; Reininger, B.; Ureda, J.R.; Thompson, S.J. Associations between self-reported and objective physical environmental factors and use of a community rail-trail. Prev. Med. 2001, 32, 191–200. [Google Scholar] [CrossRef] [PubMed]
- Giles-Corti, B.; Donovan, R.J. The relative influence of individual, social and physical environment determinants of physical activity. Soc. Sci. Med. 2002, 54, 1793–1812. [Google Scholar] [CrossRef]
- Parks, S.E.; Housemann, R.A.; Brownson, R.C. Differential correlates of physical activity in urban and rural adults of various socioeconomic backgrounds in the United States. J. Epidemiol. Community Health 2003, 57, 29–35. [Google Scholar] [CrossRef] [Green Version]
- Reyes-García, V.; Menendez-Baceta, G.; Aceituno-Mata, L.; Acosta-Naranjo, R.; Calvet-Mir, L.; Domínguez, P.; Rodríguez-Franco, R. From famine foods to delicatessen: Interpreting trends in the use of wild edible plants through cultural ecosystem services. Ecol. Econ. 2015, 120, 303–311. [Google Scholar] [CrossRef] [Green Version]
- Tardío, J.; Pardo-de-Santayana, M.; Morales, R. Ethnobotanical review of wild edible plants in Spain. Bot. J. Linn. Soc. 2006, 152, 27–71. [Google Scholar] [CrossRef] [Green Version]
- Pardo de Santayana, M.; Pieroni, A.; Puri, R.K. Ethnobotany in the New Europe: People, Health and Wild Plant Resources; Berghahn Books: New York, NY, USA, 2008; ISBN 978-1-78238-124-2. [Google Scholar]
- Hamilton, A.C. Medicinal plants, conservation and livelihoods. Biodivers. Conserv. 2004, 13, 1477–1517. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Patients | Sex | Age | |||||||
|---|---|---|---|---|---|---|---|---|---|
| n = 250 | Man n = 133 | Women n = 115 | p-Value | 16–30 n = 7 | 31–50 n = 57 | 51–65 n = 68 | >65 n = 116 | p-Value | |
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |||
| Reasons for Visiting Montseny NP-BR | |||||||||
| Enjoy | 112 (44.8) | 54 (40.6) | 58 (50.4) | 0.155 | 5 (4.46) | 34 (30.4) | 26 (23.2) | 47 (42.0) | 0.028 ** |
| Health | 66 (26.4) | 33 (24.8) | 32 (27.8) | 0.694 | 1 (1.52) | 16 (24.2) | 22 (33.3) | 27 (40.9) | 0.534 |
| Tranquility | 101 (40.4) | 50 (37.6) | 51 (44.3) | 0.342 | 3 (3.00) | 30 (30.0) | 29 (29.0) | 38 (38.0) | 0.082* |
| Leisure | 42 (16.8) | 29 (21,8) | 13 (11.3) | 0.042 ** | 0 (0.00) | 6 (14.6) | 9 (22.0) | 26 (63.4) | 0.123 |
| Plant-picking | 70 (28.0) | 45 (33.8) | 53 (46.1) | 0.066 * | 3 (4.35) | 9 (13.0) | 22 (31.9) | 35 (50.7) | 0.088 * |
| Benefits of Nature in Relation to Health | |||||||||
| Pure air | 68 (27.2) | 32 (24.1) | 36 (31.3) | 0.257 | 1 (14.3) | 20 (35.1) | 16 (23.5) | 30 (25.9) | 0.451 |
| Tranquility | 44 (17.6) | 18 (13,5) | 25 (21,7) | 0.125 | 1 (14.3) | 12 (21.1) | 17 (25.0) | 14 (12.1) | 0.117 |
| Health | 25 (10.0) | 14 (10.5) | 11 (9.57) | 0.969 | 1 (14.3) | 5 (8.77) | 10 (14.7) | 9 (7.76) | 0.365 |
| Exercise | 12 (4.80) | 8 (6.20) | 4 (3.48) | 0.528 | 0 (0.00) | 3 (5.26) | 4 (5.88) | 5 (4.31) | 0.905 |
| Spiritual | 2 (0.80) | 1 (0.75) | 1 (0.87) | 1.000 | 0 (0.00) | 1 (1.75) | 0 (0.00) | 1 (0.86) | 0.525 |
| Health-Related Activities | |||||||||
| Exercise | 204 (81.9) | 107 (81.1) | 95 (82.6) | 0.881 | 5 (71.4) | 48 (84.2) | 55 (80.9) | 94 (81.7) | 0.816 |
| Plant-picking | 99 (39.6) | 45 (33.8) | 53 (46.1) | 0.066 * | 3 (4.35) | 9 (13.0) | 22 (31.9) | 35 (50.7) | 0.088 * |
| Patients n = 250 | Diabetes n = 52 | Obesity n = 71 | Heart Dis. n = 107 | Hypertension n = 147 | |||||
|---|---|---|---|---|---|---|---|---|---|
| n (%) | n (%) | p-value | n (%) | p-value | n (%) | p-value | n (%) | p-value | |
| Reasons for Visiting Montseny NP-BR | |||||||||
| Enjoy | 112 (44.8) | 16 (30.8) | 0.031 ** | 28 (39.4) | 0.374 | 42 (39.3) | 0.162 | 58 (39.5) | 0.041 ** |
| Health | 66 (26.4) | 14 (26.9) | 1.000 | 18 (25.4) | 0.919 | 28 (26.2) | 1.000 | 39 (26.5) | 1.000 |
| Tranquility | 101 (40.4) | 19 (36.5) | 0.622 | 33 (46.5) | 0.290 | 46 (43.0) | 0.554 | 58 (39.5) | 0.838 |
| Leisure | 42 (16.8) | 12 (23.1) | 0.192 | 9 (12,7) | 0.353 | 20 (18.7) | 0.602 | 32 (21.8) | 0.023 ** |
| Plant-picking | 70 (28.0) | 19 (36.5) | 0.167 | 21 (29.6) | 0.796 | 32 (29.9) | 0.661 | 48 (32.7) | 0.057 |
| Benefits of Nature in Relation to Health | |||||||||
| Pure air | 68 (27.2) | 13 (25.0) | 0.889 | 19 (26.8) | 1.000 | 24 (22.4) | 0.168 | 37 (25.2) | 0.635 |
| Tranquility | 44 (17.6) | 3 (5.77) | 0.019 ** | 6 (8.45) | 0.026 ** | 16 (15.0) | 0.434 | 18 (12.2) | 0.010 ** |
| Health | 25 (10.0) | 7 (13.5) | 0.522 | 8 (11.3) | 0.862 | 12 (11.2) | 0.733 | 17 (11.6) | 0.470 |
| Exercise | 12 (4.80) | 2 (3.85) | 1.000 | 6 (8.45) | 0.106 | 7 (6.54) | 0.415 | 9 (6.12) | 0.369 |
| Spiritual | 2 (0.80) | 0 (0.00) | 1.000 | 1 (1.41) | 0.490 | 1 (0.93) | 1.000 | 0 (0.00) | 0.165 |
| Health-Related Activities | |||||||||
| Exercise | 204 (81.9) | 38 (74.5) | 0.166 | 55 (77.5) | 0.340 | 85 (80.2) | 0.655 | 118 (80.3) | 0.433 |
| Plant-picking | 99 (39.6) | 19 (36.5) | 0.768 | 26 (36.6) | 0.620 | 46 (43.0) | 0.414 | 64 (43.5) | 0.153 |
| Patients n = 250 | Allergies n = 47 | Respiratory Dis. n = 51 | Anx./Depress. n = 78 | Osteoarthritis n = 79 | |||||
|---|---|---|---|---|---|---|---|---|---|
| n (%) | p-value | n (%) | p-value | n (%) | p-value | n (%) | p-value | ||
| Reasons for Visiting Montseny NP-BR | |||||||||
| Enjoy | 112 (44.8) | 20 (42.6) | 0.856 | 42 (82.4) | 1.000 | 34 (46.6) | 0.903 | 26 (32.9) | 0.015 ** |
| Health | 66 (26.4) | 15 (31.9) | 0.442 | 16 (31.4) | 0.468 | 25 (32.1) | 0.226 | 24 (30.4) | 0.415 |
| Tranquility | 101 (40.4) | 22 (46.8) | 0.407 | 24 (47.1) | 0.354 | 37 (47.4) | 0.165 | 31 (39.2) | 0.908 |
| Leisure | 42 (16.8) | 14 (29.8) | 0.015** | 9 (17.6) | 1.000 | 8 (10.3) | 0.093 * | 16 (20.3) | 0.418 |
| Plant-picking | 70 (28.0) | 11 (23.4) | 0.550 | 13 (25.5) | 0.785 | 24 (30.8) | 0.614 | 20 (25.3) | 0.624 |
| Benefits of Nature in Relation to Health | |||||||||
| Pure air | 68 (27.2) | 19 (40.4) | 0.038 ** | 16 (31.4) | 0.566 | 26 (3.3) | 0.189 | 15 (19.0) | 0.067 * |
| Tranquility | 44 (17.6) | 7 (14.9) | 0.743 | 7 (13.7) | 0.543 | 15 19.2) | 0.782 | 13 (16.5) | 0.885 |
| Health | 25 (10.0) | 3 (6.38) | 0.558 | 6 (11.8) | 0.834 | 9 (11.5) | 0.750 | 8 (10.1) | 1.000 |
| Exercise | 12 (4.80) | 3 (6.38) | 0.558 | 2 (3.92) | 1.000 | 1 (1.28) | 0.111 | 4 (5.06) | 1.000 |
| Spiritual | 2 (0.80) | 1 (2.13) | 0.341 | 0 (0.00) | 1.000 | 1 (1.28) | 0.528 | 1 (1.27) | 0.533 |
| Health-Related Activities | |||||||||
| Exercise | 204 (81.9) | 39 (83.0) | 1.000 | 42 (82.4) | 1.000 | 65 (83.3) | 0.832 | 64 (81.0) | 0.937 |
| Plant-picking | 99 (39.6) | 22 (46.8) | 0.339 ** | 20 (39.2) | 1.000 | 30 (38.5) | 0.914 | 28 (35.4) | 0.439 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romanillos, T.; Maneja, R.; Varga, D.; Badiella, L.; Boada, M. Protected Natural Areas: In Sickness and in Health. Int. J. Environ. Res. Public Health 2018, 15, 2182. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15102182
Romanillos T, Maneja R, Varga D, Badiella L, Boada M. Protected Natural Areas: In Sickness and in Health. International Journal of Environmental Research and Public Health. 2018; 15(10):2182. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15102182
Chicago/Turabian StyleRomanillos, Teresa, Roser Maneja, Diego Varga, Llorenç Badiella, and Martí Boada. 2018. "Protected Natural Areas: In Sickness and in Health" International Journal of Environmental Research and Public Health 15, no. 10: 2182. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15102182