Translation and Validation of the Malay Version of the Parents’ Satisfaction Scale (PSS-M) for Assessment of Caregivers’ Satisfaction with Health Care Services for Children with Autism Spectrum Disorder


 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting and Participants
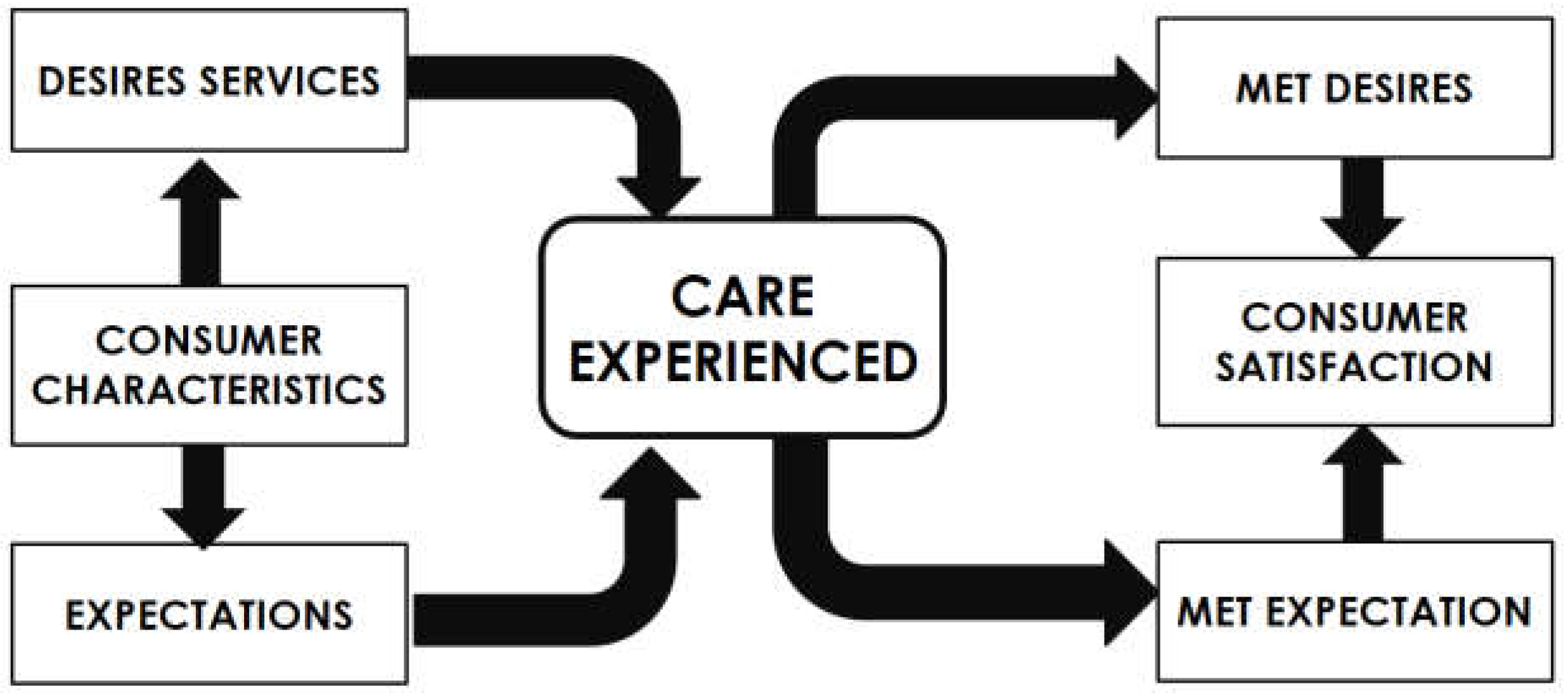
2.2. Parent Satisfaction Scale (PSS)
- (1)
- Preparation
- (2)
- Forward Translation
- (3)
- Reconciliation
- (4)
- Back Translation
- (5)
- Back Translation Review
- (6)
- Harmonisation
- (7)
- Cognitive Debriefing
- (8)
- Review of Cognitive Debriefing Results and Finalisation
- (9)
- Proof-Reading
- (10)
- Final Report
Pre-Testing of Parent Satisfaction Scale Questionnaire
2.3. Statistical Analysis
2.4. Ethical Consideration
3. Results
3.1. Socio-Demographic Characteristics of the Caregivers
3.2. Socio-Demographic Characteristics of the Children with ASD
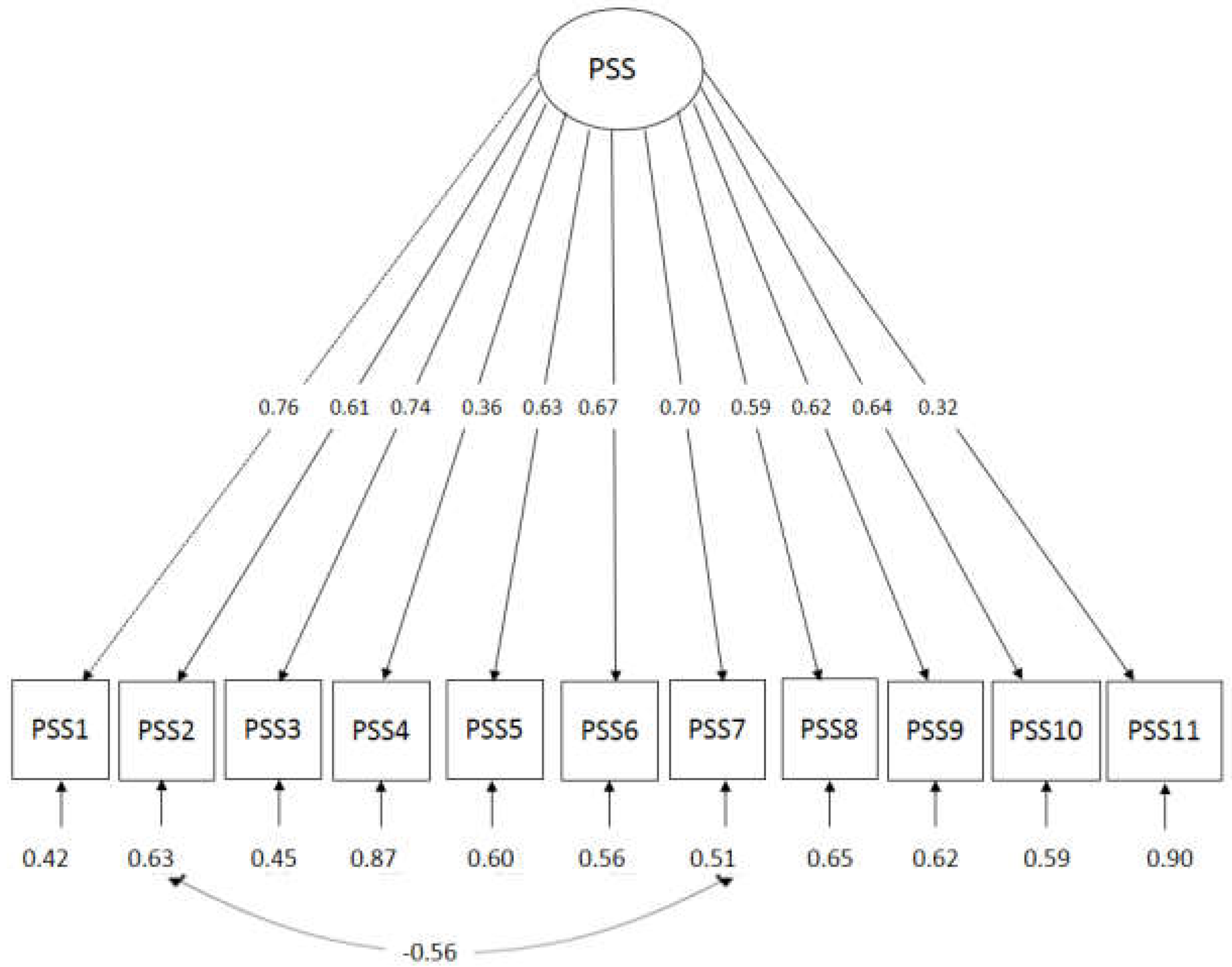
3.3. Confirmatory Factor Analysis of PSS at Specialist Centre
4. Discussion
Limitation of the Study
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Oberst, M.T. Patients’ perceptions of care: Measurement of quality and satisfaction. Cancer 1984, 53, 2366–2373. [Google Scholar] [CrossRef] [PubMed]
- Russell, S.; McCloskey, C.R. Parent perceptions of care received by children with an autism spectrum disorder. J. Pediatr. Nurs. 2016, 31, 21–31. [Google Scholar] [CrossRef] [PubMed]
- Klettlinger, D.; Wirfel, L.; Bielak, B. Caregiver Perceptions of Healthcare Providers and Environments Related to Children with Autism Spectrum Disorder; University of Akron: Akron, OH, USA, 2015. [Google Scholar]
- Moh, T.A.; Magiati, I. Factors associated with parental stress and satisfaction during the process of diagnosis of children with autism spectrum disorders. Res. Autism Spectr. Disord. 2012, 6, 293–303. [Google Scholar] [CrossRef]
- Rivard, M.; Lépine, A.; Mercier, C.; Morin, M. Quality Determinants of Services for Parents of Young Children with Autism Spectrum Disorders. J. Child Fam. Stud. 2015, 24, 2388–2397. [Google Scholar] [CrossRef]
- Robert, M.; Leblanc, L.; Boyer, T. When satisfaction is not directly related to the support services received: Understanding parents’ varied experiences with specialised services for children with developmental disabilities. Br. J. Learn. Disabil. 2015, 43, 168–177. [Google Scholar] [CrossRef]
- APA. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; APA: Washington, DC, USA, 2013. [Google Scholar]
- MOH. Management of Autism Spectrum Disorder in Children and Adolescents; Ministry of Health, Malaysian Psychiatry Association, Academy of Medicine Malaysia: Kuala Lumpur, Malaysia, 2014.
- Pascoe, G.C. Patient satisfaction in primary health care: A literature review and analysis. Eval. Program Plan. 1983, 6, 185–210. [Google Scholar] [CrossRef]
- Gerkensmeyer, J.E.; Austin, J.K. Development and testing of a scale measuring parent satisfaction with staff interactions. J. Behav. Health Serv. Res. 2005, 32, 61–73. [Google Scholar] [CrossRef] [PubMed]
- Gerkensmeyer, J.E. Examining Parent Satisfaction with Services for Children and Adolescents with Mental Health Problems. Ph.D. Thesis, Indiana University, Bloomington, IN, USA, 1999. [Google Scholar]
- Braiden, H.-J.; Bothwell, J.; Duffy, J. Parents’ experience of the diagnostic process for autistic spectrum disorders. Child Care Pract. 2010, 16, 377–389. [Google Scholar] [CrossRef]
- Chiri, G.; Warfield, M.E. Unmet need and problems accessing core health care services for children with autism spectrum disorder. Matern. Child Health J. 2012, 16, 1081–1091. [Google Scholar] [CrossRef] [PubMed]
- Karst, J.S.; Van Hecke, A.V. Parent and family impact of autism spectrum disorders: A review and proposed model for intervention evaluation. Clin. Child Fam. Psychol. Rev. 2012, 15, 247–277. [Google Scholar] [CrossRef] [PubMed]
- Muskat, B.; Greenblatt, A.; Nicholas, D.B.; Ratnapalan, S.; Cohen-Silver, J.; Newton, A.S.; Craig, W.R.; Kilmer, C.; Zwaigenbaum, L. Parent and health care provider perspectives related to disclosure of autism spectrum disorder in pediatric emergency departments. Autism 2016, 20, 986–994. [Google Scholar] [CrossRef] [PubMed]
- Daniels, A.M.; Como, A.; Herguner, S.; Kostadinova, K.; Stosic, J.; Shih, A. Autism in Southeast Europe: A Survey of Caregivers of Children with Autism Spectrum Disorders. J. Autism Dev. Disord. 2017, 47, 2314–2325. [Google Scholar] [CrossRef] [PubMed]
- Siklos, S.; Kerns, K.A. Assessing the diagnostic experiences of a small sample of parents of children with autism spectrum disorders. Res. Dev. Disabil. 2007, 28, 9–22. [Google Scholar] [CrossRef] [PubMed]
- MOH. Autism Spectrum Disorder Research in Malaysia; Technical Report; Ministry of Health: Kuala Lumpur, Malaysia, 2015.
- MOH. Malaysia Health System Performance; Ministry of Health: Kuala Lumpur, Malaysia, 2017.
- Almeida, R.S.D.; Bourliataux-Lajoinie, S.; Martins, M. Satisfaction measurement instruments for healthcare service users: A systematic review. Cad. Saude Publica 2015, 31, 11–25. [Google Scholar] [CrossRef]
- Martinez, S.M.; Ainsworth, B.E.; Elder, J.P. A review of physical activity measures used among US Latinos: Guidelines for developing culturally appropriate measures. Ann. Behav. Med. 2008, 36, 195–207. [Google Scholar] [CrossRef] [PubMed]
- Wild, D.; Grove, A.; Martin, M.; Eremenco, S.; McElroy, S.; Verjee-Lorenz, A.; Erikson, P. Principles of good practice for the translation and cultural adaptation process for patient-reported outcomes (PRO) measures: Report of the ISPOR task force for translation and cultural adaptation. Value Health 2005, 8, 94–104. [Google Scholar] [CrossRef] [PubMed]
- Hair, J.F., Jr.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis, 7th ed.; Prentice Hall: Upper Saddle River, NJ, USA, 2009; Volume 761. [Google Scholar]
- Palad, Y.Y.; Madriaga, G.O. Reliability of the Filipino version of the Parent Satisfaction Scale: A preliminary study. Hong Kong Physiother. J. 2014, 32, 73–78. [Google Scholar] [CrossRef]
- Cook, D.A.; Beckman, T.J. Current concepts in validity and reliability for psychometric instruments: Theory and application. Am. J. Med. 2006, 119, 166. e7–166. e16. [Google Scholar] [CrossRef] [PubMed]
- Raykov, T. Estimation of congeneric scale reliability using covariance structure analysis with nonlinear constraints. Br. J. Math. Stat. Psychol. 2001, 54, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Pituch, K.A.; Stevens, J.P. Applied Multivariate Statistics for the Social Sciences: Analyses with SAS and IBM’s SPSS; Routledge: Abingdon, UK, 2015. [Google Scholar]
- Schreiber, J.B.; Nora, A.; Stage, F.K.; Barlow, E.A.; King, J. Reporting structural equation modeling and confirmatory factor analysis results: A review. J. Educ. Res. 2006, 99, 323–338. [Google Scholar] [CrossRef]
- Brown, T.A. Confirmatory Factor Analysis for Applied Research; Guilford Publications: New York City, NY, USA, 2014. [Google Scholar]
- Gerkensmeyer, J.E.; Austin, J.K.; Miller, T.K. Model testing: Examining parent satisfaction. Arch. Psychiatr. Nurs. 2006, 20, 65–75. [Google Scholar] [CrossRef] [PubMed]
- Hays, J. People, Population and Languages of Malaysia. Facts and Details. 2015. Available online: http://factsanddetails.com/southeast-asia/Malaysia/sub5_4b/entry-3153.html (accessed on 5 September 2018).
- Quah, C. Issues in the translation of English affixes into Malay. Meta J. Trad./Meta Transl. J. 1999, 44, 604–616. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | N (%) | Mean (SD) |
|---|---|---|
| Age | 38.39 (7.60) | |
| Sex | ||
| Female | 87 (79.1) | |
| Male | 23 (20.9) | |
| Occupation | ||
| Professional | 42 (38.2) | |
| Non-Professional | 35 (31.8) | |
| Housewife/Unemployed | 33 (30.0) | |
| Marital Status | ||
| Single | 10 (9.1) | |
| Married | 100 (90.9) | |
| Main Caregiver | ||
| Mother | 60 (54.5) | |
| Father | 8 (7.3) | |
| Both | 42 (38.2) | |
| Education | ||
| Secondary school and below | 33 (30.0) | |
| Diploma and above | 77 (70.0) | |
| Distance home to tertiary care | ||
| Less than 25 km | 64 (58.0) | |
| 25 km or more | 46 (41.8) | |
| Household income (Ringgit Malaysia; RM) | ||
| ≤RM 2000 | 23 (20.9) | |
| RM 2000 to less than RM 5000 | 49 (44.5) | |
| RM 5000 to less than RM 8000 | 24 (21.8) | |
| ≥RM 8000 | 14 (12.7) | |
| Number of children | 2.96 (1.71) | |
| Availability of transportation | ||
| Yes | 103 (93.6) | |
| No | 7 (6.4) | |
| Problem getting to tertiary care | ||
| Yes | 11 (10.0) | |
| No | 99 (90.0) | |
| Problems in accompanying during appointments | ||
| Yes | 26 (23.6) | |
| No | 84 (76.4) | |
| Medical Problems | ||
| Yes | 3 (2.7) | |
| No | 107 (97.3) |
| Variables | N (%) | Mean (SD) |
|---|---|---|
| Age | 7.39 (3.44) | |
| Gender | ||
| Boy | 95 (86.4) | |
| Girl | 15 (13.6) | |
| Birth Order | 1.88 (1.53) | |
| ASD with comorbidity | ||
| Yes | 66 (60.0) | |
| No | 44 (40.0) | |
| Age of caregiver start concern | 2.36 (1.27) | |
| Caregiver concerns and worries | ||
| Speech delay | ||
| Yes | 105 (95.5) | |
| No | 5 (4.5) | |
| Delay in walking | ||
| Yes | 23 (20.9) | |
| No | 87 (79.1) | |
| Social problem | ||
| Yes | 63 (57.3) | |
| No | 47 (42.7) | |
| Dislikes changes | ||
| Yes | 35 (31.8) | |
| No | 75 (68.2) | |
| Hyperactive child | ||
| Yes | 53 (48.2) | |
| No | 57 (51.8) | |
| Learning disability | ||
| Yes | 55 (50.0) | |
| No | 55 (50.0) | |
| Medical problem | ||
| Yes | 8 (7.3) | |
| No | 102 (92.7) | |
| Hearing Problem | ||
| Yes | 11 (10.0) | |
| No | 99 (90.0) | |
| Hypersensitivity | ||
| Yes | 34 (30.9) | |
| No | 76 (69.1) | |
| Sleeping problem | ||
| Yes | 32 (29.1) | |
| No | 77 (70.0) | |
| No worries | ||
| Yes | 10 (9.1) | |
| No | 100 (90.9) | |
| School | ||
| Not schooling | 21 (19.1) | |
| Government | 38 (34.5) | |
| Non-government | 51 (46.4) | |
| Registered with social welfare | ||
| Yes | 64 (58.2) | |
| No | 46 (41.8) | |
| Age of diagnosis | 5.01 (1.91) | |
| Age when the caregiver first sought help | 3.67 (2.03) |
| Statements | Mean (SD) | n (Percent (%)) | Minimum Maximum | ||||
|---|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 4 | |||
| 1. Overall, I was satisfied with the staff | 3.10 (0.66) | - | 6 (5.5) | 1 (0.9) | 79 (71.8) | 24 (21.8) | 1.4 |
| 2. I was satisfied with the availability of the staff | 3.10 (0.68) | - | 16 (14.5) | - | 64 (58.2) | 38 (16.7) | 1.4 |
| 3. I was satisfied with the way the staff helped me understand my child’s problems | 2.98 (0.93) | - | 16 (14.5) | - | 64 (58.2) | 30 (27.3) | 1.4 |
| 4. I was satisfied with the convenience of appointments with the staff | 2.54 (0.92) | - | 27 (24.5) | 2 (1.8) | 76 (69.1) | 5 (4.5) | 1.4 |
| 5 I was satisfied with the caring and concern the staff showed for my child | 3.07 (0.89) | - | 13 (11.8) | - | 63 (57.3) | 34 (30.9) | 1.4 |
| 6. I was satisfied with how the staff treated me with respect | 3.19 (0.77) | - | 8 (7.3) | - | 65 (59.1) | 37 (33.6) | 1.4 |
| 7. I was satisfied with how the staff listened to what I had to say | 3.03 (0.76) | - | 10 (9.1) | - | 77 (70.0) | 23 (20.9) | 1.4 |
| 8. I was satisfied with how the staff kept me informed about changes in the care of my child. | 2.88 (0.79) | - | 13 (11.8) | 3 (2.7) | 78 (70.9) | 16 (14.5) | 1.4 |
| 9. I was satisfied with how the staff helped me find the services my child needed. | 3.08 (0.77) | - | 9 (8.2) | 1 (0.9) | 72 (65.5) | 28 (25.5) | 1.4 |
| 10. I was satisfied with how the staff included me in decision making about my child’s treatment | 2.98 (0.78) | - | 11 (10.0) | 1 (0.9) | 77 (70.0) | 21 (19.1) | 1.4 |
| 11. I was satisfied with the support I received from the staff. | 2.04 (1.10) | - | 55 (50.0) | 5 (4.5) | 41 (37.3) | 9 (8.2) | 1.4 |
| Total PSS score | 31.99 (5.74) | ||||||
| Model | χ2 (df) | P | χ2diff (df) | P | SRMR | RMSEA | 90% CI | CFI | TLI | AIC | BIC |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Model 1 | 75 (44) | <0.001 | 0.064 | 0.081 | 0.053, 0.108 | 0.90 | 0.87 | 2624 | 2713 | ||
| Model 2 | 52.8 (43) | 0.014 | 61.7 (1) | <0.001 | 0.056 | 0.050 | 0.000, 0.079 | 0.97 | 0.96 | 2598 | 2690 |
| PSS-M Items | Factor Loading | Raykov’s rho | 95% CI |
|---|---|---|---|
| PSS 1 | 0.76 | 0.851 | 0.81, 0.89 |
| PSS 2 | 0.61 | ||
| PSS 3 | 0.74 | ||
| PSS 4 | 0.36 | ||
| PSS 5 | 0.63 | ||
| PSS 6 | 0.67 | ||
| PSS 7 | 0.70 | ||
| PSS 8 | 0.59 | ||
| PSS 9 | 0.62 | ||
| PSS 10 | 0.64 | ||
| PSS 11 | 0.32 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nik Adib, N.A.; Ibrahim, M.I.; Ab Rahman, A.; Bakar, R.S.; Yahaya, N.A.; Hussin, S.; Nor Arifin, W. Translation and Validation of the Malay Version of the Parents’ Satisfaction Scale (PSS-M) for Assessment of Caregivers’ Satisfaction with Health Care Services for Children with Autism Spectrum Disorder. Int. J. Environ. Res. Public Health 2018, 15, 2455. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15112455
Nik Adib NA, Ibrahim MI, Ab Rahman A, Bakar RS, Yahaya NA, Hussin S, Nor Arifin W. Translation and Validation of the Malay Version of the Parents’ Satisfaction Scale (PSS-M) for Assessment of Caregivers’ Satisfaction with Health Care Services for Children with Autism Spectrum Disorder. International Journal of Environmental Research and Public Health. 2018; 15(11):2455. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15112455
Chicago/Turabian StyleNik Adib, Nik Aida, Mohd Ismail Ibrahim, Azriani Ab Rahman, Raishan Shafini Bakar, Nor Azni Yahaya, Suria Hussin, and Wan Nor Arifin. 2018. "Translation and Validation of the Malay Version of the Parents’ Satisfaction Scale (PSS-M) for Assessment of Caregivers’ Satisfaction with Health Care Services for Children with Autism Spectrum Disorder" International Journal of Environmental Research and Public Health 15, no. 11: 2455. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15112455