A Theoretical and Empirical Linkage between Road Accidents and Binge Eating Behaviors in Adolescence

 ,
,
Abstract
:1. Introduction
1.1. Binge Eating Behaviors (BEbs) and Motor Vehicle Collisions in Adolescence
1.2. The Present Study
2. Method and Measures
2.1. Study Design and Setting
2.2. Measures
2.2.1. Emotional and Behavioral Assessment
2.2.2. Alexithymia
2.2.3. Impulsivity
2.2.4. Binge Eating Behaviors
2.2.5. Motor Vehicle Collisions
2.2.6. Statistical Analyses
3. Results
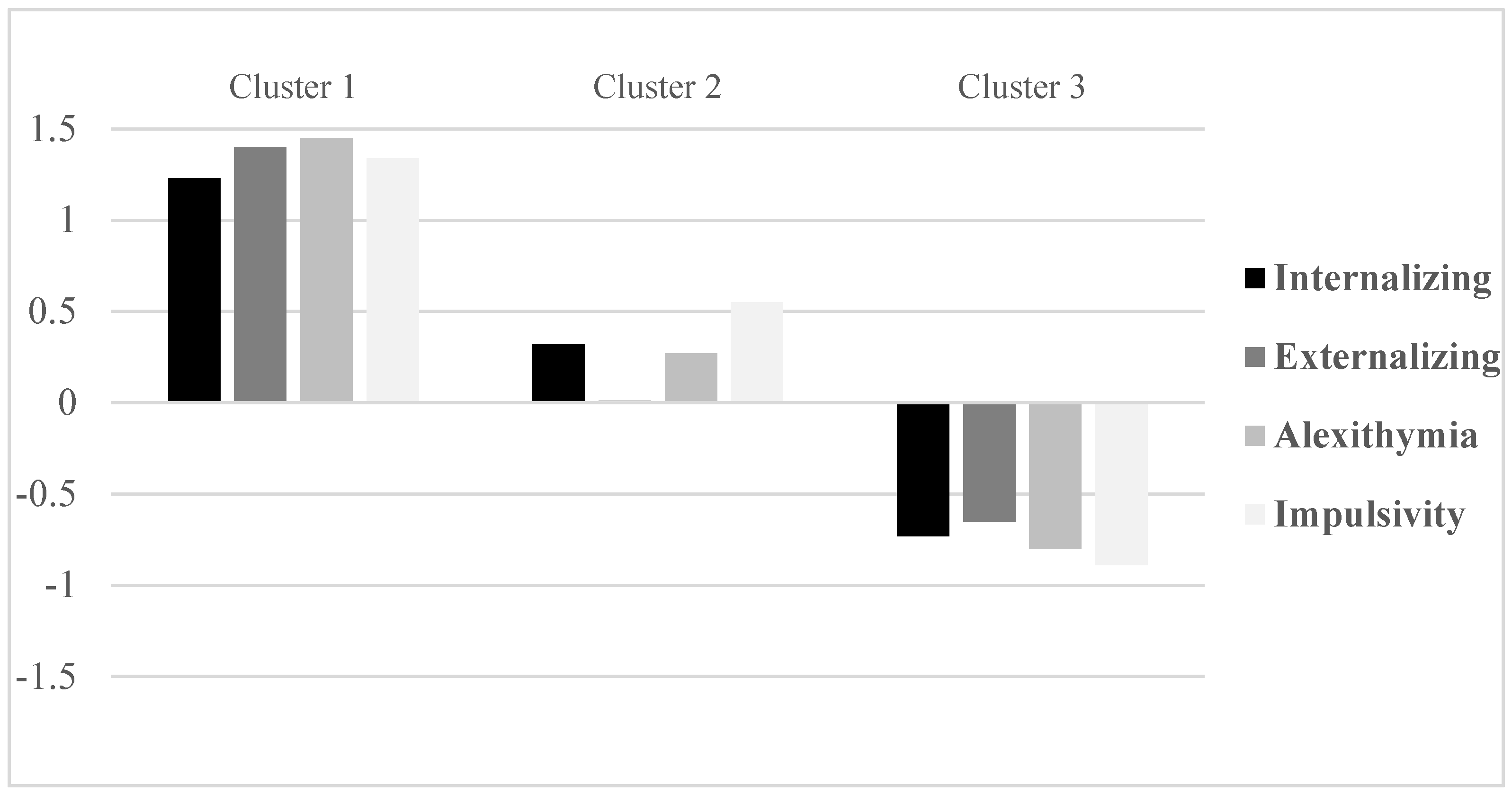
3.1. Clusters of Maladaptive Emotional–Behavioral Functioning in MVC Adolescents
3.2. Prevalence of Clinical BEbs and MVCs in the Three Clusters
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Mitchell, J.E.; Myers, T.; Crosby, R.; O’Neill, G.; Carlisle, J.; Gerlach, S. Health care utilization in patients with eating disorders. Int. J. Eat. Disord. 2009, 42, 571–574. [Google Scholar] [CrossRef] [PubMed]
- Day, A.J.; Brasher, K.; Bridger, R.S. Accident proneness revisited: The role of psychological stress and cognitive failure. Accid. Anal. Prev. 2012, 49, 532–535. [Google Scholar] [CrossRef] [PubMed]
- Cameron, C.M.; Purdie, D.M.; Kliewer, E.V.; McClure, R.J. Long-term mortality following trauma: 10 year follow-up in a population-based sample of injured adults. J. Trauma 2005, 59, 639–646. [Google Scholar] [PubMed]
- Blakemore, S.J. Imaging brain development: The adolescent brain. Neuroimage 2012, 61, 397–406. [Google Scholar] [CrossRef] [PubMed]
- Capobianco, M.; Pizzuto, E.A.; Devescovi, A. Gesture–speech combinations and early verbal abilities. Interact. Stud. 2017, 18, 55–76. [Google Scholar] [CrossRef]
- Kullik, A.; Petermann, F. Attachment to parents and peers as a risk factor for adolescent depressive disorders: The mediating role of emotion regulation. Child Psychiatry Hum. Dev. 2013, 44, 537–548. [Google Scholar] [CrossRef] [PubMed]
- Paciello, M.; Fida, R.; Cerniglia, L.; Tramontano, C.; Cole, E. High cost helping scenario: The role of empathy, prosocial reasoning and moral disengagement on helping behavior. Personal. Individ. Differ. 2013, 55, 3–7. [Google Scholar] [CrossRef]
- Paciello, M.; Fida, R.; Tramontano, C.; Cole, E.; Cerniglia, L. Moral dilemma in adolescence: The role of values, prosocial moral reasoning and moral disengagement in helping decision making. Eur. J. Dev. Psychol. 2013, 10, 190–205. [Google Scholar] [CrossRef]
- Giedd, J.N. The teen brain: Insights from neuroimaging. J. Adolesc. Health 2008, 42, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Paus, T.; Keshavan, M.; Giedd, J.N. Why do many psychiatric disorders emerge during adolescence? Nat. Rev. Neurosci. 2008, 9, 947–957. [Google Scholar] [CrossRef] [PubMed]
- Poletti, M. Neurocognitive functioning in borderline personality disorder. Riv. Psichiatr. 2009, 44, 374–383. [Google Scholar] [PubMed]
- Preti, A.; de Girolamo, G.; Vilagut, G.; Alonso, J.; Graaf, R.; Bruffaerts, R.; Demyttenaere, K.; Pinto-Meza, A.; Haro, J.M.; Morosini, P.; ESEMeD-WMH Investigators. The epidemiology of eating disorders in six European countries: Results of the ESEMeD-WMH project. J. Psychiatr. Res. 2009, 43, 1125–1132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hilbert, A.; Pike, K.M.; Wilfley, D.E.; Fairburn, C.G.; Dohm, F.A.; Striegel-Moore, R.H. Clarifying boundaries of binge eating disorder and psychiatric comorbidity: A latent structure analysis. Behav. Res. Ther. 2011, 49, 202–211. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Shahly, V.; Hudson, J.I.; Supina, D.; Berglund, P.A.; Chiu, W.T.; Gruber, M.; Aguilar-Gaxiola, S.; Alonso, J.; Andrade, L.H.; et al. A comparative analysis of role attainment and impairment in binge-eating disorder and bulimia nervosa: Results from the WHO World Mental Health Surveys. Epidemiol. Psychiatr. Sci. 2014, 23, 27–41. [Google Scholar] [CrossRef] [PubMed]
- Bryant-Waugh, R.; Markham, L.; Kreipe, R.E.; Walsh, B.T. Feeding and eating disorders in childhood. Int. J. Eat. Disord. 2010, 43, 98–111. [Google Scholar] [CrossRef] [PubMed]
- Babore, A.; Trumello, C.; Candelori, C.; Paciello, M.; Cerniglia, L. Depressive symptoms, self-esteem and perceived parent-child relationship in early adolescence. Front. Psychol. 2016, 7, 982. [Google Scholar] [CrossRef] [PubMed]
- Cimino, S.; Cerniglia, L.; Carlos, A.; Jezek, S.; Erriu, M.; Tambelli, R. Developmental trajectories of body mass index and emotional behavioral functioning of underweight children: A longitudinal study. Sci. Rep. 2016, 6, 20211. [Google Scholar] [CrossRef] [PubMed]
- Dooley-Hash, S.; Banker, J.D.; Walton, M.A.; Ginsburg, Y.; Cunningham, R.M. The prevalence and correlates of eating disorders among emergency department patients aged 14–20 years. Int. J. Eat. Disord. 2012, 45, 883–890. [Google Scholar] [CrossRef] [PubMed]
- Cerniglia, L.; Cimino, S.; Ballarotto, G.; Monniello, G. Parental loss during childhood and outcomes on adolescents’ psychological profiles: A longitudinal study. Curr. Psychol. 2014, 33, 545–556. [Google Scholar] [CrossRef]
- Smink, F.R.E.; van Hoeken, D.; Hoek, H.W. Epidemiology of eating disorders: Incidence, prevalence and mortality rates. Curr. Psychiatry Rep. 2012, 14, 406–414. [Google Scholar] [CrossRef] [PubMed]
- Swanson, S.A.; Crow, S.J.; Le Grange, D.; Swendsen, J.; Merikangas, K.R. Prevalence and correlates of eating disorders in adolescents. Results from the national comorbidity survey replication adolescent supplement. Arch. Gen. Psychiatry 2011, 68, 714–723. [Google Scholar] [CrossRef] [PubMed]
- Dooley-Hash, S.; Lipson, S.K.; Walton, M.A.; Cunningham, R.M. Increased emergency department use by adolescents and young adults with eating disorders. Int. J. Eat. Disord. 2013, 46, 308–315. [Google Scholar] [CrossRef] [PubMed]
- Cerniglia, L.; Cimino, S.; Ballarotto, G.; Casini, E.; Ferrari, A.; Carbone, P.; Cersosimo, M. Motor vehicle accidents and adolescents: An empirical study on their emotional and behavioral profiles, defense strategies and parental support. Transp. Res. Part F Traffic Psychol. Behav. 2015, 35. [Google Scholar] [CrossRef]
- Sarma, K.M.; Carey, R.N.; Kervick, A.A.; Bimpeh, Y. Psychological factors associated with indices of risky, reckless and cautious driving in a national sample of drivers in the Republic of Ireland. Accid. Anal. Prev. 2013, 50, 1226–1235. [Google Scholar] [CrossRef] [PubMed]
- Marengo, D.; Settanni, M.; Vidotto, G.; Ciairano, S. Profili di personalità e rischio stradale in adolescenza: uno studio longitudinale in ambiente simulato e reale. Ricerche di Psicologia 2012, 1, 33–61. [Google Scholar] [CrossRef]
- Henderson, A.F.; Joseph, A.P. Motor vehicle accident or driver suicide? Identifying cases of failed driver suicide in the trauma setting. Injury 2012, 43, 18–21. [Google Scholar] [CrossRef] [PubMed]
- Mann, R.E.; Asbridge, M.; Stoduto, G.; Smart, R.G.; Goldbloom, D.S.; Vingilis, E.R.; Wickens, C.M. Psychological distress and collision involvement among adult drivers. Stress Health 2010, 26, 127–134. [Google Scholar] [CrossRef]
- Corstorphine, E.; Waller, G.; Lawson, R.; Ganis, G. Trauma and multi-impulsivity in the eating disorders. Eat. Behav. 2007, 8, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Frank, G.K. Altered brain reward circuits in eating disorders: chicken or egg? Curr. Psychiatry Rep. 2013, 15, 396. [Google Scholar] [CrossRef] [PubMed]
- Brockmeyer, T.; Skunde, M.; Wu, M.; Bresslein, E.; Rudofsky, G.; Herzog, W.; Friederich, H.C. Difficulties in emotion regulation across the spectrum of eating disorders. Compr. Psychiatry 2014, 55, 565–571. [Google Scholar] [CrossRef] [PubMed]
- Danner, U.N.; Ouwehand, C.; van Haastert, N.L.; Hornsveld, H.; Ridder, D.T. Decision-making impairments in women with binge eating disorder in comparison with obese and normal weight women. Eur. Eat. Disord. Rev. 2012, 20, e56–e62. [Google Scholar] [CrossRef] [PubMed]
- Campbell, K.; Peebles, R. Eating Disorders in Children and Adolescents: State of the Art Review. Pediatrics 2014, 134, 582–592. [Google Scholar] [CrossRef] [PubMed]
- Young, M.S.; Mahfoud, J.M.; Walker, G.H.; Jenkins, D.P.; Stanton, N.A. Crash dieting: The effects of eating and drinking on driving performance. Accid. Anal. Prev. 2008, 40, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Bina, M.; Graziano, F.; Bonino, S. Risky driving and lifestyles in adolescence. Accid. Anal. Prev. 2006, 38, 472–481. [Google Scholar] [CrossRef] [PubMed]
- Grucza, R.A.; Prybeck, T.R.; Cloninger, C.R. Prevalence and correlates of binge eating disorder in a community sample. Compr. Psychiatry. 2007, 48, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Herzog, D.B.; Dorer, D.J.; Keel, P.K.; Selwyn, S.E.; Ekeblad, E.R.; Flores, A.T.; Greenwood, D.N.; Burwell, R.A.; Keller, M.B. Recovery and relapse in anorexia and bulimia nervosa: A 7.5-year follow-up study. J. Am. Acad. Child Adolesc. Psychiatry. 1999, 38, 829–837. [Google Scholar] [CrossRef] [PubMed]
- Van Son, G.E.; van Hoeken, D.; van Furth, E.F.; Donker, G.A.; Hoek, H.W. Course and outcome of eating disorders in a primary care-based cohort. Int. J. Eat. Disord. 2010, 43, 130–138. [Google Scholar] [CrossRef] [PubMed]
- Linville, D.; Cobb, E.; Lenee-Bluhm, T.; López-Zerón, G.; Gau, J.M.; Stice, E. Effectiveness of an eating disorder preventative intervention in primary care medical settings. Behav. Res. Ther. 2015, 75, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Bornstein, M.H.; Bradley, R.H. Socioeconomic Status, Parenting, and Child Development; Routledge: London, UK, 2014. [Google Scholar]
- Achenbach, T.M.; Rescorla, L.A. The Achenbach System of Empirically Based Assessment (ASEBA) for ages 1.5 to 18 years. In The Use of Psychological Testing for Treatment Planning and Outcomes Assessment, 3rd ed.; Maruish, M.R., Ed.; Erlbaum: Mahwah, Burlington, VT, USA, 2004; pp. 179–213. [Google Scholar]
- Frigerio, A.; Montirosso, R. La valutazione su base empirica dei problemi emotivo-comportamentali in età evolutiva. Infanzia e adolescenza 2002, 1, 38–48. [Google Scholar]
- Bagby, R.M.; Parker, J.D.A.; Taylor, G.J. The twenty-item Toronto Alexithymia scale-I. Item selection and cross-validation of the factor structure. J. Psychosom. Res. 1994, 38, 23–32. [Google Scholar] [CrossRef]
- La Ferlita, V.; Bonadies, M.; Solano, L.; de Gennaro, L.; Gonini, P. Alessitimia e adolescenza: Studio preliminare di validazione della TAS-20 su un campione di 360 adolescenti italiani. Infanzia Adolescenza 2007, 6, 131–144. [Google Scholar]
- Parker, J.D.; Bagby, R.M.; Taylor, G.J.; Endler, N.S.; Schmitz, P. Factorial validity of the 20-item Toronto Alexithymia Scale. Eur. J. Pers. 1993, 7, 221–232. [Google Scholar] [CrossRef]
- Patton, J.H.; Stanford, M.S.; Barratt, E.S. Factor structure of the Barratt impulsiveness scale. J. Clin. Psychol. 1995, 51, 768–774. [Google Scholar] [CrossRef]
- Vasconcelos, A.G.; Malloy-Diniz, L.; Correa, H. Systematic review of psychometric proprieties of Barratt impulsiveness scale version 11 (BIS-11). Clin. Neuropsychiatry 2012, 9, 61–74. [Google Scholar]
- Fossati, A.; Di Ceglie, A.; Acquarini, E.; Barratt, E.S. Psychometric properties of an Italian version of the Barratt Impulsiveness Scale-11 (BIS-11) in nonclinical subjects. J. Clin. Psychol. 2001, 57, 815–828. [Google Scholar] [CrossRef] [PubMed]
- Gormally, J.; Black, S.; Daston, S.; Rardin, D. The assessment of binge eating severity among obese persons. Addict. Behav. 1982, 7, 47–55. [Google Scholar] [CrossRef]
- Di Bernardo, M.; Barciulli, E.; Ricca, V.; Mannucci, E.; Moretti, S.; Cabras, P.L.; Rotella, C.M. Validazione della versione italiana della Binge Eating Scale in pazienti obesi. Minerva Psichiatr. 1998, 39, 125–130. [Google Scholar]
- Dalle Grave, R.; Calugi, S.; Petroni, M.L.; Di Domizio, S.; Marchesini, G.; QUOVADIS Study Group. Weight management, psychological distress and binge eating in obesity. A reappraisal of the problem. Appetite 2010, 54, 269–273. [Google Scholar] [CrossRef] [PubMed]
- Greeno, C.G.; Marcus, M.D.; Wing, R.R. Diagnosis of binge eating disorder: Discrepancies between a questionnaire and clinical interview. Int. J. Eat. Disord. 1995, 17, 153–160. [Google Scholar] [CrossRef]
- Grupski, A.E.; Hood, M.M.; Hall, B.J.; Azarbad, L.; Corsica, J. Utility of the binge eating scale in screening for binge eating disorder with bariatric surgery candidates. Obes. Surg. 2013, 23, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Marcelli, D.; Ingrand, P.; Ingrand, I.; Delamour, M. Échelle d’évaluation du risque de récidive (ecarr). Étude de validation prospective d’une répétition d’accident. La psychiatrie de l’enfant 2011, 54, 253–299. [Google Scholar] [CrossRef]
- Murray, J.; Ehlers, A.; Mayou, R.A. Dissociation and post-traumatic stress disorder: Two prospective studies of road traffic accident survivors. Br. J. Psychiatry 2002, 180, 363–368. [Google Scholar] [CrossRef] [PubMed]
- Cicchetti, D.; Cohen, D.J. Developmental Psychopathology, Vol 3: Risk, Disorder, and Adaptation, 2nd ed.; Wiley: New York, NY, USA, 2006. [Google Scholar]
- Towner, E.; Dowswell, T. Community-based childhood injury prevention interventions: What works? Health Promot. Int. 2002, 17, 273–284. [Google Scholar] [CrossRef] [PubMed]
- Carli, V.; Hoven, C.W.; Wasserman, C.; Chiesa, F.; Guffanti, G.; Sarchiapone, M. A newly identified group of adolescents at “invisible” risk for psychopathology and suicidal behavior: Findings from the SEYLE study. World Psychiatry 2014, 13, 78–86. [Google Scholar] [CrossRef] [PubMed]
- Heatherton, T.F.; Baumeister, R.F. Binge eating as escape from self-awareness. Psychol. Bull. 1991, 110, 86–108. [Google Scholar] [CrossRef] [PubMed]
- Laghi, F.; Liga, F.; Baumgartner, E.; Baiocco, R. Time perspective and psychosocial positive functioning among Italian adolescents who binge eat and drink. J. Adolesc. 2012, 35, 1277–1284. [Google Scholar] [CrossRef] [PubMed]
- Cimino, S.; Cerniglia, L.; Paciello, M.; Sinesi, S. A six-year prospective study on children of mothers with eating disorders: The role of paternal psychological profiles. Eur. Eat. Disord. Rev. 2013, 21, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Brewer, R.; Cook, R.; Cardi, V.; Treasure, J.; Bird, G. Emotion recognition deficits in eating disorders are explained by co-occurring alexithymia. R. Soc. Open Sci. 2015, 2, 140382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mond, J.M.; Myers, T.C.; Crosby, R.D.; Hay, P.J.; Mitchell, J.E. Bulimic eating disorders in primary care: Hidden morbidity still? J. Clin. Psychol. Med. Settings 2010, 17, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Cimino, S.; Cerniglia, L.; Porreca, A.; Simonelli, A.; Ronconi, L.; Ballarotto, G. Mothers and fathers with binge eating disorder and their 18-36 months old children: A longitudinal study on parent-infant interactions and offspring’s emotional-behavioral profiles. Front. Psychol. 2016, 7, 580. [Google Scholar] [CrossRef] [PubMed]
- Bingham, C.R.; Shope, J.T. Adolescent developmental antecedents of risky driving among young adults. J. Stud. Alcohol 2004, 65, 84–94. [Google Scholar] [CrossRef] [PubMed]
- Taubman-Ben-Ari, O.; Katz-Ben-Ami, L. Family climate for road safety: A new concept and measure. Accid. Anal. Prev. 2013, 54, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Lumley, M.A.; Norman, S. Alexithymia and health care utilization. Psychosom. Med. 1996, 58, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Hoytema van Konijnenburg, E.M.M.; Lee, J.H.; Teeuw, A.H.; Lindeboom, R.; Brilleslijper-Kater, S.N.; Sieswerda-Hoogendoorn, T.; van Goudoever, J.B.; Lindauer, R.J.L. Psychosocial problems of children whose parents visit the emergency department due to intimate partner violence, substance abuse or a suicide attempt. Child Care Health Dev. 2017, 43, 369–384. [Google Scholar] [CrossRef] [PubMed]
- Babeva, K.; Hughes, J.L.; Asarnow, J. Emergency department screening for suicide and mental health risk. Curr. Psychiatry Rep. 2016, 18, 100. [Google Scholar] [CrossRef] [PubMed]
- Whitaker, R.C.; Wright, J.A.; Pepe, M.S.; Seidel, K.D.; Dietz, W.H. Predicting obesity in young adulthood from childhood and parental obesity. N. Engl. J. Med. 1997, 337, 869–873. [Google Scholar] [CrossRef] [PubMed]
- Capobianco, M.; Riccio, G.; Devescovi, A. Early communicative and language development in preterm infants without neurological damage. J. Appl. Res. Intellect. Disabil. 2010, 23, 513. [Google Scholar]


{kind=link}
| Dimensions | Cluster 1 | Cluster 2 | Cluster 3 | Cut-Off Score (Rounded) | Cluster 1 | Cluster 2 | Cluster 3 | |||
|---|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | |||||
| Internalizing | 37.00 | 4.89 | 27.15 | 8.31 | 15.73 | 5.98 | 39.93 (40) | 20% | 5% | 0% |
| Externalizing | 26.22 | 3.04 | 16.32 | 6.20 | 11.67 | 2.99 | 26.90 (27) | 38% | 5% | 0% |
| Alexithymia | 65.19 | 4.85 | 46.73 | 8.34 | 30.02 | 5.47 | 65.91 (66) | 35% | 0% | 0% |
| Impulsivity | 98.70 | 8.19 | 81.51 | 6.69 | 50.19 | 5.75 | 98.13 (98) | 21.6% | 0% | 0% |
| Cluster | NO % (N) | YES % (N) | Total % (N) |
|---|---|---|---|
| 1 | 0 (0) | 100 (37) | 100 (37) |
| 2 | 0 (0) | 100 (41) | 100 (41) |
| 3 | 100 (81) | 0 (0) | 0 (0) |
| Total % (N) | 50.94 (81) | 49.06 (78) | 100 (159) |
| Cluster | Number of Past Accidents | ||
|---|---|---|---|
| ≥4% (N) | =3% (N) | 1 or 2% (N) | |
| 1 | 97.30 (36) | 2.70 (1) | 0 (0) |
| 2 | 4.88 (2) | 53.66 (22) | 41.46 (17) |
| 3 | 12.35 (10) | 32.10 (26) | 55.56 (45) |
| Total % (N) | 30.19 (48) | 30.82 (49) | 38.99 (62) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cimino, S.; Simonelli, A.; Parolin, M.; Ballarotto, G.; Carbone, P.; Cerniglia, L. A Theoretical and Empirical Linkage between Road Accidents and Binge Eating Behaviors in Adolescence. Int. J. Environ. Res. Public Health 2018, 15, 355. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15020355
Cimino S, Simonelli A, Parolin M, Ballarotto G, Carbone P, Cerniglia L. A Theoretical and Empirical Linkage between Road Accidents and Binge Eating Behaviors in Adolescence. International Journal of Environmental Research and Public Health. 2018; 15(2):355. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15020355
Chicago/Turabian StyleCimino, Silvia, Alessandra Simonelli, Micol Parolin, Giulia Ballarotto, Paola Carbone, and Luca Cerniglia. 2018. "A Theoretical and Empirical Linkage between Road Accidents and Binge Eating Behaviors in Adolescence" International Journal of Environmental Research and Public Health 15, no. 2: 355. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15020355