PALTEM: What Parameters Should Be Collected in Disaster Settings to Assess the Long-Term Outcomes of Famine?


Abstract
:1. Introduction
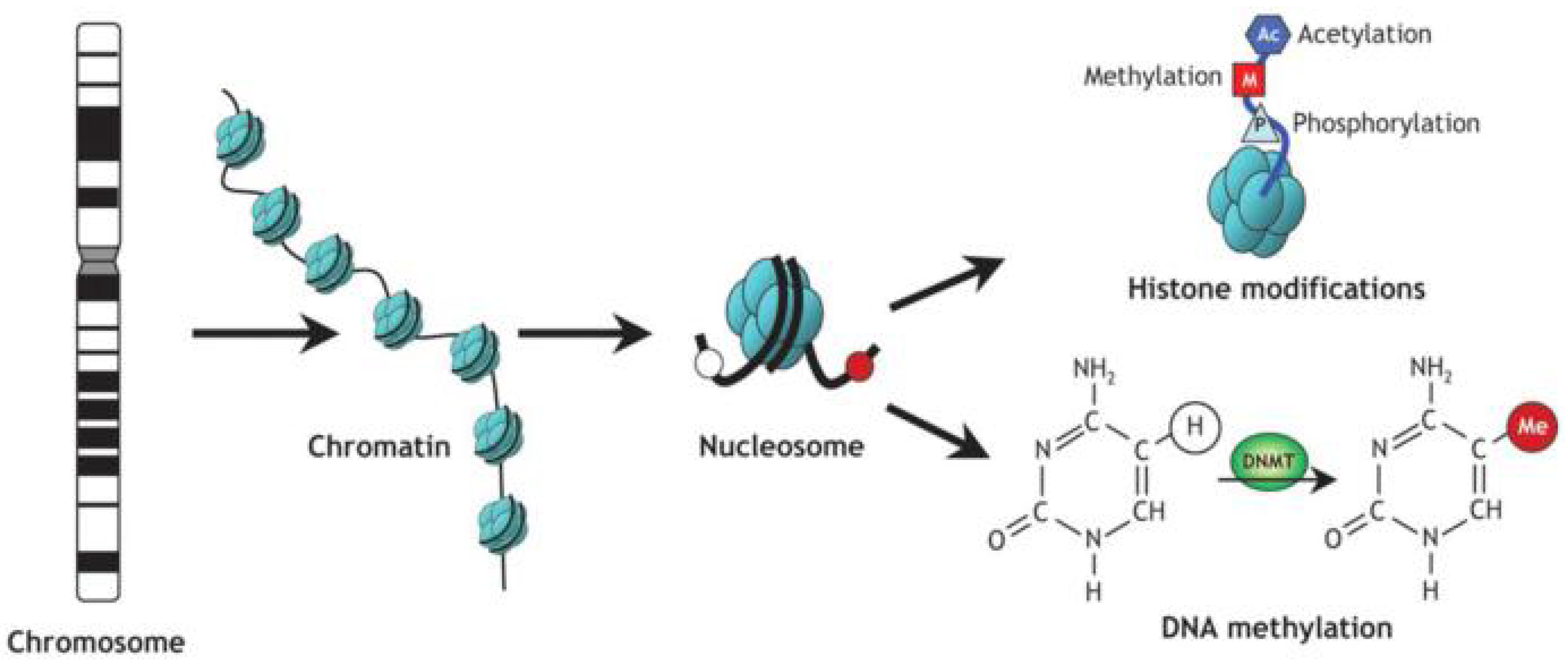
1.1. Epigenetic Mechanisms
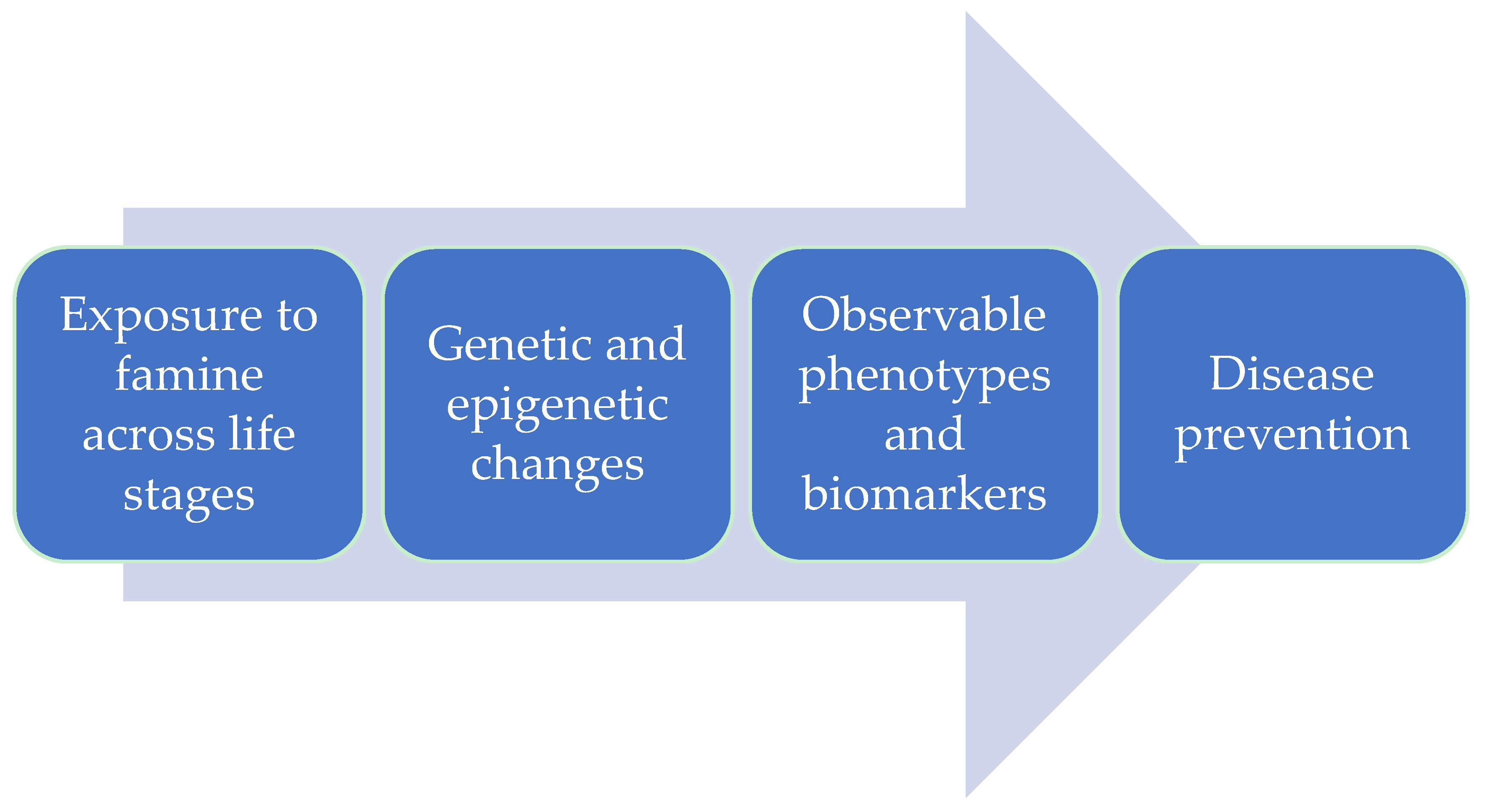
1.2. Epigenetics and Environmental Exposure to Famine
2. Materials and Methods
2.1. Identifying the Research Question
2.2. Finding Relevant Studies
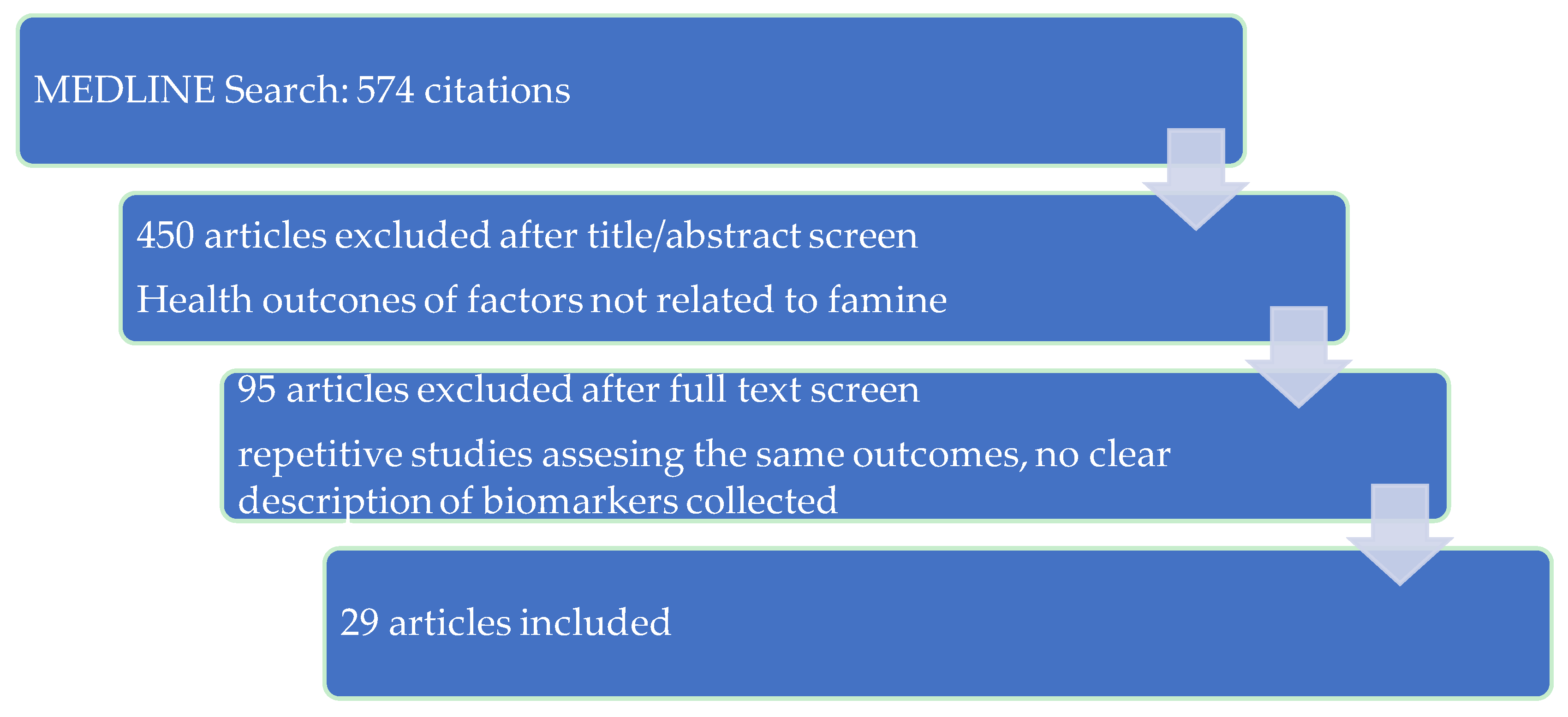
2.3. Selecting the Studies
2.4. Charting the Information
2.5. Summarizing the Results
3. Results
3.1. Common Health Outcomes
3.2. Metabolic Outcomes
3.3. Cardiovascular Disease
3.4. Respiratory Disease
3.5. Reproductive Outcomes
3.6. Neuropsychiatric Outcomes
3.7. Oncologic Outcomes
3.8. Others
3.9. Proposed Parameters
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
Appendix A
Appendix A.1. The Dutch Famine Birth Cohort
Appendix A.2. The Holocaust Survivors
Appendix A.3. The China’s Great Famine
Appendix A.4. The Siege of Leningrad
Appendix A.5. The Överkalix Study
Appendix A.6. The Biafran Study
Appendix B

{kind=link}
{kind=link}
{kind=link}
| First Author, Year | Cohort Description | Aim of Study | Collected Variables and Parameters | Outcomes and Effect Size |
|---|---|---|---|---|
| The Dutch Famine Birth Cohort | ||||
| Stein, 1975 [63] | Seven cohorts of unequal size, based on the criterion of stage of gestation in relation to famine exposure: August–October 1944 (conceived and born before famine); November–January 1944–1945 (exposed at the third semester); Februar–April 1945 (exposed at the second and third trimester); May–June 1945 (exposed to famine during the middle 6 months of gestation); July–September 1945 (exposed during first and second trimester of gestation); October–January 1945–1946 (exposed during the first semester); Februar–March 1946 (conceived and born after the famine). | To study the effects of famine during pregnancy on six indices at birth of the newborns. | Independent variables:
|
|
| Lopuhaa, 2000 [30] | Five cohorts of unequal size, based on the criterion of stage of gestation in relation to famine exposure: 264 born before famine 1 November 1943 to 6 January 1945); 140 exposed to famine in late gestation 29 April 1945 to 18 August 1945); 137 exposed to famine in mid gestation (29 April 1945 to 18 August 1945); 87 exposed to famine in early gestation (19 August 1945 to 8 December 1945); 284 conceived after famine (9 December 1945 to 28 February 1947 ). | To study the effects of famine during pregnancy on the prevalence of the obstructive airways disease and atopy in the first generation. | Independent variables:
|
|
| Roseboom, 2000 [64] | Five cohorts of unequal size, based on the criterion of stage of gestation in relation to famine exposure: 264 born before famine (1 November 1943 to 6 January 1945); 140 exposed to famine in late gestation (7 January 1945 to 28 April 1945); 137 exposed to famine in mid gestation (29 April 1945 to 18 August 1945); 87 exposed to famine in early gestation (19 August 1945 to 8 december 1945); 284 conceived after famine (9 December 1945 to 28 February 1947). | To study the effects of famine during pregnancy on the prevalence of coronary heart disease in first generation. | Independent variables:
|
|
| Fransen, 2016 [65] | The Prospect-EPIC cohort [66], categorized as [67]: Unexposed (3450); Moderately exposed (2838); Severely exposed (1237). Total: 7527 women. | To investigate the association between exposure to famine in childhood and adolescence and unhealthy lifestyle later in life for the first generation. | Independent variables:
|
|
| Elias, 2003 [68] | The Prospect-EPIC cohort [66], categorized as [67]: Unexposed (45); Moderately exposed (28); Severely exposed (14). Total: 87 women. | To investigate the consequences of childhood exposure to famine on the insulin-like growth factor axis in first generation. | Independent variables:
|
|
| Painter, 2005 [44] | Five cohorts of unequal size, based on the criterion of stage of gestation in relation to famine exposure: 264 born before famine (1 November 1943 to 6 January 1945); 140 exposed to famine in late gestation (7 January 1945 to 28 April 1945); 137 exposed to famine in mid gestation (29 April 1945 to 18 August 1945); 87 exposed to famine in early gestation (19 August 1945 to 8 December 1945); 284 conceived after famine (9 December 1945 to 28 February 1947). | To study the effects of famine during pregnancy on the prevalence of microalbuminuria in first generation. | Independent variables:
| Odds ratio (OR) for albumin-creatinine ratio (ACR) ≥ 2.5 compared with non-exposed group, adjusted for gender, age, adult BMI, smoking, SES (ISEI-92), SBP, IGT or non-insulin dependent diabetes mellitus (NIDDM) (2-h glucose > 7.8 or known diabetic), cholesterol, and ECG abnormalities:
|
| Van Noord, 2004 [14] | Doorlopend Onderzoek Morbiditeit en Mortaliteit (DOM) cohort [69], categorized as [67] unexposed, moderately and severely exposed. | To explain the opposing effects of caloric deprivation during pregnancy and childhood on breast cancer and its risk factors in the first generation. | Independent variables:
| Crude hazard ratio for breast cancer risk:
|
| Painter, 2006 [26] | Subjects exposed to the 1944–1945 Dutch famine during late (n = 160), mid- (n = 138), or early (n = 87) gestation and 590 unexposed subjects at age 50 or 58 year. | To investigate the early onset of coronary disease in first generation after prenatal exposure to famine. | Independent variables:
| Persons conceived during the famine were 3 years younger than the unexposed persons at the time of CAD diagnosis (47 years compared with 50 years) and had a higher cumulative incidence of CAD [13%; hazard ratio (HR) adjusted for sex: 1.9; 95% CI: 1.0, 3.8] than did the unexposed persons. |
| Stein, 2007 [70] |
| To assess the relation between gestational exposure to famine and offspring length, weight, indexes of adiposity in middle age (for the first generation). | Independent variables:
| Exposure to starvation during gestation is strongly associated with a wide range of distribution of BMI among middle-age women (p-value < 0.05 for all, except the waist-to-hip ratio, for which p-value < 0.10). No other measures of length or body proportions in either men or women were associated with this condition. |
| De Rooij, 2007 [15] | Seven hundred and eighty-three subjects born before the famine (n = 238), exposed to famine in late gestation (n = 141), in mid gestation (n = 116), in early gestation (n = 74) and conceived after the famine (n= 214). | To determine the association between prenatal famine exposure and the prevalence of metabolic syndrome in first generation. | Independent variables:
| Exposure to famine during gestation was not significantly associated with the metabolic syndrome (OR: 1.2; 95% CI: 0.9, 1.7). Birth weight also was not significantly associated with the metabolic syndrome (OR: 1.3/1-kg decrease in birth weight; 95% CI: 0.9, 1.8/1-kg decrease in birth weight). Exposure to famine during gestation was associated with significantly higher triacylglycerol concentrations (0.1 g/L; 0.0, 0.2 g/L). Men exposed to famine in early gestation had significantly lower HDL-cholesterol concentrations (−0.08 mmol/L; −0.14, 0.00 mmol/L) than did unexposed men |
| Painter, 2008 [71] | Eight hundred and fifty-five subjects: 264 unexposed and born before famine, 350 prenatally exposed to famine, 242 unexposed and conceived after famine; 1496 subjects of the second generation (F2), accordingly to the exposure status of the first generation (F1). | To assess the effects of prenatal exposure to famine on neonatal adiposity and health in later life. | Independent variables:
| F2 birth length was decreased (−0.6 cm, p adjusted for F2 gender and birth order = 0.01) and F2 ponderal index was increased (+1.2 (kg/m3), p adjusted for F2 gender and birth order = 0.001). F1 women exposed to famine in utero also responded that had poor health 1.8 (95% CI, 1.1–2.7) times more frequently in later life than that of F1 unexposed women. |
| Van Hoek, 2009 [72] | Seven hundred and seventy-two subjects born before the famine (n = 233), exposed to famine in late gestation (n = 140), in mid gestation (n = 117), in early gestation (n = 71) and conceived after the famine (n = 211). | To investigate the effects of fetal malnutrition on type 2 diabetes risk and related phenotypes in first generation of offspring. | Independent variables:
| The TCF7L2 and IGF2BP2 variants were associated with increased type 2 diabetes mellitus (T2DM)/IGT risk (TCF7L2: OR 1.39 [95% CI 1.08–1.79], IGF2BP2: 1.43 [1.11–1.85]) and increased area under curve (AUC) for glucose (TCF7L2: β = 4.5 [1.0–8.1], IGF2BP2: β = 3.6 [0.1–7.1]). The CDKAL1 variant associated with a decreased AUC for insulin (β = −8.2 [−16.1 −0.41]), which became less strong after adjustment for BMI. The IGF2BP2 showed a significant interaction on AUC glucose (β interaction −9.2 [−16.2 −2.1], p-value = 0.009). None of the polymorphisms was associated with birth weight. |
| Haars, 2010 [73] | One thousand and thirty-five women from DOM project [69]: 452 unexposed to the famine, 358 moderately exposed and 225 severely exposed. | To examine how breast density is affected by short caloric restriction in childhood and adulthood, and whether the effect is dependent on the exposure age. | Independent variables:
| In unexposed compared to severely exposed women, means varied from 124 cm2 to 121 cm2 (p-value = 0.50) for breast size, from 23.4 to 21.8 cm2 (p-value = 0.48) for amount of dense tissue, from 87.7 to 85.4 cm2 (p-value = 0.55) for non-dense tissue and from 22.8 to 22.3% (p-value = 0.78) for relative density. Only among women who were younger than 10 years during the famine was the amount of non-dense tissue significantly lower with higher exposure, with 53.1 cm2 for severely exposed compared to 77.8 cm2 (p-value = 0.03) for unexposed. |
| Botden, 2012 [74] | Seven hundred ninety-three individuals born as term singletons in Amsterdam around the famine in the Netherlands during World War II, as described in detail earlier [75]. | To investigate whether Sirutin 1 (SIRT1) influences fetal programming during malnutrition. | Independent variables:
| A significant interaction was found between two SIRT1 single nucleotide polymorphisms (SNPs) and exposure to famine in utero on T2DM risk (p-value = 0.03 for rs7895833; p-value = 0.01 for rs1467568). Minor alleles of these SNPs were associated with a lower prevalence of T2DM only in individuals who had been exposed to famine prenatally (OR for rs7895833 0.50 [95% CI 0.24–1.03], p-value = 0.06; for rs1467568 0.48 [0.25–0.91], p-value = 0.02). |
| Van Abeelen, 2012 [76] | Seven thousand five hundred and fifty-seven women from Prospect-EPIC cohort [66], with the exposure age classified into three categories: childhood (age 0–9 years), adolescence (age 10–17 years), and young adulthood (age ≥18 years) [67]. | To investigate the association between childhood and adulthood undernutrition and T2DM in adulthood. | Independent variables:
| For moderate famine exposure, the age-adjusted T2DM HR was 1.36 (95% CI [1.09–1.70]); for severe famine exposure, the age-adjusted HR was 1.64 (1.26–2.14) relative to unexposed women. |
| Tobi, 2012 [77] | One hundred and twenty individuals: 60 (28 males and 32 females, age at examination 58.1 year [SD, 0.35 year]) exposed to famine around the moment of conception and first 10 weeks of gestation; 24 same-sex siblings (11 male, 13 female) conceived and born before the famine; 36 same-sex siblings (17 male, 19 female) conceived and born after the famine. Age at examination 57.0 year [SD, 5.9 year]. | To test if the associations between famine exposure and genetic variation are independent and to contrast the effect sizes of these associations. | Independent variables:
| The average deoxyribonucleic acid (DNA) methylation difference between exposed and unexposed was 0.5 SD for significantly associated differentially methylated regions (DMRs). Only the interactions between prenatal famine exposure and INSIGF SNPs rs3842756 (p = 0.048) and rs689 (p = 0.016) in relation to IGF2 DMR1 methylation were significant. |
| Tobi, 2015 [78] | Three hundred and forty-eight exposed to famine in utero: 73 in weeks 1–10 of gestation; 123 in weeks 11–20 of gestation; 143 in weeks 21–30 of gestation; 128 in weeks 31-delivery. (Some individuals meet the definition for exposure in two adjacent gestation periods.) 160 time-controls (1943–1947). 303 same-sex siblings. | To study the epigenome-wide association for famine exposure during specific gestation periods and for exposure to famine in any period during gestation. | Independent variables:
| Famine exposure during gestation weeks 1–10, but not weeks 11–20, 21–30 or 31-delivery, was associated with an increase in DNA methylation of cytosine phosphate guanine (CpG) dinucleotides cg20823026 (FAM150B), cg10354880 (SLC38A2) and cg27370573 (PPAP2C) and a decrease of cg11496778 (OSBPL5/MRGPRG) (p < 5.9 × 10−7, positive false discovery rate (PFDR) <0.031). There was an increase in methylation of TACC1 and ZNF385A after exposure during any time in gestation (p < 2.0 × 10−7, PFDR = 0.034) and a decrease of cg23989336 (TMEM105) after exposure around conception. SD: 0.3–0.6. |
| De Rooij, 2016 [34] | One hundred and eighteen subjects: 41 exposed to famine in early gestation; 77 unexposed to famine in gestation. Mean age: 67.5 year. | To assess the effects of undernutrition during early gestation on brain size, structure, and white matter integrity at 68 year. | Independent variables:
Diffusion Tensor Imaging (DTI) scan; Fluid-attenuated inversion recovery (FLAIR) scan. | Intracranial volume (ICV) and total brain volume (TBV) were larger in males than in females [119 mL (95% CI: 88–150) and 116 mL (86–146)]. Birth weight, head circumference at birth and at age 68 were all significantly positively associated with ICV and TBV (all p < 0.05). Males exposed to famine during early gestation had smaller ICV than unexposed males with a mean difference of 58 mL (98% CI: 11–106), corresponding to a difference of ∼5%. |
| Roseboom, 2000 [42] | Seven hundred and twenty-five subjects: 209 born before famine; 117 exposed to famine in late gestation; 41 exposed to famine in mid-gestation; 65 exposed to famine in early gestation; 226 conceived after famine. | To assess the effect of maternal malnutrition on plasma fibrinogen and factor VII concentrations in first generation adults. | Independent variables:
| Plasma fibrinogen concentrations differed by −0.01 g/L (95% CI, −0.14–0.11) in those exposed in late gestation, by −0.03 g/L (95% CI, −0.16–0.11) in those exposed in mid gestation, and by 0.13 g/L (95% CI, −0.03–0.30) in those exposed in early gestation, compared with non-exposed people. Plasma factor VII concentrations differed by 0.4% (95% CI, −5.4%–6.6%) in those exposed to famine in late gestation, by 1.5% (95% CI, −4.6%–8.1%) in those exposed in mid gestation. and by −11.8% (95% CI, −18.4–−4.8%) in those exposed in early gestation, compared with non-exposed people. |
| The Chinese Famine Cohort | ||||
| Li Y, 2011 [17] | Seven thousand eight hundred and seventy-four individuals From severely affected famine area: 834 non-exposed, 334 fetal exposed, 641 early childhood exposed, 630 mid-childhood exposed, 613 late childhood exposed; From less severely affected famine area: 1120 non-exposed, 671 fetal exposed, 1013 early childhood exposed, 958 mid-childhood exposed, 1060 late childhood exposed. | To examine if there is any association between fetal exposure to famine and the risk of metabolic syndrome in later life. | Independent variables:
| Severely affected famine area (prevalence, OR, 95% CI, p of metabolic syndrome):
|
| Li QD, 2012 [79] | Birth cohorts who were exposed to the 1959–1961 Chinese famine and birth cohorts who were not exposed. | To describe the stomach cancer mortality trends in different cohorts that had been exposed to long-term malnutrition during early life. | Independent variables:
| For males: relative risk (RR) 2.39, 95% CI 1.51–3.77. For females: RR 1.64, 95% CI 1.02–2.62. |
| Wang PX, 2012 [28] | Twelve thousand and sixty-five subjects born in Nanhai and Zhongshan areas in 1957–1964. | To assess the impact of exposure to the 1959–1961 Chinese Great Famine during fetal development and first 2 years of postnatal life on the risk of hypertension, short stature and obesity in adulthood. | Independent variables:
| Subjects exposed during the 1st trimester only had significantly higher SBP, DBP and risk of hypertension [adjusted OR = 1.36 (1.03, 1.79)]. The risk of hypertension was about 1.8-fold higher in subjects exposed to famine during infancy only (p < 0.001), and 1.3-fold higher in subjects exposed during both fetal development and infancy (p < 0.001), but was not significantly elevated in those exposed during fetal development only overall (p = 0.15). |
| Shi, 2013 [80] | Two thousand and seven subjects born between 1952 and 1964, from Jiangsu province, China. | To investigate if early life exposure to famine is related to higher risk of anemia in adulthood. | Independent variables:
| Prevalence of anemia in adulthood:
|
| Huang, 2014 [43] | Seventy thousand five hundred and forty-three women born between 1957–1965, in Zhejiang Province, China. | To investigate the associations between early life exposure to the 1959–1961 Chinese Great Famine and the levels of protein in urine in adulthood. | Independent variables:
| Famine exposure and levels of proteinuria in the rural sample (mg/day), (n= 51,978, OR (95% CI), p-value): Pre-famine cohort: 1.28 (0.73, 2.25), 0.366; Famine cohort: 1.53 (1.04, 2.16), 0.031; Post-famine cohort: 1.26 (0.99, 1.59), 0.052. Famine exposure and levels of proteinuria in the urban sample (mg/day), (n = 4563, OR (95% CI), p-value): Pre-famine cohort: 0.63 (0.18, 2.21), 0.471; Famine cohort: 0.90 (0.36, 2.28), 0.824; Post-famine cohort: 1.17 (0.65, 2.10), 0.610. |
| Wang, 2015 [18] | Six thousand eight hundred and ninety-seven adults from East China, Shanghai and 7 provinces: 1245 non-exposed (born after 1975); 1808 non-exposed born between 1963–1974); 745 fetal-exposed (1959–1962); 1911 childhood-exposed (1949–1958); 1188 adolescence/adult-exposed (1921–1948). | To explore whether early life exposure to famine and high economic status in adulthood is associated with diabetes in later life. | Independent variables:
| Exposure to starvation in utero, associated with a high economic status in adult life increases the prevalence of diabetes in middle ages and old ages. Famine exposure during the fetal period (OR 1.53, 95% CI 1.09–2.14) and childhood (OR 1.82, 95% CI, 1.21–2.73) was associated with diabetes. Subjects living in areas with high economic status had a greater diabetes risk in adulthood (OR 1.46, 95% CI 1.20–1.78). In gender-specific analyses, fetal-exposed men (OR 1.64, 95% CI, 1.04–2.59) and childhood-exposed women (OR 2.81, 95% CI, 1.59–4.97) had significantly greater risk of diabetes. |
| The Siege of Leningrad Survivors (prospective cohort study, St. Petersburg, Russia) | ||||
| Sparen, 2004 [24] | Three thousand nine hundred and seven men born in 1916–35 in Petrogradsky district, Russia | To determine whether starvation during increased growth periods have long term health consequences. | Independent variables:
| Men exposed to famine in puberty had an increased mortality from ischemic heart disease (RR 1.39, 95% CI 1.07–1.79) and stroke (1.67, 1.15–2.43), including hemorrhagic stroke (1.71, 0.90–3.22). |
| Koupil, 2007 [25] | Five thousand six hundred and thirty-four subjects, resident in St. Petersburg between 1975–1982: 3905 men born between 1916–1935; 1729 women born between 1910–1940. | To investigate the long-term consequences of the food deprivation on cardiovascular risk factors and mortality in surviving adults. | Independent variables:
| Higher mean SBP among women who experienced the severest starvation at age 6–8 years and in men who were exposed to the starvation at age 9–15 years: age adjusted differences in SBP were 7.4 (95% CI: −1.4, 16.2) mm Hg in women and 3.3 (95% CI: 1.1, 5.5) mm Hg in men. Exposure to siege was associated with a statistically significant excess among men only, with a fully adjusted overall OR for men exposed at age 6–25 of 1.20 (95% CI: 1.03, 1.39) for mean blood pressure. |
| Rotar, 2015 [81] | Three hundred and six subjects of 64–81 years, who experienced famine during the Siege; 51 age and sex-matched subjects, aged 67–82, non-exposed. | To assess cardiovascular health, markers of cardiovascular aging and telomere length in survivors of the Siege of Leningrad. | Independent variables:
| Both men and women exposed had shorter telomere length: T/S ratio 0.44 (0.25; 0.64) vs. controls 0.91 (0.47; 1.13) (p-value < 0.0001). |
| The Biafran Study Cohort (cohort study, Enugu, Nigeria) | ||||
| Hult, 2010 [27] | One thousand three hundred and thirty-nine adults, from the Human group igbo, born between 1965–1973, Nigeria: 388 exposed to famine in early childhood (born 1965–1967); 292 exposed to fetal-infant famine (born 1968–January 1970); 486 unexposed (born 1971–1973); 173 in transitional period (Februar–December 1970). | To study the risks for hypertension, diabetes and overweight in adults, after fetal and infant exposure to famine. | Independent variables:
| OR and CI for 40 years-old subjects exposed to famine:
|
References
- Network, F.S.I. Global Report on Food Crises 2017; World Food Programme: Rome, Italy, 2017; p. 16. [Google Scholar]
- Novik, K.L.; Nimmrich, I.; Genc, B.; Maier, S.; Piepenbrock, C.; Olek, A.; Beck, S. Epigenomics: Genome-wide study of methylation phenomena. Curr. Issues Mol. Biol. 2002, 4, 111–128. [Google Scholar] [PubMed]
- Robertson, K.D.; Wolffe, A.P. DNA methylation in health and disease. Nat. Rev. Genet. 2000, 1, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Iguchi-Ariga, S.M.; Schaffner, W. CpG methylation of the cAMP-responsive enhancer/promoter sequence TGACGTCA abolishes specific factor binding as well as transcriptional activation. Genes Dev. 1989, 3, 612–619. [Google Scholar] [CrossRef] [PubMed]
- Sato, F.; Tsuchiya, S.; Meltzer, S.J.; Shimizu, K. MicroRNAs and epigenetics. FEBS J. 2011, 278, 1598–1609. [Google Scholar] [CrossRef] [PubMed]
- Le Dinh Luong. Basic Principles of Genetics. Available online: http://cnx.org/contents/41c4c77e-a44c-431f-bbc0-32eb72726630@1 (accessed on 25 April 2018).
- Barker, D.J. Fetal origins of coronary heart disease. BMJ 1995, 311, 171–174. [Google Scholar] [CrossRef] [PubMed]
- Barker, D.J.; Winter, P.D.; Osmond, C.; Margetts, B.; Simmonds, S.J. Weight in infancy and death from ischaemic heart disease. Lancet 1989, 2, 577–580. [Google Scholar] [CrossRef]
- Heindel, J.J.; Balbus, J.; Birnbaum, L.; Brune-Drisse, M.N.; Grandjean, P.; Gray, K.; Landrigan, P.J.; Sly, P.D.; Suk, W.; Cory Slechta, D.; et al. Developmental Origins of Health and Disease: Integrating Environmental Influences. Endocrinology 2015, 156, 3416–3421. [Google Scholar] [CrossRef] [PubMed]
- Veenendaal, M.V.; Painter, R.C.; de Rooij, S.R.; Bossuyt, P.M.; van der Post, J.A.; Gluckman, P.D.; Hanson, M.A.; Roseboom, T.J. Transgenerational effects of prenatal exposure to the 1944-45 Dutch famine. BJOG 2013, 120, 548–553. [Google Scholar] [CrossRef] [PubMed]
- Rozek, L.S.; Dolinoy, D.C.; Sartor, M.A.; Omenn, G.S. Epigenetics: Relevance and Implications for Public Health. Annu. Rev. Public Health 2014, 35, 105–122. [Google Scholar] [CrossRef] [PubMed]
- Saulnier, D.D.; Brolin, K. A systematic review of the health effects of prenatal exposure to disaster. Int. J. Public Health 2015, 60, 781–787. [Google Scholar] [CrossRef] [PubMed]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Van Noord, P.A. Breast cancer and the brain: A neurodevelopmental hypothesis to explain the opposing effects of caloric deprivation during the Dutch famine of 1944-1945 on breast cancer and its risk factors. J. Nutr. 2004, 134, 3399s–3406s. [Google Scholar] [CrossRef] [PubMed]
- De Rooij, S.R.; Painter, R.C.; Holleman, F.; Bossuyt, P.M.; Roseboom, T.J. The metabolic syndrome in adults prenatally exposed to the Dutch famine. Am. J. Clin. Nutr. 2007, 86, 1219–1224. [Google Scholar] [CrossRef] [PubMed]
- Lussana, F.; Painter, R.C.; Ocke, M.C.; Buller, H.R.; Bossuyt, P.M.; Roseboom, T.J. Prenatal exposure to the Dutch famine is associated with a preference for fatty foods and a more atherogenic lipid profile. Am. J. Clin. Nutr. 2008, 88, 1648–1652. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Jaddoe, V.W.; Qi, L.; He, Y.; Wang, D.; Lai, J.; Zhang, J.; Fu, P.; Yang, X.; Hu, F.B. Exposure to the chinese famine in early life and the risk of metabolic syndrome in adulthood. Diabetes Care 2011, 34, 1014–1018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, N.; Wang, X.; Han, B.; Li, Q.; Chen, Y.; Zhu, C.; Chen, Y.; Xia, F.; Cang, Z.; Zhu, C.; et al. Is Exposure to Famine in Childhood and Economic Development in Adulthood Associated With Diabetes? J. Clin. Endocrinol. Metab. 2015, 100, 4514–4523. [Google Scholar] [CrossRef] [PubMed]
- Zheng, X.; Wang, Y.; Ren, W.; Luo, R.; Zhang, S.; Zhang, J.H.; Zeng, Q. Risk of metabolic syndrome in adults exposed to the great Chinese famine during the fetal life and early childhood. Eur. J. Clin. Nutr. 2012, 66, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Gluckman, P.D.; Hanson, M.A.; Cooper, C.; Thornburg, K.L. Effect of in utero and early-life conditions on adult health and disease. N. Engl. J. Med. 2008, 359, 61–73. [Google Scholar] [CrossRef] [PubMed]
- Roseboom, T.; de Rooij, S.; Painter, R. The Dutch famine and its long-term consequences for adult health. Early Hum. Dev. 2006, 82, 485–491. [Google Scholar] [CrossRef] [PubMed]
- Kin, C.F.; Shan, W.S.; Shun, L.J.; Chung, L.P.; Jean, W. Experience of famine and bone health in post-menopausal women. Int. J. Epidemiol. 2007, 36, 1143–1150. [Google Scholar] [CrossRef] [PubMed]
- Weisz, G.M.; Albury, W.R. Osteoporosis in survivors of early life starvation. Aust. J. Prim. Health 2013, 19, 3–6. [Google Scholar] [CrossRef] [PubMed]
- Sparen, P.; Vagero, D.; Shestov, D.B.; Plavinskaja, S.; Parfenova, N.; Hoptiar, V.; Paturot, D.; Galanti, M.R. Long term mortality after severe starvation during the siege of Leningrad: Prospective cohort study. BMJ 2004, 328, 11. [Google Scholar] [CrossRef] [PubMed]
- Koupil, I.; Shestov, D.B.; Sparen, P.; Plavinskaja, S.; Parfenova, N.; Vagero, D. Blood pressure, hypertension and mortality from circulatory disease in men and women who survived the siege of Leningrad. Eur. J. Epidemiol. 2007, 22, 223–234. [Google Scholar] [CrossRef] [PubMed]
- Painter, R.C.; de Rooij, S.R.; Bossuyt, P.M.; Simmers, T.A.; Osmond, C.; Barker, D.J.; Bleker, O.P.; Roseboom, T.J. Early onset of coronary artery disease after prenatal exposure to the Dutch famine. Am. J. Clin. Nutr. 2006, 84, 322–327. [Google Scholar] [CrossRef] [PubMed]
- Hult, M.; Tornhammar, P.; Ueda, P.; Chima, C.; Bonamy, A.K.; Ozumba, B.; Norman, M. Hypertension, diabetes and overweight: Looming legacies of the Biafran famine. PLoS ONE 2010, 5, e13582. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.X.; Wang, J.J.; Lei, Y.X.; Xiao, L.; Luo, Z.C. Impact of fetal and infant exposure to the Chinese Great Famine on the risk of hypertension in adulthood. PLoS ONE 2012, 7, e49720. [Google Scholar] [CrossRef] [PubMed]
- Van Abeelen, A.F.; Elias, S.G.; de Jong, P.A.; Grobbee, D.E.; Bossuyt, P.M.; van der Schouw, Y.T.; Roseboom, T.J.; Uiterwaal, C.S. Famine in the young and risk of later hospitalization for COPD and asthma. PLoS ONE 2013, 8, e82636. [Google Scholar] [CrossRef] [PubMed]
- Lopuhaa, C.E.; Roseboom, T.J.; Osmond, C.; Barker, D.J.; Ravelli, A.C.; Bleker, O.P.; van der Zee, J.S.; van der Meulen, J.H. Atopy, lung function, and obstructive airways disease after prenatal exposure to famine. Thorax 2000, 55, 555–561. [Google Scholar] [CrossRef] [PubMed]
- Song, S. Assessing the impact of in utero exposure to famine on fecundity: Evidence from the 1959-61 famine in China. Popul. Stud. 2013, 67, 293–308. [Google Scholar] [CrossRef] [PubMed]
- Elias, S.G.; van Noord, P.A.; Peeters, P.H.; den Tonkelaar, I.; Kaaks, R.; Grobbee, D.E. Menstruation during and after caloric restriction: The 1944-1945 Dutch famine. Fertil. Steril. 2007, 88, 1101–1107. [Google Scholar] [CrossRef] [PubMed]
- Yarde, F.; Broekmans, F.J.; van der Pal-de Bruin, K.M.; Schonbeck, Y.; te Velde, E.R.; Stein, A.D.; Lumey, L.H. Prenatal famine, birthweight, reproductive performance and age at menopause: The Dutch hunger winter families study. Hum. Reprod. 2013, 28, 3328–3336. [Google Scholar] [CrossRef] [PubMed]
- De Rooij, S.R.; Caan, M.W.; Swaab, D.F.; Nederveen, A.J.; Majoie, C.B.; Schwab, M.; Painter, R.C.; Roseboom, T.J. Prenatal famine exposure has sex-specific effects on brain size. Brain 2016, 139, 2136–2142. [Google Scholar] [CrossRef] [PubMed]
- Hoek, H.W.; Brown, A.S.; Susser, E. The Dutch famine and schizophrenia spectrum disorders. Soc. Psychiatry Psychiatr. Epidemiol. 1998, 33, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Na, L.; Ma, H.; Zhang, Z.; Li, T.; Lin, L.; Li, Q.; Sun, C.; Li, Y. Multigenerational effects of parental prenatal exposure to famine on adult offspring cognitive function. Sci. Rep. 2015, 5, 13792. [Google Scholar] [CrossRef] [PubMed]
- Xie, S.H.; Lagergren, J. A possible link between famine exposure in early life and future risk of gastrointestinal cancers: Implications from age-period-cohort analysis. Int. J. Cancer 2017, 140, 636–645. [Google Scholar] [CrossRef] [PubMed]
- Keinan-Boker, L.; Vin-Raviv, N.; Liphshitz, I.; Linn, S.; Barchana, M. Cancer incidence in Israeli Jewish survivors of World War II. J. Natl. Cancer Inst. 2009, 101, 1489–1500. [Google Scholar] [CrossRef] [PubMed]
- Holt, R.I. Fetal programming of the growth hormone-insulin-like growth factor axis. Trends Endocrinol. Metab. 2002, 13, 392–397. [Google Scholar] [CrossRef]
- Elias, S.G.; Peeters, P.H.; Grobbee, D.E.; van Noord, P.A. Breast cancer risk after caloric restriction during the 1944–1945 Dutch famine. J. Natl. Cancer Inst. 2004, 96, 539–546. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.P.; Peng, B.; Tang, L.; Sun, R.; Hu, S.; Wen, X.Y.; Que, P.; Wang, Y.H. Fetal and infant exposure to the Chinese famine increases the risk of fatty liver disease in Chongqing, China. J. Gastroenterol. Hepatol. 2016, 31, 200–205. [Google Scholar] [CrossRef] [PubMed]
- Roseboom, T.J.; van der Meulen, J.H.; Ravelli, A.C.; Osmond, C.; Barker, D.J.; Bleker, O.P. Plasma fibrinogen and factor VII concentrations in adults after prenatal exposure to famine. Br. J. Haematol. 2000, 111, 112–117. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Guo, C.; Nichols, C.; Chen, S.; Martorell, R. Elevated levels of protein in urine in adulthood after exposure to the Chinese famine of 1959-61 during gestation and the early postnatal period. Int. J. Epidemiol. 2014, 43, 1806–1814. [Google Scholar] [CrossRef] [PubMed]
- Painter, R.C.; Roseboom, T.J.; van Montfrans, G.A.; Bossuyt, P.M.; Krediet, R.T.; Osmond, C.; Barker, D.J.; Bleker, O.P. Microalbuminuria in adults after prenatal exposure to the Dutch famine. J. Am. Soc. Nephrol. 2005, 16, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Lin, X.; Lim, I.Y.; Wu, Y.; Teh, A.L.; Chen, L.; Aris, I.M.; Soh, S.E.; Tint, M.T.; MacIsaac, J.L.; Morin, A.M.; et al. Developmental pathways to adiposity begin before birth and are influenced by genotype, prenatal environment and epigenome. BMC Med. 2017, 15, 50. [Google Scholar] [CrossRef] [PubMed]
- Biro, F.M.; Wien, M. Childhood obesity and adult morbidities. Am. J. Clin. Nutr. 2010, 91, 1499s–1505s. [Google Scholar] [CrossRef] [PubMed]
- Murray, R.; Bryant, J.; Titcombe, P.; Barton, S.J.; Inskip, H.; Harvey, N.C.; Cooper, C.; Lillycrop, K.; Hanson, M.; Godfrey, K.M. DNA methylation at birth within the promoter of ANRIL predicts markers of cardiovascular risk at 9 years. Clin. Epigenet. 2016, 8, 90. [Google Scholar] [CrossRef] [PubMed]
- Bacos, K.; Gillberg, L.; Volkov, P.; Olsson, A.H.; Hansen, T.; Pedersen, O.; Gjesing, A.P.; Eiberg, H.; Tuomi, T.; Almgren, P.; et al. Blood-based biomarkers of age-associated epigenetic changes in human islets associate with insulin secretion and diabetes. Nat. Commun. 2016, 7, 11089. [Google Scholar] [CrossRef] [PubMed]
- Wallace, R.G.; Twomey, L.C.; Custaud, M.A.; Moyna, N.; Cummins, P.M.; Mangone, M.; Murphy, R.P. Potential Diagnostic and Prognostic Biomarkers of Epigenetic Drift within the Cardiovascular Compartment. BioMed Res. Int. 2016, 2016, 2465763. [Google Scholar] [CrossRef] [PubMed]
- Van Hoesel, A.Q.; Sato, Y.; Elashoff, D.A.; Turner, R.R.; Giuliano, A.E.; Shamonki, J.M.; Kuppen, P.J.; van de Velde, C.J.; Hoon, D.S. Assessment of DNA methylation status in early stages of breast cancer development. Br. J. Cancer 2013, 108, 2033–2038. [Google Scholar] [CrossRef] [PubMed]
- Terry, M.B.; McDonald, J.A.; Wu, H.C.; Eng, S.; Santella, R.M. Epigenetic Biomarkers of Breast Cancer Risk: Across the Breast Cancer Prevention Continuum. Adv. Exp. Med. Biol. 2016, 882, 33–68. [Google Scholar] [PubMed]
- Fu, D.G. Epigenetic alterations in gastric cancer (Review). Mol. Med. Rep. 2015, 12, 3223–3230. [Google Scholar] [CrossRef] [PubMed]
- Kok-Sin, T.; Mokhtar, N.M.; Ali Hassan, N.Z.; Sagap, I.; Mohamed Rose, I.; Harun, R.; Jamal, R. Identification of diagnostic markers in colorectal cancer via integrative epigenomics and genomics data. Oncol. Rep. 2015, 34, 22–32. [Google Scholar] [CrossRef] [PubMed]
- Staunstrup, N.H.; Starnawska, A.; Nyegaard, M.; Christiansen, L.; Nielsen, A.L.; Borglum, A.; Mors, O. Genome-wide DNA methylation profiling with MeDIP-seq using archived dried blood spots. Clin. Epigenet. 2016, 8, 81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wren, M.E.; Shirtcliff, E.A.; Drury, S.S. Not all biofluids are created equal: Chewing over salivary diagnostics and the epigenome. Clin. Ther. 2015, 37, 529–539. [Google Scholar] [CrossRef] [PubMed]
- Ravelli, A.C.; van Der Meulen, J.H.; Osmond, C.; Barker, D.J.; Bleker, O.P. Obesity at the age of 50 y in men and women exposed to famine prenatally. Am. J. Clin. Nutr. 1999, 70, 811–816. [Google Scholar] [CrossRef] [PubMed]
- Smil, V. China’s great famine: 40 years later. BMJ 1999, 319, 1619–1621. [Google Scholar] [CrossRef] [PubMed]
- Ashton, B.; Hill, K.; Piazza, A.; Zeitz, R. Famine in china, 1958-61. Popul. Dev. Rev. 1984, 10, 613–645. [Google Scholar] [CrossRef]
- Pavlov, D.V. Leningrad 1941: The Blockade; University of Chicago Press: Chicago, IL, USA, 1956. [Google Scholar]
- Olsson, M.; Svensson, P. Agricultural growth and institutions: Sweden, 1700–1860. Eur. Rev. Econ. Hist. 2010, 14, 275–304. [Google Scholar] [CrossRef]
- Bygren, L.O.; Kaati, G.; Edvinsson, S. Longevity determined by paternal ancestors’ nutrition during their slow growth period. Acta Biotheor. 2001, 49, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Aall, C. Relief, nutrition and health problems in the Nigerian-Biafran war. J. Trop. Pediatr. 1970, 16, 70–90. [Google Scholar] [CrossRef] [PubMed]
- Stein, Z.; Susser, M. The Dutch famine, 1944–1945, and the reproductive process. II. Interrelations of caloric rations and six indices at birth. Pediatr. Res. 1975, 9, 76–83. [Google Scholar] [PubMed]
- Roseboom, T.J.; van der Meulen, J.H.; Osmond, C.; Barker, D.J.; Ravelli, A.C.; Schroeder-Tanka, J.M.; van Montfrans, G.A.; Michels, R.P.; Bleker, O.P. Coronary heart disease after prenatal exposure to the Dutch famine, 1944-45. Heart 2000, 84, 595–598. [Google Scholar] [CrossRef] [PubMed]
- Fransen, H.P.; Peeters, P.H.; Beulens, J.W.; Boer, J.M.; de Wit, G.A.; Onland-Moret, N.C.; van der Schouw, Y.T.; Bueno-de-Mesquita, H.B.; Hoekstra, J.; Elias, S.G.; et al. Exposure to Famine at a Young Age and Unhealthy Lifestyle Behavior Later in Life. PLoS ONE 2016, 11, e0156609. [Google Scholar] [CrossRef] [PubMed]
- Boker, L.K.; van Noord, P.A.; van der Schouw, Y.T.; Koot, N.V.; Bueno de Mesquita, H.B.; Riboli, E.; Grobbee, D.E.; Peeters, P.H. Prospect-EPIC Utrecht: Study design and characteristics of the cohort population. European Prospective Investigation into Cancer and Nutrition. Eur. J. Epidemiol. 2001, 17, 1047–1053. [Google Scholar] [CrossRef] [PubMed]
- Bogin, B. Patterns of Human Growth; Cambridge University Press: Cambridge, UK, 1999. [Google Scholar]
- Elias, S.G.; Keinan-Boker, L.; Peeters, P.H.; Van Gils, C.H.; Kaaks, R.; Grobbee, D.E.; Van Noord, P.A. Long term consequences of the 1944–1945 Dutch famine on the insulin-like growth factor axis. Int. J. Cancer 2004, 108, 628–630. [Google Scholar] [CrossRef] [PubMed]
- Collette, H.J.A.; Rombach, J.J.; Day, N.E.; De Waard, F. Evaluation of screening for Breast Cancer in a non-randomised study (the DOM project) by means of a case-control study. Lancet 1984, 323, 1224–1226. [Google Scholar] [CrossRef]
- Stein, A.D.; Kahn, H.S.; Rundle, A.; Zybert, P.A.; van der Pal-de Bruin, K.; Lumey, L.H. Anthropometric measures in middle age after exposure to famine during gestation: Evidence from the Dutch famine. Am. J. Clin. Nutr. 2007, 85, 869–876. [Google Scholar] [CrossRef] [PubMed]
- Painter, R.C.; Osmond, C.; Gluckman, P.; Hanson, M.; Phillips, D.I.; Roseboom, T.J. Transgenerational effects of prenatal exposure to the Dutch famine on neonatal adiposity and health in later life. BJOG 2008, 115, 1243–1249. [Google Scholar] [CrossRef] [PubMed]
- Van Hoek, M.; Langendonk, J.G.; de Rooij, S.R.; Sijbrands, E.J.; Roseboom, T.J. Genetic variant in the IGF2BP2 gene may interact with fetal malnutrition to affect glucose metabolism. Diabetes 2009, 58, 1440–1444. [Google Scholar] [CrossRef] [PubMed]
- Haars, G.; van Gils, C.H.; Elias, S.G.; Lokate, M.; van Noord, P.A.; Peeters, P.H. The influence of a period of caloric restriction due to the Dutch famine on breast density. Int. J. Cancer 2010, 126, 2211–2215. [Google Scholar] [CrossRef] [PubMed]
- Botden, I.P.; Zillikens, M.C.; de Rooij, S.R.; Langendonk, J.G.; Danser, A.H.; Sijbrands, E.J.; Roseboom, T.J. Variants in the SIRT1 gene may affect diabetes risk in interaction with prenatal exposure to famine. Diabetes Care 2012, 35, 424–426. [Google Scholar] [CrossRef] [PubMed]
- Ravelli, A.C.; van der Meulen, J.H.; Michels, R.P.; Osmond, C.; Barker, D.J.; Hales, C.N.; Bleker, O.P. Glucose tolerance in adults after prenatal exposure to famine. Lancet 1998, 351, 173–177. [Google Scholar] [CrossRef]
- Van Abeelen, A.F.; Elias, S.G.; Bossuyt, P.M.; Grobbee, D.E.; van der Schouw, Y.T.; Roseboom, T.J.; Uiterwaal, C.S. Famine exposure in the young and the risk of type 2 diabetes in adulthood. Diabetes 2012, 61, 2255–2260. [Google Scholar] [CrossRef] [PubMed]
- Tobi, E.W.; Slagboom, P.E.; van Dongen, J.; Kremer, D.; Stein, A.D.; Putter, H.; Heijmans, B.T.; Lumey, L.H. Prenatal famine and genetic variation are independently and additively associated with DNA methylation at regulatory loci within IGF2/H19. PLoS ONE 2012, 7, e37933. [Google Scholar] [CrossRef] [PubMed]
- Tobi, E.W.; Slieker, R.C.; Stein, A.D.; Suchiman, H.E.; Slagboom, P.E.; van Zwet, E.W.; Heijmans, B.T.; Lumey, L.H. Early gestation as the critical time-window for changes in the prenatal environment to affect the adult human blood methylome. Int. J. Epidemiol. 2015, 44, 1211–1223. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.D.; Li, H.; Li, F.J.; Wang, M.S.; Li, Z.J.; Han, J.; Li, Q.H.; Ma, X.J.; da Wang, N. Nutrition deficiency increases the risk of stomach cancer mortality. BMC Cancer 2012, 12, 315. [Google Scholar] [CrossRef]
- Shi, Z.; Zhang, C.; Zhou, M.; Zhen, S.; Taylor, A.W. Exposure to the Chinese famine in early life and the risk of anaemia in adulthood. BMC Public Health 2013, 13, 904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rotar, O.; Moguchaia, E.; Boyarinova, M.; Kolesova, E.; Khromova, N.; Freylikhman, O.; Smolina, N.; Solntsev, V.; Kostareva, A.; Konradi, A.; et al. Seventy years after the siege of Leningrad: Does early life famine still affect cardiovascular risk and aging? J. Hypertens. 2015, 33, 1772–1779, discussion 1779. [Google Scholar] [CrossRef] [PubMed]



| Study Cohort | Context | Number of Articles |
|---|---|---|
| The Dutch Famine Birth Cohort | The German-occupied territory of Netherlands during the winter of 1944–1945 | 75 |
| The Holocaust Survivors | More than 1000 ghettos in the eastern and central part of Europe, 1939–1945 | 448 |
| The China’s Great Famine | China during The Great Leap, 1959–1961 | 22 |
| The Siege of Leningrad | The German occupied city of Leningrad between 8 September 1941–1927 January 1944 | 16 |
| Överkalix Cohort Study | Överkalix parish, Sweden, a sample from births in 1890, 1905, 1920, 1935 | 8 |
| Biafran Study | The Nigerian Civil War, 1967–1970 | 5 |
| Health Outcome Category | Examples |
|---|---|
| Metabolic | increased triacylglycerol concentration increased weight and body mass index metabolic syndrome impaired glucose tolerance and diabetes mellitus changes in dietary preferences, tendency to consuming high-fat diet osteoporosis with premature onset |
| Cardiovascular | ischemic heart disease cerebrovascular disease, stroke coronary artery disease with early onset increased blood pressure |
| Respiratory | asthma chronic obstructive pulmonary disease obstructive airways disease reduced lung function |
| Reproductive | impaired fecundity menstrual irregularities early onset of menopause |
| Neurological and psychiatric | smaller brain and intracranial volume congenital abnormalities schizophrenia and schizophrenia spectrum personality disorders changes in visual-motor skills, mental flexibility and selective attention |
| Oncologic | esophageal cancer gastric cancer colorectal cancer liver cancer breast cancer |
| Others | fatty liver disease increased levels of fibrinogen concentrations decreased levels of factor VII concentrations proteinuria microalbuminuria reduced creatinine clearance reduced Immunoglobulin E concentration |
| Parameter | Qualification of the Personnel and Collecting Conditions | Storing Conditions | Level of Financial Resources Needed | Applications |
|---|---|---|---|---|
| Retrospective data collection: | Data abstractors: experience with retrospective data collection from clinical record, clinical and research experience, educational preparation in health care profession Training and orientation to the study protocol needed Data collection tools | Paper document or electronic record | Low | Assess the risk for adiposity in early childhood, metabolic diseases, especially obesity, impaired glucose tolerance (IGT), type 2 diabetes mellitus (T2DM), coronary arterial disease (CAD) Assess the risk for cardiovascular diseases (CVD) |
| Child’s birth weight and size | ||||
| Maternal pre-pregnancy BMI (ppBMI) | ||||
| Gestational weight gain (GWG) | ||||
| Mother’s glucose level | ||||
| Mother’s dietary habits: calorie intake, iron, fruits, preference for salty, fat food | ||||
| Clinical measurements: | Healthcare workers: clinical and research experience, educational preparation in health care profession | Paper document or electronic record | Low | Assess the risk for metabolic diseases, especially obesity, IGT, T2DM, CAD Assess the risk for CVD |
| Skinfold thickness | ||||
| Waist to hip ratio and BMI | ||||
| Heart rate (HR) | ||||
| Pulse wave velocity (PWV) | ||||
| Biological samples for post-hoc DNA methylation tests: | Healthcare workers: clinical and research experience, educational preparation in health care profession | Possible storage for years, enabling post-hoc analyses as knowledge evolves on specific DNA methylation sites. Assess the risk for metabolic diseases and pancreatic islets function; CVD and risk for stroke; Immunoglobulin E (IgE) concentration, osteoarthritis (OA) and rheumatoid arthritis (RA); cancer, tumor recurrence, survival and response to chemotherapeutic strategy | ||
| Buccal swabs of saliva | Buccal swab pouches | −20 °C to 25 °C, up to 3 weeks | Low | |
| Dried blood samples (DBS) | Whatman 903 filter cards, 3.2 mm punch | Room temperature, for years | Low | |
| Peripheral blood samples | Needles and syringes, tubes containing sterile EDTA solution | 4 °C, −20 °C, or −80 °C, with or without 10% DMSO, for the following time periods: overnight (i.e., 15 h), 72 h, 1 week, or 1 month | High | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moraru, A.; De Almeida, M.M.; Degryse, J.-M. PALTEM: What Parameters Should Be Collected in Disaster Settings to Assess the Long-Term Outcomes of Famine? Int. J. Environ. Res. Public Health 2018, 15, 857. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15050857
Moraru A, De Almeida MM, Degryse J-M. PALTEM: What Parameters Should Be Collected in Disaster Settings to Assess the Long-Term Outcomes of Famine? International Journal of Environmental Research and Public Health. 2018; 15(5):857. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15050857
Chicago/Turabian StyleMoraru, Alexandra, Maria Moitinho De Almeida, and Jean-Marie Degryse. 2018. "PALTEM: What Parameters Should Be Collected in Disaster Settings to Assess the Long-Term Outcomes of Famine?" International Journal of Environmental Research and Public Health 15, no. 5: 857. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15050857