1. Introduction
Earthquakes are among the most terrifying and destructive of all natural hazard-caused disasters, which can arguably lead to incalculable environmental damage, construction damage, loss of life, population displacement, overcrowding, propitious circumstances for an epidemic and threats to health [
1]. China, one of the world’s most earthquake-prone countries [
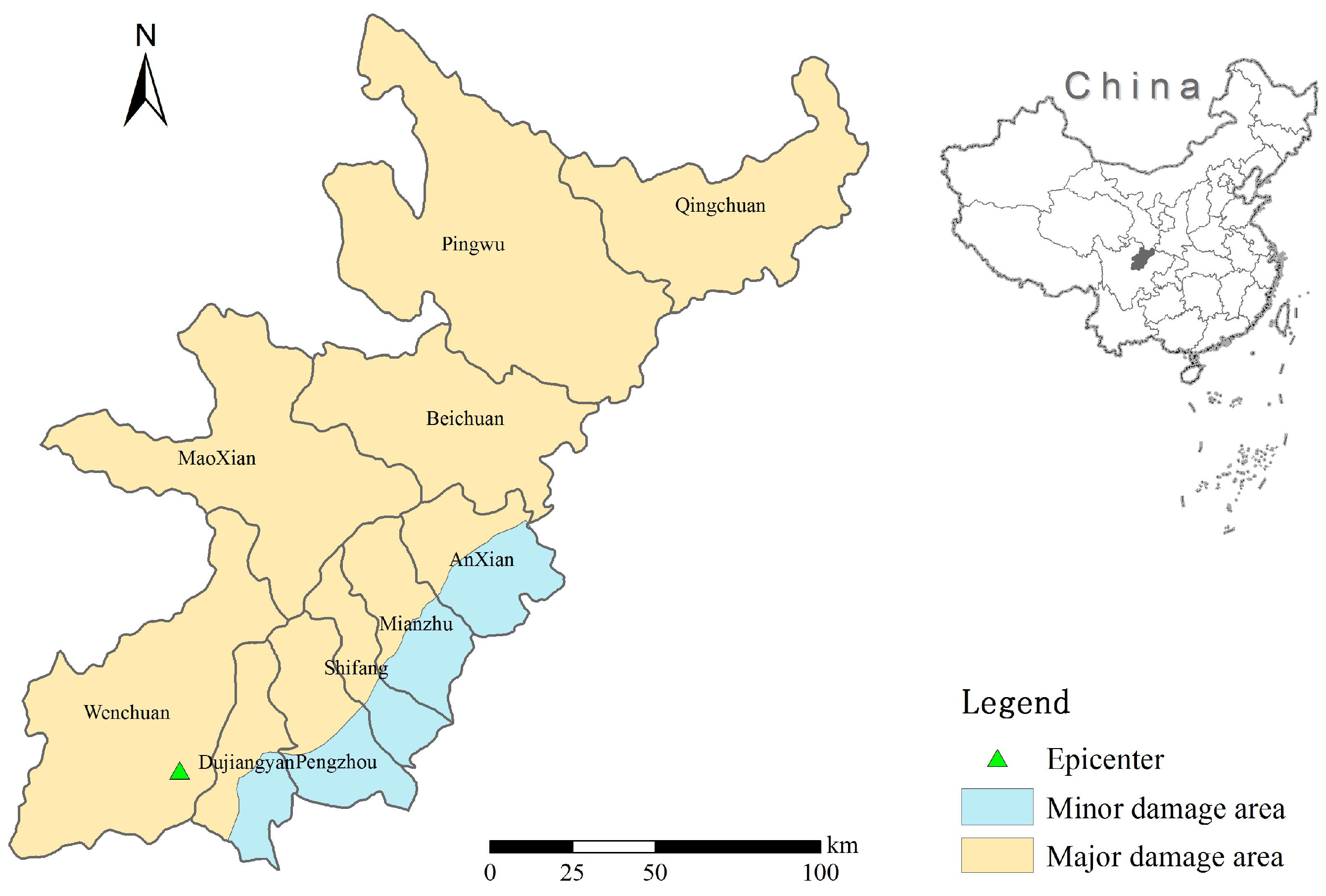
2], has experienced significant such damage events in recent years, such as the 2008 Wenchuan earthquake [
3], the 2010 Yushu earthquake [
4], and the 2013 Ya’an earthquake [
5]. The Wenchuan earthquake in the Sichuan province of China affected the most people [
1].
Emergency management activities relating to earthquake include preparedness, mitigation, response and recovery, e.g., the FEMA approach in USA, EU Civil protection in Europe, and Emergency Management in Australia [
6]. After a major earthquake, from the viewpoint of public health, timely emergency response is crucial to reduce casualties and guide relief efforts [
7]. A proper multistage continuous assessment [
1] to identify urgent public health issues is the most critical component of earthquake response.
In the early hours after an earthquake, collecting information and evaluating the extent of damage is essential for anticipating the healthcare needs of survivors, managing critical conditions [
8], and allocating limited resources. Casualties and injuries estimation is one of the most crucial processes to measure the severity of damage [
9]. The methods used to determine the loss of life caused by earthquakes can be divided into two categories. In the first category, the empirical function is proposed based on the relationship between earthquake parameters and the number of casualties reported by historical data; In the second category, the research focuses on the relationship between building damage and the number of casualties [
10], which is more accurate and reliable as building damage is main cause of earthquake casualties and injuries in China [
11,
12].
Earthquakes severely destroy or overwhelm the health infrastructure and medical service system, which hampers disaster victims’ timely access to health services. Injury and soft tissue infections are expected during the first few days after earthquake. In contrast, water source and foodborne diseases, respiratory and close contact diseases, insect-borne and natural focus diseases are anticipated for up to one month after an earthquake [
13,
14]. Identifying areas where medical services are deficient [
15,
16] is important to ensure the most appropriate medical rescuers quickly reach the disaster area where they are most needed.
The public health issues after an earthquake usually include the interruption of access to safe water and sanitation facilities, increased exposure and susceptibility to disease, population displacement with overcrowding, etc. Landslides triggered by an earthquake can cause the displacement of water pipes and building damage, resulting in water supply difficulties [
17]. The damage to drinking water supply systems and sanitation facilities on a large scale can hinder disaster victims from accessing safe water and food, which will increase the risk of waterborne and foodborne disease outbreaks. Chaos caused by population displacement and overcrowding [
18] is also associated primarily with communicable disease outbreaks. The first response in preventing an outbreak is to provide adequate shelter as soon as possible to the affected population. Emergency facility locations for earthquake victims need to be well planned [
19].
Valid and rapid information acquirement is critical to enable decision-making and resource prioritization by health care providers and emergency management officials during the response immediately after a disaster [
20]. Geographic information systems (GIS) provide a useful tool to help with this issue [
21]. Gridded population distribution maps can be used in public health applications and risk evaluation [
22,
23,
24] to predict the affected population. Remote sensing images are an important information source for an accurate overview of earthquake-induced damages [
25] using optical, LIDAR, or synthetic aperture radar (SAR) from satellite or aerial platforms [
26]. In recent years, with the development of a high resolution Earth observation system in China, high-resolution satellite imagery has been used in disaster emergency monitoring and evaluation [
27], which improves the textural and spatial feature extraction to help identify damaged regions more accurately [
28,
29].
This paper aimed to build a framework for rapid public health needs assessment, which objectives include: (1) estimating casualties and injuries; (2) identifying damaged medical facilities; (3) estimating drinking water needs; (4) identifying areas at risk of disease; and (5) identifying temporary settlement sites. This assessment will provide technical support for public health emergencies management after earthquakes.
5. Discussion
This paper discussed a framework of rapid public health needs assessment after earthquakes using GIS technology and high-resolution remote sensing images. In post-disaster situations, this assessment is essential in the rapid implementation of control measures through re-establishment and the improvement of primary healthcare delivery [
46]. Remotely sensed data have been increasingly used for monitoring, surveillance, or risk mapping. Capabilities of geographic information systems extended its use into operational disease surveillance and control. This high-resolution image solution would guide the application of Chinese satellites in public health.
Casualties and injuries estimation after an earthquake is crucial to support the design of the public health emergency response and needs to be evaluated as soon as possible. The casualty estimation model depends on the building damage situation, because in China, buildings and infrastructure are mainly responsible for the loss of lives and injuries [
47] and therefore important factors of vulnerability to earthquakes [
12]. Population distribution and its variations are another factors that influence the casualty rate. Thus, the proposed two-step estimation method considering both building collapse and population distribution could be completed in several hours accurately. The number of injuries in the 10 districts and counties affected in the Wenchuan earthquake was estimated by this paper as 288,438, compared with the injury census of 374,643 [
31], so the accuracy of our estimation is about 77%.
Damage to public infrastructure often leads to disruptions in medical care. In our evaluation, the collapse rate of medical buildings was 82.3%, while in the investigation it was 67.5% [
1]. This serious event on such a scale needs extraordinary efforts to cope with it, often with outside help or international aid.
The earthquake damage of the water supply system causes great difficulty and influences the survival of the victims. In most cases, the main health problems are caused by poor hygiene due to insufficient water and by the consumption of contaminated water. The effect on water quality of an earthquake is mainly manifested in the following two aspects: on the one hand, the direct impact of the ecological balance breakdown causes a great change to the water environment; on the other hand, damage to the industrial infrastructure and mining enterprises can result in a large number of pollutants being released into the local environment which can have a serious influence [
1]. Temporary water source setting assessment considered safety and convenience, which would further guide post-earthquake recovery and reconstruction. Actually, after the Wenchuan earthquake, the water sources were capable of meeting the demands of local residents [
48], but the destruction of water systems limited the supply of drinking water. What’s more, in the extreme cases after the earthquake, victims did not trust water supply, and lacked knowledge of water purification treatment. Thus, basic water demands should be estimated according to the minimum health need standards. The assessment of water requirements is aimed to provide a reference for the storage and transportation of relief materials. In addition, more than 20,000 medical and health workers participated in the earthquake response, as well as emergency workers from other departments, such as electric power, water conservancy, traffic, and for these there was a lack of statistics. Thus, this assessment does not consider the demand of safe drinking water for rescue workers.
The primary driver to influence the risk for communicable diseases after natural hazard-caused disasters is the interplay of safe water and sanitation facilities, the degree of crowding, the underlying health status of the population, and the availability of healthcare services [
49]. There could be outbreaks of infectious diseases after an earthquake, such as acute watery diarrhea [
50], hepatitis E [
51], and coccidiomycosis [
52]. Epidemiological studies of disasters have led to important environmental and policy changes [
53]. However, natural hazard-caused disasters do not import of diseases [
54]. Thus, the prompt assessed the risk for different contagious diseases after the Wenchuan earthquake through historic surveillance data would be helpful for situation awareness. Delay in public health assessments will decrease the efficiency of disease prevention efforts [
55]. The incidences of water-borne and foodborne disease, bacterial dysentery and other infectious diarrhea disease were higher than those of the unaffected area in the first four weeks. Factors contributing to disaster severity include environmental damage, seasonal variation and crowded conditions. No outbreak of infectious disease or other public health emergency was reported in the Wenchuan earthquake [
56].
For natural foci diseases, schistosomiasis was selected to be evaluated. After the Ya’an earthquake, the damaged streams and ditches caused a widening of the water surface which would potentially leading to the spread of Oncomelania snails. Meanwhile, the people who were relocated due to the earthquake may have higher exposures to the contaminated environment. High risk areas were mapped to provide clues to guide disaster management.
For impacts on public health, injury and psychosocial damage are important effect [
57], while an indirect threat to epidemics comes from possible disruption of food and water security and environmental safety. This threat is increased by the displacement of populations as a result of damage to residential buildings. In China, measures generally are in place to prevent this from happening [
58]. The quality of earthquake response depends on the settlement selection strategy. Here, indicators were selected following several principles. Through the comparison of remote sensing images, we can see that the location of our site is consistent with the distribution of relief tents set up after the actual investigation.
This methodology is useful for ex post evaluations, some application could provide suggestions for ex-ante evaluations, which would be significant to strengthen national emergency preparedness capacity [
59]. In emergency management information system, the GIS package should be emphasized to integrate and analysis multi-source data timely.
In the further post-earthquake recovery, the quality of construction should be emphasized. Especially in urban areas, where most residential buildings are made from concrete and brick, the main danger comes from collapsing buildings and falling debris. This threat is increased by the fact that many buildings in Chinese cities are high-rise. However, since the 1990s codes for construction and planning have been specified, which has led to higher levels of earthquake-resistance and better construction standards. The danger posed by earthquakes can be limited by building structures that can withstand earthquakes and will retain sufficient structural integrity to avoid collapse [
60].
Disease surveillance systems should be strengthened, which is generally sufficient for controlling transmission of epidemic diseases. Usual post-disaster sanitation measures should be taken, especially the cardiovascular disease prevention [
61] and mental health awareness [
62]. Early implementation of immunization campaigns probably has a protective effect, and vaccination is recommended each time non-immunized populations are moved to camps.
All natural disasters are unique in that the affected regions have different social, economic, and health backgrounds, but many similarities exist, and knowledge about these can ensure that the health and emergency medical relief and limited resources are well-managed. Good disaster management must link data collection and analysis to the decision-making process [
63]. How to use this rapid assessment in emergency management needs further discussion.

 ,
, 







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}